成人加護病房鋸齒桿菌院內泌尿道感染的監測與處置; Surveillance and Management of Nosocomial Urinary Tract Infections by Serratia Marcescens in an Intensive Care Unit
32
0
0
全文
(2) APICU and those of nosocomial S. marcescens UTI in the hospital and in APICU were 2.15, 16.26, 0.31, and 6.69 episodes/1,000 patient-days, respectively (p<0.01). The infection rates of nosocomial UTI and of nosocomial S. marcescens UTI were not changed significantly through cleaning and disinfecting the APICU (17.5 vs. 19.9 episodes/1,000 patient-days, p=0.53; 8.7 vs. 6.3 episodes/1,000 patient-days, p=0.38, respectively). Seventeen S. marcescens isolates from urine samples of patients and five isolates from environment in APICU were analyzed by PFGE, which 3 different clones of S. marcescens were identified.. The infection rates of total and S. marcescenes UTI in APICU were significantly higher than those of hospital, which revealed significant urinary infection and S. marscescens infection occurring in APICU. The infection rates of nosocomial UTI in APICU were not changed despite closing wards and proper cleaning and disinfecion. The macrorestriction patterns of genomic DNA by PFGE revealed that there were clonal spreading of S. marscescens in patients and environments of APICU. Further delineation of the mode of transmission of nosocomial urinary tract infection is needed.. Key words: Serratia marcescens, nosocomial infection, pulsed-field gel electrophoresis, adult patient intensive care unit..
(3) INTRODUCTION. Urinary tract infections (UTIs) constitute the most common nosocomial infections in many hospitals, and contribute to considerable morbidity and mortality1.. Many UTIs are related with use of medical devices such as. indwelling catheters or invasive procedures of urogenital tract.. Serratia. marcescens is a well-known causative organism that may cause nosocomial urinary tract infection2, pneumonia3 , blood stream infection3, and soft tissues infection4, which often develops drug resistance rapidly that would cause a range of infections difficult to treat 5,6.. As a family of Enterobacteriaceae, S. marcescens is a Gram-negative bacilli that can be found in soil, water, foodstuff, animals, sewage , etc. Some of them, under feasible circumstances such as adequate oxygen supply, medium composition, and prompt temperature, have the ability to produce a red pigment called prodigiosin7,8,9. Pigmented S. marcescens, with considerable virulence to mice and cytotoxins production on Vero, CHO, Hep-2, and HeLa cells, was found to be cultured with low frequency and low infection rates in experienmented mice, different from those in non-pigmented strains 10.. Through an active surveillance system of nosocomial infections, we have found unordinary high infection rates of UTIs and those caused by S. marcescens in our APICU when compared with those of our hospital during the same surveillance period. In order to rule out an outbreak of UTIs caused by S. marcescens, we analyzed the infection rates of UTIs and the infections rates of UTI caused by S. marcescens in APICU and those in our hospital during an.
(4) 18-month study period. And we also examined the impacts of cleaning and disinfecting the APICU on the infection rates of UTIs and those of UTIs caused by S. marcescens in APICU. The infection rates of nosocomial infections (UTIs, respiratory tract infections – RTIs, blood stream infections – BSIs, and surgical site infection s– SSIs) during the period were also analyzed. For epidemiologic survey, we collected the S. marcescens isolates from urine cultures of infected patients and the cultures of environment screen to perform PFGE to identify the source of infection and to rule out clonal spreading in APICU.. MATERIALS AND METHODS. Setting. The Tung’s Taichung MetroHarbor Hospital, located in the Taichung County of Taiwan, is a 1,042-bed tertiary teaching hospital.. The APICU. locates at the west side of the ninth floor of the building and most of the patients are critical surgical patients who need intensive monitoring and treatment.. The neighborhoods are one medical ward and one medical. intensive care unit. The APICU contains 20 beds including one room with negative pressure, which can be used for isolation patients with air-borne disease such as tuberculosis.. Sinks are available at each bed.. Infection. control policy with standard precaution such gloves use and hand hygiene is strictly required..
(5) Surveillance Procedures. During the period 1 st April 2001 to 30th September 2002, the surveillance data of nosocomial infections were retrieved retrospectively from computer data base.. Patients were considered to acquire nosocomial infections. according to the standard definitions of nosocomial infections by Center for Disease Control and Prevention11.. The infection rates (represented with. incidence per 1,000 patient-day) of UTIs, RTIs, BSIs, SSIs, and other infections of the hospital were analyzed monthly. The infection rates of UTIs due to S. marcescens of the hospital and those of the APICU during the study period were also analyzed.. The demographic data of patients acquired. nosocomial UTIs in APICU, including sex, age, underlying diseases, reasons for admission to APICU, dates of admission and discharge, lengths of stay in APICU, duration of indwelling transurethral catheters use, major clinical manifestations, outcomes, bacterial isolates from urine specimens, and antimicrobial susceptibility test results of isolates were also reviewed.. Cleaning and Disinfection of the APICU and the Collection of Surveillance Data. After well discussion at the Infection Control Committee of the Tung’s Taichung MetroHarbor Hospital on 8th March 2002, the committers made the decision to close the APICU temporally (27th and 28th March 2002) for cleaning and disinfecting the APICU. 0.1% sodium hypochloride solution was used to wash the floor, tables, and the wall, and 70% alcohol solution was used to wash the surface of instrument such as EKG monitors, monitors and.
