Epidemiological characteristics and risk factors of hepatocellular
carcinoma
CHIEN-JEN CHEN,* MING-WHEI YU*t AND YUN-FAN LIAWS
*Graduate Institute
ofEpidemiology and *Department
ofPublic Health, College
ofPublic Health, National
Taiwan University and $Liver Research Unit, Chang Gung Memorial Hospital, Taipei, Taiwan, Republic
ofChina
Abstract
Hepatocellular carcinoma (HCC) is one of the major cancers in the world. There is a striking variation in HCC incidence rates between various countries, with a highest-to-lowest ratio of 112.5 for males and 54.7 for females. The high-risk populations are clustered in sub-Saharan Africa and eastern Asia. The male-to-female ratio for HCC ranges from<
1 to 6.4 and mostly from 2 to 4. There exist significant variations in the incidence of HCC among different ethnic groups living in the same area and among migrants of the same ethnic groups living in different areas. The age curves of HCC are significantly different in various countries, suggesting variability in exposure to risk factors. Chronic carriers of hepatitis B and C viruses (HBV and HCV, respectively) have an increased risk of HCC. The relative and attributable HCC risk of HBV and HCV carrier status varies in different countries. There exists a synergistic interaction on HCC between the two viruses. Aflatoxin exposure, cigarette smoking, heavy alcohol consumption, low vegetable intake, inorganic arsenic ingestion, radioactive thorium dioxide exposure, iron overload and the use of oral contraceptives and anabolic steroids have been documented as HCC risk factors. Recent molecular epidemiological studies have shown that low serum retinol levels as well as elevated serum levels of testosterone, neu oncoprotein and aflatoxin B,-albumin adduct are associated with an increased HCC risk. There is a synergistic interaction on HCC between chronic HBV infection and aflatoxin exposure. Familial aggregation of HCC exists and a major susceptibility gene of HCC has been hypothesized. Patients of some genetic diseases are at an increased risk of HCC. The genetic polymorphisms of cytochrome P450 2E1 and 2D6 and arylamine N-acetyltransferase 2 are associated with the development of HCC. A dose- response relationship between aflatoxin exposure and HCC has been observed among chronic HBV carriers who have null genotypes of glutathione S-transferaseM1
orT1,
but not among those who have non-null genotypes. Human hepatocarcinogenesis is a multistage process with the involvement of a multifactorial aetiology. Gene-environment interactions are involved in the development of HCC in humans.Key
words: aetiology, epidemiology, gene-environment interaction, hepatocellular carcinoma.INTRODUCTION
Hepatocellular carcinoma (HCC) is a highly malignant disease with an extremely poor prognosis. It is a major cancer with approximately one million deaths annually in the world.' For the effective prevention of HCC, it is essential to explore risk factors associated with the disease. The occurrence of HCC varies in time, place and person. These epidemiological characteristics of a disease may provide clues for the formation of hypotheses regarding risk factors for the disease. The epidemiological hypotheses may be further elucidated through case-control and cohort studies. The present paper describes the epidemiological characteristics and
multiple risk factors of HCC with special emphasis on studies performed in Taiwan.
EPIDEMIOLOGICAL
CHARACTERISTICS
International and intranational variation
Based on the incidence data of liver cancer registered in different areas in the world,2 there was a striking difference of the age-adjusted incidence of liver cancer in different countries in 1983-87. As shown in Table 1, the ratio between the highest and lowest age-adjusted
Correspondence: Professor C-J Chen, Graduate Institute of Epidemiology, College of Public Health, National Taiwan University, 1 Jen-Ai Road Section 1, Taipei 10018, Taiwan, Republic of China. Email: < [email protected]>
Table 1 International comparison of age-adjusted inci- dence rates (100 000) of liver cancer
~ ~ ~~~~~
Country, region Male Female Ratio
Thailand, Khon Kaen China, Qidong Mali, Bamako Japan, Osaka Hong Kong Gambia Singapore (Chinese) Philippines, Manila Italy, Trieste Switzerland, Geneva France, Bas Rhin Spain, Basque County Peru, Trujillo Sweden
US, SEER (Black) UK, SE Scotland Germany, Saarland Canada
Australia, Victoria
US,
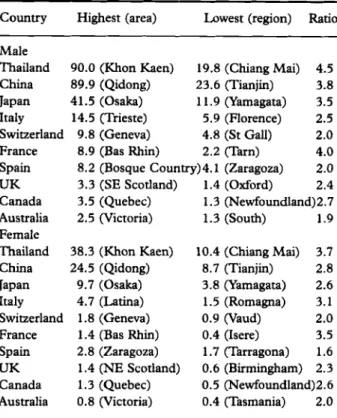
SEER (White) Iceland Paraguay, Ascucion Ireland, Southern Netherlands, Maastricht Highesdlowest ratio 90.0 89.9 47.9 41.5 39.2 36.0 26.8 23.7 14.5 9.8 8.9 8.2 7.4 4.5 4.2 3.3 4.0 2.6 2.5 2.4 2.4 1.1 1.1 0.8 112.5 38.3 24.5 21.4 9.7 9.6 12.1 7.0 8.0 2.5 1.8 1.4 2.6 5.1 2.6 1.4 1.2 1.6 1.0 0.8 1.1 1.7 1.5 1.1 0.7 54.7 2.4 3.7 2.2 4.3 4.1 3.0 3.8 3.0 5.8 5.4 6.4 3.2 1.5 1.7 3.0 2.8 2.5 2.6 3.1 2.2 1.4 0.7 1.1 1.1Table 2 Intranational variation of age-adjusted incidence rates (per 100 000) of liver cancer in selected counmes
Country Highest (area) Lowest (region) Ratio
Male
Thailand 90.0 (Khon Kaen) 19.8 (Chiang Mai) 4.5
China 89.9 (Qidong) 23.6 (Tianjin) 3.8
Japan 41.5 (Osaka) 11.9 (Yamagata) 3.5
