Rhambdomyolysis induced by Hypothyroidism in A Patient with Hypopharyngeal Cancer:
A Case Report and Review of the Literature
Hao-Wen Lin
Division of Endocrinology and Metabolism, Department of Internal Medicine, National Taiwan University Hospital, Yun-Lin branch
Abstract
Though neuromuscular involvement is common in hypothyroid patients, rhambdomyolysis is only seen in case reports and usually with precipitating factors such as strenuous exercise or statin. Here we reported a rare case of rhambdomyolysis induced by post treatment hypothyroidism in a patient with hypopharyngeal cancer. A 41 year-old male with left oral cancer and left hypopharyngeal cancer suffered from myagia about one year after he underwent total laryngopharyngectomy and concurrent radiochemotherapy. There was no major trauma, no local necrosis and he did not take medications which may induce rhambdomyolysis. Recent magnetic resonance imaging revealed no evidence of local recurrence. Lab data revealed high creatine phosphokinase (CPK) of 13034 IU/L (38-160 IU/L), hypocalcemia with calcium of 7.1mg/dl (8.3-10.5mg/dl) and deteriorated renal function. Hydration and urinary alkalization were given. Further investigation revealed overt hypothyroidism and hypoparathyroidism. The free thyroxin was <0.4 ng/dL (0.7-1.48ng/dL) and the thyrotropin was 171µIU/mL (0.35-1.94µIU/mL). The thyroid peroxidase antibody was 0.4 IU/mL (0-5.61 IU/
mL). After supplement of levothyroxin and calcium carbonate, the patient achieved euthyroid, his myalgia improved, the CPK level decreased to normal limit and the creatinine decreased to baseline. Hypothyroidism should be kept in mind and treat properly with patients suffering from unexplained rhambdomyolysis. (J Intern Med Taiwan 2013; 24: 418-423)
Key Words: Rhambdomyolysis, Hypothyroidism, Hypopharyngeal cancer
Introduction
Hypothyroidism stands a rare cause of rhambdomyolysis1. Though muscle involvement is common in hypothyroid patients2-5, rhambdomyol- ysis caused by hypothyroidism is rare, seen in case reports, and usually with a precipitating factor6-16. Here we reported a rare case of rhambdomyolysis
induced by post treatment hypothyroidism in a patient with hypopharyngeal cancer.
Case Presentation
We reported a 41-year-old male who suffered from myalgia of shoulder and legs for months. He had history of left oral cancer and left hypopharyngeal cancer. The initial presentation of left oral squamous
Reprint requests and correspondence:Dr. Hao-Wen Lin
Address:Division of Endocrinology and Metabolism, Department of Internal Medicine, National Taiwan University Hospital, Yun-Lin branch, No.579, Sec. 2, Yunlin Rd., Douliu City, Yunlin County 640, Taiwan
cell carcinoma was intermittent sorethroat in 2010.
He underwent wide excision of tumor and left selec- tive neck lymph node dissection on 2010/03/16. The pathological staging was pT2N0M0, stage II.
During follow up, left hypopharyngeal tumor was noted. Neck magnetic resonance imaging (MRI) on 2010/08/17 revealed an irregular enhancing lesion about 1.8cm at the left tongue base and oropharynx, suspected recurrent oropharyngeal tumor and an irregular mass involving the left pyriform sinus and bilateral posterior hypopharyngeal wall with greatest dimension about 3.9 cm, suspected hypo- pharyngeal cancer. Biopsy of hypopharyngeal tumor revealed squamous cell carcinoma. The staging was cT4aN0M0, stage IVA.
Due to direct tumor invasion of thyroid carti- lage, he underwent total laryngopharyngectomy, right selective neck dissection level II-IV, left modi- fied radical neck dissection type I and tracheostmy on 2010/9/8
He underwent concurrent chemoradiotherapy with weekly cisplatin from 2010/10 to 2010/12.
Radiotherapy consisted of 66Gy in 33 fractions at 2Gy per fraction was delivered to hypopharyngeal tumor bed and bilateral upper neck, 60Gy was deliv- ered to bilateral lower neck, and 54Gy was delivered to bilateral supraclavicular fossa.
He had follow up at our oncology and otolar- yngology clinic. Neck MRI on 2011/8/23 revealed no evidence of local recurrence.
