Background: Obesity is a risk factor for gallbladder disease. The authors analyze the prevalence and clin- icopathology of gallbladder disease among obese patients in Taiwan.
Methods: Prevalence and various clinical factors associated with cholelithiasis were studied in 199 patients who were undergoing bariatric surgery for obesity. Clinical data (gender, age, BMI and associated diseases), laboratory evaluation and immunoglobulin G antibodies against Helicobacter pylori were obtained from the patient records. The histopatholog- ic findings of the gallbladder were also examined ret- rospectively. The degree of acute inflammation, chron- ic inflammation, cholesterolosis, cholesterol polyp and gastric metaplasia was determined and scored.
Results: Of the patients, 91% (n=181) were females and 9% (n=18) were males, age 34.26 ± 8.41 years, with mean BMI 35.28 ± 6.11 kg/m2. The prevalence of cholelithiasis was 10.1%. Increased diastolic blood pressure and HBsAg carrier were the only significant factors associated with cholelithiasis. All obese patients in our study presented with variable degrees of chronic mononuclear cell infiltration in the gall- bladder mucosa. Cholesterolosis was present in 100 patients (50.3%), followed by gastric metaplasia (27.1%), cholesterol polyp (16.1%) and acute inflam- mation (9.5%). Multivariate analysis showed an asso- ciation between cholelithiasis and acute and chronic inflammation. The predictors of cholesterolosis were BMI, waist circumference and high-sensitivity C-reac- tive protein. The seroprevalence of H. pylori was 42.2%. Older age, abnormal liver function tests, calci- um and HBsAg carrier were significantly different between H. pylori-seropositive and H. pylori-seroneg- ative obese patients. However, we could rarely find H.
pylori within the gallbladder mucosa.
Conclusion: Cholelithiasis in Asian obese patients is significantly associated with increased diastolic blood pressure and hepatitis B surface antigen carri- ers. Because chronic liver disease seems to be a risk factor for cholelithiasis in both non-obese and obese populations, prophylactic cholecystectomy can be considered in obese patients with HBsAg positivity.
We did not find evidence that H. pylori has a role in the pathogenesis of gallbladder disease and gall- stone by histologic and serologic examinations.
Furthermore, mucosal abnormalities of acute and chronic inflammatory cell infiltration are common in obese patients, which related to cholelithiasis.
Key words: Morbid obesity, gallbladder disease, Helicobacter pylori, histopathology
Abbreviations:
BMI, body mass index; H. pylori, Helicobacter pylori;
HBsAg, hepatitis B surface antigen; GGT, γ-glutamyltrans- ferase; HOMA-IR, homeostatic model assessment method - insulin resistance; ALT, alanine transaminase;
AST, aspartate transaminase
Introduction
Obesity is a pan-endemic health problem in both Western and Eastern countries. Gallstones are a common problem and even a greater problem in the obese population. The prevalence rate for gallstone varies among different populations in the world.
Prevalence of gallbladder disease has ranged from 2-15% in various non-obese populations as meas- ured by ultrasonography.1Prevalence of gallbladder disease in obese patients undergoing bariatric sur-
Gallbladder Disease among Obese Patients in Taiwan
Phui-Ly Liew, MD
1; Weu Wang, MD
2; Yi-Chih Lee, MHA
3; Ming-Te Huang, MD
2; Yang-Chu Lin, PhD
4; Wei-Jei Lee, MD, PhD
51
Department of Pathology, En-Chu Kong Hospital and Graduate Institute of Medical Sciences, Taipei Medical University;
2Department of Surgery, Taipei Medical University Hospital;
3Graduate Institute of Business Administration, Fu-Jen Catholic University, Hsin-Chuang City;
4Department of Business Administration, Soochow University, Taipei City; and
5Department of Surgery, Min- Sheng General Hospital, Taoyuan Hsien, Taiwan
Correspondence to: Dr. Wei-Jei Lee, 15 F, Department of Surgery, No 168, Ching-Kuo Road, Taoyuan Hsien, Taiwan.
