1
NONCLINICAL FACTORS ASSOCIATED WITH TREATMENT WITH PERITONEAL DIALYSIS IN ESRD PATIENTS IN TAIWAN
Hsiu-Chen Huang,
1,2Jiun-Yi Wang,
2Chia-Chu Chang,
1Ping-Fang Chiu,
1Ming-Che Chiang,
1and Yu Yang
1Division of Nephrology,
1Department of Internal Medicine, Changhua Christian Hospital, Changhua;
Department of Healthcare Administration,
2Asia University, Taichung, Taiwan, ROC
Correspondence to: J.Y. Wang, Department of Healthcare Administration, Asia University, No. 500, Lioufeng Road, Wufeng, Taichung County 41354, Taiwan, ROC.
Received 8 June 2009; accepted 21 January 2010.
♦♦
♦♦
♦ Objectives: Less than 10% of end-stage renal disease (ESRD) patients in Taiwan receive peritoneal dialysis (PD), which reveals the situation of underutilization of PD. We thus aimed to investigate factors associated with treatment with PD in ESRD patients in Taiwan.
♦♦
♦♦
♦ Patients: Patients that were 18 years of age or older and had been on dialysis for at least 3 months since 2001 were recruited and interviewed with a structured questionnaire.
♦♦
♦♦
♦ Results: 98 hemodialysis (HD) and 102 PD patients were recruited. In univariate analysis, age, sex, level of education, employment status, marital status, traffic time, family sup- port, patient cognition, and receptivity were correlated with treatment with PD. Multivariate analysis showed that pa- tients that were not married (p = 0.006), that spent more time traveling to the dialysis clinic (p = 0.006), that were not emergent at the start of dialysis (p = 0.003), and that had better family support (p = 0.045), a higher cognition of dialysis (p = 0.034), and stronger receptivity to dialysis (p < 0.001) were more likely to receive PD.
♦♦
♦♦
♦ Conclusions: We recommend patients follow the standard process to obtain more exhaustive information, consulta- tion, and early referral. In addition, we suggest healthcare providers remind patients to take into account such nonclinical factors as family support and patient receptiv- ity when they choose their dialysis modality.
Perit Dial Int 2010; 30:xx–xxx www.PDIConnect.com epub ahead of print: doi: 10.3747/pdi.2009.00112
KEY WORDS: Patient cognition; dialysis modality; end- stage renal disease; hemodialysis.
T
he incidence and prevalence rates of end-stage renal disease (ESRD) in Taiwan (418 and 2226 per million in 2006) have persisted at high levels in recent years (1).Although there is a small fraction of patients receiving
renal transplant therapy, most patients need to take long-term dialysis. Medical expenses arising therein be- come a heavy burden on the finances of the National Health Insurance (2).
Among ESRD patients in Taiwan, the proportion using peritoneal dialysis (PD) is much lower than that using hemodialysis (HD). An annual report of dialysis utiliza- tion in Taiwan shows that the proportions of PD and HD utilization are 8.5% and 91.5% respectively (3). This imbalanced result indicates that PD is underused. It has been reported that nephrologists in Canada and in the United Kingdom thought 37% and 38% respectively of ESRD patients should be treated with PD to optimize pa- tients’ clinical outcomes (4,5). Although nephrologists in other countries suggested a relatively low proportion, it still stands at 20% and above (6–8).
Generally, a chronic kidney disease (CKD) patient should follow a standard process to receive complete resources of medical care, education, and consultation.
Information on dialysis modality is expected to be pro- vided to a patient with CKD stage 4 or earlier. A patient will then select an appropriate dialysis modality based on his/her preference or doctor’s suggestion. Practically, however, some patients either receive insufficient infor- mation or are not willing to participate in the process (9). The result is that a portion of patients do not follow the standard process, thereby increasing the possibility of emergent dialysis; that is, patients did not have a planned start for dialysis and proceeded to acute HD through temporary HD catheters.
When patients face choosing a dialysis modality, they may not be sure what to do or what should be taken into account. From a patient’s point of view, consideration of clinical evaluations is a professional matter and they might feel that they should follow their doctors’ advice.
