中 國 醫 藥 大 學
臨床醫學研究所
碩士學位論文
大白鼠血管週邊脂肪組識對血管影響之新進展
Novel vascular actions of rat aortic
perivascular adipose tissue
指 導 教 授 : 關超然 教 授
共同指導教授: 謝文聰 副教授
中文摘要
大白鼠血管週邊脂肪組識對血管影響之新進展
肥胖乃長久以來影響身體健康的一個問題,肥胖已被證實與很多疾病有關,諸 如高血壓、糖尿病、冠心病、心衰竭、腦中風等。今天,由於社會的進步,飲 食之多元化,使肥胖在全球之比率日益俱增。基於肥胖對身體之不良影響科學 界已著手研究脂肪組識細胞,他們發現脂肪細胞其實是有多功能性的,因其內 之 Adiponnectin 可分泌脂肪激酶 Adipokines,而引發出自體分泌,旁分泌及內 分泌等種種作用。 血管是控制血壓的一重要角色,血管主要包含有三層,即內層的內皮細胞層、 中層的平滑肌層,以及外層的外膜層,而外膜層又往往被二到三條的週邊血管 脂肪組織所圍繞著,在最近 10 年中,學者們紛紛提出,此等週邊血管脂肪組 織,是會釋出一些未知之因子,來調節血管功能,因而與血壓有關。在大多數 之研究結果認為,此等因子是有增加血管之舒張能力,而少數學者則認為有增 加血管之收縮能力,此因子暫定為 是一種血管衍生舒張因子, (Adiposederived relaxing factor ADRF) 我們利用大白鼠之動脈及其週邊所黏附的脂肪組 織在不同的情況下,諸如有脂肪黏附的主動脈血管環,去脂肪組織之血管環, 及去脂肪組織而附加脂肪組識溶液之血管環,與不同的試劑,如苯腎上腺素 ( Phenylnephrine PE ) 氯化鉀 (Potassium Chloride KCl ) Carbocheol ( CCh )及血管
收縮素Angiotensin Ⅱ Ang. Ⅱ ) 進行反應,結果顯示,不論在有黏附脂肪組織的
血管環,或在脂肪組織而附加脂肪組織溶液之血管環,在與 PE 及 KCl 反應
下,皆有增加血管收縮之作用,又當我們用 NG-Nito- arginine methyl ester ( L-NAME ) 來抑制內皮細胞釋放 Nitie Oxide ( NO ) 後,此等收縮現象依然存在。 當洗去收縮劑 ( PE 及 KCl )後,那些有黏附脂肪組織的血管環,對血管舒張之 速度,又比那些去脂肪組織的血管環有明顯緩慢性作用。因此,我們暫定此等 脂肪組織,會釋放一種因子,命名為『 脂肪細胞衍生因子 』 ( Adipose derived Factor ADF ) 此等因子是有提高血管收縮之能力的。
前之血管環,其有良好之血管舒張作用。但在附加脂肪組織溶液後,則有明顯 之減低舒張作用,而此一作用反應,在洗去脂肪組織溶液後,又可回復之前之 血管舒張作用,在與血管收縮素 Ang. Ⅱ 作用時,發現在去脂肪組織之血管環 中,那些有附加脂肪組織溶液的血管環,對血管收縮的能力,遠較那些沒有附 加脂肪組織溶液的血管環為高,此外,當脂肪溶液加熱到沸點時,則會喪失其 血管收縮的作用,故可假想此等脂肪組織,為一種蛋白質類之結構物,加熱後 會被去自然 (De-nature) 而被破壞。 結論,經過多次實驗所得之結果,我們發現,週邊血管脂肪組織,確實是有增 加血管收縮之作用,雖然此些發現與之前之文獻報告大有出入,但在現實生活 中,肥胖人士容易產生高血壓及血管之病變,則又達到一合理共識之據點。
Abstract
A novel vascular action of perivascular adipose tissue
Obesity has been a long term problem in health. It was proved to have a high relationship to many systemic diseases, such as hypertension, diabetes mellitus, coronary vascular disease, heart failure and stroke. Large increase in the prevalence of obesity over the world have resulted largely from alterations in environmental factors that increase energy intake and reduce physical activity sedentary to lifestyle and work activities.
To learn the pathological effect of obesity to the body, scientists studied adipose tissue cells. They found that the adipose cells have multiple functions which release adipokines to exert autocrine, paracrine and endocrine effects. Blood vessel plays an important role in blood pressure control . They consist of three main layers: The inner endothelial layer, the media smooth muscle layer and the outer adventitia layer which is also surrounded by fat tissue called perivascular adipose (fat) tissues (PVAT). In recent years, investigators have been proposed that the perivascular adipose tissue could affect vascular reactivity via releasing some unknown factors and can thus provide the regulation of blood pressure. Most of the previous studies found that the perivascular adipose tissue exerts a vessel relaxation effect and a diffusible adipose derived relaxation factor (ADRF) was thus proposed although not yet identified.. We have studied the effects of PVAT on the rat thoracic aortic artery under different conditions, such in fat - intact aortic rings, fat - denuded aortic rings, fat denude aortic rings following transfer of solution incubated with fat (fat solution) or boiled fat solution. Aorta were stimulated with phenylnephrine (PE), potassium chloride (KCl), angiotensin II (Ang II), and the carbachol (CCh). In contrast to the previously study, we found that either the in situ aortic fat or the solution incubated with isolated fat can increase contractile response in the form of enhanced sensitivity to PE and KCl. This respondes persist even after the inhibition of the endothelium nitric oxide (NO) production with NG-nitro-L arginine methyl ester (L-NAME). Upon wash out of PE and KCl, a slower relaxation rate was found in the aortic rings with intact perivascular adipose tissues. For the endothelium dependent relaxation to carbachol (CCh), it was
contractile response in the upon transfer of fat pre-incubated solution. When the fat solution has been boiled, no enhance contractile response was he notion that obese people with high visceral fat content has a higher risk in developing high blood pressure and vascular complications characteristic of metabolic syndrome
Acknowledgements
I am grateful to Professor Chiu Yin Kwan for guiding me to the field of scientific research and helping me with basic medical knowledge.
I thank Associate Professor Wen Tsong Hsieh for helping the materials’ preparation, technical skill and biological statistics.
I also thank all the technicians and staffs in the laboratory of Department of Pharmacology, who assist me in my whole experimental procedure and the use of equipments.