Fax: 886-3-3469291; e-mail: [email protected]
gery has been found to range as 60-95% when eval- uated by gross and histologic examination after cholecystectomy.2-7 Dittrick et al8 concluded that obese patients have an increased incidence of benign gallbladder disease, and the relative risk was correlated with increase in the BMI. Two prospec- tive studies by Csendes et al9,10 suggested that chronic inflammatory changes could occur prior to the appearance of stones. Morbidly obese patients not only have a high frequency of gallstones, but also a high proportion of abnormal histologic find- ings in the gallbladder mucosa and a high probabil- ity of developing stones after bariatric surgery.
Taiwan is a newly industrialized country and the incidence of obesity is accelerating. The prevalence of gallstones for Chinese people in Taiwan was 4.3%, and was associated with age and diabetes mellitus.11 The prevalence, multiple risk factor analysis and histologic change of gallbladder dis- ease and gallstones in the Eastern Asian obese pop- ulation have rarely been investigated.
Helicobacter pylori is a gram-negative spiral- shaped bacillus. Recently, Helicobacter species and H. pylori DNA have been identified in resected gall- bladder tissue with chronic cholecystitis and in the bile samples.12Helicobacter species associated with the pathogenesis of human cholelithiasis and chole- cystitis was hypothesized.13,14 However, controver- sial results exist, and whether H. pylori infection plays a role remains to be determined.15-18 A large- scale study19 failed to identify the presence of H.
pylori in areas of gastric metaplasia of resected gall- bladders, suggesting that Helicobacter species rarely colonize the gallbladder epithelium. Lack of histological correlation associating Helicobacter species with hepatobiliary diseases was also noted.18,20H. pylori infection is prevalent in Taiwan.
As reported by Wu M-S et al,21the seroprevalence of H. pylori was 43.7% for morbidly obese patients and 60.0% for controls.21 The relationship of the association of obese patients with gallbladder dis- ease and H. pylori remains unclear.
The aim of this study was to retrospectively inves- tigate the clinicopathologic features of gallbladder disease and the association with seroprevalence of H. pylori among obese patients in Taiwan.
Materials and Methods
Study Design, Patient Selection and Preoperative Assessment
The retrospective study was performed with approval of the ethics committee of the En-Chu Kong Hospital. From February 1999 to October 2005, extensive preoperative and perioperative data collec- tion on 199 obese patients who underwent concomi- tant cholecystectomy during weight reduction sur- gery was evaluated. The inclusion criteria were a his- tory of obesity of >5 years duration, BMI >37 kg/m2 or BMI >32 kg/m2in the presence of diabetes alone or two other significant obesity-related co-morbidi- ties,22 documented weight-loss attempts in the past, and good motivation for surgery. Written informed consent was obtained from all patients who agreed to undergo weight reduction surgery. Ultrasound of the gallbladder was performed if the patients had symp- toms that were suggestive of biliary disease.
The preoperative assessment included a clinical and familial assessment, a psychiatric assessment, anthropometric measurements and laboratory tests.
Laboratory tests included blood count tests, liver function tests, fasting lipid profiles, fasting glucose profile, fasting insulin, C-peptide, high-sensitivity C- reactive protein, HbA1c, HOMA-IR= (insulin x glu- cose)/ 22.5, hepatitis B and C serology (HBsAg and antibody to Hepatitis C virus). Venous blood sam- ples were obtained from the patients and the sera were stored at -70C until tested. A commercially available enzyme-linked immunosorbent assay (ELISA) kit (IBL, Hamburg, Germany) with report- ed sensitivity and specificity of >95% was used to investigate the prevalence of H. pylori infection. All assays were performed in duplicate and interpreted by a single laboratory investigator unaware of the sample status. Western blot assay for IgG was per- formed if an equivocal result was noted for ELISA.