(6) keyboards of computers and ventilators, etc.. The urinals, the taps, and the tubes of ventilators were put into 0.5% sodium hypochloride solution for at least one hour and were cleaned with distilled water. The twenty sinks were washed with 0.5% sodium hypochloride solution. The APICU was reopened on 29th March 2002. The infection rates of nosocomial UTIs and those caused by S. marcescens in APICU within 6 months before cleaning and disinfection were compared with the same parameters of within 6 months after cleaning and disinfection.. Microbiologic Methods. Twenty sinks and six urinals in APICU were sampling for environmental screening and all five S. marcescens isolates were cultured from five of the twenty sinks and zero from the urinals. Twenty-two S. marcescens isolates, including 17 isolates from urine cultures of patients in APICU and five isolates from cultures of environment al sampling of sinks in APICU, were submitted for antibiogram typing and PFGE typing. The twenty-two isolates were initial identified of S. marcescens by traditional biochemistry methods (fermentation of lactose, sucrose, and glucose in triple sugar iron agar; positive response of citrate test; negative response of urease test; negative response of indole and indole pyruvic acid –IPA test and positive response of motility test; positive response of Voges-Proskauer – VP test; positive response of ornithine test; positive response of DNase test; and negative response of arabinose test). All isolates were confirmed by the automated API 20E system (API-BioMerieux, La Balme les Grottes, France). The susceptibility tests to antibiotics were checked at our Clinical Microbiology Laboratory with disc diffusion method,.
(7) according to the recommendation of the National Committee for Clinical Laboratory Standards (NCCLS) 12. The antibiotics choosing for Kerby-Bauer disk-diffusion tests of drug susceptibility were cefazolin (30 ug), cefoxitin (30 ug), cefotaxime (30 ug), ceftriaxone (30 ug), imipenem/cilastatin (10 ug), gentamicin (10 ug), amikacin (30 ug), ciprofloxacin (5 ug), ampicillin (10 ug), cefepime (30 ug), ampicillin/sulbactam (20 ug), amoxicillin/clavulanic acid (30 ug), and piperacillin/tazobactam (100 ug piperacillin/tazobactam 30 ug).. Molecular Method. The genomic DNA was prepared as previous reports13,14 . The 2% low melting agarose (Bio-Rad Laboratories, Richmond, Calif.) was put into SE buffer and was kept at 56 0C, and 2 cc mixed SE buffer was put into each of the two 75x12 mm test tubes and was kept at 4 0C. The bacterial suspension was prepared by harvesting the pure isolates of S. marcescens on culture plates and was adjust the bacterial concentration to 108 CFU/ml in saline-EDTA buffer (75 mM NaCl and 25 mM EDTA [PH7.5]), with a API densimeter (12-13%) (API-BioMerieux, La Balme les Grottes, France). Each 500 ul of bacterial suspension was loaded in the 1.5 cc eppendorfs kept in ice. Then put the eppendorfs on 40-56 0C for 3 minutes and add 500 ul low melting agarose to the eppendorf mixture. Put the 200 ul mixture of bacterial and low melting agarose into 2 molds (each 100 ul bacterial mixture was added into one mold) with temperature of 4 0C for 15 minutes to solidify a 100-ul plug mold. The DNA block was added with 2 ml of lysozyme buffer (10 mM Tris-HCl [pH7.6], 100 mM EDTA, 100 mM NaCl, 0.5% Brij58, 0.2% sodium deoxycholate, 0.5% sodium lauryl sarcosine, 20 ul of lysozyme [0.5 mg/ml]) at 37 0C for 2 hours..
(8) Following the step, the lysozyme buffer was replaced by 2 ml of proteolysis buffer (1% sodium lauryl sarosine, 0.5 M EDTA [pH 9.5], 20 ul of proteinase K [500 ug/ml; Sigma]), and this solution was incubated with gentle shaking at 56 0. C for 24 hours.. The DNA blocks were washed once for one hour at room temperature in 10 ml of Tris-EDTA buffer (10 mM Tris-HCl [pH 7.5], 10 mM EDTA) to eliminate the lysed bacterial material and to inactivate prteinase K activity. The DNA blocks were washed once for 30 to 60 minutes at 37 0C in Tris-EDTA buffer containing 1 mM phenylmethylsulfonyl fluoride (PMSF, Sigma). To remove PMSF, the DNA blocks were washed once in 3-4 ml of Tris-EDTA buffer at 4 0C for 30-60 minutes. The DNA blocks were cut into 1/3 to 1/2 in thickness gel slices (1 by 3.5 by 5.0 mm) and were dispensed to 5 ml distilled water at 4 0C for one hour, and the slices were incubated for 24 hours with reaction buffer containing 20 U of restriction endonuclease SpeI (Advanced Biotecnologies Ltd., London, United Kingdom).. Restriction fragments of. DNA, which were loaded in 1.0 to 1.2% SeaKem GTG agarose (FMC Bioproducts, Rockland, Maine) and running buffer, were separated by PFGE with CHEF-DRII apparatus (Bio-Rad Laboratories).. Electrophoresis was. performed at 6 V/cm and 14 0C. The run time was 22 hours with pulse time ramping from 5 to 25 seconds (initial time: 5 seconds, final time: 25 seconds). The lambda ladder (marker) used Staphylococcus aureus (NCTC 8325, England).. The pulse-field fingerprints were normalized with the molecular. weight marker and were computerized with dendrogram according to the similarities of bands distribution (GelCompar II software).. Isolates were. considered to be genetically indistinguishable or identical if their restriction.
