Review Article:
Acupuncture for Attenuating Dyspnea in Patients with Chronic Obstructive Pulmonary Disease
Pin-Kuei Fu1 and Ching-Liang Hsieh2,3,4*
1Division of Critical Care & Respiratory Therapy, Department of Internal Medicine, Taichung Veterans General Hospital, Taichung, 407, Taiwan
2Department of Chinese Medicine, China Medical University Hospital, Taichung, 40402, Taiwan
3Graduate Institute of Integrated Medicine, College of Chinese Medicine, China Medical University, Taichung, 40402, Taiwan
4Acupuncture Research Center, China Medical University, Taichung, 40402, Taiwan *Correspondence should be addressed to Dr. Ching-Liang Hsieh, Graduate Institute of
Integrated Medicine, College of Chinese Medicine, China Medical University, 91 Hsueh-Shih Road, Taichung 40402, Taiwan
TEL: 886-4-22053366 (ext. 3500) Fax: 886-4-22037690
E-mail: [email protected] Running title: Acupuncture and COPD
Abstract
Chronic obstructive pulmonary disease (COPD) is an increasingly serious global health problem that is associated with significant morbidity and mortality. The main pathological feature of COPD is the persistent limitation of respiratory airflow, which leads to fatigue, dyspnea, and decreased physical activity. Dyspnea is a cardinal symptom of COPD, and increases in severity as the course of COPD progresses. Therefore, the Global Initiative for Chronic Obstructive Lung Disease (GOLD) recommended in 2011 that COPD assessment should based on the combination of symptoms, lung function, and the risk of exacerbations. Acupuncture has become a popular treatment for various medical conditions. Whether acupuncture can improve lung function and exercise capacity in COPD patients by attenuating the dyspnea and fatigue associated with COPD is unclear. In our review, we discuss the latest assessment criteria for COPD according to the revised GOLD guidelines, and summarize the most common outcome measures used to assess COPD patients. We also discuss the results of clinical trials of acupuncture treatment for COPD. The concept of the minimal clinically important difference score of outcome measures in COPD is also addressed.
1. Introduction
Chronic obstructive pulmonary disease (COPD) can be caused by cigarette smoking or exposure to noxious inhalants. The COPD has become an increasingly serious worldwide health problem that is associated with significant morbidity and mortality . It is estimated that COPD will be the third leading cause of death worldwide, and the fifth leading contributor to global disease burden by 2020 . The main pathological feature of COPD is persistent restricted respiratory airflow caused by chronic airway inflammation, which leads to decreased physical activity, fatigue, and dyspnea .
The previous guidelines for the assessment of COPD severity and treatment suggested lung function testing, especially the measurement of the 1-s forced expiratory volume (FEV1). Dyspnea, the subjective sensation of difficulty during breathing, is a cardinal symptom of COPD, and its severity and magnitude increase as COPD progresses . Therefore, the Global Initiative for Chronic Obstructive Lung Disease (GOLD) revised the assessment criteria for COPD in 2011, recommending that COPD patients should based on a combination of symptoms, lung function, and the risk of exacerbation .
Pulmonary rehabilitation (PR) is suggested as a non-pharmacological treatment for COPD patients to improve their exercise tolerance and decrease the dyspnea and fatigue . However, whether acupuncture may be an effective non-pharmacologic treatment in COPD to attenuate dyspnea and fatigue, improve lung function, and increase exercise capacity is uncertain. In this review, we introduce the recently revised GOLD guidelines for the assessment of COPD, and summarize the most common outcome measures used in COPD. We also analyze the results of recent clinical trials of acupuncture treatment for COPD.
2. Overview of the GOLD-2011 guidelines for COPD assessment
Since 2001, the GOLD has published its recommendations for the clinical diagnosis and management of COPD. The latest GOLD guidelines were announced in 2011, and emphasize
that the assessment of COPD should include the evaluation of the combined symptoms of the severity of respiratory airflow limitations, the history of exacerbations, and the comorbidities . In contrast to previous recommendations, the new GOLD guidelines place less emphasis on spirometry testing for the evaluation of disease severity than on the evaluation of symptoms. The absolute level of FEV1 is no longer considered to be the only tool for severity classification in COPD, based on its lack of reliability as a marker for the severity of dyspnea, exercise
limitation, and health status impairment .