Pathological Assessment
Sections of gallbladder specimens were examined and histologic parameters graded using hematoxylin- eosin stain. Each specimen was blindly interpreted by one pathologist (P-L L). Parameters included (a) degree of acute inflammation (i.e. epithelial and stro- mal neutrophil infiltration), (b) chronic inflammation
(mononuclear cell infiltration), (c) cholesterosis, (d) presence of cholesterol polyp and (e) gastric meta- plasia. Acute inflammation was graded on a 0 to 3 semi-quantitative scale: (0) no polymorphonuclear (PMN) infiltration, (1) focal mild neutrophil infiltra- tion (<10PMN/high-powered field (HPF)), (2) focal dense neutrophil infiltration (10-20 PMN/HPF), (3) diffuse and dense neutrophil infiltration (>20 PMN/HPF). Mononuclear cell infiltration was scored on a 0 to 3 semi-quantitative scale: (0) no inflamma- tion, (1) mild inflammation (slight increase in mononuclear cells without lymphoid follicles), (2) moderate inflammation (dense but focal mononuclear inflammatory cell infiltrate without lymphoid folli- cles) and (3) severe inflammation (dense and diffuse mononuclear inflammatory cell infiltration with or without lymphoid follicles). Cholesterolosis was scored on a 0 to 2 semi-quantitative scale: (0) none, (1) mild cholesterolosis and (2) prominent choles- terolosis. Cholesterol polyp was assessed on a 0 to 2 semi-quantitative scale: (0) none, (1) few polyps and (2) many polyps. Gastric metaplasia was assessed on a 0 to 3 semi-quantitative scale: (0) no metaplasia, (1)
<10% of mucosa, (2) 10-50% of mucosa, (3) >50%
of mucosa. The modified Giemsa stain was used for identification of H. pylori in cases of interest.
Statistical Analysis
Data were expressed as median ± interquartile range, mean ± SD and percentages. Statistical analyses were performed using Chi-square test and Mann-Whitney U tests. Multivariate analysis was done on factors that were significant in the univari- ate analysis. Stepwise selection method, logistric regression and Spearman rank correlation were used to assess the significance of associations between ordinal or continuous predictors’ variables. A P- value of <0.05 was considered statistically signifi- cant. The SPSS statistical software (SPSS, Inc., Chicago, IL) was used for statistical analysis.
Results
We studied 199 patients consisting of 18 men and 181 women. The mean age was 34.26 ± 8.41 years, and the mean BMI was 35.28 ± 6.11 kg/m2. Gallstones
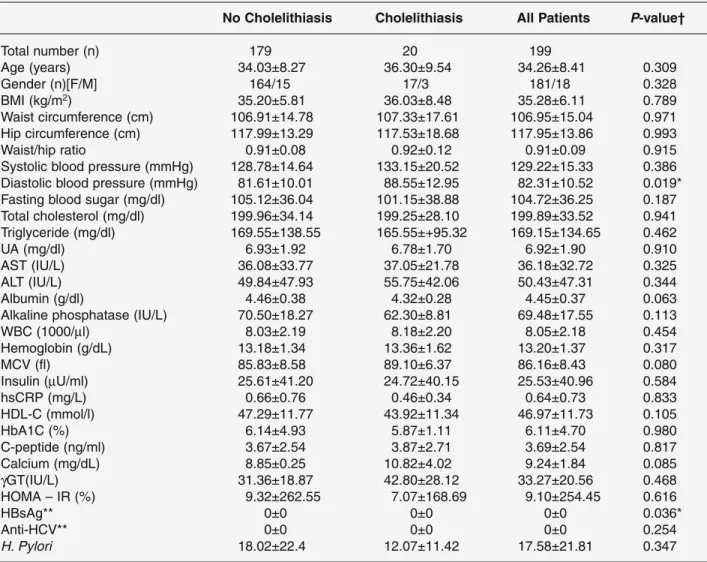
were detected in 20 patients. The prevalence rate was 10.1% (20/199). Table 1 demonstrates the comparison of demographic and clinical characteristics between patients with cholelithiasis and without cholelithiasis.
The diastolic blood pressure (P=0.019) and HBsAg carrier (P=0.036) were significantly different. Further logistic regression analysis showed that only increased diastolic blood pressure (P=0.021) was independently associated with cholelithaisis.
On pathological examination, all obese patients pre- sented with chronic inflammatory cell infiltration in their resected gallbladder specimens (Figure 1).