Italy 14.5 (Trieste) 5.9 (Florence) 2.5
France 8.9 (Bas Rhin) 2.2 (Tarn) 4.0
Spain 8.2 (Bosque country)4.1 (Zaragoza) 2.0
UK 3.3 (SE Scotland) 1.4 (Oxford) 2.4
Canada 3.5 (Quebec) 1.3 (Newfoundland)2.7
Female
Thailand 38.3 (Khon Kaen) 10.4 (Chiang Mai) 3.7
China 24.5 (Qidong) 8.7 (Tianjin) 2.8
Japan 9.7 (Osaka) 3.8 (Yamagata) 2.6
Italy 4.7 (Latina) 1.5 (Romagna) 3.1
Switzerland 9.8 (Geneva) 4.8 (St Gall) 2.0
Australia 2.5 (Victoria) 1.3 (South) 1.9
Switzerland 1.8 (Geneva) 0.9 (Vaud) 2.0
France 1.4 (Bas Rhin) 0.4 (Isere) 3.5
Spain 2.8 (Zaragoza) 1.7 (Tarragona) 1.6
UK 1.4 (NE Scotland) 0.6 (Birmingham) 2.3
Canada 1.3 (Quebec) 0.5 (Newfoundland)2.6
Australia 0.8 (Victoria) 0.4 (Tasmania) 2.0
Data taken from Cancer Incidence in Five Continents, Voume
VI.2
Data taken from Cancer Incidence in Fzve Continents, Volume
VI.2
incidence rates in the world was 112.5 (90.0 1100 000 in Khon Kaen zrs 0.8 /lo0 000 in Maastricht) for males and 54.7 (38.31100000 in Khon h e n 'us 0.71100 000 in Maastricht) for females. The areas of highest liver cancer incidence rates are located in sub-Saharan Africa and eastern Asia, including Khon h e n , Qidong, Bamako, Osaka, Hong Kong, Gambia, Singapore and Manila. The significant difference in liver cancer incidence among various countries may be attributable to differences in their ethnic composition and natural and sociocultural environments. The male-to-female ratio of age-adjusted liver cancer incidence rates ranged from 0.7 (Ascucion, Paraguay) to 6.4 (Bas
Rhin,
France) but was mostly between 2 and 4. The gender difference may be due to discrepancies in the hepatitis B surface antigen (HBsAg) carrier rate, lifestyles, occupational exposure and hormone status between males and females.In addition to the significant international variation, there were also significant intranational differences in age-adjusted incidence rates of HCC.2 In the 10 countries included in Table 2, the ratios between highest and lowest age-adjusted incidence rates within the countries ranged from 1.9 to 4.5 for males and from
1.6 to 3.7 for females. The highest ratio was observed in Thailand for both males and females. This discrepancy suggests that host susceptibility and/or
exposures to risk factors may be different in different areas of the same country. For example, the strikingly high mortality rate among residents in the Penghu Islets and the endemic area of blackfoot disease in Taiwan may be attributable to heavy exposure to aflatoxin and ingested inorganic arsenic, re~pectively.~
Ethnic and migrant variation
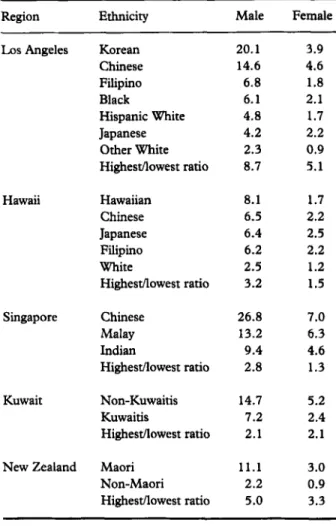
T h e difference in incidence rates of a given disease among different ethnic groups living in the same area suggests that specific ethnic background, either genetic or cultural, may play a more important role in the determination of the disease than common living environments shared by various ethnic groups. Table 3
shows the ethnic variation in age-adjusted incidence rates of liver cancer in L o s Angeles, Hawaii, Singapore, Kuwait and New Zealand.2 T h e ethnic difference was more striking in L o s Angeles and New Zealand than in the other three areas. The highest-to-lowest ratio was 8.7 for males and 5.1 for females in Los Angeles and 5.0 for males and 3.3 for females in New Zealand. There was a significant difference in age-adjusted liver cancer incidence rates among Chinese, Filipinos and Japanese in Los Angeles, but not in Hawaii.
T h e difference in incidence rates of a given disease among migrants of the same ethnic group living in different areas suggests that environmental factors rather
Table 3 Ethnic difference in age-adjusted incidence rates (per 100 000) of liver cancer
Region Ethnicity Male Female
LAX Angeles Hawaii Singapore Kuwait New Zealand Korean Chinese Filipino Black Hispanic White Japanese Other White Highestllowest ratio Hawaiian Chinese Japanese Filipino White Highestllowest ratio Chinese Malay Indian Highestnowest ratio Non-Kuwaitis Kuwaitis Highestnowest ratio Maori Non-Maori Highesdlowest ratio 20.1 14.6 6.8 6.1 4.8 4.2 2.3 8.7 8.1 6.5 6.4 6.2 2.5 3.2 26.8 13.2 9.4 2.8 14.7 7.2 2.1 11.1 2.2 5.0 3.9 4.6 1.8 2.1 1.7 2.2 0.9 5.1 1.7 2.2 2.5 2.2 1.2 1.5 7.0 6.3 4.6 1.3 5.2 2.4 2.1 3.0 0.9 3.3
Data taken from Cancer Incidence in Five Continenu, Elume VI.2
than ethnic background may play a major role in the determination of the disease. Table 4 illustrates migrant variations in age-adjusted incidence rates of liver cancer for Chinese, Japanese, Filipinos and Jewish people.2 The highest-to-lowest ratio among Chinese was 13.8 for
males and 11.1 for females. Migrants living in Los
Angeles and Hawaii had a lower liver cancer incidence rate than those of the same ethnic group living in Asia. Jewish people born in Africa or Asia had the highest incidence of liver cancer compared with those who were born in Europe, America or Israel, exhibiting ratios of
1.7 for males and 3.5 for females. The migrant difference was observed for both males and females. The ethnic and migrant variation in age-adjusted incidence rates of liver cancer suggests that both ethnic and environmental factors are important determinants.