Dedicated to my parents
and family
Contents
Abstract
Chinese I English IIIAcknowledgements
VDedication VI
Contents
VIILists of figures
XList of abbreviations used
XIIChapter 1:
Preface
11. Study background
1-1 Vascular tissue and function 21-2 Adipose tissue and function 4
1-3 Diseases that relative with obesity 1-3-1 Metabolic syndrome 6
1-3-2 Coronary artery disease 8
1-3-3 Diabetes mellitus 10
1-3-4 Hypertension 12
1-4 Physiology of blood vessel contraction and relaxation 14
1-4-1 Factors controlling vascular contraction 1-4-1-1 Calcium signal 17
1-4-1-2 α1 adrenergic receptors 19
1-4-1-3 Angiotensin 20
1-4-1-4 Endothelin 23 1-4-2 Factors controlling vascular relaxation
1-4-2-3 Potassium channels
1. ATP sensitive potassium channels 30
2. Voltage depend potassium channels 31
3. Calcium sensitive potassium channels 31
1-4-2-4: The effect of PVAT to the blood vessels- 32
The previous literatures review
2. Aim of study and hypothesis
33Chapter 2:
Materials and Methods
2-1.Materials 34 2-2. Methods 36 2-3. Chemicals 39 2-4. Statistical analysis 39Chapter 3:
Results
3-1 Effects of perivascular adipose tissue (PVAT) on contractions to Phenylnephrine and potassium chloride 403-2 Effects of fat solution on aortic contraction to Phenylnephrine and Potassium chloride 45
3-3 Effects of different concentrations of fat solution on contractions to Phenylnephrine and potassium chloride 50
3-4 Effects of boiled fat solution on contractions to Phenylnephrine and potassium chloride 52
3-5 The role of endothelium-nitric oxide formation on the effect of fat solution on contraction to Phenylnephrine 53
Chapter 4
Discussion
63References
66List of Figures
Fig.1 Basic structure of blood vessel P 3 Fig.2 Adipose tissue as an endocrine organ P 5 Fig.3 Metabolic syndrome P 7 Fig.4 Formation of atheroma in coronary artery disease P 9 Fig.5 Pathological change in diabetes mellitus P11 Fig.6 Adipose tissue and hypertension P13 Fig.7 Calcium and smooth muscle contraction P16 Fig.8 Angiotensin II and its receptors P21 Fig.9 Angiotensin AT1 receptor and vessel constriction P22 Fig.10 Function of endothelin (ET1) receptors P24 Fig.11 Mechanism of smooth muscle contraction
and relaxation P26 Fig.12 Nitric oxide (NO) and smooth muscle relaxation P29 Fig.13 Rat thoracic aorta P35 Fig.14 Prepare and transfer of fat solution P37 Fig.15 Methods of transfer fat solution P38 Fig.16 Effect of fat intact (F+) and fat denuded (F-) aortic
rings on contraction of potassium chloride (KCl) P41 Fig.17 Contraction response curves of KCl in F+ and F-
aortic rings P42 Fig.18 Effect of F+ and F- aortic rings on contraction
of phenylnephrine (PE) P43 Fig.19 Contraction response curve of PE in F+ and F- aortic rings P44 Fig.20 Effect of transfer F solution on contraction of PE (tracing) P46 Fig.21 Effect of transfer F solution on contraction of PE (bar) P47 Fig.22 Effect of transfer F solution on contraction of KCl (tracing) P48 Fig.23 Effect of transfer F solution on contraction of KCl (bar) P49
Fig.26 Effect of boiled F solution on contraction of PE and KCl P52 Fig.27 Role of endothelium-nitric oxide (NO) formation on
effect of F solution on contraction of PE (tracing) P54 Fig.28 Role of endothelium-nitric oxide (NO) formation on
effect of F solution on contraction of PE (bar) P55 Fig.29 Effect of F solution on Carbachol (CCh) induce
aortic relaxation (tracing) P57 Fig.30 Effect of F solution on Carbachol (CCh) induce
aortic relaxation (bar) P58 Fig.31 Effect of transfer F solution on contraction of
angiotensin II P59 Fig.32 Effect of transfer F solution compare to Ringer’s
solution on contraction of angiotensin II P60 Fig.33 Vascular tachyphylaxis effect on repeat contraction
of angiotensin II P61
Fig.34 Effect of F solution on the resting tension of aortic rings P62
List of Abbreviations
ADF Adipose derived factor ADP Adenosine 5 diphophate
ADRF Adipose derived relaxing factor Ang.II Angiotensin II
AT1 Angiotensin II receptor 1 ATP Adenosine tri-phosphatase ATP Adenosine tri-phosphate BMI Body mass index
CaM Calcium calmodulin complex c-AMP Cyclic adenosine monophosphate CCh Carbachol
c-GMP Cyclic guanosine monophosphate CNG Cyclic nucleotide gated
DAG 1-2, Diacylglycerol DHPs 1, 4-dihydropyridines
EDCF Endothelial derived contractive factor EDRF Endothelial derived relaxing factor eNOS Endothelium nitric oxide synthase ERK Extracellular signal regulate kinase ET Endothelin
F - Fat tissue denuded F + Fat tissue intact F solution Fat solution FFA Free fatty acid
GPCR G protein coupled receptor GTP Guanosine triphosphate
iNOS Inducible nitric oxide synthase
L-NAME NG-nitro-L arginine methyl ester LTCC L-type calcium channel
MAPK Mitogen activate protein kinase MLC Myosin light chain
MLCK Myosin light chain kinase
NADPH Nicotinamide adenine dinucleotide phosphate NCX Sodium calcium exchange
nNOS Neuron nitric oxide synthase NO Nitric oxide
ONOO Peroxynitrite
PAI-1 Plasminogen active inhibitor-1 PDE1 Phosphodiasterase-1
PE Phenylnephrine
PIP2 Phosphatidyl inositol 4-5 bisphosphate PKC Protein kinase C
PLC Phospholipase C
PVAT Perivascular adipose tissue
RAS Renin angiotensin aldosterone system RyR Ryanodine receptor
SEM Standard error of the mean SOD Superoxide dismutase SR Sarcoplasmic reticulum TNF Tumor necrosis factor TTCC T-type calcium channel
VDCC Voltage depend calcium channel VSM Vascular smooth muscle
VSMC Vascular smooth muscle cell
Chapter 1
Preface
Obesity is defined as an excess of body fat accumulation with elevated body mass index (BMI). Men and women with a BMI of 25.0 to 29.9 Kg/m2 are considered over weight, and those with a BMI > 30 Kg/m2 are considered obese (1).
Obesity is a global epidemic as a result of confluent socioeconomic condition and high caloric food intake, not only in developed countries, but also reaching epidemic proportion in the developing countries.
Large epidemiological studies have established that there is a strong inverse relationship between BMI and mortality (2). The etiology of obesity is complex and still not well understood. It can involve in genetic, life style, environmental and psychological factors (3). Under the normal physiological condition, body fat is stored as energy depot (Calories) in adipocytes. A lean adult has about 35 billion adipocytes. Each adipocyte contains about 0.4 to 0.6 μg of triglycerides (4). The triglyceride storage within adipose tissue constitutes the body major energy reserve. The pool average of a man and a woman with normal weight has a 10-20% and 15-25% adipose tissue, respectively (5). When this stored energy lost balance due to excessive food intake or insufficient use of energy, the excessive calories are stored as fat in adipose fat tissue resulting in obesity. Obesity is a significant risk factor for many systemic diseases, direct or indirectly associated with an increased incidence and prevalence of heart disease, diabetes, hypertension, stroke, cardiac arrhythmia and dyslipidemia (6). All these diseases involve structural and /or functional changes in blood vessels.
Today, physicians and health care professionals are facing the challenge combating against in the complications and sequelae of obesity. The blood vessels of many visceral organs are surrounded by perivascular fat tissues, but the roles of these fat tissues other than its insolating and protecting effects are not clear. To find out whether the perivascular fat tissue has any physiological impact on the blood vessel
1. Background
1-1.Vascular tissues and functions
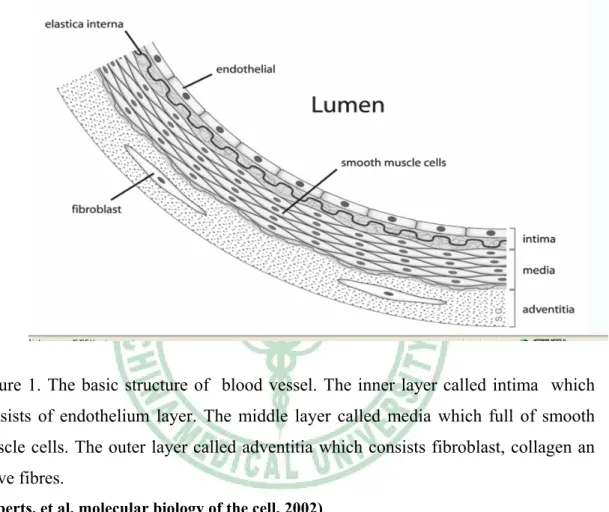
The basic constituents of the wall of blood vessels have 3 concentric layers, the intima, media and outer layers (figure 1). Beside these 3 layers, there are also tissue surrounding the outer vessel wall. For example, 2 to 3 strips of fat tissue are associated with rat aorta. In smaller arteries the entire vessel segments are surrounded by fat tissues.
The intima (endothelial layer) consists of a single layer of endothelial cells with minimal underlying sub-endothelial connective tissue. It is separated from the media by a dense elastic membrane called the internal elastic lamina. Functions of the endothelial layer are structural maintenance of vessel wall, homeostasis and normal circulatory function. As a semi-permeable membrane, endothelium controls the transfer of small and large molecules across the vascular wall. It also expresses adhesion molecule, cytokines and chemokines (7). These vasoactive molecules result either in vasodilatation or vasoconstriction functioning as relaxing factors, such as nitric oxide (NO) (8, 9) and contracting factors, such as endothelin (ET) (10).Under normal physiological condition, they exist in a balanced and co-ordinated manner. The media (smooth muscle layer) consists of concentric sheets of smooth muscle cells embedded in the frame work of connective tissue, such as collagen and elastin fibers It receives oxygen and nutrients by direct diffusion from the vessel lumen.(11) The primary function of smooth muscle layer is to maintain vascular tone and to regulate peripheral vascular resistance. They are two types of contraction, phasic and tonic depending on the nature of the stimuli. These contractile and elastic compoments can resist the pressure generated by the heart pump (12).
The outer (adventitia) layer, a very complex layer consisting of connective tissues, collagen fibers, nerve fibers and small vessels. The collagen fibers may blend into those of the adjacent tissue. The function of the adventitia involved stabilizing and anchoring the blood vessels (13). The fibroblasts derived from adventitia also possess the capacity of contracting and relaxing (14). They have recently been shown to be a rich source of reactive oxygen species thus limiting nitric oxide bioactivity (15). The
Figure 1. The basic structure of blood vessel. The inner layer called intima which consists of endothelium layer. The middle layer called media which full of smooth muscle cells. The outer layer called adventitia which consists fibroblast, collagen an nerve fibres.