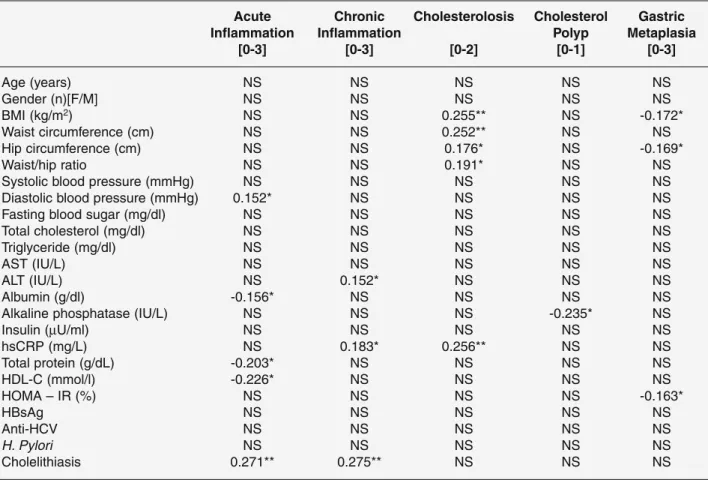
Cholesterolosis (Figure 2) was present in 100 patients (50.3%), gastric metaplasia was present in 54 patients (27.1%), cholesterol polyp was present in 32 patients (16.1%), and 19 patients (9.5%) had acute inflamma- tion. Clinical and laboratory correlations with scored histological features on gallbladder specimen are shown in Table 2. Predictors of the degree of acute inflamma- tion were best correlated with diastolic blood pressure and cholelithiasis. Inverse relationship was noted between acute inflammation and albumin, total protein and high-density lipoprotein cholesterol. Predictors of chronic inflammation were serum ALT, high-sensitivity C-reactive protein and cholelithiasis. The best predictors of cholesterolosis were BMI, waist circumference, hip circumference, waist/hip ratio and high-sensitivity C- reactive protein. Alkaline phosphatase was inversely related to cholesterol polyp. BMI, hip circumference and high-density lipoprotein cholesterol were found to be inversely related to gastric metaplasia.
Serologic testing for H. pylori was done in 154 patients, and the seroprevalence of H. pylori was 42.2 % (65/154). Clinical characteristics including age (P=0.009), AST (P=0.007), ALT (P=0.001), calcium (P=0.032) and HBsAg carrier (P =0.041) were different between H. pylori-positive and H.
pylori-negative patients. After recheck with logistic regression, only serum calcium showed a significant difference (P=0.042).
Discussion
In this study, we demonstrated that the prevalence of gallstones was 10.1% in our obese patients. The risk factors associated with gallstone formation were diastolic blood pressure and hepatitis B surface anti-
gen (HBsAg) carriers. However, gender, age, BMI, hyperlipidemia, and diabetes mellitus were not sig- nificantly associated with gallstones. Further logistic regression analysis revealed that only increased dias- tolic blood pressure was independently associated with cholelithiasis. Obesity is a chronic inflammato- ry condition and is strongly linked to raised levels of pro-inflammatory factors.23 Visceral fat and adipocytes are key regulator sites for the process of
inflammation, and atherosclerotic lesions are essen- tially an inflammatory response. Endothelial activa- tion correlates with visceral body fat, possibly through inappropriate secretion of cytokines.24 A previous study25 concluded that subjects with gall- stone disease had an increased risk of having coro- nary heart disease, which is frequently a part of the metabolic syndrome.26This study provided evidence of an important role between cholelithiasis, inflam-
Table 1. Comparison of demographic and clinical characteristics between patients with cholelithiasis and without cholelithiasis
No Cholelithiasis Cholelithiasis All Patients P-value†
Total number (n) 179 20 199
Age (years) 34.03±8.27 36.30±9.54 34.26±8.41 0.309
Gender (n)[F/M] 164/15 17/3 181/18 0.328
BMI (kg/m2) 35.20±5.81 36.03±8.48 35.28±6.11 0.789