Temporal variation
Based on the liver cancer incidence rates reported by the International Agency for Research on Cancer,2>& the secular trend of age-adjusted incidence rates of liver
Table 4 Migrant comparison of age-adjusted incidence rates (per 100 000) of liver cancer
Ethnicity Region* Male Female
Chinese Japanese Filipino Jews China, Qidong Hong Kong China, Shanghai Singapore China, Tianjin L o s Angeles Hawaii Highestflowest ratio Osaka Hiroshima Yamagata Hawaii L o s Angeles Highestllowest ratio Manila Rizal Los Angeles Hawaii Highestllowest ratio Africa or Asia Europe or America Israel Highesdlowest ratio 89.9 39.2 30.6 26.8 23.6 14.6 6.5 13.8 41.5 28.2 11.9 6.4 4.2 10.0 23.7 20.7 6.8 6.2 3.8 3.1 2.7 1.8 1.7 24.5 9.6 10.7 7.0 8.7 4.6 2.2 11.1 9.7 7.5 3.8 2.5 2.2 4.4 8.0 8.3 1.8 2.2 4.4 1.4 1.1 0.4 3.5
*Living areas for Chinese, Japanese and Filipino; birth Data taken from Cancer Incidence in Five Continents, klume areas for Jews.
w.
*
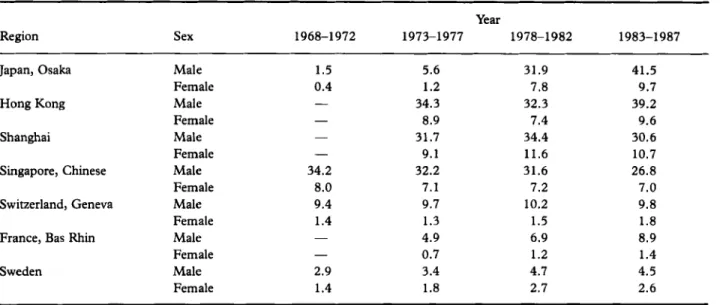
cancer was quite different in different areas. As shown in Table 5, the liver cancer incidence rates in Osaka, Japan, increased rapidly from 1.5 to 41.5 1100 000 for males and from 0.4 to 9.7 /lo0 000 for
females from 1968 to 1987. The trend of an increase in
the incidence of liver cancer was consistent with that reported previously.’ The incidence rates of liver cancer in males and females in Hong Kong, Sweden and Bas Rhin, France, increased steadily, albeit showing a lesser
increase, during the same period of The
increase in incidence rates may be attributable to either an improvement in diagnosis or an increased exposure to
risk
factors. While the age-adjusted liver cancer incidence rates in Shanghai and Geneva remained almost unchanged, those in Singapore decreased significantly for males, from 34.2 to 26.8 /lo0 000, andalso for females, from 8.0 to 7.0 /lo0 000. The decrease
in incidence rates may be due to the decrease in exposures to
risk factors.
An eight-fold increase in the incidence ofHCC
has been reported in Florence, Italy from 1958 to 1982; but a constant mortality rate fromprimary liver cancer was observed in England and Wales from 1975 to 1992.9 The trend of increasing mortality
Table 5 Secular trend of age-adjusted incidence rates (per 100 000) in selected regions, 1968-1987
Region Sex
Year
1968-1972 1973-1977 1978-1982 1983-1987
Japan, Osaka Male 1.5 5.6 31.9 41.5
Female 0.4 1.2 7.8 9.7
Hong Kong Male - 34.3 32.3 39.2
Female - 8.9 7.4 9.6
Shanghai Male - 31.7 34.4 30.6
Female - 9.1 11.6 10.7
Singapore, Chinese Male 34.2 32.2 31.6 26.8
Female 8.0 7.1 7.2 7.0
Switzerland, Geneva Male 9.4 9.7 10.2 9.8
Female 1.4 1.3 1.5 1.8
France, Bas Rhin Male - 4.9 6.9 8.9
Female - 0.7 1.2 1.4
Sweden Male 2.9 3.4 4.7 4.5
Female 1.4 1.8 2.7 2.6
Data taken from Cancer Incidence in Five Continents, Volume l l I - V I . 2 * ~
Table 6
100 000) of liver cancer in selected regions
Comparison of age-specific incidence rates (per
Age Qidong Khon Bamako Osaka Hong Gambia
Kaen Kong 1&14 20-24 25-29 30-34 35-39 40-44 45-49 50-54 55-59 60-64 65-69 70-74 75-79 ASR 15-19 0.3 > 1.1 > 7.4 > 40.4 > 114.1 > 172.3 > 211.2> 244.1 > 221.8< 267.6 < 206.0 < 207.2 < 149.6 < 133.3 < 89.9 0.0 0.4 1
.o
6.4 16.2 35.6 70.5 125.4 250.0 373.6 404.3 427.9 482.5 387.1 90.0 1.7 > 4.8 > 6.8 > 17.1 > 28.6 > 58.1 > 78.5 > 108.3 > 99.0 < 117.1 < 184.7 < 109.7 < 306.1 > 133.1 < 47.9 0.2 0.1 0.3 0.6 1.6 5.5 14.4 33.4 109.2 181.1 217.1 234.7 246.3 237.1 41.5 0.9< 1.5 1.1 < 2.0 1.7< 7.4 5.0< 28.1 1 2 . M 38.6 20.5< 44.2 46.7< 55.8 66.7< 94.3 93.1 > 58.2 123.6Z 84.3 155.1> 78.8 181.7> 64.8 196.8 - 206.1 - 39.2 36.0 ~ASR, age-adjusted rate.
Data taken from Cancer Incidence in Five Continents, Volume v1.2
rates from liver cancer in Taiwan was more striking in males than in females.IO This gender difference in a secular trend suggests that risk factors other than the improvement in HCC diagnosis may play important roles in the development of HCC in Taiwan.
Age variation
Table 6 shows the age-specific incidence rates of liver cancer in males in six select areas.2 Despite the fact that
the age-adjusted incidence rate of liver cancer was quite similar in Khon Kaen and in Qidong, the current age curves of liver cancer incidence rates were different. The incidence rates of liver cancer for age groups < 50 years were higher in Qidong than in Khon Kaen, while the incidence rates of people 2 50 years of age were lower in Qidong than in Khon Kaen. This seems to suggest that the liver cancer risk factors in the two areas may be different; the exposure to risk factors occurred earlier in Qidong than in Khon Kaen or the induction period of liver cancer may be longer in Khon Kaen than in Qidong. Similar contrasts are shown in Table 6 for Bamako, Hong Kong, Osaka and Gambia with lower rates for those people below 50 years of age and higher rates for those 50 years or older in the two Asian areas than in the two African areas.