1-2 Adipose tissue and function
Fat tissue (adipose tissue) is a loose connective tissue that contains many lipid filled cells called adipocytes. The formation of adipose tissue is controlled by the adipose gene. Adipocyte is derived from fibroblast-like precursor cells (pre-adipocytes) under appropriate stimulatory condition (17). Adipose tissue contains, leukocytes, macrophages, small blood vessels and pro-inflammatory cytokines and chemokines (18).Obesity is associated with enlarged fat cells and an increased number of macrophages in the adipose tissue surrounding individual adipocytes (19). Adipose tissue is commonly found beneath the skin, and is also found around the internal organs such as abdominal cavity, intestine and blood vessels. An increased mass of adipose tissue can occur by hyperplastic growth , which is an increase in number of adipocytes or by hypertrophic growth, an increase in size of adipocytes. Both increased number and size of adipose tissue can result in obesity (20)
The adipose tissue function as the major storage site for fat in the form of triglycerides. Approximately, 1 gram of fat can yield 9 Kilo.calories.(21) In mammals, adipose tissue is found in 2 different forms: The white adipose tissue and the brown adipose tissue, the latter found mainly in infants. White adipose tissue is distributed in multiple depots found both subcutaneously and internally. Approximately 60-85% of weight of white adipose tissue is lipid, it serves as heat insulation, mechanical cushion to protect organs from mechanical damage and energy source. With the discovery of leptin, white adipose tissues are recognized to secret several hormones. The function of adipokines involved lipid metabolism, insulin sensitivity, vascular function and blood pressure regulation (22). Brown adipose tissue which derives its color from rich vascularization and dense mitochondria is predominantly comprised of multilocular adipose cells. It stores nutrients in the form of triglycerides to generate heat in order to warm the body (23).
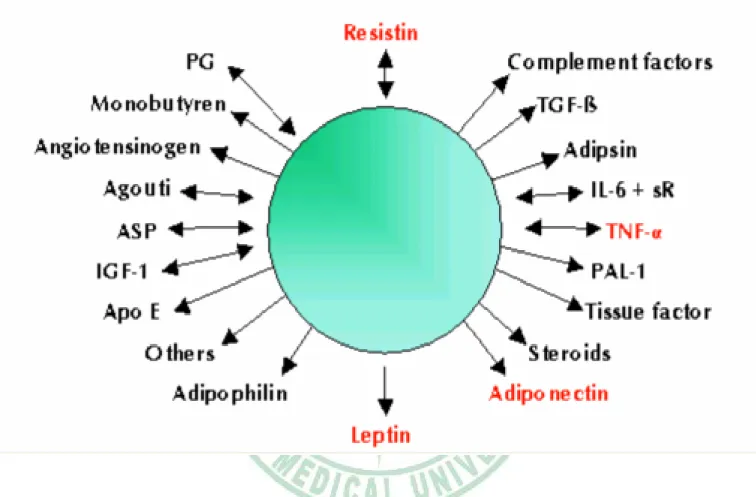
Adipose tissue also severs as an important endocrine organ (figure 2). for many secretory substance, such as adiponectin, leptin, resistin, tumor necrosis factors (TNF), plasminogen activate inhibitor (PAI-1), angiotensin (Ang), acylation-stimulating protein (ASP) and Interlukein-6 (IL-6), to name a few (24) (figure 2).
Figure 2
: Adipose tissue can secret more than 20 different kinds of hormones, which play many important physiological functions.(Gema, Frobeck, Mattew. 2001)
1-3. Diseases that are related to obesity
1-3-1: Metabolic syndrome:
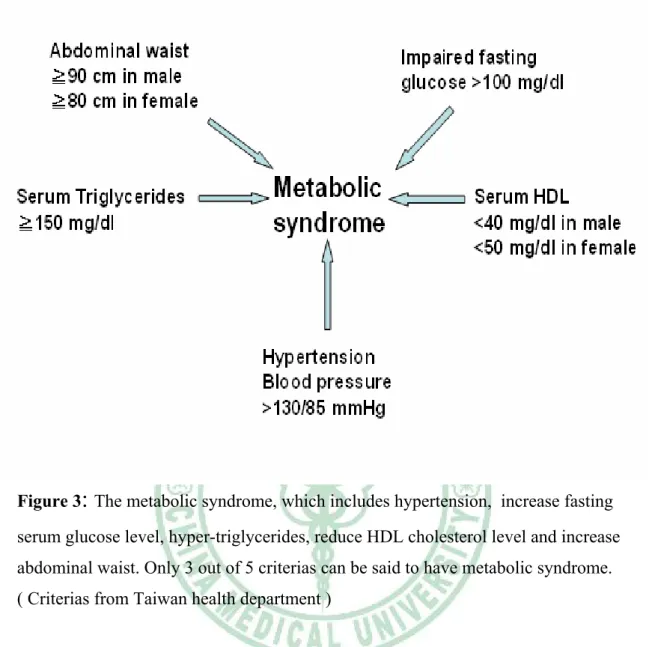
European investigators recognized that abdominal adiposity was related to greater risk of cardiovascular events. The key components of metabolic syndrome include central obesity, insulin resistance, high triglycerides, low high density lipoprotein (LDL) and hypertension (25) (figure 3). The body mass index (BMI) is equal to the weight in kilograms divided by the height in meters squared. It is defined that normal BMI: 18.5 to 25 Kg/m2. Overweight: 25 to 30 Kg/m2. Obesity: > 30 Kg/m2 (26). Adipose tissue is and active secretory organ that elaborates a variety molecule known as adiopkinase. This kinase including tumor necrosis factor (TNF), α-interleukin-6, leptin, resistins and adiponectin,(24) all that mediated many of the metabolic change in the metabolic syndrome. The TNF α - interleukin-6 plays as an inflammatory marker in skeletal muscle and liver. Leptin can reflect adipose tissue mass and body energy balance, the plasma leptin level was found to be predictive of cardiovascular events. Resistin as a hormone that links obesity to diabetes by increasing insulin resistance. Adiponectin has antiatherogenic properties, can maintains coronary flow reserve, inhibit monocyte adhesion to endothelial cells, reduce macrophages that transform to foam cells and prevent the episode of thrombus formation (27, 28). However, adiponectin, which is produced only by the white adipose tissue. This hormone is reduced in states of insulin resistance, such as obesity and type II diabetes. And thus, in metabolic syndrome, patient is easily to get coronary artery disease, stroke or others vascular disease due to the reduce formation of adiponectin (29) (figure 3).
Figure 3
:
The metabolic syndrome, which includes hypertension, increase fasting serum glucose level, hyper-triglycerides, reduce HDL cholesterol level and increase abdominal waist. Only 3 out of 5 criterias can be said to have metabolic syndrome. ( Criterias from Taiwan health department )1-3-2: Coronary artery disease
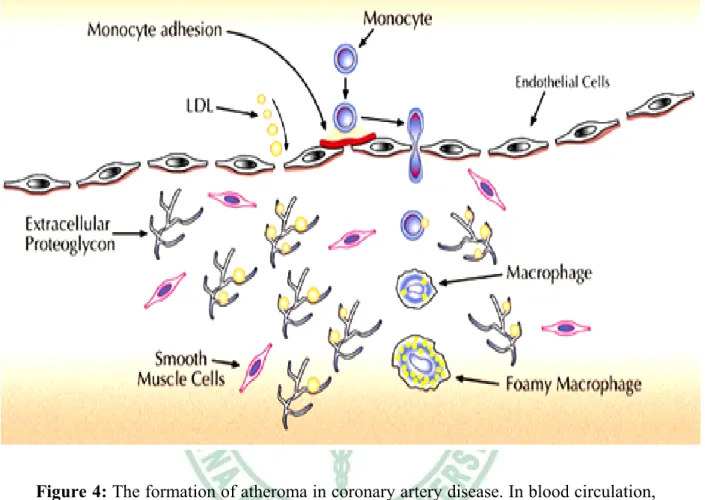
Coronary artery disease is due to chronic inflammatory response of the arterial wall initiated by injury to the endothelium, called atherosclerosis (30). Frequently also called cholesterol – dependent clogging of the arteries. In hyperlipidemia, particularly hypercholesterolemia, a high level of low density lipoprotein (LDL) may directly injure endothelial layer, and impair endothelial function through increase by reactive oxygen spieces accumulation –collectively, termed “oxidative stress” (31). In endothelial dysfunction, monocytes adhere to the endothelium and migrate into intima that differential into macrophage, at that it also increase permeability of leukocytes vascular cells adhesion molecule and lympocytes. All these substance migrate from smooth muscular layer to the endothelial layer and transform into macrophage. Marcophage then becomes activate, will engulf oxidative LDL form a foam cell (31). Accumulate of the foam cells then form a plaque When the blood pressure increases – resulting in increased shear stress to the blood vessels, the plaque ruptures, and further attracts a large amount of platelets and leukocytes which aggregate to the plaque and form a thrombus (atheroma) (32). When this thrombus enlarged, it will block the circulation of coronary blood vessel, which reduce the blood flow, form coronary artery disease. This process is demonstrated as shown in figure 4.