Thus, the remaining factors patients can take into account may be nonclinical factors. In the present study, there- fore, we proposed to identify nonclinical factors associ- ated with treatment with PD for ESRD patients in Taiwan.
by guest on July 22, 2013http://www.pdiconnect.com/Downloaded from
ognition of self-care, and impact of dialysis therapy on daily living. In total, there were ten 4-point items within the scale (see Table 2); the expected range of the scale was 10 – 40.
Four interviewers attended a 4-hour training session and conducted several mock one-to-one interviews be- fore the main task. The PD patients were invited by tele- phone to participate. The consenting patients were interviewed in an unused clinic, the HD unit, or a wait- ing room. All the interviews were conducted in 2008 be- tween January and April.
The validity of the instrument was assessed by 7 phy- sicians and professionals. The content validity index for each item and scale in the questionnaire achieved 0.8 or above. A pilot sample of 20 patients was also recruited to examine the reliability of the instrument for modifi- cation. Cronbach’s coefficient alpha was 0.820, 0.794, and 0.826 for family support scale, cognition scale, and receptivity of dialysis scale, respectively.
Means and standard deviations for continuous data and frequencies and percentages for categorical data are presented to demonstrate patient characteristics. Cat- egorical variables with sparse cells (i.e., too few patients in at least 1 subgroup) were collapsed as binary in the analysis. Univariate analyses, including two-sample t-tests for continuous variables and univariate logistic regression analysis or chi-square tests for categorical variables, were conducted to study correlations between factors and dialysis modality. Factors with a p value <
0.1 in univariate analyses were then entered into the multiple logistic regression model to re-verify the sig- nificance without a model selection process. All statis- tical analyses were performed using SPSS version 12.0 (SPSS Inc., Chicago, IL, USA).
SUBJECTS AND METHODS
In this cross-sectional study, ESRD patients that were in care from 2001 to 2007 in a medical center in Mid- Taiwan were recruited and interviewed using a structured questionnaire. Patients were eligible to be recruited if they (1) had been on dialysis for at least 3 months and had not changed dialysis modality, (2) had no contra- indications, (3) were able to communicate in Chinese or Taiwanese with clear consciousness, and (4) consented to participate in the study. The study protocol was ap- proved by the Institutional Review Board of the Changhua Christian Hospital.
The structured interview questionnaire collects mainly patient data related to social demographic char- acteristics, emergent status of the start of dialysis, fam- ily suppor t, cognition of dialysis modality, and receptivity to dialysis therapy. Family support was mea- sured by a mini-scale that included four items selected from a national survey (10). Each item was measured on a Likert 5-point scale, resulting in the scale ranging from 4 to 20. The cognition scale of dialysis was established by referring to the checklist of Health Education for Di- alysis Therapy announced by the Bureau of National Health Insurance. There are eight items rated on a 4-point scale, including patient’s understanding of dialysis modality, prior physical preparation, and fre- quencies and other settings of dialysis (see Table 1).
Moreover, because of the essential difference in opera- tion between PD and HD therapies, we thought that pa- tient receptivity to dialysis was also an important factor associated with the modality. We thus constructed a scale of patient receptivity to dialysis that included patient’s perceived feeling of the medical services, rec-
TABLE 1
Items and Descriptive Results of Patient Cognition of Dialysis Modality
Item HDa PDa
1. Do you understand well the principle of each dialysis modality? 2.17±0.93 3.25±0.91 2. Do you know what prior physical preparation is needed for each modality, such as
preparation of vascular access and insertion of the PD catheter? 2.30±0.98 3.36±0.94 3. Do you understand well in what way and in what place each modality is taken? 2.41±0.98 3.44±0.87 4. Do you know how frequently and how long each modality takes? 2.26±0.97 3.49±0.91 5. Do you understand well what you need to pay attention to in diet for each modality? 2.04±0.87 2.96±1.03 6. Do you understand well the possible complications of each modality? 2.03±0.90 2.39±1.07 7. Do you understand well the contraindications to each modality? 1.90±0.86 2.07±1.05 8. Overall, do you understand well the advantages and disadvantages of each modality? 2.05±0.89 3.27±0.90 HD = hemodialysis; PD = peritoneal dialysis.
aAll items are rated on a Likert 4-point scale, where 1 = completely disagree, 2 = tend to disagree, 3 = tend to agree, and 4 = completely agree and are presented as mean±SD.
by guest on July 22, 2013http://www.pdiconnect.com/Downloaded from
RESULTS
Of 221 patients that were requested to participate in the study, 18 refused. The overall participation rate was 92%. Among the 203 patients identified as eligible for participation, only 3 did not complete the interview.
