Extremely High CK-MB Levels Exceeding Total CK Levels in A Patient with Chest Pain:A Case Report
Shu-Jung Tsai, Tsang-En Wang, Shee-Chan Lin, Chi-In Lo*, Ching-I Lo**, and Chi-Yuan Tseng***
Division of Gastroenterology, Department of Internal Medicine *Department of Internal Medicine, **Urology, ***Pathology Mackay Memorial Hospital, Taipei, Taiwan
Abstract
An 82-year-old man presented with left chest pain and was found to have an elevated creatine kinase MB (CK-MB) value greatly exceeding the total creatine kinase (CK) activity. Subsequent electrophoresis showed that creatine kinase MM (CK-MM) accounted for 100% of the total CK activity. Eventually, the patient was diagnosed with prostatic adenocarcinoma (stage D). His elevated CK-MB was most likely due to the presence of macro CK. It is important to be aware of different causes of CK isoenzyme elevation. When the patient's condition is not compatible with myocardial infarction, malignancy must be considered. ( J Intern Med Taiwan 2003;14: 243-247 )
Key Words:Creatine kinase, Creatine kinase MB, Acute myocardial infarction, Prostatic adenocarcinoma
Introduction
Commonly available tests to assess cardiac injury include creatine kinase (CK) and CK isoenzymes. The latter include CK-BB, which predominates in brain, prostate, gut, lung, bladder, uterus, placenta, and thyroid, and CK-MM, found in skeletal and
cardiac muscle. CK-MB is present, to various degrees, in heart muscle (25% to 46%
of CK activity) and also to a minor degree in skeletal muscle (<5%)1.Classically, an increase in the myocardial-specific enzyme CK-MB is considered the hallmark of acute myocardial infarction, and increased levels are frequently interpreted by the clinician as objective evidence of myocardial cell damage. However, increased CK-MB may be found in the absence of myocardial injury, notably when macro
creatine kinase or CK-BB is present in the plasma. These forms of the enzyme interfere with the immunoinhibition methods normally used in emergency room laboratories to measure CK-MB.
We present a patient with extremely high levels of CK-MB and discuss the approach to diagnosis, laboratory methods for the determination of CK-MB, and technical reasons for false positive elevations of CK-MB.
Case Report
An 82-year-old man came to the emergency department because of left chest pain of one day's duration. Myocardial ischemia was initially considered. The pain was unrelated to external pressure or movement, did not radiate to the jaw or back, and was not relieved by rest. The patient had noted nausea and poor appetite a few days earlier. He denied cough, fever, wheezing, dyspnea, hemoptysis, or weight loss.
He complained of nocturia (6 to 7/night), urinary frequency, and decreased caliber of the urine stream for several days. He also noted right flank soreness for a month.
There was no history of urinary urgency. He had had a transurethral resection of the prostate gland (TURP) for benign prostatic hypertrophy at the age of 73.
He did not use alcohol, tobacco, or illegal drugs. There was no history of diabetes mellitus, hypertension, hyperlipoproteinemia, asthma, or chest trauma.
The patient's temperature in the emergency department was 37.4 ℃, the pulse was 104, the respiratory rate was 20, and the blood pressure was 142/61 mmHg. There were no skin lesions or lymphadenopathy. The head and neck were normal. The carotid pulses were full without bruits. The lungs were clear. The heart, abdomen, arms and legs were normal. There was punch tenderness of the right costovertebral angle.
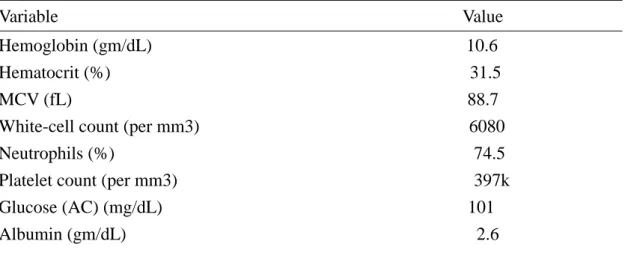
The results of hematologic and other blood tests are shown in Table 1. The CK level was 964 U/L, the CK-MB level was 1205 U/L, and the aspartate aminotransferase level was 80 U/L. Serial enzyme values are shown in Figure 1.