Figure 4: The formation of atheroma in coronary artery disease. In blood circulation,
when LDL is increase, monocytes then adhere into the endothelial layer. Then migrate into the media layer and derived into macrophages. Macrophages engulf LDLs and become the foam cells. Large amount of foam cells accumulate to form a plaque. When the plaque rupture, lots of platelets, leukocytes aggregate into the plaque to form an atheroma.
1-3-3: Diabetes mellitus
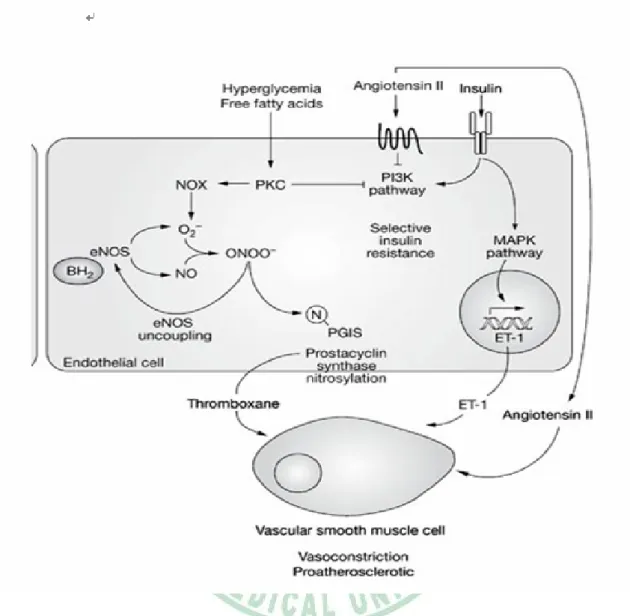
Adipose tissues not only store lipid fuel but also release free fatty acids (FFAs) and glycerol into the circulation via lipolysis. Adipose tissue lipolysis is regulated primarily by insulin inhibition and catecholamines stimulation (33). Obesity is associated with several abnormalities of adipose tissue lipolysis, most notably resulting in higher FFA concentrations and insulin resistance. Insulin stimulates glucose disposal in muscle and suppress plasma FFA concentrations. Thus, Obesity is an important risk factor of type 2 diabetes mellitus. Hyperglycemia independently impairs endothelial function, probably acting in part through decreased generation of nitric oxide and in part through protein kinase C (PKC) and the formation of reactive oxygen species. The increase activity of PKC, activates the formation of vasoconstrictor endothelin-1 and decrease activity of the vasodilator endothelial nitric oxide synthase (eNOs), (34). Increase production of tumor necrosis factor – α (TNF-α) by adipocytes can reduces insulin sensitivity, reduces activity of insulin receptors substrate (IRS-1) and enhance production of pro-coagulant molecule plasminogen activator inhibitor (PAI-1) which leading to increase insulin resistance, formation of free fatty acid and reduce fibrinolysis that induces vascular occlusion disease (35) (figure 5).
Figure 5
:
In diabetes patient, hyperglycemia increases free fatty acid. This can active protein kinase C (PKC), PKC blocks PI3K pathway, reduces NO formation and increase endothelin-1 (ET-1). All these result in vasoconstriction. Also, adipocytes secrete tumor necrosis factor-1 ( TNF-1) which reduce insulin sensitivity.1-3-4: Hypertension
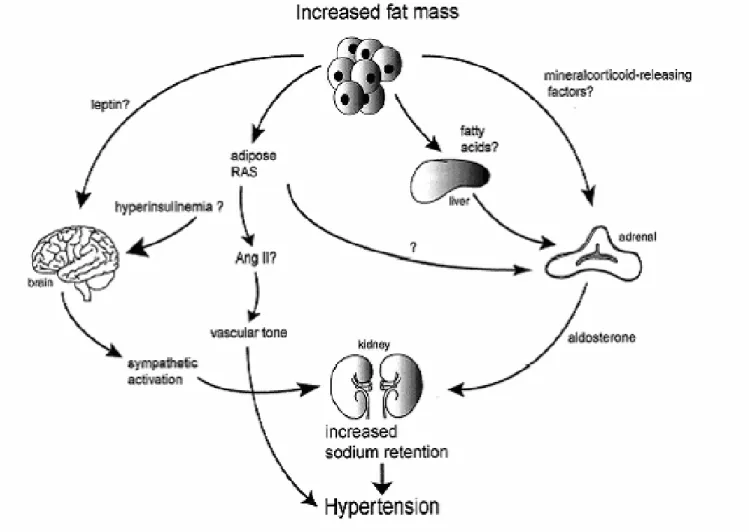
Blood pressure can be increased by a number of interactive and complicated mechanisms. It includes, increased circulating blood volume, abnormal vasoconstriction, decreased vascular relaxation and increased cardiac output (36). The causes of essential hypertension are not clear. It may relative to many factors, such as ethnic origin (black > white), environments and diet (high salt diet), gender (male > female), psychological problem (anxiety and stress), age, obesity, heavy drinking (37). All these can increase peripheral vascular resistance. The secondary hypertension are usually due to hormonal factors. The increase adrenalin or angiotensin. cause vessel constriction. In adrenal tumor, such as pheochromocytoma, has an excessive secretion of catecholamines (38). In renal disease, such as renal artery stenosis, which induce large amount of renin-angiotensin secretion (39). In parenchymal renal disease, often associated with sodium and water retention (40).The abnormalities of vascular resistance may also contribute to the patho-physiology of obesity-related hypertension. Elevated free fatty acids (FFAs) have been found to cause increased vasoconstriction and reduced nitric oxide mediated vaso-relaxation (41, 42). It has also been suggested that there is an increased activity of the sympathetic nervous system by leptin in some obesity phenotypes, adipose tissue can secrete renin-angiotensin-aldosterone system (RAAS), which activates the formation of angiotensin II, fatty acid increases aldosterone secretion from adrenal gland (43), all these may contribute to the vasoconstriction, observed in the obesity-associated hypertension (figure 6).
Figure 6: The adipose tissue has several factors to induce vasoconstriction. Through leptin to increase sympathetic activity, fatty acids to increase aldosterone secretion all cause sodium retention. The adipose RAS can increase angiotensin II secretion. All these can cause vasoconstriction..
1-4. Physiology of blood vessel contraction and relaxation
The blood vessel tone is elicited by smooth muscle in the medial vessel wall. Smooth muscle cells are responsible for the contractile capabilities of blood vessels (large and small arterials, veins), respiratory tract, gastrointestinal tract, bladder, male and female reproductive tracts.
Being different from the skeletal muscle and cardiac muscles, smooth muscle is non-striated muscle. There are two types of smooth muscle arrangements in the body: multi-unit and single-unit. The single-unit type, also called unitary smooth muscle, is far more common. Whereas the former presents itself as distinct muscle fibers that are usually activated by their own nerve fibers, the latter operate as a single unit and are arranged in sheets or bundles (44). Smooth muscle cells have, in general, single nuclei and a plethora of mitochondria. In order to contract, the cells contain thick actin filaments and a thick element called myosin. Whereas the filaments are essentially the same in smooth muscle as they are in skeletal and cardiac muscle, the smooth muscle cell contains less protein than a typical striated muscle cell and much less myosin. The actin content is similar, so the ratio of actin to myosin is ~6:1 in striated muscle and ~15:1 in smooth muscle ( 44, 45). Smooth muscle does not contain the protein troponin; instead calmodulin (which takes on the regulatory role in smooth muscle), caldesmon and calponin are significant proteins expressed within smooth muscle (44).
Unlike in striated muscle, the actin and myosin in smooth muscles are not arranged into distinct sarcomeres that form orderly bands throughout the muscle cell. The Actin filaments attach to the sarcolemma by focal adhesions or attachment plaques and attach to other actin filaments via dense bodies (acting much like Z-lines in striated muscle). Evidence indicates that smooth muscle myosin is not bipolar with a central bare zone as in striated muscle, but is either side-polar or row-polar, and has no bare zone (45).
The sarcolemma possess microdomains specialized to cell-signaling events and ion channels called caveolae. These invaginations in the sarcoplasma contain a host of
proteins (RhoA, G alpha), Protein kinase C, Protein Kinase A, ion channels (L type Calcium channels, ATP sensitive Potassium channels,) in close proximity. The caveolae are often in close proximity to sarcoplasmic reticulum or mitochondria, and have been proposed to organize signaling molecules in the membrane (44, 45).
Smooth muscle contraction:
Smooth muscle contraction is caused by the sliding of myosin and actin filaments (a sliding filament mechanism) over each other (46). Myosin functions as an ATPase utilizing ATP to produce a molecular conformational change of part of the myosin and produces movement. Movement of the filaments over each other happens when the globular heads protruding from myosin filaments attach and interact with actin filaments to form crossbridges. The myosin heads tilt and drag along the actin filament a small distance (10-12 nm). The heads then release the actin filament and adopt their original conformation. They can then re-bind to another part of the actin molecule and drag it along further. This process is called crossbridge (46). Unlike cardiac and skeletal muscle, smooth muscle does not contain the calcium-binding protein troponin. Contraction is initiated by a calcium-regulated phosphorylation of a heavy meromyosin, rather than a calcium-activated troponin system (47).