RISK
FACTORS
Hepatitis viruses
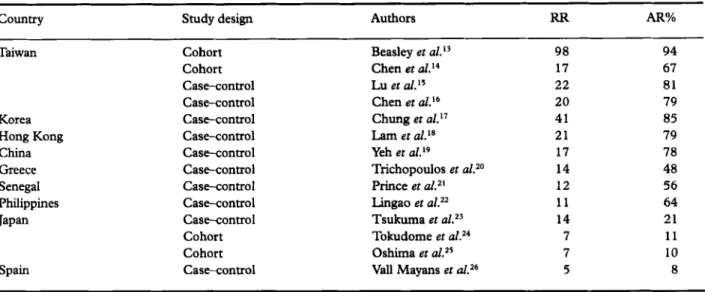
Chronic infections of both hepatitis B and C viruses (HBV and HCV) are important risk factors of HCC in the world.”,12 However, the relative risk (RR) and the population attributable risk percentage
(AR%)
for chronic HBV infection varied in different areas, as shown in Table 7.13-26 The RR for the carrier status of HBV surface antigen (HBsAg) ranged significantly from 5 in Spain to more than 20 in Taiwan, Korea and Hong Kong. The AR% for HBsAg carrier status also had a wide range from less than 10% in Spain to more than 70% in Taiwan, Korea, Hong Kong and China (Table 7). The difference in RR and AR% implies that the prevalence of HCC risk factors other than HBsAg carrier status may be different in these areas. The existence of other independent risk factors may reduce the RR and AR% of HBsAg carrier status. The carrier status of HBV e antigen (HBeAg) was also associatedTable 7 Relative risk
(RR)
and population attributable risk percentage(AR%)
of developing hepatocellular carcinoma for hepatitis B surface antigen carrier statuscounny
~~
Study design Authors
RR
AR%~~ Taiwan Korea Hong Kong China Greece Senegal Philippines Japan Spain Cohort Cohort Case-control Case-control Case-control Case-control Case-control Case-control Case-control Case-control Case-control Cohort Cohort Case-control Beasley et aL13 Chen et al.I4 Lu et d.I5 Chen et al.I6 98 94 17 67 22 81 20 79 Chung et al.I7 41 85 Lam et a1.I8 21 79 Yeh et a2.I9 17 78 Trichopoulos et aLZo 14 48 Prince et aL2I 12 56 Lingao et aLZ2 11 64 Tsukuma et 14 21 Tokudome et aLz4 7 11 Oshima et al.25 7 10
Val1 Mayans et aLZ6 5 8
Table 8 Relative risk (RR) and population attributable risk percentage (AR%) of developing hepatocellular carcinoma for anti-HCV seropositivity
country Study design Authors
RR
AR%Japan USA Spain South Mica Taiwan Greece Senegal Mozambique
Case vs blood donor Case-control Case vs blood donor Case-control Case vs blood donor Case vs blood donor Case-control Case vs blood donor Case-control Case-control Case-control Case-control Case-control Watanabe et aLZ7 Tanaka et aLZ8 Hasan et d.29 Di Bisceglie et aL30 Vargas et aL3’ Bruk et ~ 1 . ’ ~ Kew et al.33 Chen et ~ 2 . ’ ~ Chuang et al.35 Yu et ~ 2 . ’ ~ Zavitsanos et a2. 37 Coursaget et al.38 Dazza et al.39 218 52 134 7 116 38 62 37 33 24 10 6 1 69 60 50 11 53 73 29 25 17 9 12 3 < 1
with an increased risk of HCC among chronic HBsAg carriers. In a recent case-control study, the RR of developing HCC was 17.9 for carriers of only HBsAg and 64.7 for carriers of both HBsAg and HBeAg compared with non-carriers as the referent.16
Several case series, case-control and cohort studies have shown significant associations between HCV
infection and HCC risk.2747 The
RR
for theseropositivity of antibodies against HCV (anti-HCV) was much higher in case series studies than those in case-control studies, as shown in Table 8. This may be due to the choice of healthy blood donors who may have lower anti-HCV prevalence than the general population as the comparison group. The
RR
estimated from case-control and cohort studies was as high as 62in South Africa and 52 in Japan, but as low as 1.1 in Mozambique (”able 8). The AR% for anti-HCV ranged from less than 1% in Mozambique to 60% in Japan (Table 8). Similarly, the wide variation in RR and AR% implies that the importance of H C C risk factors other than anti-HCV seropositivity may be different in these areas.
In areas where chronic HBV and HCV infections are both prevalent. but not correlated, there may exist mutual confounding effects on HCC between HBV and HCV. The
RR
for chronic HBV infection will be severely underestimated if no adjustment for HCV infection is made and vice versa.41 Furthermore, recent case-control and cohort studies have documented the synergistic effects on H C C between chronic HBV andTable 9 Interactive effect on hepatocellular carcinoma between chronic hepatitis B and C viruses infection HBsAdAnti-HCV seropositivity
Country Study design Authors -I- 4
+
+
l- +I+Taiwan Case-control Case-control Case-control Case-control Cohort USA Case-control Greece Case-control Italy Case-control Vietnam Case-control Japan Case-control Yu et al.36 Chuang et ai.35 Tsai et aL40 Sun et al." Chang et al.42 Yu et aL4' Kalamani et al.44 Stroffolini et al.45 Cordier et Tanaka et al.47 1.0 1
.o
1.o
1.o
1.o
1.o
1.o
1.o
1.o
1.o
15.6 27.1 92.0 4.0 34.0 4.8 11.5 21.3 36.4 339.6 22.1 14.0 29.6 24.6 44.6 4.4 4.5 13.3 76.1 293.7 m 40.1 96.0 m m m 74.4 77.0*
WHBsAg, hepatitis B surface antigen.
*Neither cases nor controls were seropositive for both HBsAg and anti-HCV.
Table 10 Selected studies on association between aflatoxin exposure and risk of hepatocellular carcinoma
country Study design Authors
(Aflatoxin present)
Major findings
Mozambique and South Africa Ecological (8 districts) Swaziland Ecological (10 regions) Kenya Ecological (9 districts) China Ecological (Guanxi) Ecological (49 areas) Cohort (Shanghai) Ecological (8 areas) Case-control Case-control (7 areas) Cohort (Taipei) (Penghu) Taiwan
Van Rensburg et a1.48 Peers et al.49 Autrup et aL50 Yeh et aL5' Campbell et ~ 1 . ~ ~ Ross et al.53 Hatch et ~ 1 . ~ ~ Chen et aLS5 Wang et Chen et aL5' r = 0.64*(male), r = 0.71*(female) (Food sampling) Significant association (Food sampling) r = 0.75* (Bantu people) (Urinary level) r = 1 .OO* (Food sampling) r=0.17+ (Urinary level) RR= 3.8* (Urinary level) r = 0.29*(male), r = 0.17(female) (Urinary level) RR= 5.5*
(Albumin adduct level)
RR= 5.5* (Urinary level)
RR = 2.8** (Albumin adduct level) Dose-response relation*
(Albumin adduct level) *P< 0.05; **0.05 < P < 0.10; t, not significant; RR, relative risk.
