Hypoaesthesia Occurs In Acute Whiplash Irrespective Of Pain and Disability Levels and the Presence of Sensory Hypersensitivity
Andy Chien, B.Phty (Hons)
PhD Candidate, Division of Physiotherapy
The University of Queensland QLD 4072 Australia Eli Eliav, DMD, PhD
University of Medicine and Dentistry New Jersey Newark, New Jersey, 07101, United States
Michele Sterling, PhD MPhty BPhty Grad Dip Manip Phty Associate Director
Centre of National Research on Disability and Rehabilitation Medicine (CONROD) The University of Queensland, Mayne Medical School
Herston Road, Herston QLD 4006 Australia &
Senior Lecturer, Division of Physiotherapy
The University of Queensland QLD 4072 Australia Corresponding Author:
Andy Chien
Tel: +61 7 3346 4791 (direct) Fax: +61 7 3346 4603
Abstract
Objectives: In contrast to the increasing knowledge of the sensory dysfunction involved in
chronic Whiplash Associated Disorders (WAD), the use of comprehensive Quantitative Sensory Testing (QST) in the acute stage of the condition is sparse. In this study we sought to investigate the presence of sensory hypoaesthesia in participants with acute whiplash injury.
Methods: Fifty-two volunteers within four weeks post a motor vehicle accident and 31
healthy asymptomatic volunteers were recruited for this study. We classified our cohort into either a “high-risk” (n=17; signs associated with poor recovery including Neck Disability Index scores >30, cold and mechanical hyperalgesia, heightened Brachial Plexus Provocation Test responses) or “low risk” group (without these signs). Detection thresholds to electrical, thermal and vibration stimuli measured in lower cervical nerve root innervation zones; psychological distress and posttraumatic stress symptoms were compared between the groups using MANCOVA.
Results: Both the high- and low -risk groups exhibited significant elevation in sensory
detection when compared to controls (p>0.05). There was no difference in detection thresholds between the two whiplash groups, except for electrical detection which was greater in the high risk group (p<0.05). Both groups were psychologically distressed.
Discussion: Our findings demonstrate generalised hypoesthesia in acute WAD suggesting
adaptive central nervous system processing mechanisms are involved, regardless of pain and disability. The elevated levels of psychological distress seen in both groups may also play a role.
Keywords: Acute whiplash, Sensory hypersensitivity, Sensory hypoaesthesia, Quantitative
1. Introduction
The heterogeneous nature of whiplash associated disorders (WAD) is emerging 37, 39, 46. There
is evidence to suggest that a subgroup of patients with chronic WAD present with generalised sensory hypersensitivity 7, 27, 43. The presence of these sensory disturbances have also been
reported to be associated with delayed recovery and persistent symptoms 16, 40. Augmented
central pain processing mechanisms 3, 7, 27 as well as possible peripheral nerve tissue
involvement 42 have been proposed as models to account for this phenomena, however, the
exact underlying mechanisms remain unclear.
The involvement of somatosensory system dysfunction in chronic WAD was further
demonstrated in a recent study utilizing a comprehensive Quantitative Sensory Testing (QST) protocol which included thermal, vibration and electrical stimulation 5. The results of that
study indicated that a combination of both pain (mechanical and cold) and detection threshold (heat and electrical) measures provided high sensitivity and specificity in discriminating the whiplash patients from asymptomatic controls. The widespread hypoaesthetic changes identified in chronic WAD have been shown to be similar to those found in patients with cervical radiculopathy 4. It was concluded that these results provided further evidence that
somatosensory disturbances are important features in the presentation of chronic WAD.
In contrast to the increasing knowledge of the sensory dysfunction involved in chronic WAD, the use of comprehensive QST in the acute stage of the condition is sparse. Kasch et al., 17
demonstrated mechanical hyperalgesia in acutely injured WAD participants. Sterling et al., 41
also found mechanical and cold hyperalgesia to be features that distinguished whiplash patients who reported higher levels of pain and disability to those with lesser symptoms. Some of these sensory abnormalities are predictors for poor functional recovery 16, 40 and may
be indicative of potential peripheral nerve injury 42. However, comprehensive QST with a
special focus on the detection thresholds examining the different subclasses of nerve fibres has not been used previously in an acute whiplash cohort.
In this study we sought to investigate the presence of hypoaesthesia (elevated detection thresholds) in participants with acute whiplash injury. QST has been previously shown to be a reliable tool to characterize the somatosensory phenotype of patients with different pain conditions 35. As we have previously demonstrated the use of QST as a valid tool to
characterise chronic WAD 5, 40, the main aim of the study was to compare the sensory
presentation (detection thresholds) of participants with features associated with poor recovery (higher pain and disability, sensory hypersensitivity) to those without these signs. We
hypothesized that participants with the presence of moderate/high levels of pain and disability and sensory hypersensitivity would also show elevated detection thresholds.