However, he suffered from myalgia over bilateral shoulders and legs since 2011/9. Lab data revealed high creatine phosphokinase (CPK) of 11341 IU/l (38-160 IU/l) and elevated lactate dehy- drogenase (LDH) of 1968 IU/L (260-450 IU/L) on 2011/10/6. Admission was suggested however he refused. Oral sodium bicarbonate and hydration were given. Followed lab data showed persistent elevated CPK and abnormal renal function compared to his baseline creatinine 1.2mg/dl (Table 1.) He was admitted on 2011/10/14 for rhambdomyolysis.
Among admission, his consciousness was clear with the Glasgow coma scale E4VTM6. His body weight was 70.2 kg and he was 176 cm in height. The blood temperature was 36.2°C, the pulse rate was 60 beats per minute, and the respiratory rate was 18/min. His blood pressure was 108/75 mmHg. The neck was supple with tracheotomy tube. The chest expanded symmetrically and the breath sounds were clear. The heartbeats were regular without audible murmur. His abdomen was soft and flat without tenderness and the bowel sounds were normoac- tive. The extremities were freely movable without pitting edema. There was no obvious local necrosis at otolaryngology field.
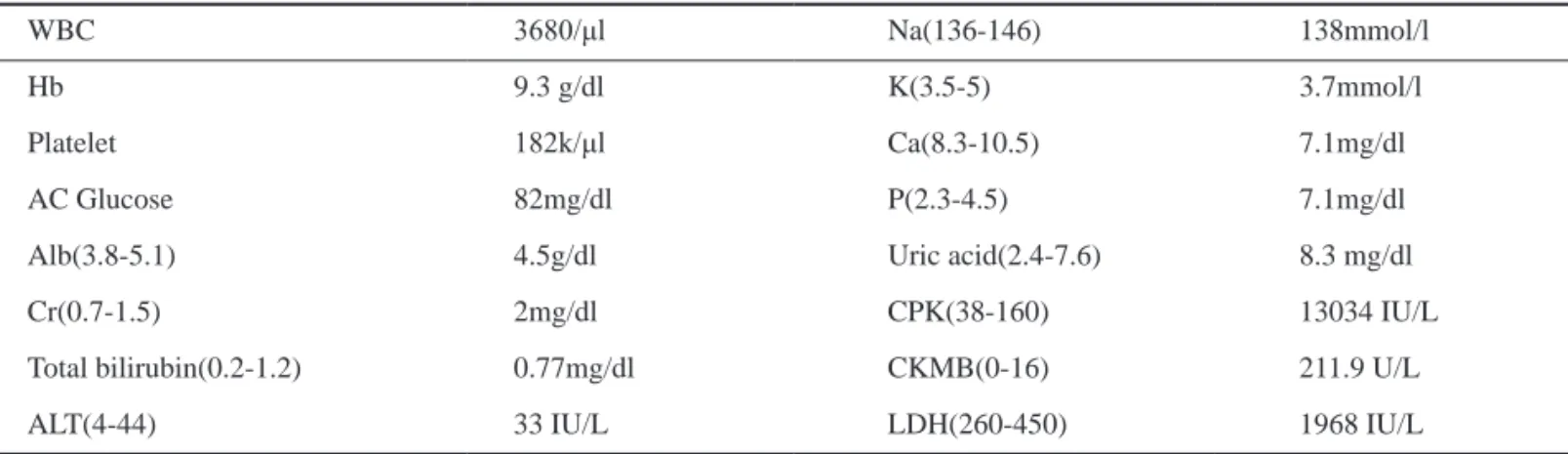
Laboratory data was listed in Table 1. Hypo- calcemia, hyperphosphatemia and elevation of uric acid were noted. The urinary analysis revaled pH 6.0, RBC 0-2/HPF, and negative occult blood. The CPK and Creatine Phosphokinase-MB (CK-MB)
Table 1. Lab data on 2011/10/14
WBC 3680/μl Na(136-146) 138mmol/l
Hb 9.3 g/dl K(3.5-5) 3.7mmol/l
Platelet 182k/μl Ca(8.3-10.5) 7.1mg/dl
AC Glucose 82mg/dl P(2.3-4.5) 7.1mg/dl
Alb(3.8-5.1) 4.5g/dl Uric acid(2.4-7.6) 8.3 mg/dl
Cr(0.7-1.5) 2mg/dl CPK(38-160) 13034 IU/L
Total bilirubin(0.2-1.2) 0.77mg/dl CKMB(0-16) 211.9 U/L
ALT(4-44) 33 IU/L LDH(260-450) 1968 IU/L
both elevated. Test of urine myoglobin level was unable to be performed at our hospital.