HCV infections, as shown in Table 9.35336340-47 T h e
synergistic interaction between chronic HBV and HCV infections was observed in all but one study.4o
Aflatoxin
exposureIn a cohort study, the traditional Chinese vegetarian diet has been associated with an increased risk of HCC.I4 This
may result from the high consumption of fermented soy beans and their products, which may be contaminated with mycotoxins. Early case-control studies failed to find
significant associations between human HCC and afiatoxin e x p o s ~ r e . * ~ J ~ J ~ This may be due to the limitation of using dietary questionnaires to assess exposure to aflatoxin. T h e association between aflatoxin and H C C has been documented in several ecological, case-control and cohort studies using food sampling or biomarkers to quantify aflatoxin exposure, as shown in
Table 1 0.4E57 Statistically sigdicant correlations between dietary aflatoxin exposure and H C C mortality or morbidity were observed in all ecological studies performed in Mozambique,48 South Africa,“* Swaziland49 and China.51 Ecological correlation between urinary
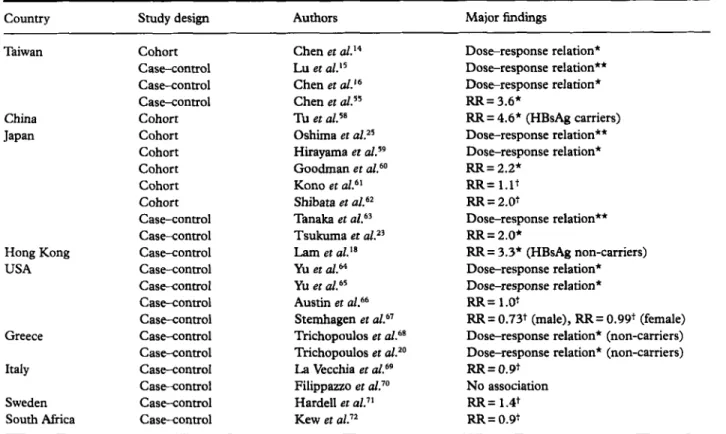
Table 11 Selected studies on association between cigarette smoking and risk of hepatocellular carcinoma
Country Study design Authors Major findings
~~ Taiwan China Japan Hong Kong USA Greece Italy Sweden South Africa ~~ ~ Cohort Case-control Case-control Case-control Cohort Cohort Cohort Cohort Cohort Cohort Case-control Casecontrol Case-control Case-control Case-control Case-control Case-control Case-control Case-control Case-control Casecontrol Case-control Case-control Chen et al.I4 Lu et al.15 Chen et d.16 Chen et al.5s Tu et a1.5s Oshima et d Z s Hirayama et aLS9 Goodman et Kono et a L 6 I Shibata et al.62 Tanaka et ~ 1 . ~ ~ Tsukuma et al.=' Lam et al." Yu et aLM Yu et al. 65 Austin et a1.66 Stemhagen et ~ 1 . ~ ~ Trichopoulos et a1.@' Trichopoulos et a L 2 0 La Vecchia et al.69 Filippazzo et a L 7 0 Hardell et a1.I' Kew et Doseresponse relation* Dose-response relation** Doseresponse relation* RR= 3.6* RR = 4.6* (HBsAg carriers) Doseresponse relation** Dose-response relation* RR = 2.2*
RR=
l.ltRR
= 2.0t Dose-response relation** R R = 2.0* RR = 3.3* (HBsAg non-carriers) Doseresponse relation* Dose-response relation* RR= l.0t RR = 0.73t (male), R R = 0.99t (female) Dose-response relation* (non-camers) Dose-response relation* (non-carriers) RR = 0.91No association RR= 1.4t
RR= 0.91 * P < 0.05; **0.05 < P < 0.10; t, statistically non-significant; RR, relative risk.
aflatoxin levels and liver cancer mortality was statistically significant in Kenyaso and but not in China.5z The cohort study performed in Shanghai has shown a significant association between urinary ailatoxin levels and HCC risk, showing a multivariate-adjusted
RR
of 3 X s 3 This study also showed a synergistic interaction betweenHBsAg carrier status and urinary aflatoxin levels. Compared with non-HBsAg carriers who had no detectable urinary level of aflatoxin as the referent (RR = l.O), the RR of developing HCC were 1.9, 4.8 and 60.1, respectively, for
HBsAg
carriers with an undetectable urinary aflatoxin level, non-carriers with a detectable urinary ailatoxin level and HBsAg carriers with a detectable urinary aflatoxin level. In a recent case- control study in Taiwan, the detectable urinary allatoxin level was also significantly associated with an increased HCC risk showing an RR of 5.5.56 The detectable serum level of aflatoxin B,-albumin adduct was found to be associated with an increased risk of HCC in two studies in T a i ~ a n , ~ ~ . ~ ~ while a sigdicant dose-response relation- ship between serum aflatoxin B,-albumin adduct levels and HCC risk was observed in a cohort study performed in the Taipei metropolitan area.57Cigarette smoking
The association between cigarette smoking and HCC is inconsistent in case-conaol and cohort studies shown in Table 11. The cigarette smoking habit was found to be
associated with a significantly increased HCC risk in several studies in China?* Japan," and Hong Kong,I8 but not in other studies in Japan,6'@ the USA,66,67 Ital~,6~9~O Sweden,7I and southern A f i i ~ a . ' ~ The dose-response relationship between cigarette smoking quantity and H C C risk has been reported in case-control or cohort studies in Taiwan,1k16 Japan?5J9@3 the USA,'~65 and Greece?oz68 The cigarette smoking effect on HCC was limited to HBsAg carriers or non-carriers in some studies, while it remained statistically significant after adjustment for HBsAg carrier status in other studies. Furthermore, a synergistic interaction between daily cigarette smoking quantity and HBsAg camer status has also been documented.16 Compared with HBsAg-negative non-smokers as the referent group (RR
=
1.O),
theRR
of developing H C C were 1.8, 20.7 and 318.0, respectively, for HBsAg-negative smokers, HBsAg-positive non- smokers and HBsAg-positive smokers. There was also a synergistic interaction between cigarette smoking and anti-HCV seropo~itivity.~~ Compared with anti-HCV- negative non-smokers as the referent group (RR= l.O), the RR of developing HCC were 1.6, 6.0 and 14.6, respectively, for anti-HCV-negative smokers, anti-HCV- positive non-smokers and anti-HCV-positive smokers.Alcohol consumption
Alcohol drinking has been documented as the risk factor for H C C in most epidemiological studies shown
Table 12 Selected studies on association between alcohol consumption and risk of hepatocellular carcinoma
country Study design Authors Major findings
Taiwan Cohort Chen et a1.I4 RR = 3.1* (heavy drinkers)