2. Materials and Methods
2.1 Participants
Fifty-two volunteers (20 males, 32 females; mean age 36.3 ± 13.1 years) with neck pain as a result of a motor vehicle accident and 31 healthy asymptomatic volunteers (6 males, 25 females; mean age 31.4 ± 8.9 years) were recruited for this study.
The whiplash subjects were recruited within 1 month of injury via hospital accident and emergency departments, primary care practices and from advertisement within radio and print media. Subjects were excluded if they experienced concussion, loss of consciousness or head injury as a result of the accident, if they reported previous history of neck or upper quadrant pain that required treatment and if they had been diagnosed with a psychiatric disorder.
The control group was recruited from the general community provided they had no
complaints of spinal, upper or lower limb pain and had never experienced trauma or injuries to the cervical spine, head, and upper quadrant or knee regions requiring medical treatment. The study was approved by the institutional medical research ethics committee. All the subjects were unpaid volunteers and all gave written informed consent before inclusion.
2.2 Pain Threshold Measures
o 2.2.1 Pressure pain thresholds (PPTs)
PPT’s were determined using a pressure algometer with a probe size of 1 cm2 and application
rate of 40 kPa/s (Somedic AB, Farsta, Sweden). Test sites included the articular pillars of C5/6, nerve trunk of the median nerve (bilaterally) at the anterior elbow and at a bilateral remote site (muscle belly of tibialis anterior). These sites were selected as they have previously shown to be affected in chronic whiplash 5, 42. Triplicate recording were taken at
each site and the mean values used for analysis. o 2.2.2 Cold pain thresholds
Thermotest (Somedic AB, Farsta, Sweden) was used to determine cold pain thresholds. The thermode was applied directly over the skin of mid-cervical region as well as over the dorsal aspect of the hand. The mean of three trials at each site was calculated for analysis. The testing procedure has been described in more detail in a previous study 5.
o 2.2.3 Brachial Plexus Provocation Test (BPPT)
The BPPT was performed in all groups. The BPPT 9 has been used and described previously
in studies of whiplash 5, 42. With the patient in a supine position, the test was performed in the
combined with wrist and finger extension, shoulder external rotation and elbow extension. Subjects were asked to indicate to the examiner during elbow extension when they first perceived pain anywhere along the tested arm. The angle of elbow extension was then measured and the subjects were also asked to indicate their pain experienced during the test on a 10cm visual analogue scale (VAS).
2.3 Detection Threshold measures o 2.3.1 Vibration thresholds (VTs)
A vibrometre (Somedic AB, Stockholm, Sweden) was used to supply mechanical stimulation to the hand. After three test stimuli were applied to the muscle belly of brachioradialis in order to familiarise the subject, readings were then taken over areas of the hand innervated by distal aspect of the C6 (palmar aspect of the 1st metacarpal), C7 (palmar aspect of 2nd
metacarpal) and C8 dermatomes (dorsum of the 5th metacarpal). We have previously shown these sites to be affected in chronic whiplash 5. Triplicate recordings were taken at each site
and the mean values used for analysis.
o 2.3.2 Thermal (hot, cold) detection thresholds (TDTs)
Incorporating the method of limits, the Thermotest (Somedic AB, Farsta, Sweden) with a 25x50mm thermode was used. Detection thresholds were measured over areas of the hand innervated by the C6 and 7 (dorsum over the 1st and 2nd metacarpal) and C8 (dorsum of the 5th
metacarpal) dermatomes. We have previously shown these sites to be affected in chronic whiplash 5. The temperature was preset to either increase or decrease at a rate of 1°C/sec from
a baseline of 30°C. Triplicate recordings were taken at each site and the mean values used for analysis.
A non-noxious method of electrocutaneous stimulation applied using The Neurometer CPT/C device (Neurotron., Baltimore, USA) was used in a method of limits procedure to allow determinations of Current Perception Threshold (CPT). Sites tested were those innervated by C5/6 (lateral elbow, inferior to elbow joint line), C7 (distal phalanx of index finger); C8 (distal phalanx of 5th digit) and Tibialis anterior as a remote site. We have previously shown
these sites, at the frequency of 250Hz, to be affected in chronic WAD . Triplicate recordings were taken at each site and the mean values used for analysis.
2.4 Questionnaires
Most likely as a consequence of persisting symptoms and disability, people with chronic WAD and other chronic neck pain conditions often show signs of psychological distress 22, 29.