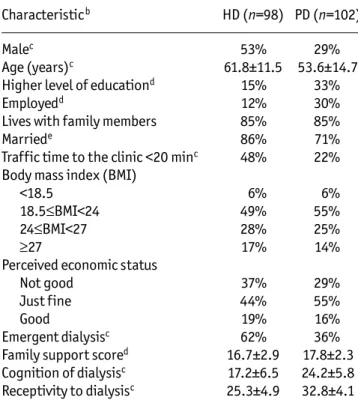
Patient characteristics are listed in Table 3. For PD and HD groups of patients respectively, 29% and 53% were males, average age was 54 and 62 years, and most pa- tients were married (71% and 86%), had lower level of education (67% and 85%), and were unemployed (70%
and 88%). While approximately half the patients in each group were rated 18.5 – 24 in body mass index measure- ment (defined as normal according to the cutoffs sug- gested by Department of Health in Taiwan), 14% and 17%
in the two groups were higher than 27 (obese). In addi- tion, the proportions of emergent dialysis were 36% and 62% in PD and HD groups, on average, and are displayed year by year in Figure 1.
Results of univariate analysis (Table 3) showed that sex (p = 0.001), age (p < 0.001), educational level (p = 0.005), marital status (p = 0.046), employment status (p = 0.003 ), family support (p = 0.002), traffic time to the dialysis clinic (p < 0.001), emergent dialysis (p <
0.001), cognition of dialysis (p < 0.001), and receptivity to dialysis (p < 0.001) were significantly correlated with treatment by PD.
Two models were considered in the multivariate analy- sis (Table 4). In model 1, in which patient cognition of and receptivity to dialysis were ignored, sex, employment status, marital status, emergent dialysis, traffic time, and family support showed significant association with
treatment by PD. In model 2, a more saturated model, most of the demographic factors were not significant except for marital status; emergent dialysis, traffic time, family support, patient cognition of dialysis, and recep- tivity to dialysis were significantly associated with treat- ment by PD. Otherwise, by model diagnosis, variables in both models have no remarkable colinearity (variance inflation factor < 2), the models were well fit (p = 0.23 and 0.63 for models 1 and 2 by Hosmer–Lemeshow test), and they had good explanatory ability (Nagelkerke R2 = 0.42 and 0.74).
DISCUSSION
In the present study, we aimed to identify nonclinical factors associated with dialysis modality. We should first recall that, because the ratio of PD:HD utilization in this medical center (approximately 1:1.4) is different from the prevalent group in Taiwan, the overall patient char- acteristics in the study are not representative of the Tai- wanese dialysis population owing to the overweight PD group. The only way to understand patient characteris- tics is to interpret them by PD/HD groups.
While age distributions of PD/HD groups in our study are similar to the Taiwanese dialysis population (11), the proportion of females in the PD group shows an increase of almost 10%. Selection bias may influence results of this study. For example, proportions of unmarried and patient cognition in the PD group are slightly overesti- mated. The median age of patients is also lower than in some other populations (1,11–13). This may be due par- tially to poorer survival of elderly patients and the TABLE 2
Items and Descriptive Results of Patients’ Perceived Receptivity to Dialysis Therapy
Item HDa PDa
1. I do mind if any visual change to my body occurs. 2.32±0.95 3.15±0.81
2. I do mind if people know that I receive dialysis. 1.97±1.10 2.66±1.02
3. I feel useless if I need somebody’s help to have my meal or go to the toilet over a long-term. 2.53±1.10 3.47±0.79
4. I feel uncomfortable going to hospitals frequently. 2.38±1.02 3.34±0.74
5. Getting medical service in clinics often reminds me that I am ill. 2.13±1.03 3.41±0.69 6. I feel safe only when medical care is operated by healthcare providers, even if it is not
complicated. (negative item)b 2.07±0.89 1.54±1.17
7. I hope I am able to perform self-care when I am ill, for as long as my health status allows. 3.40±0.73 3.75±0.54
8. I worry about self-care. (negative item)b 1.07±1.03 0.69±0.92
9. I hope dialysis therapy will not interfere with my social activities. 2.87±0.95 3.60±0.65
10. I hope I can schedule dialysis by myself. 2.84±0.95 3.71±0.57
HD = hemodialysis; PD = peritoneal dialysis.