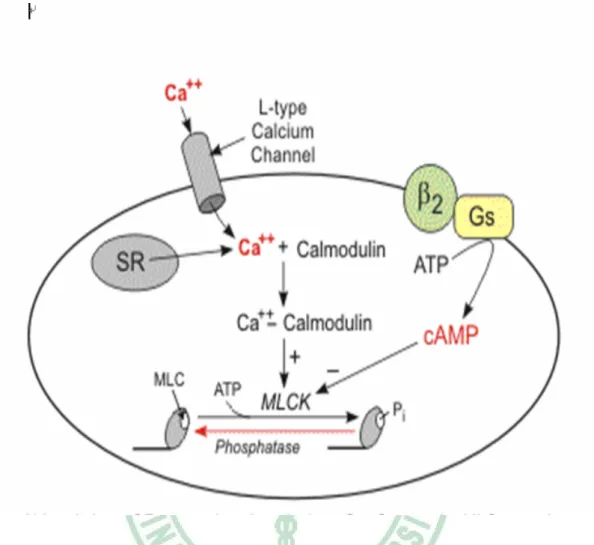
Crossbridge cycling cannot occur until the myosin heads have been activated to allow crossbridges formation. It needs the presence of ATP. The myosin heads are made up of heavy and light protein chains. When the light chains are phosphorylated, they become active and will allow contraction to occur (47, 48). The enzyme that phosphorylates the light chains is called myosin light-chain kinase (MLCK). In order to control contraction, MLCK will work only when the muscle is stimulated to contract. Stimulation will increase the intracellular concentration of calcium ions. These bind to a molecule called calmodulin, and form a calcium-calmodulin complex. It is this complex that will bind to MLCK to activate it, allowing the chain of
Figure 7: In smooth muscle cell, increase level of cytosol calcium can be increased
through calcium influx L-type calcium channel in sarcolemma and calcium release from sarcoplasmic reticulum (SR) inside cell. The calcium binds to calmodulin. This complex then active myosin light chain kinase (MLCK), which increase myosin-actin interaction form muscle contraction.
1-4-1 Factors in controlling vascular smooth muscle contraction
1-4-1-1: Calcium signalling in vascular smooth muscle: In the plasma membrane, there is L-type calcium channel, a voltage gated calcium channels. When an α1 stimulation occur, form an active membrane potential that depolarize cell membrane. This L-type calcium channel then open, allowing calcium ions influx into cell and bind to the Ryanodine receptor (RyR) of the sarcoplasmic reticulum (SR). The RyR open, release large amount of calcium from SR through the RyR (50).
α1 also form an active signal to the G-protein coupling receptor (GPCR). GPCR then activate the formation of IP3, the IP3 then releases calcium from SR through the IP3
sensitive calcium release channels. The calcium ions which are release in cytosol then binds to an protein-calmodulin and form calcium/calmodulin complex. This complex binds to myosin light chain kinase (MLCK), to activate MLCK, then phosphorylate myosin light chain and increase the myosin binds to actin cause smooth muscle contraction (50).
1. Voltage-dependent calcium channel (VDCC):
This channel are activate at depolarized membrane potential. High selective for calcium that allowing substantial amounts of calcium to enter the cells when membrane is depolarized and do not conduct the sodium or potassium. In voltage depend Ca. Channels, There are five subtypes: such as L,T, N, P and R types. The L and T types are predominant in cardiac muscles, where the L type are predominant in smooth muscle. The others are in nerve terminals (51).
(a). L type calcium channels (LTCC): represent a long lasting opening channel, are characterized by a large single–channel conductance are sensitivity to the 1,4-dihydropyridines (DHPs) and activation at larger depolarizations (52). Opening of the L-type calcium channel causes influx of extracellular Ca2+ into cytosol, which then binds to
calmodulin The activated calmodulin molecule activates myosin light chain kinase (MLCK),which phosphorylates the myosin thick filaments These channels are particularly important in regulating the contraction of cardiac and smooth muscle. It composed of three main subunits (53).
β subunit: is a small protein without transmembrane - spanning domains. It influences the behavior of the LTCC and serve as a molecular chaperone to direct the α subunit on the surface membrane, a high affinity to the dihydropyridine site.
δ subunit: Mostly in skeletal muscle, function unknown
The calcium influx through the LTCC involves voltage and calcium dependent transitions in channel conformation that cause the pore-forming α1 subunit to transiently allow permeation of calcium into the myocyte. At resting potential (-80 mV), the LTCC is primarily in a closed but available in open state. Depolarization leads to the opening of the α1 subunit pore, and calcium. moves into the cell down its electrochemical gradient. On the other hand, further depolarization also leads to LTCC inactivation (54)
(b). T type calcium. channel (TTCC): a transient/short type. Widely distributed in cardiac pacemaker and atria tissue. It is hyperpolarization sensitive that cause calcium. influx into cells and becomes cells depolarization. When in cells depolarization, This channel rapid to inactivate. T channels mediate calcium. entry into neurons, and thereby control various calcium. dependent functions such as regulation of other channels, enzymes (55).
(2). Sodium/Calcium exchange (NCX):This channel can active transport of calcium outwards across the cell membrane and inward across the membrane of sacroplasmic reticulum, dependent on the activity of calcium. dependent ATPase. It also extruded calcium. from cell in Na/Ca exchange. This exchanger transfers three sodiums. for one calcium and, therefore, produces a net hyperpolarizing current when it is extruding calcium. The energy for calcium extrusion comes from the electrochemical gradient for sodium, but not directly from the ATP hydrolysis (56).
1-4-1-2: α1 adrenergic receptors
α1 adrenergic receptors cause contraction and promotes the growth of vascular smooth muscle cells. There are three subtypes of α1 receptors (α1a, α1b, α1d) (57). The α1a receptor is the predominant receptor causing vasoconstriction in many vascular beds including mammary, mesenteric, splenic, hepatic, pulmonary and coronary. It is also the major subtype in vena cava, the saphenous and pulmonary vein. α1b receptor is the most abundant subtype in the heart and α1d receptor is the predominant receptor causing vasoconstriction in the aorta (57).
All the adrenergic receptors are link to guanine nucleotide binding protein (G protein) that target the release of catecholamines, α1 adrenergic receptors are predominant in smooth muscle of blood vessels. They are members of G protein coupled receptor super family. Upon activation, α1 adrenergic receptor results in the regulation of multiple effectors system. The primary signal transduction involves activation of the α1 to couples to Gq. GTP then binds to Gq and moves to phospholipids Cβ (PLCβ). PLCβ becomes activated, it can cleave phosphatidyl inositol 4-5-bisphosphate (PIP2) to inositol trisphosphate (IP3) and Diacylglycerol (DAG) in the plasma membrane (58). The IP3 then diffuse from the plasma membrane to the sacroplasmic reticulum (SR). SR then binds to specific IP3 receptors and cause calcium release from SR to the cytosol. When the intracellular calcium rises to about 10-6 M (1 μM), calcium that bind to a variety of calcium regulate proteins including
calmodulin (CaM) – an acidic protein with four high affinity calcium binding sites (59). The binding of calcium to calmodulin, activates the CaM kinase. This kinase than phosphorylates a number of target enzymes. In smooth muscle, CaM kinase can activate myosin light chain kinase (MLCK) that phosphorylated myosin light chain (MLC), and activates smooth muscle contraction as previously described (figure 7).
1-4-1-3: Angiotensin II
Angiotensin II is derived from angiotensinogen. When body sodium level falls in the distal renal tube, or a fall in renal perfusion pressure, the renal sympathetic nerve becomes activated. Where the β-adrenoceptor agonist and the prostaglandin I 2 are all stimulate rennin secretion. Renin stimulates angiotensinogen release from liver cells. The angiotensinogen then circulate through the lung and cleave to form angiotensin I. An enzyme, angiotensin convertive enzyme (ACE) that converts angiotensin I to angiotensin II (60). The receptor of angiotension II, especially AT1 subtype, is
involved in several physiological effects, such as the sympathetic activities, cells growth, water and sodium retention and vasoconstriction (figure 8).