An electrocardiogram showed a sinus tachycardia at a rate of 100 per minute. A chest radiograph revealed a configuration suggestive of hypertensive cardiovascular disease. A radiograph of the abdomen showed paralytic ileus and osteophytes of the lower thoracic and lumbar spine. Abdominal sonography revealed right
hydronephrosis. The patient was admitted to the hospital because of right
hydronephrosis, unexplained chest pain, and the extremely high levels of CK-MB.
Electrophoresis revealed that CK-MM accounted for 100% of the total CK activity.
An intravenous pyelogram showed right hydronephrosis and hydroureter to the right vesicoureteral junction. The prostate specific antigen was 821.1 ng/ml. Prostate sonography showed a heterogenous gland with an uneven capsule. A urodynamic
study revealed a low uroflow rate and the presence of residual urine. A bone scan revealed multiple foci of increased uptake in the skull, cervical and thoracolumbar spine, pelvis, ribs, sternum, scapulae, and femora. Based on these findings, the patient was operated on for prostate cancer and underwent TURP and bilateral orchiectomy for stage D adenocarcinoma of the prostate.
Discussion
CK activity is greatest in striated muscle, brain, and heart tissue. The active form of CK is a dimer composed of two subunits, so that only three different pairs of subunits can exist: BB, MB, and MM 1. CK activity may also be found in a macromolecular form called macro CK. It is often found transiently in up to 6% of patients, but only a small proportion of these have abnormal total CK activities. Macro CK exists in two forms, types 1 and 2. Type 1 is usually a complex of CK-BB and IgG, but other complexes have been described, such as CK-MM with IgA. Type 2 is an oligomeric mitochondrial CK with a reported prevalence between 0.5% and 2.6% 1.
The three major techniques for measuring CK isoenzymes are electrophoresis, ion-exchange chromatography, and immunologic methods. Electrophoresis is generally considered the most specific means of identifying the isoenzymes, but the presence of atypical macro-CK isoenzymes can lead to inaccurate results 2,3.
Immunoinhibition is simpler and faster than immunoprecipitation and is more commonly used. In this method anti-CK-M antibody is used to inhibit both M subunits of CK-MM and the single M subunit of CK-MB, allowing determination of the enzyme activity of B subunits. Then the CK-MB value is computed by a doubling of the activity of the B subunits. If this is the technique used by a clinical laboratory to detect CK-MB, it must assume the absence of CK-BB or macro CK from the tested serum 1. This is a potential source of a false positive CK-MB. An elevated CK-BB may spuriously double the CK-MB. Furthermore, macro CK is not inhibited by antibodies to either CK-M or CK-B and thus can also cause spuriously high CK-MB values when using the immunoinhibition method 4,5. Electrophoresis of CK enzymes may be the best way to resolve problems with immunoinhibition 6.
The equipment used in our hospital for electrophoresis is the Rapid ElectroPhoresis unit (Rep R , Cat. No. 3078) from Helena Laboratories (Beaumont, Texas, USA). The Rep R is a totally automated electrophoresis system designed for high-volume and through-put analysis. The on-board computer controls sample application onto
agarose gels, electrophoresis at various programmable voltages and currents, substrate application and incubation, drying, and precision densitometry 7.
The falsely elevated CK-MB in our patient was not related to CK-BB because electrophoresis revealed only CK-MM. Was CK-MM therefore the cause of his
falsely elevated CK-MB? Another possibility is macro CK (type 1 or 2), which may be difficult to differentiate from CK-MM on electrophoresis alone 8. In one electrophoretic system, the macro CK might appear to be distinct from CK-MM, while in another system, macro CK might migrate along with the CK-MM and easily be mistaken for it 9. We suspect this was the case in our patient and that he in fact had macro CK. We would need a suitable electrophoretic method that clearly demonstrates this unusual isoenzyme to confirm our impression 9.