For symptom assessment, several validated questionnaires have been used to distinguish patients with severe symptoms from those with less severe symptoms. The GOLD now
recommends that the Modified British Medical Research Council (mMRC) Questionnaire or the COPD Assessment test (CAT) be used to assess dyspnea in COPD . In addition, the new GOLD guidelines recommend that, all COPD patients should first be assessed using the mMRC or CAT scale, with an mMRC grade of > 2 or a CAT score of ≥ 10 as the definition of severe symptoms. Subsequent assessment of exacerbation risk is suggested to include both spirometry testing and the analysis exacerbation history, with GOLD 3 or 4 spirometry classification and 2 or more exacerbations during the preceding year each representing high risk . Thus, according to the GOLD-2011 guidelines, the severity of COPD can classified as category A, B, C, or D (Figure 1).
3. Outcome measures and the minimal clinically important difference score
The COPD requires a multifaceted approach to clinical assessment and treatment. The most common methods for assessing COPD progression rely on lung function testing, with an
emphasis on FEV1. However, current trends in clinical practice focus on the evaluation of clinical outcomes and patient-reported measures, such as dyspnea, exercise capacity, exacerbations, level of physical activity, and health status, as essential parts of the clinical assessment of COPD beyond FEV1 measurements . The outcomes that have been most
frequently applied to the assessment and treatment of COPD, including pulmonary rehabilitation, are summarized in Table 1.
The outcome measures are further classified into dyspnea scales, quality of life scales, exercise capacity scales, pulmonary function test score, and a multidimensional score . Because dyspnea is the most common COPD-related presentation, several different approaches have been used for measuring dyspnea in clinical trials, among which the Medical Research Council Scale (MRCS), the Modified Borg Scale (MBS), the Shortness of Breath Questionnaire the Baseline Dyspnea Index, and the Transition Dyspnea Index are most often used. For quality of life measures, the scales most commonly applied are the St. George Respiratory Questionnaire (SGRQ), the Chronic Respiratory Disease Questionnaire, the Medical Outcomes Study Short Form-36, and the frequency of exacerbations.
The methods most often used for assessing exercise capacity following treatment for COPD patients were the 6-Minute Walk test (6MWT), the Incremental Shuttle Walk test, the Endurance Shuttle Walk test, and ergometry (usually bicycle-ergometer or treadmill). Pulmonary function tests, including measurements of the FEV1, the functional residual capacity, the inspiratory capacity, the residual volume, and the total lung capacity have been frequently applied. Currently, multidimensional scoring, such as that based on the BODE index and the CAT is thought to be an important prognosticator for COPD patients.
We suggest that acupuncture clinical trials that evaluate the treatment effect as the endpoint should use a standard set of outcome measures (Table 1). In addition, we suggest that the outcome measures should be quantified based on the minimal clinically important difference score (MCID). The MCID was developed by Jaeschke et al in 1989 to improve assessments in which instrument-based measurements of outcomes that show statistically significant changes after intervention are not accompanied by significant changes in clinical parameters . A summary of the MCIDs of standard outcome measures is shown in Table 1.
4. The clinical trials of acupuncture in COPD
In our survey of the literature for studies of acupuncture treatments for COPD, we used the keywords “Acupuncture AND COPD” to search for clinical trials in the Pub Med database. All potentially relevant full-text articles in English that used dyspnea or breathlessness as an endpoint, were included in our review. We reviewed 9 clinical trials (Table 2), including one descriptive study trial and 8 randomized controlled trials (RCTs) . Two of the RCTs used transcutaneous electrical nerve stimulation over acupoints (Acu-TENS), and the remaining 7 trials used standard acupuncture for COPD patients. The outcome measures that were used included the reduction of dyspnea or the improvement of lung function. In 6 of the 9 trials, positive results were observed following the acupuncture treatments , with the 2 studies of Acu-TENS treatment reporting improvements in both dyspnea and lung function in stable COPD patients .
The detailed information regarding the study design, the patient selection, and the outcome measures of the clinical trials of acupuncture treatments for COPD are listed in Table 2. Jobst et al used a 3-week randomized controlled study to investigate whether acupuncture provided benefits based on subjective scores of dyspnea following the 6MWT . Twenty-six COPD patients were enrolled in the acupuncture and control groups. The 4 subjective scores derived from the outcome measures were the general wellbeing, the shortness-of-breath, the oxygen cost, and the modified Borg scores. The 6MWT and lung function testing, including the peak expiratory flow rate, the FEV1, and the forced vital capacity measurements, were also
conducted.