Waist circumference (cm) 106.91±14.78 107.33±17.61 106.95±15.04 0.971 Hip circumference (cm) 117.99±13.29 117.53±18.68 117.95±13.86 0.993
Waist/hip ratio 0.91±0.08 0.92±0.12 0.91±0.09 0.915
Systolic blood pressure (mmHg) 128.78±14.64 133.15±20.52 129.22±15.33 0.386 Diastolic blood pressure (mmHg) 81.61±10.01 88.55±12.95 82.31±10.52 0.019*
Fasting blood sugar (mg/dl) 105.12±36.04 101.15±38.88 104.72±36.25 0.187 Total cholesterol (mg/dl) 199.96±34.14 199.25±28.10 199.89±33.52 0.941 Triglyceride (mg/dl) 169.55±138.55 165.55±+95.32 169.15±134.65 0.462
UA (mg/dl) 6.93±1.92 6.78±1.70 6.92±1.90 0.910
AST (IU/L) 36.08±33.77 37.05±21.78 36.18±32.72 0.325
ALT (IU/L) 49.84±47.93 55.75±42.06 50.43±47.31 0.344
Albumin (g/dl) 4.46±0.38 4.32±0.28 4.45±0.37 0.063
Alkaline phosphatase (IU/L) 70.50±18.27 62.30±8.81 69.48±17.55 0.113
WBC (1000/μl) 8.03±2.19 8.18±2.20 8.05±2.18 0.454
Hemoglobin (g/dL) 13.18±1.34 13.36±1.62 13.20±1.37 0.317
MCV (fl) 85.83±8.58 89.10±6.37 86.16±8.43 0.080
Insulin (μU/ml) 25.61±41.20 24.72±40.15 25.53±40.96 0.584
hsCRP (mg/L) 0.66±0.76 0.46±0.34 0.64±0.73 0.833
HDL-C (mmol/l) 47.29±11.77 43.92±11.34 46.97±11.73 0.105
HbA1C (%) 6.14±4.93 5.87±1.11 6.11±4.70 0.980
C-peptide (ng/ml) 3.67±2.54 3.87±2.71 3.69±2.54 0.817
Calcium (mg/dL) 8.85±0.25 10.82±4.02 9.24±1.84 0.085
γGT(IU/L) 31.36±18.87 42.80±28.12 33.27±20.56 0.468
HOMA – IR (%) 9.32±262.55 7.07±168.69 9.10±254.45 0.616
HBsAg** 0±0 0±0 0±0 0.036*
Anti-HCV** 0±0 0±0 0±0 0.254
H. Pylori 18.02±22.4 12.07±11.42 17.58±21.81 0.347
NOTE. For continuous demographics and anthropometric: mean ± SD, P-value Mann-Whitney U test. Gender, HBsAg and Anti-HCV, P-value chi-square test.
HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; HbA1c, hemoglobin A1c;
hsCRP, high-sensitivity C-reactive protein; WBC, white blood cell.
*P<0.05
**Data are given as median ± interquartile range.
†Data given for the comparison between no cholelithiasis and cholelithiasis groups.
mation, endothelial dysfunction and increased dias- tolic blood pressure in the obese population. A prospective study reported by Sheen I-S et al27sug- gested that chronic liver disease, particularly liver cirrhosis, was a risk factor for cholecystolithiasis.
This is an interesting issue because Taiwan is an endemic area for hepatitis B virus (HBV) infection, with 15-20% of its population being hepatitis B sur- face antigen (HBsAg) carriers, including many with chronic hepatitis and liver cirrhosis. Besides, Taiwan has a relative lower prevalence of gallstones11than in Western populations. The true prevalence of gall- bladder disease and gallstones in obese patients with chronic liver disease is undetermined. It is a unique opportunity to examine the prevalence of gallstones in this particular obese population. In our study, HBsAg was positive in 13.4% of 199 obese patients;
further studies between the roles for virology factor of hepatitis B in gallstone formation with the pro- gression of liver disease are needed in a larger cohort with a control non-obese population.