(9) patterns had the same numbers of band and the corresponding bands were the same apparent sizes. Isolates were considered to be closely related if their PFGE patterns showed two to three band differences, consistent with a single genetic eve nt. Isolates were considered to be possibly related if their PFGE patterns showed four to six band differences, consistent with two independent genetic events. Isolates were unrelated if their PFGE patterns showed seven or more band differences, consistent with three or more independent genetic events15.. Isolates with 80% or more similarities in dendrogram were. considered indistinguishable or closely related.. Statistic Methods. Pearson’s χ2 test was used to analyzed the categorical variables, and when cell sizes were small, Fisher’s exact test was used.. Continuous. variables were analyzed by use of Student ’s t test. The p value of less than 0.05 was considered statistically significant.. All tests were 2-sided.. Computations were performed by use of SPSS version 4.0 (Chicago, IL. U.S.A.).. RESULTS. Nosocomial Surveillance Data. During the 18-month study period, the patient-hospitalization days per month of the Tung’s Taichung MetroHarbor Hospital ranged from 10,012 days.
(10) to 21,207 days, and the patient-hospitalization days per month of APICU ranged from 406 days to 588 days. Figure 1 reveals the relative proportions of urinary tract infections (UTIs), respiratory tract infections (RTIs), blood stream infections (BSIs), and surgical site infections (SSIs) by month during the study period. Most of the study period, UTIs were the leading cause of nosocomial infections (ranging from 34.4% to 55.8%), followed by BSIs (ranging from 17.4% to 53.8%), SSIs (ranging from 2.5% to 24.1%), and RTIs (ranging from 1.7% to 19.2%). Figure 2 reveals the average proportions of UTIs (47%), BSIs (29%), SSIs (11%), RTIs (8%), and other infections (5%) during the study period.. UTIs still accounted for the most common. nosocomial infections in our hospital. Figure 3 reveals the infection rates of UTIs and those caused by S. marcescens in our hospital and in APICU by month, respectively. This showed that the infection rates of UTIs and those caused by S. marcescens in APICU are higher than those of the hospital, respectively. Table 1 shows the comparisons between total number of UTIs, numbers of UTIs cause by S. marcescens, and the infection rates of hospital and those parameters of APICU.. The average infection rate of UTIs in. APICU was statistically higher than that in hospital (16.26 vs. 2.15 episodes per 1,000 patient-day, t value = 8.74, p < 0.001, 95% confidence interval [10.7, 17.4]). The same condition occurred in the comparisons between the average infection rate of UTIs caused by S. marcescens in APICU and that in hospital (6.69 vs. 0.31 episodes per 1,000 patient-day, t value = 5.91, p < 0.001, 95% confidence interval [4.4, 9.1]). Those results uncovered a fact that UTIs and UTIs caused by S. marcescens are more severe in APICU than those in the general hospital, which warranted epidemiologic and molecular surveys to rule out and intervention of the possible S. marcescens ourbreak in APICU. Figure.
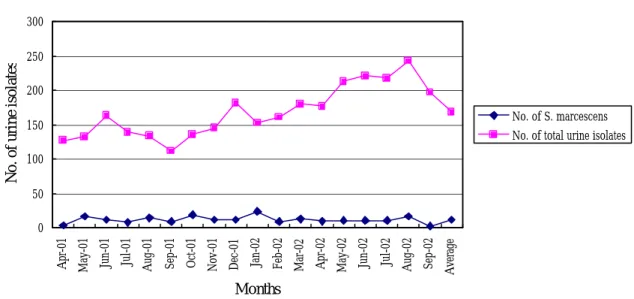
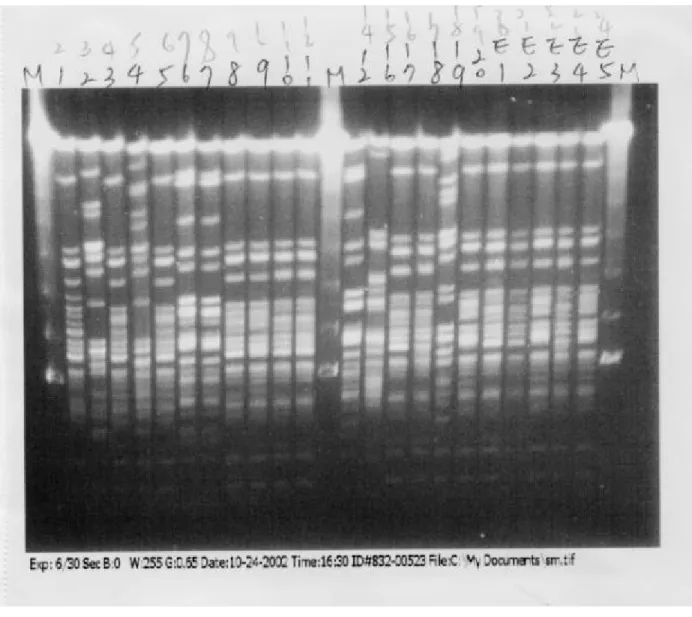
(11) 4 reveals the numbers of bacterial isolates and the numbers of S. marcescens isolates from urine specimens by month.. The average proportion of S.. marcescens in the total isolates from urine specimens was 7.5%, and the proportion was steady during the study period.. Surveillance Data before and after Cleaning and Disinfecting the APICU. Table 2 showed the impact of cleaning and disinfecting the APICU on the average nosocomial infection rate of UTIs and that caused by S. marcescens. The average nosocomial infection rates of UTIs within 6 months before and after cleaning and disinfection did not change significantly (17.5 vs. 19.9 per 1000 patient-day, t value 0.53, p = 0.61). The same condition occurred in the average nosocomial infection rates of UTIs caused by S. marcescens (8.7 vs. 6.3 per 1000 patient-day, t value 0.38, p > 0.8). The represented that only cleaning and disinfecting the enviroment of APICU with sodium hypochloride and alcohol solution is ineffective in reducing the infection rates of nosocomial UTIs in APICU.. Molecular Typing. The bands distribution patterns of DNA fragments were shown in Figure 5. The application of the PFGE technique was successful in typing of all twenty-two isolates including 5 environmental isolates but failed to show the molecular size of lambda markers (M). We had detected four different major PFGE patterns (A, B, C, and D), and each pattern had indistinguishable or close-related clones (similarities of PFGE pattern equal or more than 80%)..