There are 2 subtypes of angiotensin receptors: AT1 and AT2 receptors. The AT1
receptors activate a large array of signal transduction system to produce effects but the function of AT2 receptors are poorly defined, but may exert anti-proliferative,
pro-apoptotic, vasodilatory, proliferation and anti-hypertensive effects (61). The AT1 receptors couple to several heterotrimeric G protein, including Gq, G12, G13 and Gi, but in most cell types, AT1 receptor coupled to Gq and thus active phospholipase C β
(PLCβ). PLCβ then cause formation of IP3 and then calcium release from
sacroplasmic reticulum. The pathway is similar to that for the α1 adrenergic receptor. On the other hand, angiotensin II also exhibits an inhibitory effects on c-GMP in vascular smooth muscle cells (VSMC) by activate of Ca/Calmodulin, which stimulated by phosphodiesterase (PDE5) (62), where the PDEs play critical roles in controlling intracellular c-GMP level by converting c-GMP to 5’-GMP. Chen et.al (63) found that PDE1A1 in VSMC is rapidly activated by angiotensin II, probably by way of increasing calcium. Angiotensin II – mediated activation of PDE1A1 contribute to the effects of angiotensin II on attenuation of c-GMP accumulation. The increase of intracellular calcium, activates MLCK, activate of myosin phosphorylation, cause VSM contraction (figure 9).
Activation of Ang.II receptor also enhance the vascular production of reactive oxygen species (ROS) in part through the activation of membrane-bound NADH and NADPH oxidases (64), which are present in endothelial cells, vascular smooth muscle cells and fibroblasts. The resultant increase in nitric oxide degradation or
in-with in-active nitric oxide leads to the production of peroxynitrate (ONOO¯), a potent oxidant that contributes to vasoconstriction and vascular injury.( 64 ) (figure 10).
Figure 8 :The pathways of angiotension II formation. The ACE pathway is stimulates by renin which converts angiotensinogen to angiotensin I, then converts to angiotensin II by angiotensin converting enzyme. The angiotensin II receptor- AT1
plays several physiological effects.
Figure 9 :The angiotensin II AT1 receptor (AT1) induce vascular smooth muscle
contraction and vascular injury. Induce calcium release from sarcoplasmic reticulum (SR) through IP3 pathway. Attenuate c-GMP by phosphodiasterase 1A1(PDE1A1).
Calcium then binds to calmodulin to form CaM complex. CaM promotes myosin binding to actin in vascular smooth muscle cell (VSMC) cause smooth muscle contraction. AT1 activates NADPH oxidase with the formation of reactive oxygen
species (ROS). The production of O2¯ which react with NO to form the ONOO¯ , a
1-4-1-4: Endothelin (ET)
Endothelin is a strong vasoconstrictor produced in Endothelium. It is a 21 amino acid peptide that causes an extremely potent vasoconstriction in most vascular smooth muscle cells (VSMC). Stimuli of endothelin synthesis include many noxious factors, such as angiotensin II, thrombin, vasopressin, hypoxia et al (65). Within the endothelium, a large inactive precursor molecule, called preproendothelin, under the action of endothelin converting enzyme, is converted to an active ET-1. ET-1 exerts its vascular effects by binding to two specific receptors: the ET-A and ET-B, both belong to the superfamily of G-protein coupled receptors. The ET-A receptors are present on VSMC that promote vasoconstriction and smooth muscle proliferation. ET-B receptors are located on endothelial cells and mediate endothelium-dependent dilation by releasing nitric oxide (NO). When ET-1 binds to ET-A receptor, ET-A receptor becomes activated. This ET-A mediated responses include vasoconstriction, bronchoconstriction and aldosterone secretion (66, 67). ET-A receptors are coupled to phospholipase C, which stimulate Na-H exchange. Active of G-protein (Gq) then bound to GTP and activate phospholipids C (PLC). PLC then cleaves the phosphatidyl inositol 4-5 bisphosphate to inositol triphosphate (IP3) and
Diacylglycerol. The IP3 is a water soluble compound, diffuse from the plasma membrane to the endoplasmic reticulum (ER). When it binds to a specific receptor and cause calcium channels open, release of calcium from ER into the cytosol. When the calcium concentration rise up, calcium binds to Calmodulin and thus cause muscle contraction, as the previously described (figure 10).
Figure 10
:
In endothelium, ET-1 binds to a special receptor-ETB that release nitric oxide (NO), this NO can activate C-GMP in vascular smooth muscle and inhibits muscle contraction. The ET-1 also binds to ETA in vascular smooth muscle that activate the formation of IP3, causing calcium release and muscle contraction.1-4-2: Factors affecting vascular relaxation
1-4-2-1: β adrenergic receptor
β adrenergic receptors are members of a large super-family of receptors linked to guanine-nucleotide-binding protein (G protein). G-protein are signal transducer that conveys information from the receptors. A large super-family of receptors called G-protein coupled receptor (GPCR) is widely used to target for many receptors and drugs. The β adrenergic receptor is an integral protein with seven hydrophobic regions of 20 to 28 amino acids. Three subtypes of β adrenergic receptors are: β1, β2 and β3.(57). All the β adrenergic belong to the super-family of G-protein coupled receptor. β1 receptor is present in on cardiac muscle, and is responsible for the positive inotropic and chronotropic effects of catecholamine. β2 receptor is present on smooth muscle cells and so responsible for smooth muscle relaxation in many organs. β3 receptors is present on brown adipose tissue and gallbladder. It appears to have a role in promoting lypolysis and heat generation in fat (57).
Adrenal gland release adrenaline which bind to β -adenoceptors (β1, β2) on the
smooth muscle cell membrane. This can stimulate G-protein. G-protein than binds to guanosine 5’ di-phosphate (GDP) following hydrolysis of guanosine 5’ tri-phosphate (GTP). Then a subunit of G-protein (Gs) moves to the adenylyl cyclase and activate it. This activates adenylyl cyclase then catalyzes the formation of adenosine 3’-5’ cyclic monophosphate (c-AMP) from adenosine tri-phosphate (ATP) (68).
C-AMP also directly regulates the activity of plasma membrane cation channels-the cyclic nucleotide gated (CNG) channel (69). CNG ion channels have been found in heart, vascular smooth muscle, kidney, testis and central nervous system. These channels open and so directly binding of intracellular cyclic nucleotides and contribute to cellular control of membrane potential and intracellular calcium level when accumulation of c-AMP activates protein kinase A (PKA).
In vascular smooth muscle, β2 adrenoceptors activate the formation of c-AMP, which then phosphorylates myosin light chain kinase (MLCK) to form MLCK-(PO4)2. This
Figure 11
:
Contraction is triggered by influx of calcium through transmembrane calcium channel. The cytosol calcium ions bind to calmodulin to form a complex. This complex activated myosin light chain kinase (MLCK) that phosphorylated myosin light chain (MLC), this active the binding of myosin to actin cause muscle contraction. On the other hand, β adrenergic receptor can active adenylyl cyclase that catalyzes the formation of c-AMP. C-AMP phosphorylate MLCK becomes an inactive form – MLCK(PO4)2 cause muscle relaxation1-4-2-2: Nitric oxide (NO)
NO is a free radical gas molecule , which was discovered in endothelial cells (70). It plays as a signaling molecule in cardiovascular and nervous system as an endogenous activator of soluble guanylate cyclase, which leads to the formation of cyclic guanosine monophosphate (c-GMP), and serves as a second messenger in many cells including nerves, smooth muscle, monocytes and platelets.
NO synthase (NOS) is central to the control of NO biosynthesis. There are three known isoforms of NOS.
1. The neurons NOS (nNO or NOS-1) , a calcium/calmodium dependent enzyme was originally identified in nervous system. It is also important in smooth muscle, skeletal muscle, cardiac muscle and renal mesangial cells (71).
2. The inducible NOS (iNOS) or NOS-II), a calcium/calmodulin independent enzyme that expressed in macrophages, neutrophil, fibroblast and vascular smooth muscle . This enzyme binds calmodulin tightly. It catalyses rapid NO generation ( 71).
3. The endothelium NOS (eNOS or NOS-III), a calcium / calmodulin dependent enzyme that expressed constitutively in endothelial cells and synthesizes the NO for the regulation of blood pressure (71).
Formation of NO: The endogenous NO is produced from L-arginine in an NADPH-dependent reaction and catalyzed by nitric oxide synthase (NOS). NO is an unstable molecule, its formation is stimulated by interaction of nitric oxide synthase with the calcium/calmodulin complex. On the membrane of endothelial cell, the endothelium dependent relaxation stimulators: such
as
acetylcholine, substance P, bradykinin etc, increase cytoplasmic calcium concentration in the endothelial cells. Calcium than binds to calmodulin to form a calcium/calmodulin complex (CaM). This complex can activate NOS, which cleaves arginine into NO and citrulline. NO is found to be a strong vasodilator. (70).In smooth muscle cell, the muscle tone is dependent on the cyclic GMP mediated NO. In cell membrane, NO activate guanylate cyclase (GC). The activated of GC than convert GTP to c-GMP. c-GMP activates Protein kinase G (PKG) – a c-GMP
The increase of c-GMP contributes to the endothelium –dependent relaxation, including:
(a) stimulation of Na/K ATP, the activated Na/K ATP release endothelial derived relaxation factor (EDRF) causes opening of the ATP sensitive K channel allow large of K diffusing out of cell, leading to cell hyperpolarization (71).