Hydration and urinary alkalization were given.
However, the CPK decreased suboptimally. Further survey for rhambdomyolysis was performed. There was no evidence of trauma and local compression.
There was no obvious local necrosis at otolaryn- gology field. Reviewing back his history, he did not take alcohol, medications such as statin or colchi- cine that could cause rhambdomyolysis. There was no evidence of infection. Blood culture was done but the result was negative and the C-reactive protein was not elevated.
Metabolic factors were surveyed and revealed hypothyroidism. On 2011/10/24, the free thyroxin (free T4) was <0.4 ng/dL (0.7-1.48ng/dL) and the thyrotropin (TSH) was 171μIU/mL (0.35-1.94μIU/
mL). The thyroid peroxidase antibody (Anti-TPO) was 0.4 IU/mL (0-5.61 IU/mL). Lab data also revealed hypoparathyroidism with intact para- thyroid hormone(iPTH) <3 pg/mL (12-72pg/mL).
Levothyroxin was applied and titrated to 100mcg per day gradually. Intravenous and oral calcium supplement were applied for severe hypocalcemia.
The CPK level decreased gradually to 3688 IU/L on 2011/11/03 and serum calcium level raised to 9.8mg/dl under calcium carbonate 3g per day. His myalgia improved gradually. Hydration and urine alkalization were tapered gradually and he was discharged with oral calcium carbonate and levo- thyroxin. Euthyroid status achieved under levo- thyroxin 150mcg per day with free T4 1.29ng/dL, TSH 0.659 uIU/mL on 2012/01/18. The CPK level decreased gradually while he achieved euthyroid status (Table 2).
Discussion
Hypothyroidism induced rhambdomyolysis Rhambdomyolysis may be induced by trauma, exertion, muscle hypoxia, genetic defects, infec- tions, body temperature changes, metabolic and
electrolyte disorders, drug and toxins, or idiopathic causes1. Common nontraumatic causes include exog- enous agents toxic to muscles, especially alcohol, illicit drugs and lipid lowering agents1. Hypothy- roidism stands a rare cause of rhambdomyolysis.
In patients with hypothyroidism, muscle involvement is common. Duyff RF et al reported that 79% of hypothyroid patients had neuromus- cular complaints such as weakness, cramping, myalgia, even carpal tunnel syndrome2. Elevation of CPK is also common in hypothyroid patients2-4. The serum CPK level did not correlate with weakness2. Hekimsoy Z et al. reported a positive correlation between CPK and TSH and a negative correlation between CPK and free T3 and between CPK and free T44. Thus, hypothyroidism should be kept in mind in patients with an unexplained increase of serum CPK.
CPK elevations in hypothyroid patients were usually lower than ten times up the refer- ence level5-6. And despite common CPK elevation, rhambdomyolysis caused by hypothyroidism is rare, seen in case reports, and usually with a precipitating factor like intensive exercise, using drug such as lipid lowering agents, trauma, underlying infection, and toxins (Table 3,6-16). Our patients represents a rare case of hypothyroidism induced rhambdomyol- ysis. Hypocalcemia may be a result of rhambdomy- olysis however hypocalcemia itself might proceed rhambdomyolysis1. In our patient, the low iPTH
Table 2. Change of thyroid function Ca, and CPK level Ca
mg/dl
CPK IU/L
FT4 ng/dL
TSH μIU/mL
2011/10/14 13034 <4 171.2
2011/10/15 7.1 9835 2011/10/27 8.9 4936 2011/10/31 8.3 3946 2011/11/03 9.8 3688
2011/11/30 7.6 381 1.15 15.68
2012/01/18 8.6 127 1.29 0.659
thyroid function tests should be repeated at 6–12 month intervals after radiotherapy20.
Our patient suffered from symptoms of rhamb- domyolysis about 9 months after completion of radial therapy. Early screen of thyroid function test and early supplement might help this patient from his illness.
Mechanism of radiotherapy induced hypothy- roidism includes direct microvascular and macro- vascular damage in and around thyroid tissue, direct damage to follicular epithelium, and radiation- induced autoimmune thyroiditis18. It may also be a result of radiation-induced damage to the hypo- thalamic-pituitary axis, which results in central hypothyroidism18.