aAll items are rated on a Likert 4-point scale, where 1 = completely disagree, 2 = tend to disagree, 3 = tend to agree, and 4 = completely agree and are presented as mean±SD.
bPatient receptivity scores were calculated by summing these 10 items after the 2 negative items were recoded as descending.
by guest on July 22, 2013http://www.pdiconnect.com/Downloaded from
slightly low median age of new patients in Taiwan (1,11).
Note that, in the multivariate analysis, the most sig- nificant demographic factors in model 1 are not signifi- cant in model 2. This is because patient cognition of and receptivity to dialysis are expected to be better in PD groups after a significant length of time on dialysis. Thus, some factors become nonsignificant after adding the two factors into the model. Therefore, those significant de- mographic factors in model 1 should be considered im- portant explanator y factors for patient choice of modality. To understand associations between dialysis modality and patient cognition of and receptivity to di- alysis, together with other factors, we focus on the re- sults from model 2 in the following discussion.
Family support has been recognized as important among nonclinical factors (14). The result in our study agrees with this argument, yet the difference in family
TABLE 3
Distribution of Patient Characteristics by Dialysis Modalitya
Characteristicb HD (n=98) PD (n=102)
Malec 53% 29%
Age (years)c 61.8±11.5 53.6±14.7
Higher level of educationd 15% 33%
Employedd 12% 30%
Lives with family members 85% 85%
Marriede 86% 71%
Traffic time to the clinic <20 minc 48% 22%
Body mass index (BMI)
<18.5 6% 6%
18.5≤BMI<24 49% 55%
24≤BMI<27 28% 25%
≥27 17% 14%
Perceived economic status
Not good 37% 29%
Just fine 44% 55%
Good 19% 16%
Emergent dialysisc 62% 36%
Family support scored 16.7±2.9 17.8±2.3 Cognition of dialysisc 17.2±6.5 24.2±5.8 Receptivity to dialysisc 25.3±4.9 32.8±4.1 HD = hemodialysis; PD = peritoneal dialysis.
aProportions for categorical variables and mean±SD for con- tinuous variables are displayed.
bUnivariate logistic regression analysis was applied to study level of education, employment status, living arrangement, marital status, and traffic time; otherwise, chi-square test and 2-sample t-test were used to study categorical and con- tinuous variables respectively.
cp < 0.001.
dp < 0.01.
ep < 0.05.
Figure 1 — Proportions of emergent dialysis at the start of di- alysis in hemodialysis (HD) and peritoneal dialysis (PD) groups from 2001 to 2007.
TABLE 4
Factors Associated with Treatment with Peritoneal Dialysis Based on Multiple Logistic Regression Analysisa
Model 1 Model 2
Variable OR 95% CI OR 95% CI
Male 0.33 (0.15–0.70)b 0.47 (0.17–1.30) Age (per 10 years) 0.78 (0.60–1.00) 0.86 (0.61–1.22) Higher level of
education 2.24 (0.91–5.54) 2.07 (0.62–6.91) Employed 2.93 (1.16–7.40)c 1.12 (0.31–4.03) Married 0.31 (0.12–0.75)b 0.16 (0.04–0.59)b Emergent dialysis 0.33 (0.17–0.66)b 0.22 (0.08–0.60)b Longer traffic time 3.57 (1.70–7.54)d 4.35 (1.53–12.4)b Family support 1.26 (1.08–1.47)b 1.25 (1.01–1.54)c Cognition of dialysis 1.09 (1.01–1.17)c Receptivity to dialysis 1.47 (1.29–1.67)d Model 1 = patient cognition of and receptivity to dialysis were ignored; OR = odds ratio; 95% CI = 95% confidence interval.
aReceipt of peritoneal dialysis was coded as 1.
bp < 0.01.
cp < 0.05.
dp < 0.001.