The Jobst et al study showed that the acupuncture group had significantly greater
improvement in the 6MWT results and all of the subjective scores, compared with the control group. After three weeks of treatment, the mean distance of the 6MWT for the acupuncture group was 49.6 m greater than that of the control group. However, the results of lung function tests conducted before and after treatment showed no change in both groups. Jobst et al
proposed that their results demonstrated significantly greater improvement in dyspnea in the COPD patients who received the acupuncture treatment.
During the past 5 years, the Suzuki group has conducted 3 RCTs of acupuncture treatment for COPD . The major acupuncture points treated in the Suzuki group's studies were the LU1 (Zhongfu), the LU9 (Taiyuan), the LI18 (Futu), the CV4 (Guanyuan), the CV12 (Zhongwan), the ST36 (Zusanli), the KI3 (Taixi), the GB12 (Wangu), the BL13 (Feishu), the BL20 (Pishu), and the BL23 (Shenshu; Table 2). They determined the efficacy of acupuncture treatment in stable COPD patients for improving dyspnea following exercise using the Borg scale following the 6MWT, and the lung function tests and the SGRQ were also conducted. The Borg scale results showed mean improvements of 2.2 points , 2.0 points , and 3.6 points in the acupuncture treatment groups. They also reported improvements in the FEV1 measurements, the SGRQ scores, and 6MWT distances. The results of the Suzuki group's RCTs are summarized in Table 2.
5. Clinical significance of acupuncture in COPD based on the MCID
The results of studies that assessed outcomes based on the MCID are summarized in Table 3. The 2 RCTs in which acupuncture treatment did not improve dyspnea used the Visual Analog Scale to quantify the outcome , whereas the Suzuki group's studies used more objective methods to measure the outcome beyond the FEV1, including the MBS, the MRCS, the SGRQ, and the 6MWT . The parameters that exhibited the greatest significant differences following treatment were the MBS, the SGRQ, and the 6MWT, all of which contributed to the significant changes observed in the MCID scores. However, the changes in the MRCS and the FEV1 following treatment were of borderline significance based on the MCID score. Thus, investigators should evaluate the data from clinical trials based on both the P value and the MCID score.
The COPD is a heterogeneous, multi-component disease associated with significant clinical burden and increasing mortality. Dyspnea is a very common symptom in COPD because of the persistent airflow limitations caused by the chronic airway inflammation. In addition to
pulmonary rehabilitation (PR), a growing body of evidence suggests that acupuncture may be an effective non-pharmacologic treatment for attenuating dyspnea in COPD patients. We suggest that studies of the efficacy of acupuncture in COPD should use a standard set of subjective scales to obtain comparable evaluations of the clinical significance of their data, such as that provided by the MCID score.
Conflict of Interest
References
[1] A. Corsonello, et al. "Comorbidities of chronic obstructive pulmonary disease," Curr
Opin Pulm Med, vol. 17 Suppl 1, no. pp. S21-28, 2011.
[2] D.B. Hodgson, et al. "Thorax in focus: Chronic obstructive pulmonary disease,"
Thorax, vol. 67, no. 2, pp. 171-176, 2012.
[3] D.D. Marciniuk, et al. "Managing dyspnea in patients with advanced chronic obstructive pulmonary disease: A canadian thoracic society clinical practice guideline," Can Respir J, vol. 18, no. 2, pp. 69-78, 2011.
[4] J. Vestbo, et al. "Global strategy for the diagnosis, management and prevention of chronic obstructive pulmonary disease, gold executive summary," Am J Respir Crit
Care Med, vol. no. pp. 2012.
[5] J. Vestbo, et al. "The 2011 revision of the global strategy for the diagnosis, management and prevention of copd (gold)--why and what?," Clin Respir J, vol. 6, no. 4, pp. 208-214, 2012.
[6] C. Tantucci, Modina D. "Lung function decline in copd," Int J Chron Obstruct Pulmon
Dis, vol. 7, no. pp. 95-99, 2012.