As psychological distress has been found to be a predictor of poor outcome 40 and to account
for the potential influence of psychological distress on pain responses 33, 48, a series of
questionnaires were administrated to all participants prior to undertaking QST. All participants completed the Neck Disability Index (NDI) 50. Whiplash patients also
completed the General Health Questionnaire 28 (GHQ-28) 10 as a measure of general
psychological distress and the Impact of Events Scales (IES) 13 as a measure of posttraumatic
stress symptoms.
2.5 Procedure
In the initial assessment, all whiplash participants underwent a comprehensive physical examination by an experienced physiotherapist to ascertain their eligibility for inclusion into the study. The participants were deemed eligible if they met the criteria of WAD II38, that is
they have neck pain, tenderness on palpation and movement loss but without abnormal clinical neurological signs (muscle power, sensation and reflexes).
Separate examiners carried out the clinical examination and the QST measures and they were blind to the group allocation of the participants. The same examiners carried out their
respective testing for all of the participants to ensure consistency. The participants then completed the questionnaires and testing was performed in the following order: BPPT, PPTs, Cold pain thresholds, VTs, TDTs and CPTs.
2.6 Statistical analysis
The SPSS 15.00 statistical package for Windows was used for analyses. The Mann-Whitney test was firstly used to determine within subject side to side differences for all measures. This was done for both the control and the whiplash groups.
Based on the findings of Sterling et al., 40, participants with whiplash were classified into
either a “low risk” or a “high risk” group for poor recovery. Participants were required to fulfil the following criteria to be assigned into the high risk group: NDI score of greater than 30/100, and two out of the three of the following: cervical cold pain threshold of greater than 13°C, pressure pain threshold of less than 200kPa at the median nerve site and elbow
extension of less than 25° (from 180°) with the BPPT. The NDI score and cold pain threshold were chosen for their prognostic value of outcome following whiplash injury 40 whilst
lowered PPT at the median nerve site and heightened responses to the BPPT have also been shown to be present in those with poor recovery 44, 45.
Once the whiplash patients were classified into their respective groups, data was firstly analysed using descriptive statistics. A multi-variate analysis of covariance (MANCOVA) was then used to compare differences between the whiplash groups and the control group for
all of the QST measures, with age, gender and GHQ-28 total scores entered as covariates. Mann-Whitney test was also used to investigate for any significant differences in terms of the psychological profile between the two whiplash groups. Significance was set at p < 0.05.
3. Results
3.1 Participants
Based on the criteria described, 17 out of the 52 patients were assigned into the high risk group. This group consisted of 4 males and 13 females (mean age of 35.8 ± 14.1 years) with a mean NDI score of 48.6 (out of 100) ± 12.2 compared to 7 males and 28 females (mean age of 36.6 ± 12.2 years) with a mean NDI score of 22.5 ± 14.6 in the low risk group. The mean (SD) time post injury is 3.44 (±1.78) weeks. All of the participants with whiplash reported neck pain and 38% reported arm pain. Demographic and characteristic details of the participants are shown in table 1.
3.2 Within subjects side to side differences
No significant within subject side to side difference was found for any measures in both groups (all p>0.05). As a result, the mean of left and right side were calculated and used for further analysis.
The results of the descriptive statistics analysis are summarised in Table 2.
3.3 Detection threshold measures o 3.3.1 Vibration threshold
Significant differences were found between the three groups (p < 0.01) for all the test sites except the 1st metacarpal site. Both the whiplash groups demonstrated elevated detection
difference only between the control and the high-risk group (p < 0.05) but not with the low-risk group (p > 0.05). There was no significant difference between the two whiplash groups (figure 1).
o 3.3.2 Thermal detection threshold (hot, cold)
No significant differences were found for heat detection thresholds between the three groups (p > 0.05) at either site (figure 2).
Significant differences were found for cold detection thresholds between the three groups (p < 0.01). Post-hoc tests showed that both whiplash groups demonstrated significantly slower (delayed) cold detection thresholds when compared to controls at all sites (p < 0.05). This was more pronounced in the high-risk than the low-risk group but no significant difference was found between the two whiplash groups (p > 0.05) (figure 2).
o 3.3.3 Electrocutaneous stimulation thresholds
Significant differences were found between the three groups for all sites (p < 0.01). Post-hoc tests revealed significant differences between each of the three groups with the high risk group demonstrating the greatest elevation, followed by the low risk group compared to the controls for all of the hand sites (p < 0.05) (figure 3). Significantly elevated detection
thresholds were also found between the whiplash groups and the control group at the remote site of tibialis anterior (p < 0.01), however, no significant difference was found between the two whiplash groups (p = 0.17).
3.4 Psychological Distress
The low risk (27 ± 16) and the high risk (36 ± 17) groups both showed a total GHQ-28 scores above the normal threshold (23/24) 10 and a significant difference (p < 0.05) was found
between the two groups. When the GHQ-28 total scores were entered into the MANCOVA analysis as a covariate, group differences remained unchanged for all the QST measures with no interaction between group and GHQ-28 for any measure (p > 0.05).