Case-control Lu et RR = 0.6t
Case-control Chen et a1.I6 RR = 3.4* (heavy drinkers)
Case-control Chen et al.55 R R = 5.8* (heavy drinkers)
Cohort Hirayama et ~ 1 . ~ ~ RR= 1.9*
Cohort Goodman et aL60 RR= 1.2+
Cohort Kono et aL6' Dose-response relation*
Cohort Shibata et a1.62 Dose-response relation*
Case-control Tanaka et al.63 Dose-response relation* (non-carriers)
Case-control Tsukuma et aLZ3 RR= 3.2*
Case-control Lam et aLJa No association
Case-control Yu et a1.64 RR= 4.2* (heavy drinkers)
Case-control Austin et a1.66 Dose-response relation*
Case-control Stemhagen et Dose-response relation*
Greece Case-control Trichopoulos et a1.@' No association
Case-control Trichopoulos er aLZo No association
Italy Case-control La Vecchia et ~ 1 . ~ ~ RR = 1.5* (heavy drinkers)
Case-control Filippazzo et aL70 RR = 3.2* (alcoholics)
Sweden Case-control Hardell et aL7' Dose-response relation*
Japan Cohort Oshima et aLZ5 Dose-response relation*
Hong Kong USA
*P< 0.05; t, statistically non-significant; RR, relative risk.
in Table 12. Heavy alcohol drinkers were found to have a significantly increased HCC risk showing RR ranging from 1.5 in Italy69 to 5.8 in Penghu, Taiwan.55 Dose- response relationship has been documented between H C C risk and alcohol consumption in both case-
control and cohort s t ~ d i e ~ . ~ ~ , ~ ~ ~ ~ , ~ ~ , ~ ~ , ~ ~ But no associ- ation between alcohol consumption and H C C risk was
observed in case-control studies carried out in Taiwan,15 Japan,60 Hong Kong,18 and Greece.zo,68 The interaction between HBsAg carrier status and alcohol consumption was assessed in a recent case-control study in Taiwan.16 The study found that HBsAg- negative alcohol drinkers, HBsAg-positive non-drinkers, and HBsAg-positive drinkers had relative HCC risk of
3.4, 20.2 and 75.6, respectively, compared with HBsAg-negative non-drinkers as the referent group
(RR=
1 .O). Another case-control study in Taiwan reported a synergistic interaction between anti-HCV seropositivity and alcohol consumption on the devel- opment of HCC.36 Anti-HCV-negative alcohol drinkers, anti-HCV-positive non-drinkers, and anti-HCV-positive drinkers had relative H C C risk of 2.1, 6.1 and m, respectively, compared with anti-HCV-negative non- drinkers as the referent group(RR=
1.0).Low
vegetable consumptionand
serum retinol levelIn a recent cohort study in Taiwan, low consumption of dark-green vegetable was associated with an increased risk of HCC.I4 Compared with those who had
consumed dark-green vegetable six or more meals per week as the referent group (RR
= l), the relative risk of
developing HCC was 2.6 and 4.6, for those who consumed dark-green vegetable at 2-5 and < 2 meals per week, respectively. Based on a nested case-control study of this cohort, a low level of retinol in serum samples collected at recruitment was associated with an increased HCC risk. The lower the serum retinol level, the higher the risk of HCC. T h e RR were 3.0 and 9.0, for those who had medium and low serum retinol levels, respectively, compared with those who had a high serum retinol level as the referent group (RR = 1.0). The reverse dose-response relationship was statistically significant among HBsAg carriers and heavy cigarette smokers, respectively, but not among non- carriers and light cigarette s m o k e r ~ . ~ ~
Inorganic arsenic ingestion
Recent ecological, case-control and cohort studies have documented a significant association between HCC and ingested inorganic arsenic through medicinal, envi- ronmental and occupational exposures in Taiwan and other countries.74 In the endemic area of blackfoot disease, a unique peripheral vascular disease related to long-term exposure to inorganic arsenic through drinking artesian well the age-standardized mortality ratio (SMR) of liver cancer was 170 for male and 229 for female residents compared with the general population in Taiwan as the referent ( S M R = A dose-response relationship was reported between HCC risk and arsenic
level in drinking water in the blackfoot disease-endemic area7? and the Taiwan Island as a whole.7a The lifetime risk of HCC due to daily arsenic intake of lop& was 4.3 and 3.6 per 1000, respectively, for males and The prevalence of
HBsAg
carrier status (20%) among residents in the blackfoot disease-endemic area was reported to be similar to those in other areas in Taiwan.so The association between ingested inorganic arsenic exposure and HCC has also been documented in Japan and Germany as described in a recent review.74 In addition to HCC, arsenic is also well documented as a carcinogen for hepatoangiosar~oma.~~Thorotrast, vinyl chloride and iron
Thorotrast (trade name of radioactive thorium dioxide which is used as an X-ray contrast medium) exposure is a major risk factor for the development of hae- mangiosarcoma and also increases the risk of chol- angiocarcinoma and HCC.81 Cohort studies in Japans2 and Germanf3 have demonstrated a significant association between thorotrast exposure and liver cancer risk. Neither of the studies found a role of HBV infection as a cofactor. High-level exposure to vinyl chloride monomer has been well documented as a risk factor for haemangiosarcoma of the liver among polyvinyl chloride workers;84 it is also associated with the development of cholangiosarcomas4 and HCCaS5 No interaction between hepatitis viruses and vinyl chloride exposure has been assessed. Increased serum levels of ferritin have also been observed in liver diseases including HCC.86 Patients affected with haemo- chromatosis, a genetic disease of iron overload, were found to have an increased risk of HCCqS7 The HCC risk associated with iron overload may be particularly important among patients affected with chronic HBV and HCV infection.12