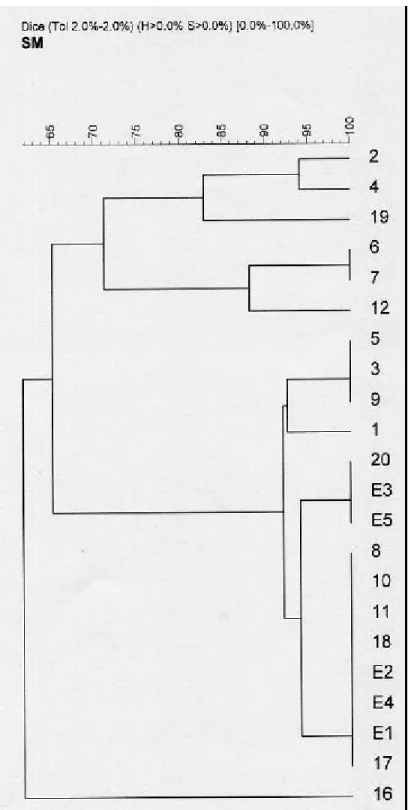
(12) Most clinical isolates (Isolate No. 1, 3, 5, 8, 9, 10, 11, 17, and 18) and all five environmental isolates (E1 to E5) were classified as closely-related clones (PFGE pattern A). Among these isolates, two environmental isolates (E3 and E5) and one clinical isolate (Isolate No. 20) were considered to be identical clones (PFGE pattern A3), while three clinical isolates (Isolate No. 3, 5, and 9) being considered to be identical clones (PFGE pattern A2). Five clinical isolates (Isolate No. 8, 10, 11, 17, and 18) and three environmental isolates (E1, E2, and E4) were classified as identical clones (PFGE pattern A4). Other six clinical isolates were classified of two different major PFGE patterns (C and D, respectively). The bands of DNA fragments of lambda ladder (marker, M) were not separated completely. Because the marker (S. aureus, NCTC 8325, England) was not freshly harvested, we supposed that failure of separating DNA fragments may be due to lysis of DNA of marker.. Antimicrobial Susceptibility Tests of S. marcescens Isolates. Table 3 listed the epidemiologic data, antimicrobial susceptibility tests, and the PFGE patterns of the S. marcescens isolates collected in this study. The S. marcescens isolates with four major different PFGE patterns had different patterns of antimicrobial susceptibility tests. Among these, some isolates with indistinguishable PFGE patterns had the same antimicrobial susceptibility tests (PFGE pattern A2 - Isolate No. 3, 5, and 9; PFGE pattern A4 – Isolate No. 8, 10, 11, 14, 15, E1, E2, E3, E4, and E5; PFGE pattern C1 – Isolate No. 6, 7, and 12). But some isolates did not behave same character (PFGE pattern B1 – Isolate No. 2, 4, and 16) and have different patterns of antimicrobial susceptibility tests despite with indistinguishable PFGE pattern..
(13) This means the phenotype (for example, antibiogram) of S. marcescens isolates in this study is not completely compatible with the genotype (e.g., PFGE).. DISCUSSION. Nosocomial urinary tract infections occur mostly with indwelling catheters and may cause considerable mortality of hospitalized patients. The attributable mortality of nosocomial UTI was estimated of 15.8% (12/76 patients) by Platt et al and the there was three-fold increase in mortality among hospitalized patients1.. During an 18-month study period, the average. proportion of nosocomial UTIs of our hospital was 47% and the mean infection rate of nosocomial UTIs was 2.50 episodes/1,000 patient-day, which did not exceed the average parameters of the Taiwan. But the percentage of UTIs in hospital-acquired infection of our hospital is higher than 35%, which was reported by National Nasocomial Infections Surveillance (NNIS) 16 system. That means hospital-acquired urinary tract infections at our hospital need to be alerted and to be resolved.. The average isolation rate of S. marcescens from positive urine cultures was 7.5% at our hospital, higher than those of the SENTRY study in Latin America reported by Gales et al. 17. (1.4% in 1998 and 1.9% in 1997,. respectively), the SENTRY study in North America reported by Jones et al 18 (0.71% in 1997), and the SENTRY study in Europe reported by Fluit et al 19 (1.12% in 1997 and 1998). The five most frequently isolated species from urinary specimens in North America were Escherichia coli (48.6%),.