[7] I.G. Tsiligianni, et al. "Assessing health status in copd. A head-to-head comparison between the copd assessment test (cat) and the clinical copd questionnaire (ccq),"
BMC Pulm Med, vol. 12, no. pp. 20, 2012.
[8] T. Glaab, et al. "Outcome measures in chronic obstructive pulmonary disease (copd): Strengths and limitations," Respir Res, vol. 11, no. pp. 79, 2010.
[9] E. Crisafulli, Clini E.M. "Measures of dyspnea in pulmonary rehabilitation,"
Multidiscip Respir Med, vol. 5, no. 3, pp. 202-210, 2010.
[10] B.R. Celli, et al. "The body-mass index, airflow obstruction, dyspnea, and exercise capacity index in chronic obstructive pulmonary disease," N Engl J Med, vol. 350, no. 10, pp. 1005-1012, 2004.
(mcid): A necessary pretense," J Man Manip Ther, vol. 16, no. 4, pp. E82-83, 2008. [12] M. Suzuki, et al. "Combined standard medication and acupuncture for copd: A case
series," Acupunct Med, vol. 30, no. 2, pp. 96-102, 2012.
[13] M. Suzuki, et al. "A randomized, placebo-controlled trial of acupuncture in patients with chronic obstructive pulmonary disease (copd): The copd-acupuncture trial (cat)," Arch Intern Med, vol. 172, no. 11, pp. 878-886, 2012.
[14] B.M. Deering, et al. "Acupuncture as an adjunct to pulmonary rehabilitation," J
Cardiopulm Rehabil Prev, vol. 31, no. 6, pp. 392-399, 2011.
[15] S.P. Ngai, et al. "Effect of 4 weeks of acu-tens on functional capacity and beta-endorphin level in subjects with chronic obstructive pulmonary disease: A randomized controlled trial," Respir Physiol Neurobiol, vol. 173, no. 1, pp. 29-36, 2010.
[16] C.A. Whale, et al. "Pilot study to assess the credibility of acupuncture in acute
exacerbations of chronic obstructive pulmonary disease," Acupunct Med, vol. 27, no. 1, pp. 13-15, 2009.
[17] M. Suzuki, et al. "The effect of acupuncture in the treatment of chronic obstructive pulmonary disease," J Altern Complement Med, vol. 14, no. 9, pp. 1097-1105, 2008. [18] K.S. Lau, Jones A.Y. "A single session of acu-tens increases fev1 and reduces
dyspnoea in patients with chronic obstructive pulmonary disease: A randomised, placebo-controlled trial," Aust J Physiother, vol. 54, no. 3, pp. 179-184, 2008. [19] G.T. Lewith, et al. "Can a standardized acupuncture technique palliate disabling
breathlessness: A single-blind, placebo-controlled crossover study," Chest, vol. 125, no. 5, pp. 1783-1790, 2004.
[20] K. Jobst, et al. "Controlled trial of acupuncture for disabling breathlessness," Lancet, vol. 2, no. 8521-22, pp. 1416-1419, 1986.
Legend
Figure 1. Chronic obstructive pulmonary disease (COPD) assessment based on the severity of symptoms, spirometry, and the risk of exacerbations. Based on the recommendations of the Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2011, patients with COPD should be evaluated using a 2-step assessment. Patients should first be assessed using the Modified British Medical Research Council (mMRC) Questionnaire or the COPD Assessment test (CAT). Patients with less symptoms, such as mMRC grade 0-1 or CAT < 10, are assigned to the left side of the box, whereas patients with more symptoms (mMRC > 2 or CAT ≥ 10) are assigned to the right side of the box. The exacerbation risk of patients should be subsequently classified as low-risk (lower area of the box) or high-risk (upper area of the box) based on spirometry results (GOLD 1-2 = low risk; GOLD 3-4 = high risk) and exacerbations history during the previous 12 mo (0-1 = low risk; ≥ 2 = high risk). Thus, the severity of COPD can classified as category A, B, C, or D.