Proportion of emergent dialysis (%)
Year of dialysis
support score between the two groups does not appear to be distinct. Married patients were found to be less likely to receive PD in this study. This is out of line with the international literature (15,16). The reasons behind it are not clear but it may be due to the low divorce rate among Taiwanese elderly. It appears that approximately
by guest on July 22, 2013http://www.pdiconnect.com/Downloaded from
half the non-married patients in the PD group in our study are single and most of them are living with rela- tives and are relatively young. Therefore, we think this is more likely the nature of the population.
The result of longer traffic time in the PD group seems to be similar to that reported in the literature, yet the reasons behind it may be dissimilar. In Taiwan, there are 459 clinics providing HD, while only 64 clinics among them can provide PD as well. Thus, the fact that HD pa- tients spend less time traveling to the clinic is due to the wider distribution of HD clinics. To give PD patients ac- cess that is more convenient and provide greater choice, we recommend that the government should map out guidance to increase the number of PD clinics.
The scale of patient receptivity was developed to help in the understanding of patient preference of dialysis modality. Whether a treatment is acceptable depends on patient receptivity; for that reason, patients should take into account their preference when making their deci- sion. Analysis of the receptivity scale showed that pa- tients would prefer self-care but worry about choosing it. This indicates that patients need more competence capacity or friendly guidance.
That prevalent PD patients have a better cognition of dialysis may imply PD therapy is more technical for pa- tients and patients that selected PD are expected to have a better understanding of dialysis. Thus, to ensure that patients understand well a dialysis modality is the first course when they face selection. Analysis of the cogni- tion scale indicated that PD patients have relatively poor cognition of “possible complications” and “contra- indications to dialysis,” while HD patients had generally poor cognition of all items. In summary, cognition of dialysis in the PD group (24.2 ± 5.8) was better than in the HD group (17.2 ± 6.5). Receptivity to dialysis in the PD group (32.8 ± 4.1) was also stronger than in the HD group (25.3 ± 4.9). Furthermore, similar to other stud- ies (17), for ESRD patients that received emergent di- alysis at the start, the odds of treatment by PD were much lower. Figure 1 shows that the proportions of patients that received emergent dialysis in the HD group were apparently higher than in the PD group, on average.
Hence, it is important to reduce the possibility of emer- gent dialysis. We therefore strongly recommend that CKD patients follow the standard process to obtain more ex- haustive information, consultation, and early referral.
Although all patients recruited in the sample had no contraindications, 149 patients reported that their doctor’s suggestion is an important factor that influenced their decision; the other 51 patients thought their doc- tors determined the dialysis modality. In fact, in our ex- perience, doctors usually respect the patient’s decision
except for clinical considerations, such as contra- indications. Nevertheless, this indicates that doctors play a key role in the selection process. As mentioned above, clinical evaluations are usually thought to be professional and one might follow their doctor’s advice. Hence, based on the results in this research, we suggest healthcare pro- viders, in addition to providing professional advice on clinical evaluations, remind patients to take into account nonclinical factors such as family support and patient receptivity. Moreover, patients should be prompted again and again to understand well dialysis modalities.
LIMITATIONS
Due to the fact that patients in the study had been on dialysis for up to 7 years, some measures were likely to be biased, especially patient cognition of and receptiv- ity to dialysis, because they are going to be better in the PD group after significant lengths of time of dialysis. We tried to explore associated factors based on 88 patients that received dialysis during the past 2 years. Most re- sults were similar to those we proposed based on the whole sample. Nonetheless, this is a preliminary study with several limitations and needs to be repeated in an incident group of patients.
While PD patients were interviewed in an unused clinic, HD patients were interviewed in the HD unit. Po- tential bias due to patients being interviewed in a pub- lic place may have arisen.
DISCLOSURES
The authors do not have any conflicts of interest to declare.
ACKNOWLEDGMENTS
This work was supported in part by the Changhua Christian Hospital, grant no. 2008-CCH-IRP-35.