(14) Enerococcus spp. (13.7), Klebsiella spp. (12.0%), Pseudomonas aeruginosa (6.2%), and Enterobacter spp. or Proteus mirabilis (3.8%, each) 18. Even in a SENTRY study of isolates from blood samples, S. marcescens was the 13th organism (1.2%) 20.. Surprising, the average infection rates of nosocomial. UTIs and of S. marcescens UTIs of APICU exceeded those of our hospital, with statistically significant difference (Table 1).. According to our study. (Figure 4), there was no significant increase of S. marcescens isolats from positive urine cultures. This may lead to the suspicion that there may be an outbreak of UTIs, especially those caused by S. marcescens, occurring in our APICU. So after a complete discussion, the Infection Control Committee decided to close the APICU for 2 days with complete cleaning and disinfection of the environments with sodium hypochloride and alcohol solution. Standard precaution with hand washing and glove use was instructed to the medical and nursing staffs. Even after cleaning and disinfection of APICU, the infection rates of nosocomial UTIs and those caused by S. marcescens did not reduce significantly. After full discussion between members of the Infection Control Committee, the possible explanations may be one or more of the following: not strictly adherence to infection control policy; loose adherence to hand hygiene and gloves wearing; patients crowding in APICU; and possible reservoirs in APICU who can transmitted the microorganisms asymptomatically through hands of staffs or surface of contaminated articles. We started to perform environmental sampling of sinks, urinals, tap water, and etc. for bacterial cultures.. Seventeen S. marcescens isolates from urine specimens of APICU. patients and five environmental isolates were evaluated by antibiogram and by molecular typing (PFGE) to rule out clonal spreading of S. marcescens in APICU..
(15) Serratia marcescens had been identified by epidemiologic and molecular surveys as the cause of outbreaks of many institutions and units of hospitals, through contamination of sinks and urinals21, electrocardiogram bulbs 22, hand-washes23, the door of incubator23, liquid medications 24, contaminated milk24,25, laryngoscope 26, hands of medical staffs26, theatre linen28, air conditioner filter30, enteral feed additive bottle31, and internal tocographs 31. After identification of the sources of infections or the reservoirs, interventions such as changing the disinfecting methods (e.g., thermal disinfection of contaminated milk bottles24 and adequate disinfection of theatre linen28), cohort isolation of infected patients from uninfected patients26,27, and education the staffs to adhere the infection control policy and hand hygiene and glove wearing26.. Most of our patients in APICU are surgical patients, and S.. marcescens infection may increase the morbidity and mortality. Brugge el al had performed a case-control study to evaluate the risk factors for acquisition of S. marcescens in a surgical intensive care unit29. After epidemiological and molecular surveys (random amplification of polymorphic DNA – RAPD), multiple different clones were demonstrated. Multivariate logistic regression analysis revealed body overweight, parenteral feeding, prolonged use of medical devices (more than 25 days), and mechanical ventilation are the independent risk factors for acquisition of S. marcescens in a surgical intensive care unit. Knowles et al reported that hematologic patients may colonize with S. marcescens and subsequently develop invasive infection during neutropenic period32. For resolving the nosocomial UTIs in APICU, the Infection Control Committee have required all staffs to strictly adhere to the infection control policy, to wear gloves while caring patients and to remove the glove after caring the patients, and to keep hand hygiene (frequent hand washing)..
(16) Genotyping of strains of bacteria with the same genus had been Phagetyping25,. performed.. polymorphic DNA (RAPD) 29, 14,18,23,24,26,27,30,33. serotyping29,32,. random. amplification. of. pulse-field gel electrophoresis (PFGE). , ribotyping18, plasmid typing28,10, restriction fragment length. polymorphism analysis (RFLP) 25, arbitrarily primed polymerase chain reaction (AP-PCR) 31, and PCR-RFLP 38 had been used with relative discriminative power in differentiate different clones of isolates. We used SpeI restriction endonuclease in PFGE for genotyping of the twenty-two isolates of S. marcescens and identified four major different PFGE patterns.. There are. several restriction endonucleases used in cutting S. marcescens DNA such as SpeI, XbaI, DraI, SspI, ApaI, Sma I, and SfiI.. SpeI was found to be the most. suitable restriction endonuclease for digestion of S. marcescens DNA in PFGE typing with good reproducibility and stability14. Experimental conditions are essential to the molecular typing. During this study, we harvested the marker not so fresh, which made the DNA fragments of the marker lyses and the resolution of fragments was poor.. Other S. marcescens isolates were. harvested freshly and the resolution of DNA fragments was good. We used the pulse time ranging from 5 to 25 seconds, thus the DNA fragments were separated promptly.. Prolonged terminal time will make the larger DNA. fragments separate widely, and the smaller DNA fragments do not show clear bands 34.. Failure to chill and wash the bacteria promptly will lead to. autodegradation of DNA fragments spontaneously and randomly due to endogenous nuclease35.. Peter YL et al had reported that plasmid profile analysis, restriction endonuclease analysis of plasmids, ribotyping, PFGE, and enterobacterial.
(17) repetitive intergenic consensus (ERIC) sequenced-based PCR (ERIC-PCR) all can demonstrate relative discriminatory power in identification of Shigella sonnei, within which PFGE and ERIC-PCR fingerprintings had the highest discriminatory power for discrimination of epidemiologically related isolates from epidemiologically unrelated strains 13.. PFGE was also considered to. have the highest degree of discriminatory power as the BOX fingerprinting with the BOX repetitive sequence in molecular typing of Streptococcus pneumoniae strain36.. Yoo JH et al also reported complete concordance. between infrequent-restriction-site PCR (IRS-PCR) and the PFGE in discriminating the isolates of S. marcescens37.. By comparing the results of antimicrobial susceptibility tests of S. marcescens isolates with those of PFGE, most indistinguishable isolates of S. marcescens have the same antimicrobial susceptibility patterns. But in PFGE pattern B1 isolates with the same genotype have different antimicrobial susceptibility pattern.. The result of this study revealed that phenotyping. isolates by antimicrobial susceptibility pattern may not be reliable. That is different from the results of Parvaz P et al 38 that antibiotic resistance patterns (antibiotype) can be considered as an additional marker to confirm the identity of strains classified in the same group by ribotyping, genotyping, or other typing methods. Additionally, most S. marcescens isolates had multiple drug resistance including resistance to most of the third and the fourth generations of cephalosporins and β-lactam/β-lactamase inhibitors except carbapenems.. CONCLUSION.