No significant difference was found between the low risk (24 ± 15) and the high risk group (27 ± 19) for the IES scores. 48% (25 out of 52) of participants obtained IES scores of more than 26, which is indicative of a moderate or greater posttraumatic stress reaction 13.
4. Discussion
Based on previous findings that certain characteristics of WAD were predictors for the development of persistent symptoms and poor recovery 40, we classified our cohort of acute
whiplash injured participants into either a “low-risk” or “high-risk” group based on their signs of sensory hypersensitivity as well as self reported pain and disability ( NDI). The results of the current study indicate that hypoaesthetic changes are also present in the early acute post-injury stage. These changes are similar to those previously identified in chronic WAD 5. Both the low– and high-risk groups exhibited a similar pattern of elevation in
sensory detection, albeit the changes were more pronounced in the high-risk group. The hypoaesthetic changes occurred independently of psychological distress (GHQ-28) and these findings support the involvement of somatosensory system dysfunction in contributing to the presentation of acute WAD.
Both the low- and high-risk groups showed a reduced sensitivity to detect vibration, electrical and cold stimuli and to a lesser extent the warmth stimuli applied to the corresponding C6-8 dermatomes. Rolke et al., 34 maintain that reduced sensitivity (increased detection threshold
level) in response to QST is an indication of abnormalities in both large and small afferent nerve fibres and/or their central connections. Our whiplash cohort (WAD II) by definition,
presented without clinical neurological signs (that is no evidence of decreased muscle power or tendon reflexes). The processes underlying the hypoaesthetic changes are unclear but investigation of similar changes in other painful musculoskeletal conditions have suggested the involvement of both the central nervous system (CNS) pain processing mechanisms 49 as
well as the peripheral nervous system dysfunction 11, 12.
Recent studies investigating different clinical conditions with a similar hypoaesthetic presentation have suggested the involvement of the CNS. Tucker et al., 49 proposed that the
generalised hypoesthesia presentation found in patients with unilateral neuropathy (carpal tunnel syndrome) as well as those with upper limb pain of uncertain aetiology is consistent with a CNS physiological inhibitory model associated with chronic pain conditions. Apkarian et al., 2 suggested that prolonged nociceptive input into the CNS may cause an inhibitory
effect which in turn “dampens” the CNS’s ability to perceive and interpret afferent sensory input. Voerman et al., 51 also found an elevation of tactile detection thresholds in patients with
chronic cervicobrachialgia without clinical or diagnostic evidence of radiculopathy. These authors hypothesised that the altered detection thresholds were due to an adaptive mechanism of the CNS involving A-beta afferent input. Similar models have been proposed to explain the generalised hypoaesthesic presentation found in chronic patellofemoral pain syndrome 14
and painful osteoarthritic hips 19. It has been suggested that since different painful conditions
showed similar widespread elevation of detection thresholds, a common CNS disturbance may be involved regardless of the individual clinical condition 49. It is acknowledged that the
applicability of the CNS inhibitory mechanisms in whiplash injury in general is largely unexplored, however, Lo et al,23 discussed the role of spinal inhibitory mechanisms in
whiplash subjects and proposed some potential neurological dysfunction along different spinal cord localities. Alternative explanations involving central processes include those of
cortical reorganisation. Patterns of cortical reorganisation have been demonstrated in chronic pain conditions such as complex regional pain syndrome that parallel impaired tactile
discrimination and correlate with pain levels 30. Such phenomena may be a plausible
explanation for our findings where greater hypoaesthetic change was found in the acute whiplash group with higher levels of pain and disability.
The above mentioned studies all involved investigation of chronic musculoskeletal pain conditions 49, 51. To the best of our knowledge, our findings are the first to show the presence
of hypoesthesia in an acute clinical population. The exact role of central inhibitory mechanisms in the acute pain stage is unclear and the majority of the available data are extracted from experimental studies. These studies proposed that the nociceptive input associated with experimentally induced pain alter one’s perception of non-noxious
stimulation due to the interaction and modulation of the C-fibres on other afferent fibres 20, 24.
Activation of nociceptive receptors has also been suggested to inhibit cutaneous touch perception 47. Such findings suggest that the presence of a nociceptive input has the capacity
to alter one’s perception of non-noxious stimulation and the effect is immediate and long lasting. The fact that the hypoaesthetic changes were observed on the homologous contralateral side and far outlasted the period of induced pain, it has been proposed that a central component may be at play 47. There is no doubt that further studies are urgently
needed to ascertain the involvement of central inhibitory mechanisms in whiplash pain and studies examining the temporal development of these hypoaesthetic changes are currently underway.