It has been well known that the prevalence of cholelithiasis increased along with the increasing duration and severity of chronic liver disease. The prevalence of cholelithiasis in liver cirrhotic patients
was 4 to 5.5 times higher than that of the healthy population. Steatosis was the basic liver cell injury and was common in morbidly obese patients. The prevalence of nonalcoholic fatty liver disease is 74- 98%, while that of nonalcoholic steatohepatitis (NASH) is up to 37% in the obese.28 About 15-20%
of patients with NASH develop cirrhosis. A previ- ous study in Taiwan demonstrated the relative risk for fatty liver was 1.77 (0.86-3.62, 95% confidence interval; P value 0.08) among gallstone cases in the normal control population.11 The prevalence and associated factors of gallstone disease in non-alco- holic fatty liver have been studied, both sharing insulin resistance as the common pathogenic mech- anism.29 Further studies are needed to clarify the relationship of cholelithiasis among chronic hepati- tis B carriers concurrent with steatohepatitis and liver cirrhosis in obese patients.
The present study is the first report assessing the histological findings using a scoring system com- prised of acute inflammation, chronic inflammation, cholesterolosis, cholesterol polyp and gastric meta- plasia in gallbladder tissue in obese patients. Our results agree with the previous reports that histolog- ical changes in the gallbladder could occur prior to
Figure 1. Chronic cholecystitis with inflammatory infiltrate and gastric metaplasia composed of mucin-secreting antral-type glands in the mucosa. (Hematoxylin and eosin; original magnification X 100).
Figure 2. Cholesterolosis with foamy macrophages with- in the lamina propria. (Hematoxylin and eosin; original magnification X 100).
the appearance of gallstones.8-10 Nearly all obese patients in our study presented with variable degrees of chronic mononuclear cell infiltration in the gall- bladder mucosa, and 50.3% presented with choles- terolosis. The best predictors of chronic inflamma- tion were serum ALT, high-sensitivity C-reactive protein and cholelithiasis. In addition, cholesterolo- sis was best correlated with body weight, BMI, waist and hip circumferences, waist/hip ratio and high-sensitivity C-reactive protein. It was interest- ing to find that both acute and chronic inflammation were significantly associated with gallstone forma- tion. The significance of pathological findings of inflammatory cell infiltration and cholesterolosis with respect to the development of gallbladder dis- ease and gallstone is not clear.
A pathological role of H. pylori with respect to the development of gallstone was not found in our study.
We could rarely find H. pylori-like microorganism on histopathologic examination. A previous study from Korea concluded that H. pylori DNA may be present in the bile but did not colonize the bile duct epitheli- um.18 The incidence of H. pylori seroprevalence in our obese patients undergoing cholecystectomy was 42.2%. Our obese patients positive for H. pylori were associated with older age, decreased liver function tests, increased serum calcium and HBsAg carrier.
We did not investigate H. pylori DNA determined by polymerase chain reaction and sequence analysis from the resected gallbladder. Our results do not exclude the possibility of Helicobacter infection as a cofactor in the development of gallstones.
Table 2. Analysis of the association between clinical and laboratory data and histological features (n=199)
Acute Chronic Cholesterolosis Cholesterol Gastric
Inflammation Inflammation Polyp Metaplasia
[0-3] [0-3] [0-2] [0-1] [0-3]
Age (years) NS NS NS NS NS
Gender (n)[F/M] NS NS NS NS NS
BMI (kg/m2) NS NS 0.255** NS -0.172*
Waist circumference (cm) NS NS 0.252** NS NS
Hip circumference (cm) NS NS 0.176* NS -0.169*
Waist/hip ratio NS NS 0.191* NS NS
Systolic blood pressure (mmHg) NS NS NS NS NS
Diastolic blood pressure (mmHg) 0.152* NS NS NS NS
Fasting blood sugar (mg/dl) NS NS NS NS NS
Total cholesterol (mg/dl) NS NS NS NS NS
Triglyceride (mg/dl) NS NS NS NS NS
AST (IU/L) NS NS NS NS NS
ALT (IU/L) NS 0.152* NS NS NS
Albumin (g/dl) -0.156* NS NS NS NS
Alkaline phosphatase (IU/L) NS NS NS -0.235* NS
Insulin (μU/ml) NS NS NS NS NS
hsCRP (mg/L) NS 0.183* 0.256** NS NS
Total protein (g/dL) -0.203* NS NS NS NS
HDL-C (mmol/l) -0.226* NS NS NS NS
HOMA – IR (%) NS NS NS NS -0.163*
HBsAg NS NS NS NS NS
Anti-HCV NS NS NS NS NS
H. Pylori NS NS NS NS NS
Cholelithiasis 0.271** 0.275** NS NS NS
NOTE. Spearman correlation coefficients used for continuous clinical and laboratory variables.
HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; hsCRP, high-sensitivity C-reac- tive protein.
**Correlation is significant at 0.01 level (2-tail).
*Correlation is significant at 0.05 level (2-tail).
Obesity and rapid weight loss induced by bariatric surgical procedures are both risk factors for the development of cholelithiasis.30-32 Preoperative ultrasonography33 or intraoperative findings other than palpable gallstones were inaccurate at predict- ing those patients who would benefit from con- comitant cholecystectomy. A review of the current standard care for cholecystectomy for patients undergoing bariatric surgery was conducted.34 A study indicated that a noninterventionist approach to the gallbladder was appropriate for patients under- going adjustable gastric banding surgery.35 Our study did not examine the prevalence and risk fac- tors of gallstone formation after bariatric operations.
Further study is warranted to estimate the risk for developing gallstone and gallbladder disease after bariatric surgery in the Asian obese population.
In conclusion, the prevalence of cholelithiasis is lower in Asian than in Western obese patients and is significantly associated with increased diastolic blood pressure and hepatitis B surface antigen carri- ers. Chronic liver disease seems to be a risk factor for cholelithiasis in both non-obese and obese popula- tions. Prophylactic cholecystectomy can be consid- ered in HBsAg positive obese patients. H. pylori has no role in the pathogenesis of gallbladder disease and gallstones by histologic and serologic examinations.
Furthermore, mucosal abnormalities of acute and chronic inflammatory cell infiltration are common in obese patients, which related to cholelithiasis.
References
1. Kodama H, Kono S, Todoroki I et al. Gallstone dis- ease risk in relation to body mass index and waist-to- hip ratio in Japanese men. Int J Obes 1999; 23: 211-6.
2. Aidonopouios AP, Papavramidis ST, Zaraboukas TG et al. Gallbladder findings after cholecystectomy in morbidly obese patients. Obes Surg 1994; 4: 8-12.
3. Calhoun R, Willbanks O. Coexistence of gallbladder disease and morbid obesity. Am J Surg 1987; 154:
655-8.
4. Fobi M, Lee H, Igwe D et al. Prophylactic cholecys- tectomy with gastric bypass operation: incidence of gallbladder disease. Obes Surg 2002; 12: 350-3.
5. Hamad GG, Ikramuddin S, Gourash WF et al.
Elective cholecystectomy during laparoscopic roux- en-y gastric bypass: is it worth the wait? Obes Surg
2003; 13: 76-81.
6. Liem RK, Niloff PH. Prophylactic cholecystectomy with open gastric bypass operation. Obes Surg 2004;
14: 763-5.
7. Guadalajara H, Baro RS, Pascual I et al. Is prophylac- tic cholecystectomy useful in obese patients undergo- ing gastric bypass? Obes Surg 2006; 16: 883-5.
8. Dittrick GW, Thompson JS, Campos D et al.
Gallbladder pathology in morbid obesity. Obes Surg 2005; 15: 238-42.
9. Csendes A, Smok G, Burdiles P et al. Histological findings of gallbladder mucosa in 95 control subjects and 80 patients with asymptomatic gallstones. Dig Dis Sci 1998; 43: 931-4.
10. Csendes A, Burdiles P, Smok G et al. Histologic find- ings of gallbladder mucosa in 87 patients with morbid obesity without gallstones compared to 87 control subjects. J Gastrointest Surg 2003; 7: 547-51.
11. Lu S-N, Chang W-Y, Wang L-Y et al. Risk factors for gallstones among chinese in taiwan. J Clin Gastroenterol 1990; 12: 542-6.
12. Fox JG, Dewhirst FE, Shen Z et al. Hepatic Helicobacter species identified in bile and gallbladder tissue from chileans with chronic cholecystitis.
Gastroenterol 1998; 114: 755-63.
13. Lin T-T, Yeh C-T, Wu C-S et al. Detection and partial sequence analysis of helicobacter pylori dna in the bile samples. Dig Dis Sci 1995; 40: 2214-9.