(18) Pulse-field gel electrophoresis is a reliable and reproducible tool in identification of isolates of nosocomial infections with high accuracy. Extensive epidemiologic survey of source of infections and adherence to infection control policy and hand hygiene should be emphasized..
(19) UTIs% RTIs% BSIs%. Ap r-0 1 Ju n-0 1 Au g-0 1 Oc t-0 1 De c-0 1 Fe b-0 2 Ap r-0 2 Ju n-0 2 Au g-0 2. Percent. 60 50 40 30 20 10 0. SSIs%. Month. Figure 1. Nosocomial infection rates during an 18-month period. UTIs: urinary tract infections, RTIs: respiratory tract infections, BSIs: blood stream infections, SSIs: surgical site infections..
(20) OTHER% 5% SSIs% 11%. UTIs% UTIs% 47%. RTIs% BSIs% SSIs%. BSIs% 29%. OTHER% RTIs% 8%. Figure 2. The average proportion of nosocomial infections. UTIs: urinary tract infections, RTIs: respiratory tract infections, BSIs: blood stream infections, SSIs: surgical site infections..
(21) UTI infection rate of hospital (1000 patient-day). 30 28. 24. APICU UTI infection rates (1000 patient-day) S. marcescens UTI infection rate of hospital (1000 patient-day). 22. APICU S. marcescens UTI infection rates (1000 patient-day). 26. 20 18 16 14 12 10 8 6 4 2 0 Apr01. May01. Jun01. Jul0 1. Aug0 1. Sep01. Oct01. Nov01. Dec0 1. Jan0 2. Feb02. Mar02. Apr02. M a y 0 2. Jun0 2. Jul02. Aug02. Sep02. Figure 3. The infection rates of nosocomial UTIs in APICU (blue line), of nosocomial UTIs caused by S. marcescens in APICU (red line), of nosocomial UTIs in the hospital (purple line), and of nosocomial UTIs caused by S. marcescens in the hospital (pink line) (episodes per 1,000 patient-day)..
(22) Monthly Frequency of Urine Isolates. No. of urine isolates. 300 250 200 No. of S. marcescens. 150. No. of total urine isolates. 100 50. Average. Sep-02. Aug-02. Jul-02. Jun-02. May-02. Apr-02. Mar-02. Jan-02. Feb-02. Dec-01. Oct-01. Nov-01. Sep-01. Aug-01. Jul-01. Jun-01. May-01. Apr-01. 0. Months. Figure 4. The numbers of total urine isolates and of the Serratia marcescens isolates from urine specimens..
(23) Figure 5. PFGE fingerprints of S. marcescens isolates from APICU and environmental screening after digestion with SpeI. Lane M, lambda ladder (S. aureus , NCTC 8325, England, Bio-Rad; molecular size maker); lanes 1-20, PFGE fingerprints of isolates 1to 20, respectively; lanes E1-E5, environmental screening isolates E1to E5, respectively..
(24) Figure 6. Analysis of the degrees of genetic relatedness (expressed as percentages) of individual strains performed by use of GelCompar II software..
(25) Items/No.(Infection rates). No.. Episodes of nosocomial UTIs of the hospital Episodes of nosocomial UTIs of APICU Episodes of S. marcescens UTIs of the hospital Episodes of S. marcescens UTIs of APICU Mean of infection rate of nosocomial UTIs of the hospital (episodes/1,000 patient-day) Mean of infection rate of nosocomial UTIs of APICU (episodes/1,000 patient-day) Mean of infection rate of S. marcescens UTIs of the hospital (episodes/1,000 patient-day) Mean of infection rate of S. marcescens UTIs of APICU (episodes/1,000 patient-day). 605. t value. p value. 95% C. I.. 146 83 60 2.15. 16.26. 8.74. < 0.001 (10.7, 17.4). 5.91. < 0.001. 0.31. 6.69. (4.4, 9.1). Table 1 The numbers and the infection rates of nosocomial urinary tract infections and urinary tract infections by S. marcescens of the hospital and APICU. (UTIs: urinary tract infections, APICU: adult patients intensive care unit)..
(26) Items/No.(Infection rates) Mean of infection rate of nosocomial UTIs of APICU (episodes/1,000 patient-day) Mean of infection rate of S. marcescens UTIs of APICU (episodes/1,000 patient-day). Before After t p disinfection disinfection value value 17.5. 19.9. 0.53. 0.61. 8.7. 6.3. 0.38 > 0.8. Table 2 The infection rates of nosocomial urinary tract infections and urinary tract infections by S. marcescens before and after cleaning and disinfection of APICU. (UTIs: urinary tract infections, APICU: adult patients intensive care unit)..