Exogenous and endogenous hormones
Use of oral contraceptives has been well documented as a risk factor for benign hepatic adenoma; it is also associated with HCC showing a lower RR.9J2 The HCC risk was found to increase with the duration of oral contraceptive use in developed countries with low HBV carrier rate,88-9L but no association was observed in countries where HBV is e n d e m i ~ . ~ ~ , ~ ~ Hepatocellular carcinoma and cholangiosarcoma have been reported in conjunction with the use of oxymatholone, an anabolic
steroid derived from Although a
significant male-to-female ratio of HCC observed in almost all countries may be explained partly by the higher prevalence of cigarette smoking and alcohol drinking in men than in women, the elevated serum testosterone level was recently reported to be associated with an increased risk of HCC.95 In this cohort study, elevated serum level of testosterone was associated with a relative HCC risk of 4.0 after adjustment for HBsAg carrier status, anti-HCV seropositivity, alcohol drinking, cigarette smoking, vegetable consumption frequency, past liver disease history, and vegetarian habit. How-
ever, no association between serum testosterone level and HCC was observed in China.96
Genetic and other diseases
Several diseases other than chronic liver diseases are associated with the development of HCC. Patients
affected with haemochromatosis, porphyria and
a-antiaypsin deficiency have been reported to have an increased risk of HCC.87*97>98
Diabetes mellitus was found to be associated with HCC showing an RR of 2.5, and drug hypersensitivity associated with an RR of 0.5.99 There was a report of HCC related to the membranous obstruction of the inferior vena cava.'O0
Familial tendency
The familial aggregation of HCC has been well documented.12 The familial aggregation may result from environmental factors such as HBV infection and/or genetic factors shared by family members. The RR for the family history of HCC was reported to be as high as 4.6 after adjustment for HBsAg carrier status, cigarette smoking and heavy alcohol drinking in Taiwan.I6 Segregation analyses have suggested the existence of a major autosomal gene for HCC. One study indicates the major gene is dominant,101 but another found it to be recessive.Io2 A recent segregation analysis in Taiwan also demonstrated an autosomal recessive gene for HCC.'03
Genetic susceptibility
Human hepatocarcinogenesis is related to exposure to Cigarette smoke, aflatoxins and other chemical car- cinogens. Chemical carcinogens are metabolically acti- vated by phase I enzymes including cytochrome P450 (CYP) enzymes and detoxified by phase
II
enzymes including epoxide hydrolase, arylamine N-acetyltrans- ferase (NAT) and glutathione Stransferase (GST). In a nested case-control study, CYP2E1 genetic poly- morphism was found to be significantly associated with the development of HCC.Io4 The relative risk of developing HCC for subjects with c,/c, genotype of CYP2El compared with those who had genotypes of c,k2 or c2/c2 was 24.3 for cigarette smokers and 1.1 for non-smokers. Alcohol consumption was also found to increase the HCC risk among cigarette smokers with c,/c, genotypes. CYP2D6-rapid metabolizers were reported to have an increased risk of HCC, while NAT2-slow acetylators are at an increased HCC risk.lo5 The relative HCC risk associated with NAT2-slow and CYPPD6-rapid genotypes was 2.6 for all subjects and 5.6 for those with serum viral markers.While no main effect on HCC was observed for the were found to modify the associations between serum level of aflatoxin B, (AFBJ-albumin adducts and HCC risk among HBsAg carrier^.^' The relative HCC risks genetic polymorphism GST
M1
and T1,57J04,L06 th eYHmpatoaollular Oaminom A
+
+
+
Metabolic rnutatlon activationcarcinogen-induced Malnutrition Immunosuppression
Low vegetable Heavy alcohol
Traditional
Chinese
vegetarian habh of consump~on intake
Cigarette smoking
-
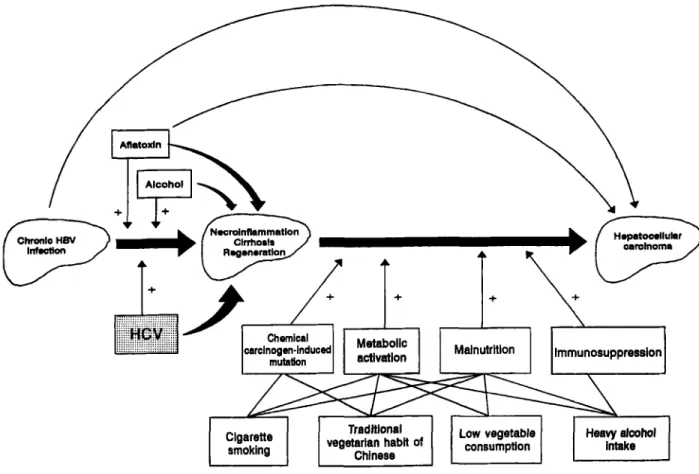
Figure 1 Hypothesized model for interactive effects of multiple risk factors for hepatocellular carcinoma in Taiwan.
were 1.6 and 3.8, respectively, for HBsAg carriers who had low and high serum level of AFB,-albumin adducts compared with those who had undetectable adduct level as the referent group. Further stratification analysis showed the dose-response relationship was statistically significant among HBsAg carriers with null genotypes of GST M1 or T1, but not among carriers with non- null genotypes.
An increased frequency of G to T transversion in codon 249 of the p53 tumour suppressor gene has been reported in areas where aflatoxin plays an important role in the development of HCC,107Jos but a lower prevalence of the mutation was observed in other areas. A significant association between genetic polymorphism of L-myc and HCC has recently been reported.Io6 The RR of developing HCC for the
LL
genotype of L-myc was 2.9 compared with the L-myc SS genotype as the referent group. In a cohort study, the elevated serum level of neu oncoprotein was found as a risk predictor of HCC.Io9 The higher the level of neu oncoprotein in serum samples collected before the diagnosis of HCC, the higher the RR of developing HCC. Furthermore, elevated serum neu oncoprotein level was significantly associated with HBsAg carrier status among healthy controls, and with cigarette smoking among HCC cases.