Table 1. Outcome measures apply in chronic obstructive pulmonary disease (COPD) Dyspnea measure scales
Parameters Recommended “Minimal clinical
important difference (MCID)” Medical Research Council Scale (MRC) 1-point
Modified Borg Scale (CR-10) 1-unit UCSD Shortness of Breath Questionnaire
(SOBQ)
5-units
Visual Analog Scale (VAS) 10%
Baseline Dyspnea Index/Transition Dyspnea Index (BDI/TDI)
1-unit
Quality of Life (QoL) scales
Parameters Recommended “Minimal clinical
important difference (MCID)” St. George`s Respiratory Questionnaire
(SGRQ)
4-points
Chronic Respiratory Disease Questionnaire (CRQ)
0.5-ponit
Medical Outcomes Study Short Form-36 (SF-36)
No MCID has been established yet
Frequency of exacerbations ≦1/year or ≧2/year Exercise Capacity
Parameters Recommended “Minimal clinical
important difference (MCID)” 6-Minute Walk Test (6MWT) 54-80 meters
Incremental Shuttle Walk Test (ISWT) 47.5 meters
Endurance Shuttle Walk Test (ESWT) No MCID has been established yet Ergometry (bicycle-ergometer or
treadmill)
No MCID has been established yet
Pulmonary Function Test
Parameters Recommended “Minimal clinical
important difference (MCID)” Forced Expiratory Volume in 1 Second
(FEV1)
Suggested 100-140 ml
Functional residual capacity (FRC), Inspiratory capacity (IC), Residual Volume (RV) and Total lung capacity
Neither a standardized classification for the severity of hyperinflation nor a MCID has been established yet
(TLC)
Multidimensional scoring systems
Parameters Recommended “Minimal clinical
important difference (MCID)”
BODE index No MCID has been established yet
CAT 3.76
BODE index comprises four components: nutritional state (BMI), airflow limitation
(Obstruction, FEV1), breathlessness (MRC Dyspnea scale), and Exercise capacity (6MWD); CAT: the COPD Assessment Test.
Basic information Intervention & control
Acupuncture points COPD status (Stable or
AE)
Outcome Measures Major Findings in Acupuncture group
Trials with positive results ¶Jobst et al. (1986); UK Lancet RCT Acupuncture & Placebo acupuncture 13 sessions in the period of 3 weeks
No mention about the acupuncture points
No mention about COPD stage
Stable COPD
Primary: Dyspnea (SOB score, General Wellbeing score, Score of Modified Borg Scale), 6MWD
1. Significant improvement in dyspnea, General
wellbeing and Modified Borg scores 2. significant increasing in 6MWD: mean increase of 107.9 m ¶Lau et al. (2008); Hong Kong Aust J Physiother. RCT Acu-TENS (N=23) & Control (N=23) Single 45-minute session
EX-B1 (Dingchuan) Stage I, II Stable COPD
Primary: Lung function (FEV1 and FVC), Dyspnea (100-mm visual analogue scale) 1. FEV1 significant increased by 0.13L 2. Dyspnea significant decreased by 11 mm ¶Suzuki et al. (2008);Japan J Altern Complement Med. RCT Acupuncture (N=15) & Control (N=15) Once a week Duration: 10 weeks LU1 (Zhongfu), LU 5 (Chize), LU9 (Taiyuan), CV4 (Guanyuan), CV12 (Zhongwan), KI3 (Taixi), BL13 (Feishu) and BL23 (Shenshu)
Stage II, III, IV
Stable COPD