Though the actuarial risk of developing hypo- thyroidism is significantly higher when the thyroid gland is included in the target radiation volume, it level suggested his hypocalcemia is a result of hypo-
parathyroidism. Treatment with levothyroxin and calcium supplement lead to a successful recovery of renal function and symptoms.
Hypothyroidism after treatment of head and neck cancer
Hypothyroidism is common in patients treated for head and neck malignancies. The incidence varies from 23-53%17-19. Mostly it has been observed after radiation, however sometimes after surgery and combined-modality therapies18. Onset of hypothy- roidism varies from 4 weeks to late as 5 or 10 years after completion of therapy18. Studies suggested thyroid function should be tested on a regular basis following radial therapy to the low-neck region17-19. The National Comprehensive Cancer Network (NCCN) clinical practice guidelines recommended Table 3. Hypothyroidism induced rhambdomyolysis*
Author Nation Age Sex Etiology of hypothyroidism
CPK (IU/L)
TSH
(μIU/mL) Precipitating factor
Renal function impairment Nobuo S, 1993 Japan 61 F Hashimoto thyroiditis 8437 110.4 Strenuous
exercise
Y
Barahona MJ, 2002 Spain 49 M Hashimoto thyroiditis 9332 147.7 No N
Kisakol G, 2003 Turkey 19 M Hashimoto thyroiditis 10210 >75 No N
Mustafa A, 2005 Turkey 31 M Hashimoto thyroiditis 2291 >100 No Y
Chowta MuktaN, 2008
India 39 M not mentioned 972 >100 Alcohol Y
Kus HT, 2010 Taiwan 75 F s/p I131 and subtotal thyroidectomy
6020 142.03 Renal function impairment
Y(CKD)
Nikolaidou C, 2010 Greece 41 F Hashimoto thyroiditis 3239U/L 75 No Y
Moeller RF, 2011 USA 15 F Hashimoto thyroiditis 34724 77.2 Strenuous exercise
N
Hurtado1 JJD, 2011 Guatemala 5 M Unknown 4615 299 Cardiac
temponate
N
Muir P, 2012 New Zealand
22 M Hashimoto thyroiditis >25000 >100 Adrenal insufficiency Hyponatremia
Y
Ying C, 2013 (5 patients)
China 37
to 62
4M 1F
1: Hashimoto thyroiditis 1: amiodarone related 3: unknown
1297 to 3573
87.25 to
>100
Not mentioned Y
*Reference 6-16.
was not possible to define a clear dose–volume effect and threshold doses are not well elucidated18-19. Studies reported increased probability of developing primary hypothyroidism when the mean radiology dose on thyroid gland increased beyond 45Gy to 65Gy18. The dose delivered to our patient (66Gy) might increase the probability of hypothyroidism.
Conclusion
Hypothyroidism should be kept in mind and treat properly with patients suffering from unex- plained rhambdomyolysis. And thyroid function should be checked periodically in patients with laryngeal or hypolaryngeal cancer whom underwent total laryngectomy and radiotherapy.
References
1. Xavier B, Esteban P, Josep MG. Rhabdomyolysis and Acute Kidney Injury. N Engl J Med 2009; 361: 62-72.
2. Duyff RF, Van den Bosch J, Laman DM, et al. Neuromus- cular findings in thyroid dysfunction: a prospective clinical and electrodiagnostic study. J Neurol Neurosurg Psychiatry 2000; 68: 750.
3. Madariaga MG. Polymyositis-like syndrome in hypothy- roidism: review of cases reported over the past twenty-five years. Thyroid 2002; 12: 331.
4. Hekimsoy Z, Oktem IK. Serum creatine kinase levels in overt and subclinical hypothyroidism. Endocr Res 2005; 31: 171.
5. Doran GR. Serum enzyme disturbances in thyrotoxicosis and myxoedema. J R Soc Med 1978; 71: 189.
6. Nikolaidou C, Gouridou E, Ilonidis G, et al. Acute renal dysfunction in a patient presenting with rhabdomyolysis due to Hypothyroidism attributed to Hashimoto’s Disease.
Hippokratia 2010; 14: 281-83.
7. Nobuo S, Michiko Y, Makoto M, et al. Rhabdomyolysis and Acute Renal Failure in a Patient with Hypothyroidism.
Internal Medicine 1993; 32: 269-71.