(b) inhibition of calcium release from endoplasmic reticulum (ER) leading to reduce intracellular calcium concentration (71).
(c) inhibition of phospholipase C and thus decreasing the production of phosphoinositide (IP3), and reducing calcium release from the ER (71).
(d) direct opening of Ca. dependent K channels, accelerating K efflux to cell and causing cells to hyperpolarize (71).
(e) Protein kinase G activates a signaling pathway that result in phosphatase myosin light chain, then turn myosin light chain in-activated and inhibit the myosin-actin interaction. Relaxation of the vascular smooth muscle cells causes blood vessels to dilate (71) (figure 12).
Figure 12 : In endothelial cell, activating a receptor to acetylcholine, bradykinin or substance P can cause calcium influx into cytosol. Calcium ions binds to calmodulin to form CaM. CaM then actives an enzyme - NOs and catalyses L-arginine to form the Nitric oxide (NO). NO diffuse to smooth muscle cells that activate c-GMP to
1-4-2-3: Potassium channels
1. ATP sensitive potassium channels (KATP)
KATP Found in various tissues including pancreatic β cells, skeletal and smooth muscle cell. These channels are inhibited by intracellular adenosine -5’ triphosphate (ATP) and activated by adenosine -5’ diphophate (ADP).(72).The current voltage relationships of KATP channel have a weak inward rectification, they allow a large K influx than do efflux, meaning that the outward current being smaller than the inward current. The inward rectification of KATP channels is due to a voltage-dependent block of outward current by internal cations, such as Mg2+ and Na+ (72). ATP has two effects on KATP channels: (a) Inhibiting channels activity. (b) maintaining the channels in an operative state.(72) When ATP is not hydrolyzed or in the absence of Mg2+, the increased activity of ATP turn KATP channel inactivated (inhibited). Closure of this channel leads to influx of K+ into cells and depolarizes the cells membrane, enhances the membrane excitability. When ATP is hydrolysis, or in the presence of Mg2+, this channel is in an actives or operative state. Opening this channel allow a large K+ efflux hyperpolarizing the cell membranes (72).
In vascular smooth muscle (VSM), KATP contributes to the resting membrane conductance controls Ca2+ entry through the voltage-dependent Ca2+ channels. The activity of vascular KATP channels is governed by the degree and the sites of phosphorylation and de-phosphorylation. In VSM, KATP can be opened by adenosine dependent protein kinase (PKA) and closed by Ca2+ dependent protein kinase (PKC). Under some situation of metabolic compromise through PKA, active C-AMP than open of these channels allow K+ efflux and membrane becomes hyperpolarization. Leading to the closure of voltage-gated Ca2+ channels and, hence, vaso-relaxation (73).
2. Voltage-dependent potassium channels:
The role of this channel is to allow influx of potassium if the concentration inside the cell drops below some minimal value. It conducts K+ ions across the cell membrane in response to changes in the membrane voltage (74)) cell membrane voltage regulates the opening of a Kv channel, which interfaces the voltage-sensor domains to the pore. the convert voltage-sensor motions directly into gate opening and closing. As the charged ions flow across the membrane, they generate an electric current. The amount of current flow is determined by two factors. First, when the gate of an ion channel opens, ions flow down the concentration gradient from high to low across the membrane, which is typical of the passive transport mechanism. Second, the flow of ions is controlled by the voltage difference across the membrane. Thus, the total ion flow is influenced by the concentration gradient of the ions, the voltage difference across the membrane, and the permeability of the ions.( 74)
3.Calcium sensitive potassium channel: This channel is part of the delayed rectifier
super family. When the membrane calcium channel opens, large of calcium influx into cytosol. The conductance Ca2+activated K+ channels contribute to action potential
repolarization and restrict the excitability of detrusor smooth muscle. In addition, the activation of voltage dependent K+ channels is involved in repolarization and after-hyperpolarization, and it has a fundamental role in stabilizing detrusor smooth muscle excitability. The increase of cytosol calcium leading this calcium sensitive channel open. This result in a large efflux of potassium ions out of the cell, causing cell hyper-polarization. At last membrane calcium channel close, less of calcium influx into cytosol. Vascular smooth muscle then relaxation- vasodilation (75).
1-4-2-4: The effect of PVAT to the blood vessels The previous literatures review
Since 1991, the PVAT was found to have a significant inhibition of the contraction induced by phenylephrine (PE). (76). Later, many investigators studies the PVAT in blood vessels and found that PVAT can cause relaxation or enhanced contraction in blood vessels..
(a) Vessel relaxation
Matthias Lohn et al (77) studied rats thoracic aortas, used transferred fat solution from isolated aortic perivascular fat tissue to the vessel without PVAT. They found that the transferred fat solution has an adventitial derived relaxing factor which plays an anti-contractile effect to the angiotensin II, serotonin and PE.
Stefan Verlohren et al (78) used rats mesenteric artery rings with either intact periadventitial adipose tissue (F+) or removed (F-) to test the contractile response to serotonins, PE and endothelin I. They found that the vasoconstriction to all stimulants were markedly reduced in intact vessels (F+) compared with vessels without periadventitial fat (F-).
Gao et al (79) found the PVAT in human thoracic artery can releases a transferable relaxation factor that acts through the activation of calcium dependent potassium channels. This relaxing factor can attenuated the maximal contraction to U46619 ( a thromboxane A2 / prostaglandin H2 agonist) and PE. This findings were present in
either vessel with intact PVAT or transfer solution incubated with PVAT to vessel without PVAT
(b) Vessel contraction
Gao et al (80) found that in rat superior mesenteric artery with intact PVAT, a vaso-active factors can be released in response to perivascular nerve activation and showed a greater contractile response to electrical field stimulation (EFS) than that without PVAT . Their results show the PVAT enhance arterial contractile response to perivascular nerve stimulation through production of superoxide mediated by NAD(P)H oxidase. This enhancement involves activation of tyrosine kinase and
2. Aim of study and hypotheses
According to the previous studies, investigators found the PVAT exerts a relaxing effect in both small and large arteries.
We wonder whether this finding is true because obese people tend to have high propensity to develop hypertension and vascular diseases compared to the non-obese people.
We have the following objectives or experimental strategies:
a. Use novel methods which are different to the previous studies. such as used fat intact ⁄ fat denuded aortic rings, to transfer fat solution or boiled fat solution to the aortic rings, use nitric oxide inhibitor to inhibit NO activity. All the aortic rings are stimulate by phenylnephrine (PE), potassium chloride (KCl), angiotensin II (Ang.II), some of them are relaxing by carbachol (CCh). To find out whether the perivascular adipose tissues (PVAT) can release a factor, “Adipocyte derived factor” (ADF), which affects vascular tones, either in vascular smooth muscle contraction, relaxation or both.
b. Since obesity is an important risk factor for increase of blood pressure, atherosclerotic change of blood vessels (81). We hypothesize that PVAT accumulation enhance blood vessels contraction. We carry out this study in order to find out whether our findings are consistent with our hypothesis or not.
Chaper 2
Materials and Methods
1. Materials
Animals and tissues preparations
Male Sprague Dawley rats (320-350 g body weight), kept in university experimental animal facilities under standard animal housing conditions were anesthetized by ether and killed instantly by cervical dislocation under the university regulation for the use of experimental animals. The thoracic aorta from 1-2 rats in each experiment were quickly removed and rinsed with Ringer’s solution to remove blood and blood clots. The entire thoracic aorta with intact PVFT and partially fat-denuded aorta are shown in figure 13
Fat intact (F +) and fat denuded (F -) aortic rings were obtained from the same rat and studied in parallel in each experiment. The loosely attached connective tissues were gently removed with tweezers and scissors. Then the vessel was cut into ring segments of 3 - 4 mm in width. The fatty tissue strips remained either intact or denuded. The composition of the Ringer’s solution was (mM): NaCl, 119; NaHCO3, 25; KCl, 4.7; KHCO3, 1.2; MgSO4, 1.2; CaCl2, 1.6; and Glucose, 1.1. Ringer’s solution was kept at 36.5 C and pH 7.3. For prolonged experiments and during equilibration, the Ringer’s solutions were replaced every 20-30 minutes. At the end of the experiment, the wet weights of aortic rings before and after removal of PVFT were measured in order to estimate the amount of fat tissues expressed as tissue wet weight..