Primary: Score of Modified Borg Scale after 6MWT Secondary: 6MWD; the lowest SpO2 during 6MWT; FEV1, FVC and VC; MIP, MEP; FHJ score
1. Borg scale score improved from 4.4 to 2.2 2. significant increasing in 6MWD: from 380.2 to 425.6 m. (+45.4 m)
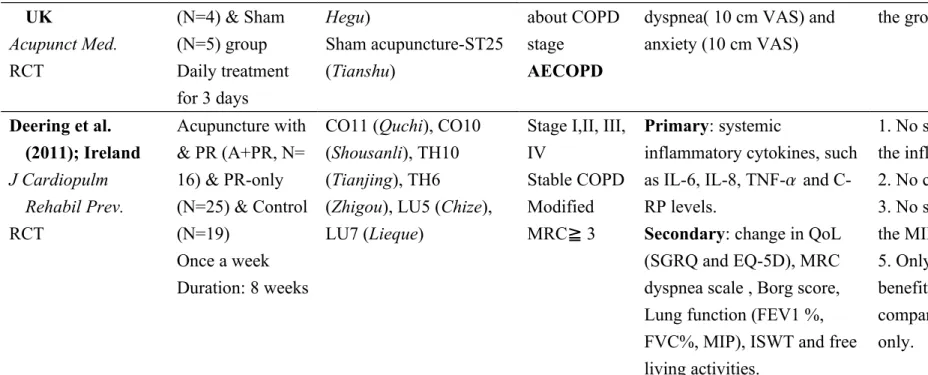
2. Post-6MWT SpO2 decline significant improved Table 2. Experimental design of clinical trials using acupuncture for dyspnea for COPD
3. Significant increasing in FEV1: from 1.25L to 1.34L 4. Significant improvement in MIP, MEP 5. Significant improvement in FHJ score ¶Ngai et al. (2010); Hong Kong Respir Physiol Neurobiol. RCT Acu-TENS (N=10) & Placebo-TENS (N=8) & Sham-TENS (N=10) 5 sessions per week Duration:4 weeks
EX-B1 (Dingchuan) No mention about COPD stage Stable COPD Primary: Physical(lung function, 6MWD) and Psychosocial (SGRQ) function. Secondary: -endorphin, immunologic marker(IL-8, TNF- , C-RP) levels 1. Significant increasing in FEV1: from 0.79L to 0.86L 2. significant increasing in 6MWD: from 305.8 to 329.5 m. (+23.7 m) 3. Post-6MWT SpO2 decline significant improved 4. SGRQ score improved (total: -5.2, activity:-9.0) 5. -endorphin increased, 6. No change in IL-8, and C-RP ¶Suzuki et al. (2012);Japan Acupunct Med Prospective case series Acupuncture (N=26) Once a week Duration: 10 weeks
LU1 (Zhongfu), LU9 (Taiyuan)
LI18 (Futu), CV4 (Guanyuan), CV12 (Zhongwan), ST36 (Zusanli), KI3 (Taixi),
Stage I, II, III, IV
Stable COPD
Primary: Score of Modified Borg Scale after 6MWT Secondary: BODE index (BMI, degree of airflow Obstruction, functional Dyspnea and Exercise
1. Borg scale score improved from 4.0 to 2.0. 2. BODE index improved from 4.0 to 2.1
3. 6MWD increased from 371.2 m to 420.0 m (+ 48.8
GB12 (Wangu), BL13 (Feishu), BL20 (Pishu) and BL23 (Shenshu)
capacity)
Other: 6MWD; the lowest SpO2 during 6MWT; Pulmonary function test (FEV1,FVC, FEV1%); Ventilator muscle strength and endurance ( MIP, MEP); MRC dyspnea scale
m)
4. SpO2 during the 6MWT 5. MRC score, nutritional status, resp. function and resp. muscle strength improved.
¶Suzuki et al. (2012);Japan
Arch Intern Med
RCT Acupuncture (N=34) & Placebo needling (N=34) Once a week Duration: 12 weeks
LU1 (Zhongfu), LU9 (Taiyuan)
LI18 (Futu), CV4 (Guanyuan), CV12 (Zhongwan), ST36 (Zusanli), KI3 (Taixi), GB12 (Wangu), BL13 (Feishu), BL20 (Pishu) and BL23 (Shenshu)
Stage II, III, IV
Stable COPD
Primary: Score of Modified Borg Scale after 6MWT Secondary: 6MWD; the lowest SpO2 during 6MWT; FEV1; SGRQ
Other: (DLCO, RV, TLC); ( MIP, MEP, Rib cage ROM); (BMI, prealbumin); MRC dyspnea scale
1. Borg scale score improved from 5.5 to 1.9 2. 6MWD,SpO2 during the 6MWT, and SGRQ
improved
3. MRC score, nutritional status, resp. function and resp. muscle strength improved.
Trials with negative results Lewith et al. (2004); UK Chest RCT, crossover study Acupuncture & mock TENS (N=24) 6 sessions Duration: 3 weeks RNE20 (Huagai), REN21(Xuanji), LI4 (HeGu) No mention about COPD stage Stable COPD
Primary: Dyspnea (VAS), SGRQ
No significant treatment difference between acupuncture and mock TENS in VAS and SGRQ scores.