The authors appreciate the three anonymous reviewers and the editor for their helpful comments that greatly improved the manuscript. We also thank the patients for their partici- pation and the nursing staff, Li- Fang Lai, Pei-Chuang Wu, Yuh- Feng Wu, and Chiung-Chiung Chang, for their assistance in recruitment of patients. We also thank Asia University for as- sistance in English editing.
REFERENCES
1. US Renal Data System. USRDS 2008 Annual Data Report.
Available at http://www.usrds.org/2008/view/esrd_
12.asp. Accessed 7 May 2009.
2. Bureau of National Health Insurance. A Public Document
by guest on July 22, 2013http://www.pdiconnect.com/Downloaded from
Associated with Reimbursement in Dialysis Patients [in Chinese]. Available at http://www.nhinb.gov.tw/upfiles/
adupload/dwn1289478037.pdf. Accessed 8 May 2009.
3. National Kidney Foundation R.O.C. Demography of Dialysis Patients in Taiwan. Available at http://www.kidney.org.tw/
index.html. Accessed 7 May 2009.
4. Jung B, Blake GP, Mehta RL, Mendelssohn DC. Attitudes of Canadian nephrologists toward dialysis modality selec- tion. Perit Dial Int 1999; 19:263–8.
5. Jassal SV, Krishna G, Mallick NP, Mendelssohn DC. Atti- tudes of British Isles nephrologists towards dialysis mo- dality selection: a questionnaire study. Nephrol Dial Transplant 2002; 17:474–7.
6. Mendelssohn DC, Mullaney SR, Jung B, Blake PG, Mehta RL. What do American nephrologists think about dialysis modality selection? Am J Kidney Dis 2001; 37:22–9.
7. Troidle L, Kliger A, Finkelstein F. Barriers to utilization of chronic peritoneal dialysis in Network #1, New England.
Perit Dial Int 2006; 26:452–7.
8. Bouvier N, Durand PY, Testa A, Albert C, Planquois V, Ryckelynck JP, et al. Regional discrepancies in peritoneal dialysis utilization in France: the role of the nephrologist’s opinion about peritoneal dialysis. Nephrol Dial Transplant 2009; 24:1293–7.
9. Shiao CC, Huang JW, Chien KL, Chuang HF, Chen YM, Wu KD. Early initiation of dialysis and late implantation of catheters adversely affect outcomes of patients on chronic peritoneal dialysis. Perit Dial Int 2008; 28:73–81.
10. Bureau of Health Promotion. 2003 Survey of Health and
Living Status of the Middle Aged and Elderly in Taiwan Survey Report [in Chinese]. Taiwan: Bureau of Health Pro- motion, Department of Health; 2006.
11. Huang CC, Cheng KF, Wu HDI. Survival analysis: compar- ing peritoneal dialysis and hemodialysis in Taiwan. Perit Dial Int 2008; 28(Suppl 3):S15–20.
12. Johnson DW, Dent H, Hawley CM, McDonald SP, Rosman JB, Brown FG, et al. Associations of dialysis modality and infectious mortality in incident dialysis patients in Aus- tralia and New Zealand. Am J Kidney Dis 2009; 53:290–7.
13. Kutner NG, Zhang R, Brogan D. Race, gender, and inci- dent dialysis patients’ reported health status and quality of life. J Am Soc Nephrol 2005; 16:1440–8.
14. Wuerth DB, Finkelstein SH, Schwetz O, Carey H, Kliger AS, Finkelstein FO. Patients’ descriptions of specific factors leading to modality selection of chronic peritoneal dialy- sis or hemodialysis. Perit Dial Int 2002; 22:184–90.
15. Little J, Irwin CA, Marshall T, Rayner H, Smith S. Predict- ing a patient’s choice of dialysis modality: experience in a United Kingdom renal department. Am J Kidney Dis 2001;
37:981–6.
16. Stack AG. Determinants of modality selection among in- cident US dialysis patients: results from a national study.
J Am Soc Nephrol 2002; 13:1279–87.
17. Mircescu G, Garneata L, Florea L, Cepoi V, Capsa D, Covic M, et al. The success story of peritoneal dialysis in Roma- nia: analysis of differences in mortality by dialysis mo- dality and influence of risk factors in a national cohort.
Perit Dial Int 2006; 26:266–75.
by guest on July 22, 2013http://www.pdiconnect.com/Downloaded from