Based on the classification system employed in the current study where the high-risk group was characterised by sensory hypersensitivity, our initial hypothesis was that the low-risk
group would present without hypoaesthesia. Surprisingly, although the changes were more pronounced in the high-risk group, no significant difference was found for vibration and thermal detection measures between the two whiplash groups. A possible explanation for the lack of difference between the two whiplash groups may be related to the central inhibition process discussed above. As stated previously, the presence of a continuous nociceptive input appears to play a major role in the initiation and maintenance of the physiological processes associated with the adaptive inhibitory mechanisms 2, 49. Indeed our ‘low-risk’ participants
reported mild to moderate levels of pain and disability (mean NDI of 22.5/100) (presumably from ongoing nociceptive input) and this may be adequate to maintain the physiological inhibitory processes. The more profound changes in the high risk group are consistent with studies of other musculoskeletal pain conditions where sensitivity to sensory stimuli was found to be correlated with intensity of the ongoing pain in the area 21. Furthermore, in
complex regional pain syndrome 31 and painful hip conditions 18, it has been found that the
reversal of sensorimotor impairment is associated with a decrease in pain. It would be interesting to investigate whether the hypopaesthetic changes found in our ‘low-risk’ group might return to normal levels when and if the symptoms reported by this group decrease.
Despite the apparent involvement of central nervous system pain processing mechanisms in WAD, it may be premature to disregard the possible involvement of peripheral mechanisms. The ‘high risk’ participants of our study demonstrated a significant increase in detection thresholds compared to controls and in most cases, the detection thresholds obtained from this group doubled those obtained from the healthy controls. The elevation in electrical detection thresholds seen in the ‘high risk’ group were comparable to those previously reported (and measured with the same equipment) in the affected limbs of patients with cervical radiculopathy 5. The presence of such pronounced sensory deficits resembles other
clinically established neuropathic conditions such as diabetes and chemical induced
polyneuropathy 1, 15 and suggests that a disruption to the peripheral sensory afferent system, at
least in the ‘high-risk’ group cannot be ruled out. Although WAD grade II does not present with an obvious nerve lesion, at least on clinical neurological examination, some data suggest more subtle nerve damage may be present 6, 8, 28. However contrary to this argument is that our
‘low risk’ group showed similar sensory disturbances. It would seem unlikely that peripheral nerve injury occurs in all following a whiplash injury, as most fully recover or have residual milder symptoms 32. Thus at this stage CNS processes would seem to be the most viable
explanation for the changes seen in this study but further investigation is warranted.
Acute posttraumatic stress reaction after whiplash injury has been suggested as an important factor in those with higher reported pain 25 and poor recovery 40. The high percentage (48%)
of patients in our study with IES scores indicative of a moderate or severe posttraumatic stress reaction is consistent with previous findings 41. Interestingly there was no difference in
IES scores between the high and low risk groups. It is possible that stress symptom responses can influence pain modulation within the CNS 26 and this could provide an explanation for the
hypoaesthetic changes seen in both our whiplash groups. However, despite elevated scores on psychological tests, group differences on QST remained significant when GHQ-28 scores were entered as covariates into the analysis. The lack of interaction between GHQ-28 and group differences may be due to the relatively small sample size of the groups but may be indicative that the changes in somatosensory function are not a direct result of psychological distress alone and potential underlying physiological changes must be considered 40.
It is acknowledge that compensation related factors may influence responses to QST 36.
compensation claim at the time of testing, it seems unlikely that the presence of hypoaesthesia found in this study is solely a result of compensation related factors. Evaluation of possible differences in sensory presentations between jurisdictions with different compensation schemes is currently underway and will hopefully be able to provide further insight on this issue in the future.
Our findings demonstrated generalised hypoesthesia in acute WAD regardless of pain and disability levels suggests that adaptive CNS processing mechanisms are involved following whiplash injury, irrespective of levels of pain/disability and sensory hypersensitivity. The elevated levels of psychological distress, particularly posttraumatic stress symptoms seen in both groups may also play a role.
Acknowledgements
This study was supported by a grant from the Australian Research Council, Motor Accidents Insurance Commission (Queensland), Suncorp General Insurance (Queensland) and the Physiotherapy Research Foundation (Australia). MS’s fellowship is funded by the National Health and Medical Research Council of Australia. AC’s scholarship is funded by the Sir Robert Menzies Foundation.
1. Abad F, Diaz-Gomez NM, Rodriguez I, et al. Subclinical pain and thermal sensory dysfunction in children and adolescents with Type 1 diabetes mellitus. Diabet Med. 2002;19:827-831.
2. Apkarian AV, Stea RA, Bolanowski SJ. Heat-induced pain diminishes vibrotactile perception: a touch gate. Somatosens Mot Res. 1994;11:259-267.