UK Acupunct Med. RCT (N=4) & Sham (N=5) group Daily treatment for 3 days Hegu) Sham acupuncture-ST25 (Tianshu) about COPD stage AECOPD
dyspnea( 10 cm VAS) and anxiety (10 cm VAS) the groups. Deering et al. (2011); Ireland J Cardiopulm Rehabil Prev. RCT Acupuncture with & PR (A+PR, N= 16) & PR-only (N=25) & Control (N=19) Once a week Duration: 8 weeks
CO11 (Quchi), CO10 (Shousanli), TH10 (Tianjing), TH6
(Zhigou), LU5 (Chize), LU7 (Lieque)
Stage I,II, III, IV
Stable COPD Modified MRC≧ 3
Primary: systemic
inflammatory cytokines, such as IL-6, IL-8, TNF- and C- RP levels.
Secondary: change in QoL (SGRQ and EQ-5D), MRC dyspnea scale , Borg score, Lung function (FEV1 %, FVC%, MIP), ISWT and free living activities.
1. No significant different in the inflammatory markers 2. No change on spirometry 3. No significant change on the MIP, the SGRQ,
5. Only small but significant benefit in Borg score compared A+PR with PR-only.
6MWT: 6-minute walk test; 6MWD: 6-minute walk distance; SpO2: oxygen saturation by pulse oximetry; FEV1: forced expiratory volume in 1 second; SGRQ: the St George Respiratory Questionnaire; DLCO: diffusing capacity of the lung for carbon monoxide; RV: residual volume; TLC: total lung capacity; MIP: maximum inspiratory mouth pressure; MEP: maximum; ROM: range of motion; BMI: body mass index; MRC: the Medical Research Council ; PR: pulmonary rehabilitation; IL: interleukin; TNF: tumor necrosis factor; CRP: C-reactive protein; QoL: Quality of life; EQ-5D: EuroQoL; ISWT: incremental shuttle walk test; AECOPD: acute exacerbations of COPD; VAS: visual analogue scale; VC: Vital capacity; FHJ score: The Fletcher Hugh-Jones category
Table 3. Analyze the clinical significant of acupuncture in COPD trials by the definition of MCID
Parameters Baseline After treatment Change Trials results
Scale 4.0 2.0 -2.0 *¶Suzuki et at (Acupunct Med. 2012)
4.4 2.2 -2.2 *¶Suzuki et at (J Altern Complement Med.
2008)
MRC 3.2 2.3 -0.9 *Suzuki et at (Arch Intern Med. 2012)
2.4 1.6 -0.85 *Suzuki et at (Acupunct Med. 2012)
SOBQ 3.9 3.0 -0.9 *Jobst et al (The Lancet. 1986)
SGRQ (total score)
46.2 30.2 -16.0
-5.2
*¶Suzuki et at (Arch Intern Med. 2012) *¶Ngai et al (Respir Physiol Neurobiol. 2010) SGRQ
(symptom)
54.7 26.9 -27.8
-0.3
*¶Suzuki et at (Arch Intern Med. 2012) Ngai et al (Respir Physiol Neurobiol. 2010) SGRQ
(activity)
58.6 44.6 -12.0
-9.0
*¶Suzuki et at (Arch Intern Med. 2012) *¶Ngai et al (Respir Physiol Neurobiol. 2010) SGRQ
(impact)
33.5 20.5 -13.0
-8.5
*¶Suzuki et at (Arch Intern Med. 2012) ¶Ngai et al (Respir Physiol Neurobiol. 2010)
6MWD 373.2 335.5 305.8 380.2 227.3 436.7 389.0 329.5 425.6 304.1 +63.5 +53.5 +23.7 +45.4 +76.8
*¶Suzuki et at (Arch Intern Med. 2012) *¶Suzuki et at (Acupunct Med. 2012)
*Ngai et al (Respir Physiol Neurobiol. 2010) *Suzuki et at (J Altern Complement Med. 2008) *¶Jobst et al (The Lancet. 1986)
FEV1 1.0 1.19 0.79 1.25 1.24 1.1 1.31 0.86 1.34 1.37 +0.07 +0.12 +0.07 +0.09 +0.13
Suzuki et at (Arch Intern Med. 2012) *¶Suzuki et at (Acupunct Med. 2012)
*Ngai et al (Respir Physiol Neurobiol. 2010) Suzuki et at (J Altern Complement Med. 2008) *¶Lau et al. (Aust J Physiother. 2008)
0.81 0.83 +0.02 Jobst et al (The Lancet. 1986) * Significant change compared with control group by the definition of study.