:
2. Methods
Contractility measurements
General conditions: After tissue dissection, all the aortic rings were equilibrated in a 5 ml organ bath solution for an hour with a pre-determined stable 2 g (usually 1.5-2.5g) optimal resting tension. After equilibration, the rat aortic rings were then stimulated with 80 mM KCl 2-3 times until they reached a stable plateau contraction. The tension is expressed as a percentage of the steady-state tension (100%) (77). At the end of the experiment (usually after 5-6 hours), the contractile responses to 80 mM KCl remained about 80-90% of the original KCl contraction. Some aortic rings were denuded of fat tissues which were then transferred to and incubated in aerated Ringer’s solution for approximately 2 hours before use (to release the adipocyte – derived factors). The clear solution after removal of the fat tissue just before use is operationally termed “ F solution” (Fat solution). These F solutions were either keep at room temperature or heated to boiling (to deactivated or destroy any heat sensitive factors) and subsequently cooled down to room temperature before adding to fat-denuded aortic rings. (Figure 14)
Unless otherwise indicated, most experiments were performed in endothelium-denuded ring preparations. The functional intactness of endothelium was checked against the degree of endothelium-dependent relaxation to 3 uM CCh after reaching plateau contraction in response to 1 uM PE In most cases, the endothelium – dependent relaxation reached a magnitude of > 60% of the PE contractile response. Relaxation to CCh of < 20% of the PE contractile response was considered to be endothelium denuded.
Preparation of F solution: Rat’s thoracic aortic rings, divided into 6 strips, usually weighing from 9.0 mg to 12 mg in each strip. Removed of fat tissue from those aortic rings and the fat tissue were transferred to a Petric dish containing 20 ml of Ringer’s solution with continuous aeration. The incubation time of at least 2 hrs was allowed to ensure a high release of adipocyte-derived factors (ADF), For control groups, fat denuded aortic rings were stimulated with PE or KCl to construct the concentration-contraction curves. For the test groups, 2 different ways were used to apply the fat solutions.
were stimulated with PE or KCl to construct the dose response curves. Figure 15, tracing 1
(2) Fat-denuded aortic rings were stored with 5 ml of Ringer’s solution, then increase the concentration of PE or KCl and added to it under the dose response curves. When a suboptimal contractile level were obtained, the Ringer’s solution were replaced by the same volume of F-solution which contained the same concentration of PE or KCl. Figure 15, tracing 2
Figure 14 : The preparation and transfer of the solution pre-incubated with PVAT to
the organ baths. First, fat tissues were removed from the thoracic aorta of the rat, and then transferred to a Patrick dish containing 20 ml of Ringer’s solution and let stand with aeration for at least 2 hrs. The solution following the removal of fat tissue by
Figure 15 : Two methods in transfer fat solution to the F- aortic rings. One is to transfer fat solution into the organ bath, after 30 minutes incubation, the rings were stimulated with PE or KCl.(tracing 1) Another way is to stimulate with PE or KCl . When the contractile reaches the plateau, the fat solution containing the same concentration of PE or KCl was introduced (tracing 2)
In some study groups, the fat tissues were placed in 2.5 ml (half volume of organ bath) of distilled water. After 2-hr incubation, the F-solution was heated till boiling. When the solution was cooled to room temperature, 2.5 ml of doubly concentrated Ringer’s solution was added and stored at a temperature of 36.5 C with continuous aeration shortly before use. This protocol helped minimize the change of the pH of the solution following heating, which tends to reduce the HCO3¯ in the solution causing altalination.
3. Chemicals
The phenylephrine (PE), potassium chloride (KCl), carbachol (CCh) and L-N-nitro-L-arginine methyl ester (L-NAME) were all purchased from Sigma chemical Co. (St. Louis, Mo USA). They were all dissolved in distilled water. PE was a 10 mM stock solution. KCl stock solution of 3 M. CCh stock solution of 330 mM. L-NAME stock solution of 30 mM
4. Statistical analysis
The results were expressed as the mean ± standard error of the mean (SEM). The Student’s t test or ANOVA test was used when comparing two or multiple values as appropriate: n represents the number of rats. A value of P<0.05 is considered statistically significance.
Chapter 3
Results
3-1 Effect of perivascular adipose tissue (PVAT) on contraction to KCl and PE
To learn whether the PVAT has an effect on vascular tone in situ. We used the fat intact aortic rings and the fat denuded aortic rings and compared their contractile responses to cumulatively added KCl and PE. When the fat-intact aortic rings were stimulated with KCl and PE, it showed a significantly enhanced sensitivity to KCl and PE manifested as increased contraction to KCl and PE as compared to the fat denuded aortic rings. At low concentration, the maximal contractile response were not changed. Also, a slower rate of relaxation was observed in the fat intact aortic rings compared to the fat denuded aortic rings upon KCl and PE wash out. The mean standard error of half time maximal relaxation (t1/2) for F + after KCl wash out is 4.21 ± 1.45 min. in compared to 1.85 ± 0.24 min. for F – in these experiments. figure.16,17.
A separate experiment stimulated by PE is shown in figure.18,19. Where the t1/2 for F+ after PE wash out is 7.3 ± 1.23 min. in compared to 3.42 ± 1.54 min. for F-.
Figure16: Representative concentration-contraction curve of KCl induced contraction
in rat aortic ring with fat intact (F+) or fat denuded (F-) aortic rings. Note the delayed onset of relaxation and the slow relaxation rate following washout of KCl in F+ compared to F-. t1/2 =half time maximal relaxation in minute.
Figure 17: The Concentration-contraction relationship of KCl-induced contraction of
the fat intact (F+, white) and fat denuded (F-, black) aortic rings. At low concentrations of KCl, the F+ showed a higher contractile response compared to F-. At the optimal concentrations of KCl, both F+ and F- showed the same level of maximal contraction. * P < 0.05
Figure 18
:
The fat intact aortic rings F + has a higher contractile response in low concentration ( 30 nM ) of PE than the Fat denuded aortic rings F-. Upon PE washout, F + rings also shows the presence of a slow relaxing rate.Figure 19
:
The effects of PE to the fat intact aortic rings (F +, white) and fat denuded aortic rings (F -, black). At low concentrations ( 30-100 nM ) of PE , the F + have a higher contractile effect to PE, compared to F -. At high concentrations (300-1000 nM) of PE, both F + and F – showed the same maximal contraction.Effect of solution following pre-incubation with perivascular fat
( F solution)
3-2 Effect of F solution on aortic contraction to PE and KCl
To learn whether the effect of fat in fat intact aorta is due to factors released and diffused out from fat tissues, we studied the effect of the F solution, Ringer’s solution on the contraction of the fat-denuded aortic rings. In the groups which were exposed to the fat solution, they showed an enhanced contractile response curves at low concentration of PE and KCl, comparable to the control groups. The mean standard error of half time maximal relaxation (t1/2) for F - in control group after PE wash out is 1.7 ± 0.75 min. and in study group is 2.1 ± 0.44 min. The mean standard error of half time maximal relaxation (t1/2) for F- in control group after KCl wash out is 1.9 ± 0.42 min. and in study group is 2.1 ± 0.55 min.
The stimulation by PE are show in figures 20, 21 The stimulation by KCl are show in figures 22, 23.
Figure 20: After transferred the F solution to the fat denuded aortic rings (F-) in
response to PE ( 0.1 uM), it showed a significant increase reactivity to PE with a rise up baseline compared to the control groups. (in before transfer F solution or upon addition Ringer solution)
The percentage of rise up baseline is 31% ( X/Y=2.2/7=31% ) RS:Ringer’s solution FS:Fat solution
Y: the magnitude in before transfer of F solution (control) X: the increment about the control
Figure 21:Transferred of F solution with the PE [100nm] showed a significant enhance vascular contractile response compared to the control group * p < 0.005
Figure 22
:
After the transfer of the F solution to the fat denuded aortic rings (F-) in response to KCl (40 mM), it showed a significant increased contractile response comparable to the control groups.(in before transfer F solution or upon addition of Ringer solution) The percentage of rise up baseline is 34% ( X/Y=3.4/10=34% )RS:Ringer’s solution FS:Fat solution Y: the magnitude in transfer of F solution (control) X: the increment about the control
Figure 23
:
Transfer of F solution with the 40mM KCl to fat denuded aortic rings caused a significant enhancement of contractile response compared to the control group. * p = 0.0053-3 Effects of different concentration fat solution on contraction to PE and KCl
To examine whether the effect of F solution is dependent upon the concentration of the substances released from the fat cells, and thus, the amount of fat tissues, we measured the weight of fat tissue incubated with a fixed volume (usually 20 ml) of Ringer’s solution in each separate experiment. The concentrations of fat solution in the groups of 100 nM of PE were between 0.34 to 1.82 mg/ml, and in the groups of 20 mM of KCl were between 0.88 to 21.8 mg/ml. In both groups, there is a positive correlation between the enhanced vascular contraction and the wet weight of fat tissues (figure 24, 25).
Figure 24: A positive correlation with an increase of vessel contraction relative to increasing concentration (from 0.34 to 1.82 mg/ml) of fat tissue in response to 100 nM PE.
Figure 25: A positive correlation with an increase of vessel contraction relative to the increasing of the concentration (from 0.88 to 21.8 mg/ml) of fat tissue in response to 20 mM KCl.