3. Banic B, Peterson F, Anderson O, et al. Evidence For Spinal Cord Hypersensitivity In Chronic Pain After Whiplash Injury and In fibromylagia. Pain. 2004;107:7-15.
4. Chien A, Eliav E, M S. Further Evidence Of A Neuropathic Component To Whiplash Pain: A Comparison With Cervical Radiculopathy Using Quantitative Sensory
Testing. Clin J Pain. 2008;in press.
5. Chien A, Sterling M, Eliav E. Hypoaesthesia occurs with sensory hypersensitivity in chronic whiplash - further evidence of neuropathic condition? Manual Therapy. 2008;EPub.
6. Chu J, Eun SS, Schwartz I. Quantitative motor unit action potentials (QMUAP) in whiplash patients with neck and upper-limb pain. Electromyogr Clin Neurophysiol. Sep-Oct 2005;45:323-328.
7. Curatolo M, Petersen-Felix S, Arendt-Nielsen L, et al. Central hypersensitivity in chronic pain after whiplash injury. Clin J Pain. Dec 2001;17:306-315.
8. Elliott J, Jull G, Noteboom JT, et al. Fatty infiltration in the cervical extensor muscles in persistent whiplash-associated disorders: a magnetic resonance imaging analysis.
Spine. Oct 15 2006;31:E847-855.
9. Elvey R. Brachial plexus tension test and the pathoanatomical origin of arm pain. In: Glasgow E, L(eds) T, eds. Aspects of manipulative therapy: Lincoln Institute of Health Sciences; 1979:105-110.
10. Goldberg DP, Hillier VF. Scaled Version of the General Health Questionnaire.
Psychol Med. 1979;9:139-145.
11. Greening J, Lynn B. Vibration sense in the upper limb in patients with repetitive strain injury and a group of at-risk office workers. Int Arch Occup Environ Health. Feb 1998;71:29-34.
12. Greening J, Lynn B, Leary R. Sensory and Autonomic Function In The Hands Of Patients With non-Specific Arm Pain (NSAP) and Asymptomatic office workers.
Pain. 2003;104:275-281.
13. Horowitz M, Wilner N, Alvarez W. Impact of Event Scale: a measure of subjective stress. Psychosom Med. May 1979;41:209-218.
14. Jensen R, Hystad T, Kvale A, et al. Quantitative sensory testing of patients with long lasting Patellofemoral pain syndrome. Eur J Pain. Aug 2007;11:665-676.
15. Jensen TS, Bach FW, Kastrup J, et al. Vibratory and Thermal Thresholds in Diabetics with and without Clinical Neuropathy. Acta Neurol Scand. Oct 1991;84:326-333.
16. Kasch H, Qerama E, Bach FW, et al. Reduced cold pressor pain tolerance in non-recovered whiplash patients: a 1-year prospective study. Eur J Pain. 2004;In Press, Corrected Proof.
17. Kasch H, Stengaard-Pedersen K, Arendt-Nielsen L, et al. Pain thresholds and tenderness in neck and head following acute whiplash injury: a prospective study.
Cephalalgia. Apr 2001;21:189-197.
18. Kosek E. [When pain goes its own ways. Mechanism-based diagnostics would make the correct choice of treatment for patients with chronic pain easier]. Lakartidningen. Apr 30 2003;100:1600-1602.
19. Kosek E, Ordeberg G. Abnormalities of somatosensory perception in patients with painful osteoarthritis normalize following successful treatment. Eur J Pain.
2000;4:229-238.
20. Lang S, Klein T, Magerl W, et al. Modality-specific sensory changes in humans after the induction of long-term potentiation (LTP) in cutaneous nociceptive pathways.
Pain. Apr 2007;128:254-263.
21. Leffler AS, Kosek E, Hansson P. The influence of pain intensity on somatosensory perception in patients suffering from subacute/chronic lateral epicondylalgia. Eur J
Pain. 2000;4:57-71.
22. Linton SJ. A review of psychological risk factors in back and neck pain. Spine. May 1 2000;25:1148-1156.
23. Lo YL, Tan YE, Fook-Chong S, et al. Role of spinal inhibitory mechanisms in whiplash injuries. J Neurotrauma. Jun 2007;24:1055-1067.
24. Magerl W, Treede RD. Secondary tactile hypoesthesia: a novel type of pain-induced somatosensory plasticity in human subjects. Neurosci Lett. May 6 2004;361:136-139.
25. Mayou R, Bryant B. Psychiatry of whiplash neck injury. Br J Psychiatry. May 2002;180:441-448.
26. McLean SA, Clauw DJ, Abelson JL, et al. The development of persistent pain and psychological morbidity after motor vehicle collision: integrating the potential role of stress response systems into a biopsychosocial model. Psychosom Med. Sep-Oct 2005;67:783-790.