(27) References:. 1. Platt R, Polk B.F., Murdock B., Rosner B. (1982). Mortaity associated with nosocomial urinary-tract infection. N. Engl. J. Med. 307(11):637-642 2. Okuda T., Endo N., Osada Y., Zen-Yoji H. (1984). Outbreak of nosocomial urinary tract infection caused by Serratia marcescens. J of Clin. Microbiol. 20:691-695 3. Shaberg D.R., Alford R.H., Anderson R., Farmer III J.J., Melly M.A., Schaffner W. (1976). An outbreak of nosocomial infection due to multiply resistant Serratia marcescens: evidence of interhospital spread. J. Infect. Dis. 134:181-188 4. Yu, V.L. (1979). Serratia marcescens. Historical perspective and clinical review. N. Eng. J. Med. 300:887-893 5. Coria-Jimenez R, Ortiz-Torres. (1994). Aminoglycoside resistance patterns of Serratia marcescens strains of clinical origin. J. Epidem. Infect. 112:125-131 6. Hechler U., Van den Weghe M., Martin H.H., Frere J. M. (1989). Overproduced β-lactamase and the outer-membrane barrier as resistance factors in Serratia marcescens highly toβ-lactamase-stable-β-lactam antibiotics. J. Gen. Microbiol. 135:1275-1290 7. Hejazi A, Falkiner F.R. (1997). Serratia marcescens. J. Med. Microbiol. 46:903-912 8. Williams R.P., Gott C.L., Qadri S.M.H. (1971). Induction of pigmentation in nonproliferating cells of Serratia marcescens by addition of single amino acid. J. Bacteriol. 106:444-448 9. Williams R.P. (1973). Biosynthesis of prodigiosin, a secondary metabolite.
(28) of Serratia marcescens. Appl. Microbiol. 116:259-268 10. Carbonell G..V., Della Colleta H.H.M., Yano T., Darini A.L.C., Levy C.E., Fonseca B.A.L. (2000). Clinical relevance and virulence factors of pigmented Serratia marcescens. FEMS Immuno. Med. Microbiol. 28:143-149. 11. Garner J.S., Javis W.R., Emori T.G.. (1998). CDC definitions for nosocomial infection. Am. J. Infect. Control. 16:128-140 12. National Committee for Clinical Laboratory Standards. Performance Standards for Antimicrobial Disc Susceptibility Test. Approved Standard NCCLS Document M2-A6, Villanova: NCCLS 1997 13. Liu P.Y.F., Lan Y.J., Hu B.S., Shi Shyr Z.Y., Tasi W.S., Lin Y.H., Tseng C.Y. (1995). Analysis of clonal relationships among isolates of Shigella sonnei by different molecular typing methods. J. Clin. Microbiol. 33:1779-1783 14. Shi Z-Y., Liu P.Y- F., Lau Y-J., Lin Y-H., Hu B-S. (1997). Use of pulsed-field gel electrophoresis to investigate an outbreak of Serratia marcescens. J. Clin. Microbiol. 35:325-327 15. Tenover F. C., Arbeit R.D., Goering R.V., Mickelsen P.A., Murray B.E., Persing D.H., Swaminathan B. (1995). Interpreting chromosomal DNA restriction patterns produced by pulse-field gel electrophoresis: criteria for bacterial strain typing. J. Clin. Microbiol. 33:2233-2239 16. National Nasocomial Infections Surveillance (NNIS) report, data summary from October 1986-April 1996. Issued May 1996 (1996) American Journal of Infection Control 24:380-8 17. Gales A.C., Jones, R.N., Gordon K.A., Sader H.S., Wilke W. W, Beach M.L., Pfaller M.A., Doern G.V., and the SENTRY Study Group (Latin America). Activity and spectrum of 22 antimicrobial agents tested against.
(29) urinary tract infection pathogens in hospitalized patients in Latin America: report from the second year of the SENTRY Antimicrobial Surveillance Program, 1998. (2000). J. Antimicrobiol. Chemotherapy 45:295-303 18. Jones R.N., Kugler K.C., Pfaller M.A., Winokur P.L., and the SENTRY Surveillance Group, North America. Characteristics of pathogens causing urinary tract infections in hospitals in North America: results from SENTRY Antimicrobial Surveillance Program 1997. (1999). Diagn. Microbiol. Infect. Dis. 35:55-63 19. Fluit A.C., Schmitz F.J., Verhoef J., and the European SENTRY Participant Group. Frequency of isolation of pathogens from bloodstream, nosocomial pneumonia, skin and soft tissue, and urinary tract infections occurring in European patients (2001) Eur. J. Clin. Microbiol. Infect. Dis. 20:188-191 20. Pfaller M.A., Jones R.N., Doern G.V, Kugler K. and the SENTRY Participant Group. Bacterial Pathogens Isolated from patient with bloodstream infection: Frequencies of occurrence and antimicrobial susceptibility patterns from the SENTRY Antimicrobial Surveillance Program (United Stages and Canada, 1997). 1998. Antimicrob. Agents. Chemother. 1762-1770 21. Simor AE, Ramage L, Wilcox L, Bull SB, Bialkowska-Hobrzanska H. Molecular and epidemiologic study of multiresistant Serratia marcescens infections in a spinal cord injury rehabilitation unit. (1988). Infect. Control. 9:20-7 22. Sokalski SJ, Jewell MA, Asmus-Shillington AC, Mulcahy J, Segreti J. An outbreak of Serratia marcescens in 14 adult cardiac surgical patients associated with 12-lead electrocardiogram bulbs. (1992). Arch. Intern. Med. 152:841-4.