Macro CK comigrating electrophorectically with creatine CK-MM can easily be unmasked by including an immunoprecipitation step before electrophoresis 8,10. The MM isoenzyme is removed first by precipitation with M-subunit-specific antibodies 10. Stein showed that detection of macro CK type 2 or exact identification of
electrophoretic bands is only possible if two independent methods are applied in combination (e.g., electrophoresis and immunoinhibition or heat inactivation and activation) 11.
Macroenzymes are serum enzymes that have a higher molecular mass than the corresponding enzymes normally found in serum under physiologic or
pathophysiologic conditions 12. There are many reports of prostatic cancer or other cancers with elevated CK-BB 2,4,13,14 or the presence of macro CK 10,12,15,16,17.
Clinicians should consider the possibility of prostatic carcinoma or other cancers when elevated CK-MB is present in patients who fail to show clear-cut clinical evidence of AMI 18. At many hospitals, assays for both CK-MB and cardiac troponins are routinely ordered for all patients with acute chest pain. The assay for CK-MB is inexpensive, and serial measurements permit detection of reinfarction.
Hence, CK-MB measurement is unlikely to disappear completely from diagnostic strategies for acute chest pain 13. The explanation for an increase in CK-MB, however, should be consistent with the clinical diagnosis and not simply equated to myocardial necrosis. We suggest that elevated CK-MB levels not consistent with the patient's condition be evaluated with electrophoresis, or better yet, with an
immunoprecipitation step before electrophoresis. Immunoinhibition is the method of choice because of (a) the ease and rapidity of performance with automated
instruments, (b) greater sensitivity than electrophoresis or a column procedure, (c) smaller sample size, and (d) lower cost per test 14.
Recognition that macroenzymes are one possible cause of elevated serum enzymes may help physicians avoid unnecessary invasive or costly procedures to investigate the abnormal enzyme levels 12. If macro CK is identified, underlying malignancy should be considered.
References
1.Moss DW, Henderson AR. Clinical enzymology. In: Brutis CA, Ashwood ER, eds.
Tietz Textbook of Clinical Chemistry. 3rd ed. Philadelphia: W.B. Saunders Co., 1999:
657-67.
2.Stein BS, Dalal FR. Creatine kinase isoenzymes and prostatic carcinoma: metastatic disease or acute myocardial infarction? J Urol 1984; 132: 142-3.
3.Sax SM, Moore JJ, Giegel JL, Welsh M. Further observations on the incidence and nature of atypical creatine kinase activity. Clin Chem 1979; 25: 535-41.
4.Jap TS, Wu QC, Ho DM, Chiang H. Spuriously high CK-MB isoenzyme activity mimicking acute myocardial infarction in a patient with adenocarcinoma of the rectum. Chin Med J (Taipei) 2000; 63: 413-7.
5.Lang H. Wurzburg U. Creatine kinase, an enzyme of many forms. Clin Chem 1982;
28: 1439-47.
6.Rosa-Jimenez F, Gasso de Campos M, Camacho Reina MV, Vazquez de Castroviejo E, Hernandez Burruezo JJ, Pousibet Sanfeliu H. Macro creatine kinase type 1 as a cause of increase of CK-MB isoenzyme. Apropos of 7 cases. Rev Esp Cardiol 1997;
50: 166-72.
7.Escobar R, Gornet TG, Wu AH. Evaluation of an automated electrophoresis analyzer for cardiac isoenzymes: the Helena Rep. Clin Chem 1988; 34: 1284.
8.Bohner J, Stein W, Steinhart R, Wurzburg U, Eggstein M. Macro creatine kinases:
results of isoenzyme electrophoresis and differentiation of the immunoglobulin-bound type by radioassay. Clin Chem 1982; 28: 618-23.
9.Sax SM, Moore JJ, Giegel JL, Welsh M. Atypical increase in serum creatine kinase activity in hospital patients. Clin Chem 1976; 22: 87-91.