14. Neri V, Margiotta M, Francesco VD et al. Dna sequences and proteic antigens of H. Pylori in chole- cystic bile and tissue of patients with gallstones.
Aliment Pharmacol Ther 2005; 22: 715-20.
15. Mendez-Sanchez N, Pichardo R, Gonzalez J et al.
Lack of association between helicobacter sp coloniza- tion and gallstone disease. J Clin Gastroenterol 2001;
32: 138-41.
16. Chen W, Li D, Cannan RJ et al. Common presence of Helicobacter DNA in the gallbladder of patients with gallstone diseases and controls. Dig Liver Dis 2003;
35: 237-43.
17. Maurer KJ, Rogers AB, Ge Z et al. Helicobacter pylori and cholesterol gallstone formation in c57l/j mice: a prospective study. Am J Physiol Gastrointest Liver Physiol 2006; 290: G175-82.
18. Myung S-J, Kim M-H, Shim KN et al. Detection of Helicobacter pylori DNA in human biliary tree and its association with hepatolithiasis. Dig Dis Sci 2000; 45:
1405-12.
19. Arnaout AH, Abbas SH, Shousha S. Helicobacter pylori is not identified in areas of gastric metaplasia of gallbladder. J Pathol 1990; 160: 333-4.
20. Leong RWL, Sung JJY. Helicobacter species and hepatobiliary diseases. Aliment Pharmacol Ther
2002; 16: 1037-45.
21. Wu M-S, Lee W-J, Wang H-H et al. A case-control study of association of Helicobacter pylori infection with morbid obesity in taiwan. Arch Intern Med 2005;
165:1552-5.
22. Lee W-J, Wang W. Bariatric surgery: Asia-Pacific perspective. Obes Surg 2005; 15: 751-7.
23. Dixon JB, O’Brien PE. Obesity and the white blood cell count: changes with sustained weight loss. Obes Surg 2006; 16: 251-7.
24. Ziccardi P, Nappo F, Giugliano G et al. Reduction of inflammatory cytokine concentrations and improvement of endothelial functions in obese women after weight loss over one year. Circulation 2002; 105: 804-9.
25. Mendez-Sanchez N, Bahena-Aponte J, Chavez-Tapia NC et al. Strong association between gallstones and cardiovascular disease. Am J Gastroenterol 2005;
100: 827-30.
26. Nervi F, Miquel JF, Alvarez M et al. Gallbladder dis- ease is associated with insulin resistance in a high risk hispanic population. J Hepatology 2006; 45: 299-305.
27. Sheen I-S, Liaw Y-F. Hepatology 1989; 9: 538-40.
28. Dixon JB, Bhathal PS, O’Brien PE. Nonalcoholic fatty liver disease: predictors of nonalcoholic steato- hepatitis and liver fibrosis in severely obese.
Gastroenterology 2001; 121: 91-100.
29. Loria P, Lonardo A, Lombardini S et al. Gallstone dis- ease in non-alcoholic fatty liver: prevalence and asso- ciated factors. J Gastroenterol Hepatol 2005; 20:
1176-84.
30. Deitel M, Petrov I. Incidence of symptomatic gall- stones after bariatric operations. Surg Gynecol Obstet 1987; 164: 549-52.
31. Seinige UL, Sataloff DH, Lieber CP et al. Gallbladder disease in the morbidly obese patient. Obes Surg 1991; 1: 51-6.
32. Kiewiet RM, Durian MF, Leersum M: gallstone for- mation after weight loss following gastric banding in morbidly obese dutch patients. Obes Surg 2006; 16:
592-96.
33. Oria HE. Pitfalls in the diagnosis of gallbladder dis- ease in clinically severe obesity. Obes Surg 1998; 8:
444-51.
34. Mason EE, Renquist KE, IBSR Data Contributors.
Gallbladder management in obesity surgery. Obes Surg 2002; 12: 222-9.
35. O’Brien PE, Dixon JB. A rational approach to cholelithiasis in bariatric surgery. Arch Surg 2003;
138: 908-12.
(Received August 10, 2006; accepted November 6, 2006)