27. Moog M, Quintner J, Hall T, et al. The late whiplash syndrome: a psychophysical study. European Journal of Pain-London. 2002;6:283-294.
28. Panjabi MM, Maak TG, Ivancic PC, et al. Dynamic intervertebral foramen narrowing during simulated rear impact. Spine. Mar 1 2006;31:E128-134.
29. Peebles JE, McWilliams LA, MacLennan R. A comparison of symptom checklist 90-Revised profiles from patients with chronic pain from whiplash and patients with other musculoskeletal injuries. Spine. Apr 1 2001;26:766-770.
30. Pleger B, Ragert P, Schwenkreis P, et al. Patterns of cortical reorganization parallel impaired tactile discrimination and pain intensity in complex regional pain syndrome.
Neuroimage. Aug 15 2006;32:503-510.
31. Pleger B, Tegenthoff M, Ragert P, et al. Sensorimotor retuning [corrected] in complex regional pain syndrome parallels pain reduction. Ann Neurol. Mar 2005;57:425-429.
32. Rebbeck T, Sindhusake D, Cameron ID, et al. A prospective cohort study of health outcomes following whiplash associated disorders in an Australian population. Inj
Prev. Apr 2006;12:93-98.
33. Rhudy JL, Meagher MW. Fear and anxiety: divergent effects on human pain thresholds. Pain. Jan 2000;84:65-75.
34. Rolke R, Baron R, Maier C, et al. Quantitative sensory testing in the German
Research Network on Neuropathic Pain (DFNS): standardized protocol and reference values. Pain. Aug 2006;123:231-243.
35. Rolke R, Magerl W, Campbell KA, et al. Quantitative sensory testing: a comprehensive protocol for clinical trials. Eur J Pain. Jan 2006;10:77-88.
36. Shy ME, Frohman EM, So YT, et al. Quantitative sensory testing: report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Neurology. Mar 25 2003;60:898-904.
37. Soderlund A, Denison E. Classification of patients with whiplash associated disorders (WAD): reliable and valid subgroups based on the Multidimensional Pain Inventory (MPI-S). Eur J Pain. Feb 2006;10:113-119.
38. Spitzer WO, Skovron ML, Salmi LR, et al. Scientific Monograph of the Quebec Task-Force on Whiplash-Associated Disorders - Redefining Whiplash and Its Management.
Spine. Apr 15 1995;20:S1-S73.
39. Sterling M. A proposed new classification system for whiplash associated disorders--implications for assessment and management. Man Ther. May 2004;9:60-70.
40. Sterling M, Jull G, Kenardy J. Physical and psychological factors maintain long-term predictive capacity post-whiplash injury. Pain. May 2006;122:102-108.
41. Sterling M, Jull G, Vicenzino B, et al. Characterization of acute whiplash-associated disorders. Spine. Jan 15 2004;29:182-188.
42. Sterling M, Jull G, Vicenzino B, et al. Sensory Hypersensitivity Occurs Soon After Whiplash Injury and Is Associated With Poor Recovery. Pain. 2003;104:509-517.
43. Sterling M, Jull G, Vicenzino B, et al. Physical and psychological factors predict outcome following whiplash injury. Pain. Mar 2005;114:141-148.
44. Sterling M, Treleaven J, Edwards SL, et al. Pressure pain thresholds in chronic whiplash associated disorder: further evidence of altered central pain processing.
Journal of Musculoskeletal Pain. 2002;10:69-81.
45. Sterling M, Treleaven J, Jull G. Responses to a clinical test of mechanical provocation of nerve tissue in whiplash associated disorder. Manual Therapy. May 2002;7:89-94.
46. Sterner Y, Gerdle B. Acute and chronic whiplash disorders--a review. J Rehabil Med. Sep 2004;36:193-209; quiz 210.
47. Stohler CS, Kowalski CJ, Lund JP. Muscle pain inhibits cutaneous touch perception.
Pain. Jun 2001;92:327-333.
48. Theorell T, Nordemar R, Michelsen H. Pain Thresholds During Standardized Psychological Stress in Relation to Perceived Psychosocial Work Situation. J
Psychosom Res. Apr 1993;37:299-305.
49. Tucker AT, White PD, Kosek E, et al. Comparison of vibration perception thresholds in individuals with diffuse upper limb pain and carpal tunnel syndrome. Pain. Feb 2007;127:263-269.
50. Vernon H, Mior S. The Neck Disability Index - a Study of Reliability and Validity. J
Manipulative Physiol Ther. Sep 1991;14:409-415.