(30) 23. Jang TN, Fung CP, Yang TL, Shen SH, Huang CS, Lee SH. Use of pulsed-field gel electrophoresis to investigate an outbreak of Serratia marcescens infection in a neonatal intensive care unit. (2001). J. Hosp. Infect. 48:13-9 24. Fleisch F, Zimmermann-Baer U, Zbinden R, Bischoff G, Arlettaz R, Waldvogel K, Nadal D, Ruef C. Three consecutive outbreaks of Serratia marcescens in a neonatal intensive care unit. (2002). Clin. Infect. Dis. 15:767-73 25. Jones BL, Gorman LJ, Simpson J, Curran ET, McNamee S, Lucas C, Michie J, Platt DJ, Thakker B. An outbreak of Serratia marcescens in two neonatal intensive care units. (2000). J. Hosp. Infect. 46:314-9 26. Villari P, Crispino M, Salvadori A, Scarcella A. Molecular epidemiology of an outbreak of Serratia marcescens in a neonatal intensive care unit. (2001). Infect. Control. Hosp. Epidemiol. 22:630-4 27. Prasad GA, Jones PG, Michaels J, Garland JS, Shivpuri CR. Outbreak of Serratia marcescens infection in a neonatal intensive care unit. (2001). Infect. Control. Hosp. Epidemiol. 22:303-305 28. Esel D, Doganay M, Bozdemir N, Yildiz O, Tezcaner T, Sumerkan B, Aygen B, Selcuklu A. Polymicrobial ventriculitis and evaluation of an outbreak in a surgical intensive care unit due to inadequate sterilization. (2002). J. Hosp. Infect. 50:170-4 29. Hejazi A, Aucken HM, Falkiner FR. Epidemiology and susceptibility of Serratia marcescens in a large general hospital over an 8-year period. (2000). J. Hosp. Infect. 45:42-6 30. Peltroche-Llacsahuanga H, Lutticken R, Haase G. Temporally overlapping nosocomial outbreaks of Serratia marcescens infections: an unexpected.
(31) result revealed by pulsed-field gel electrophoresis. (1999). Infect. Control. Hosp. Epidemiol. 20:387-8 31. Berthelot P, Grattard F, Amerger C, Frery MC, Lucht F, Pozzetto B, Fargier P. Investigation of a nosocomial outbreak due to Serratia marcescens in a maternity hospital. (1999). Infect. Control. Hosp. Epidemiol. 20:233-6 32. Knowles S, Herra C, Devitt E, O'Brien A, Mulvihill E, McCann SR, Browne P, Kennedy MJ, Keane CT. An outbreak of multiply resistant Serratia marcescens: the importance of persistent carriage. (2000). Bone Marrow Transplant. 25:873-7 33. Troillet N, Carmeli Y, Venkataraman L, DeGirolami P, Samore MH. Epidemiological analysis of imipenem-resistant Serratia marcescens in hospitalized patients. (1999). J. Hosp. Infect. 42:37-43 34. Sader HS, Perl TM, Hollis RJ, Divishek D, Herwaldt LA, Jones RN. Nosocomial transmission of Serratia odorifera biogroup. 2: Case report demonstration by macrorestriction analysis of chromosomal DNA using pulsed-field gel electrophoresis. (1994). Infect. Control. Hosp. Epidemiol. 15:390-3 35. Maslow J.N., Slutsky A.M., Arbeit R.D. (1993). Application of pulsed-field gel electrophoresis to molecular epidemiology, p. 563-572. In Persing D.H., Smith T.F., Tenover F.C., and White T.J. (ed.), Diagnostic Microbiology, Washington, D.C. 36. Hermans PW, Sluijter M, Hoogenboezem T, Heersma H, van Belkum A, de Groot R. Comparative study of five different DNA fingerprint techniques for molecular typing of Streptococcus pneumoniae strains. (1995). J. Clin. Microbiol. 33:1606-12 37. Yoo JH, Choi JH, Shin WS, Huh DH, Cho YK, Kim KM, Kim MY, Kang.
(32) MW. Application of infrequent-restriction-site PCR to clinical isolates of Acinetobacter baumannii and Serratia marcescens. (1999). J. Clin. Microbiol. 37:3108-12 38. Parvaz P, Tille D, Meugnier H, Perraud M, Chevallier P, Ritter J, Fabry J,. Sepetjan M. A rapid and easy PCR-RFLP method for genotyping Serratia marcescens strains isolated in different hospital outbreaks and patient environments in the Lyon area, France. (2002). J. Hosp. Infect. 51:96-105.
(33)
數據



+5


相關文件
Stage 3 Exposed ⁄ necrotic bone in patients with pain, infection, and one or more of the following: exposed and necrotic bone extending beyond the region of alveolar bone
Despite prophylactic and empirical antifungal treatment, the emergence of breakthrough invasive fungal infections caused by theoretically sensitive organisms as well as
Salivary lithiasis is a condition characterized by the obstruction of salivary gland or its excretory duct by a calculus or sialolith associated with: swelling, pain, and
Teeth high in the ramus, condyle or at the lower border of the mandible may require an extra-oral approach. allows good exposure of the surgical site, more control over
The reported case describes morphological characteristics, clinical course, radiographic and histopathological features, and surgical therapy of an extrafollicular variant of AOT in
Table 1 Clinicopathological features of current and reported salivary duct carcinoma presenting within sinonasal tract (n = 9) *Clinical data incomplete to reliably rule out a
2006 UK National Guideline for the management of genital tract infection with Chlamydia trachomatis British Association for Sexual Health and HIV Clinical Effectiveness
In particular, if s = f(t) is the position function of a particle that moves along a straight line, then f ′(a) is the rate of change of the displacement s with respect to the