8. Barahona MJ, Mauri A, Sucunza N, et al. Hypothyroidism as a cause of rhabdomyolysis. Endocr J 2002; 49: 621-3.
9. Kisakol G, Tunc R, Kaya A. Rhabdomyolysis in a patient with hypothyroidism. Endocr J 2003; 50: 221-3.
10. Mustafa A, Murat D, Mevlut C. Rhabdomyolysis due to hypothyroidism. Nephrol Dial Transplant 2005; 20: 847-55.
11. Chowta MuktaN, Chowta NithyanandaK. Hypothyroidism- associated rhabdomyolysis. Indian J Med Sci 2008; 62: 12:
496-7.
12. Kuo HT, Jeng CY. Overt hypothyroidism with rhabdomy- olysis and myopathy: a case report. Chin Med J 2010; 123:
633-7.
13. Moeller RF, Zecavati N, Sherafat-Kazemzadeh R, et al.
Adolescent with Rhabdomyolysis due to Undiagnosed Hypo- thyroidism. Case Rep Pediatr 2011; 2011: 670-3.
14. Hurtado JJD, Guevara W, Ramos E et al: Hypothyroidism in a five-year-old boy with rhabdomyolysis and recent history of cardiac tamponade: a case report. J Med Case Rep 2011;
5: 515.
15. Muir P, Choe MS, Croxson MS. Rapid Development of Anterotibial Compartment Syndrome and Rhabdomyolysis in a Patient with Primary Hypothyroidism and Adrenal Insuf- ficiency. Thyroid 2012; 22: 651-3.
16. Ying C, Lin T. Rare Acute Kidney Injury Secondary to Hypo- thyroidism-Induced Rhabdomyolysis. Yonsei Med J 2013;
54: 172-6.
17. Garcia-Serra A, Amdur RJ, Morris CG, et al. Thyroid func- tion should be monitored following radiotherapy to the low neck. Am J Clin Oncol 2005; 28: 255-8.
18. Miller MC, Agrawal A. Hypothyroidism in postradiation head and neck cancer patients: incidence, complications, and management. Curr Opin Otolaryngol Head Neck Surg 2009;
17: 111-5.
19. Boomsma MJ, Bijl HP, Langendijk JA. Radiation-induced hypothyroidism in head and neck cancer patients: a system- atic review. Radiother Oncol 2011; 99: 1-5.
20. Pfister DG, Ang KK, Brizel DM, et al. National Comprehen- sive Cancer Network (NCCN) Clinical Practice Guidelines in Oncology – Head and Neck Cancers. J Natl Compr Canc Netw 2011; 9: 596-650.
下咽癌治療後甲狀腺低下引起之橫紋肌溶解症
林皓雯
台大醫院雲林分院內科部 內分泌新陳代謝科
摘 要
雖然甲狀腺低下的病人常有神經肌肉的症狀,甲狀腺低下造成的橫紋肌溶解症卻很少 見,僅見於案例報告,並且通常合併有其他的加重因子:如劇烈運動或使用降血脂藥物等。
本案例報告為一下咽癌病人在接受手術和放射線治療後產生甲狀腺低下並造成橫紋肌溶解 症。此為一位 41 歲男性病患,本身有左側口腔癌和左側下咽癌。在接受全喉切除術、化療及 放射線治療後約一年開始有肌肉疼痛的症狀。病人沒有受過嚴重肢體創傷、口腔咽喉處沒有 局部壞死、也沒有服用可能造成橫紋肌溶解症的藥物。最近一次的核磁共振顯示腫瘤沒有局 部復發的情形。實驗室檢查顯示肌酸磷酸激酶 (CPK) 升高至 13034 IU/L (38-160 IU/L),同時有 低血鈣 (calcium 7.1mg/dl) (8.3-10.5mg/dl) 和肌肝酸上升。進一步的檢查顯示甲狀腺低下及副甲 狀腺低下,抗甲狀腺過氧化抗體為 0.4 IU/mL (0-5.61 IU/mL)。補充甲狀腺素和鈣後,病人甲 狀腺機能回復正常,肌肉疼痛改善,CPK 值和肌肝酸亦回復至基礎值。若病人出現原因不明 的橫紋肌溶解症,應想到是否有甲狀腺低下,仔細診斷並適當治療。