51. Voerman VF, van Egmond J, Crul BJ. Elevated detection thresholds for mechanical stimuli in chronic pain patients: support for a central mechanism. Arch Phys Med
Table 1. The demographic and characteristics of participant groups
Group Number Age (years) (mean ± SD) Gender (% female) NDI (mean ±SD)
High-risk Group 17 35.8 ± 14.1 76% 48.6 ± 12.2
Low-risk Group 35 36.6 ± 12.2 80% 22.5 ± 14.6
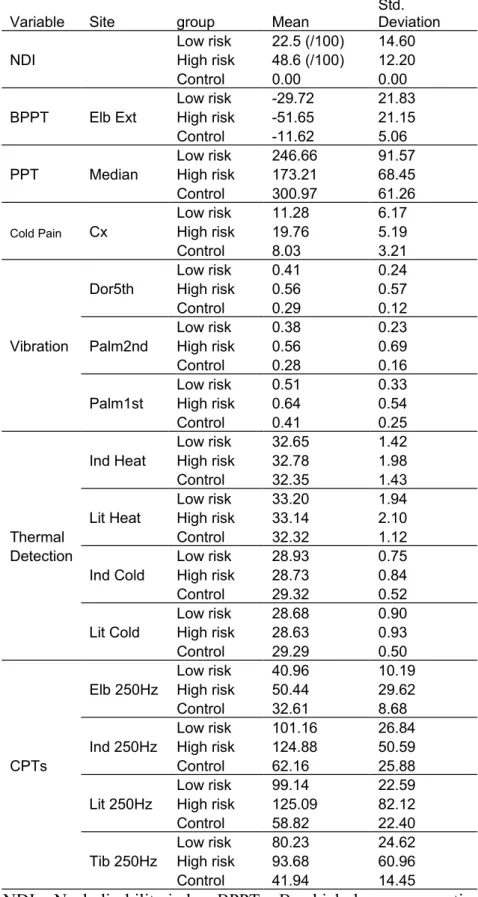
-Table 2. Mean (± SD) of each variable for each groups
Variable Site group Mean Std. Deviation
Low risk 22.5 (/100) 14.60
NDI High risk 48.6 (/100) 12.20
Control 0.00 0.00
Low risk -29.72 21.83
BPPT Elb Ext High risk -51.65 21.15
Control -11.62 5.06
Low risk 246.66 91.57
PPT Median High risk 173.21 68.45
Control 300.97 61.26
Low risk 11.28 6.17
Cold Pain Cx High risk 19.76 5.19
Control 8.03 3.21
Low risk 0.41 0.24
Dor5th High risk 0.56 0.57
Control 0.29 0.12
Low risk 0.38 0.23
Vibration Palm2nd High risk 0.56 0.69
Control 0.28 0.16
Low risk 0.51 0.33
Palm1st High risk 0.64 0.54
Control 0.41 0.25
Low risk 32.65 1.42
Ind Heat High risk 32.78 1.98
Control 32.35 1.43
Low risk 33.20 1.94
Lit Heat High risk 33.14 2.10
Thermal Control 32.32 1.12
Detection Low risk 28.93 0.75
Ind Cold High risk 28.73 0.84
Control 29.32 0.52
Low risk 28.68 0.90
Lit Cold High risk 28.63 0.93
Control 29.29 0.50
Low risk 40.96 10.19
Elb 250Hz High risk 50.44 29.62
Control 32.61 8.68
Low risk 101.16 26.84
Ind 250Hz High risk 124.88 50.59
CPTs Control 62.16 25.88
Low risk 99.14 22.59
Lit 250Hz High risk 125.09 82.12
Control 58.82 22.40
Low risk 80.23 24.62
Tib 250Hz High risk 93.68 60.96
Control 41.94 14.45
NDI = Neck disability index; BPPT = Brachial plexus provocation test; PPT = Pressure pain threshold, Median = median nerve; Dor5th = dorsal surface of the 5th metacarpal, Palm1st and
Palm2nd = palmar surface of the 1st and 2nd metacarpal; CPTs = current perception
Figure Legends
Figure 1. Mean (± SE) vibration thresholds in the control, low and high-risk whiplash groups. The stimulus was applied over areas of the hand innervated by C6 (Palm 1st), C7 (Palm 2nd)
and C8 dermatomes (Dor 5th).
Figure 2. Thermal (heat and cold) detection thresholds (means ± SE) in the control, low and high-risk whiplash groups. The stimulus was applied over the dorsum aspect of the hand corresponding to the C6 and 7 (Index: dorsum over the 2nd metacarpal) and C8 (5th: dorsum
of the 5th metacarpal) dermatomes.
Figure 3. Electrocutaneous detection thresholds at a frequency of 250Hz (means ± SE) in the control, low and high-risk whiplash groups. Sites tested were those innervated by C6 (lateral elbow, Elb), C7 (distal phalanx of index finger, Ind); C8 (distal phalanx of 5th digit, Lit) with