10.Loshon CA, Rittenhouse SE, Bowers GN, McComb RB. Unusual findings related to atypical creatine kinases in two hospitalized patients. Clin Chem 1986; 32: 207-10.
11.Stein W, Bohner J, Bahlinger M. Analytical patterns and biochemical properties of macro creatine kinase type 2. Clin Chem 1985; 31: 1952-8.
12.Galasso PJ, Litin SC, O'Brien JF. The macroenzymes: a clinical review. Mayo Clini Proc 1993; 68: 349-54.
13.Wong SS, Wu AH, Fritsche HA. Reassessment of creatine BB as a marker for cancer of the prostate, breast, and lung. Clin Chem 1987; 33: 809-11.
14.Silverman LM, Chapman JF, Jones ME, Dermer GB, Pullano T, Tokes ZA.
Creatine kinase BB and other markers of prostatic carcinoma. Prostate 1981; 2:
109-19.
15.Arenas J, Bornstein B, Mayor JJ, Santos I, Levia O, Martinez A. Macro creatine kinase type 2 in a patient with prostatic carcinoma. Clin Chim Acta 1991; 200: 53-6.
16.Lee KN, Csako G, Bernhardt P, Elin RJ. Relevance of macro creatine kinase type 1 and type 2 isoenzymes to laboratory and clinical data. Clin Chem 1994; 40: 1278-83.
17.Stein W, Bohner J, Renn W, Maulbetsch R. Macro creatine kinase type 2: results of
a prospective study in hospitalzed patients. Clin Chem 1985;31: 1959-64.
18.Manzo V, Sun T, Lien YY. Misdiagnosis of acute myocardial infarction. Ann Clin Lab Sci 1990; 20: 324-8.
19. Lee TH, Goldman L. Evaluation of the patient with acute chest pain. N Engl J Med 2000; 342: 1187-95.
20.Loshon CA, McComb RB, Bowers GN. Immunoprecipitation and electrophoresis used to demonstrate and evaluate interference by CK-BB and atypical-CK's with CK-MB determinations by immunoinhibition. Clin Chem 1984; 30: 167-8.
肌酸激酉每同功酉每 MB 型(CK-MB)異常高且超過肌酸激酉每(CK)的胸痛病人:
一病例報告
蔡樹榮 王蒼恩 林錫泉 羅志賢* 羅景易** 曾岐元***
馬偕紀念醫院 胃腸肝膽科 *一般內科 **泌尿科 ***病理科
摘 要
一位八十二歲男性主述胸痛,被發現肌酸激酉每 MB 型(CK-MB)異常升高,且超 過肌酸激酉每(CK)值。肌酸激酉每同功酉每的電泳分析顯示為百分之百的肌酸激 酉每 MM 型(CK-MM)。這種現象可能是因為出現了巨型肌酸激酉每(macro CK),而導致檢驗時 MB 型的肌酸激酉每異常上升。巨型肌酸激酉每常與惡性疾 病相關,最後這位病人被診斷出是 D 期攝護腺癌。因此了解造成肌酸激酉每同 功酉每異常變化的原因相當重要,當發現此激酉每上升情況不符合常見的心肌梗 塞時,惡性腫瘤必須列入鑑別診斷。
Table 1. Hematologic and biochemical values
Variable Value Hemoglobin (gm/dL) 10.6 Hematocrit (%) 31.5 MCV (fL) 88.7 White-cell count (per mm3) 6080 Neutrophils (%) 74.5 Platelet count (per mm3) 397k Glucose (AC) (mg/dL) 101 Albumin (gm/dL) 2.6
ALT (U/L) 54/14 Bilirubin (T/D) (mg/dL) 0.4/0.1 Alkaline phosphatase (U/L) 280 BUN (mg/dL) 16 Creatine (mg/dL) 0.8 K (meq/L) 3.5 Na (meq/L) 137 Cl (meq/L) 106