Hepatocellular carcinoma patients were reported to have a higher frequency of sister chromatid exchange
(SCE) in their peripheral lymphocytes than matched controls."' The mean f standard deviation of SCE was
15.1 k4.4 per lymphocyte at metaphase
I1 for HCC
patients and 8.9 ? 2.7 for controls who were matched with cases on age, sex, cigarette smoking and alcohol consumption. Chromosome abnormalities in peripheral lymphocytes were reported to increase among chronic HBsAg carriers.lll Loss of chromosome arms have been recently reported in HCC tissues.112-114MULTIFACTORIAL AETIOLOGY
Multistage hepatocarcinogenesis
The pathogenesis of HCC in humans is a multistage process with the involvement of multifactorial aetiology. Figure 1 shows a hypothesized model of the interaction among various risk factors for HCC in Taiwan. As reviewed by several investigators, the major pathway of hepatocarcinogenesis in Taiwan is through the HBV infection, chronic hepatitis, liver cirrhosis to HCC.115-118 There are some HCC cases developed from chronic hepatitis directly without liver cirrhosis. HCV, aflatoxin, and alcohol may either act independently or interact with HBV to induce liver cirrhosis. In this multistage process, cigarette smoking, the traditional Chinese vegetarian habit, low vegetable consumption and heavy
HOST SUSCEPTIBILITY FACTORS
lmmunity Metabolk eluyrner Hormonal stltw Qenelk Dobmomhirrn
Humonl P h m l : CYP Oeatrogen
Cellular Phase II : 082. EH Androgen
& 4 4
Healthy subJect -+ Chronic hepatitis
-
Llver cirrhosis + HCCChmmmomm abomtlon Omogma astlvatlon
IncnaMd SCE Tumwr Suppressor
(1WU IlUC(iva(lWI
ENVIRONMENTAL RISK FACTORS
BlOlOalUl facton Chemlul hcton Nutritional hctoon HBV EL HCV Emma1 Inlwml Blologl~lly
Parasites
h.
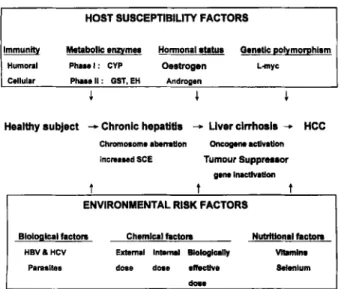
Figure 2 Host susceptibility-environment interaction and risk of hepatocellular carcinoma.
alcohol intake may increase the risk of developing HCC through their effects on the chemical carcinogen- induced mutation, metabolic activation of procar- cinogens, malnutrition and/or immunosuppression. These risk factors may interact with each other synergistically to induce the development of HCC.
Different people living in different areas during different periods of time may have different sets of risk factors for HCC. In order to design strategies for the intervention or prevention of HCC, it is essential to explore these H C C risk factors for specific populations with regard to person, time and place. Only a proportion of asymptomatic HBsAg carriers are affected with chronic active or persistent hepatitis, and only some patients with chronic hepatitis will develop liver cirrhosis. The identification of other sets of risk factors which contribute to the progress from the HBsAg carrier status to chronic hepatitis and firther to liver cirrhosis will assist in the prevention of HCC as early as possible. Further studies on risk factors of chronic hepatitis and liver cirrhosis are important for the effective control of HCC.
Gene-environment interaction
In addition to environmental risk factors including hepatitis viruses, liver parasites, chemical carcinogens through environmental, occupational and medicinal exposures, and dietary factors; individual susceptibility factors are also involved in the multistage development of H C C as shown in Fig. 2. These endogenous risk factors may be related to humoral and cellular immunity, metabolism of chemical carcinogens, hor- monal balance and susceptibility genes. In other words, the host susceptibility may be hereditary, acquired or both. Susceptible individuals exposed to environmental risk factors tend to have the highest risk of HCC compared with those who are neither susceptible nor exposed to environmental risk factors. The elucidation
of the gene-environment interactions will help the characterization of specific risk factors for specific susceptible populations. This may also improve the understanding of aetiological mechanisms of human hepatocarcinogenesis.
ACKNOWLEDGEMENT
This study was supported by grants from the
Department of Health, Executive Yuan, Republic of China.
REFERENCES
1 Bosch
FX,
Munoz N. Epidemiology of hepatocellular carcinoma. In: Bannsch P, Keppler D, Weber G, eds. Liver cell carcinoma. Dordrecht: Kluwer Academic,1989; 3-12.
2 Parkin DM, Muir CS, Whelan SL, Gao YT, Ferlay J, Powell J. Cancer Incidence in Fiwe Continents, vol.
VI.
Lyon: International Agency for Research on Cancer,1992; 930-1.
3 Lin TM, Tsu WT, Chen CJ. Mortality of hepatoma and cirrhosis of liver in Taiwan. Br. J: Cancer 1986; 54: 4 Waterhouse J, Muir C, Shanmugaratnam K et al. Cancer
Incidence in Five Conzinents, vol. 111. Lyon: International Agency for Research on Cancer, 1976; 453547. 5 Waterhouse J, Muir C, Shanmugaramam K et al. Cancer
Incidence in Five Continents, vol. IV Lyon: International Agency for Research on Cancer, 1982; 671-789. 6 Muir C, Waterhouse J, Mack T et al. Cancer Incidence in
Five Continents, vol. V. Lyon: International Agency for Research on Cancer, 1987; 796-939.
7 Okuda K, Fujimoto I, Hanai A, Urano
Y.
Changing incidence of hepatocellular carcinoma in Japan. Cancer 8 Bartoloni St Omer F, Giannini A, Napoli P.Hepatocellular carcinoma and cirrhosis: A review of their relative incidence in a 25-year period in the Florence area. Hepatogasmenterology 1984; 31: 215-17. 9 Mant JWF, Vessey MP. Trends in mortality kom primary
liver cancer in England and Wales 1975-92: Influence of oral contraceptives. Br. J: Cancer 1995; 72: 800-3. 10
Yu
MW, Tsai SF, Hsu KH et al. Epidemiologiccharacteristics of malignant neoplasms in Taiwan 11. Liver cancer. J: Nut1 Public Health Assoc. (ROC) 1988; 11
Yu MW, Chen CJ. Hepatitis B and C viruses in the
development of hepatocellular carcinoma. Crit. Rew.Chcol. Hematol. 1994; 17: 71-91.
12 London WT, McGlynn KA. Liver cancer. In: Schottenfeld D, Fraumeni F Jr, eds. Cancer: Epidemi- ology and Revention, 2nd edn. New York Oxford University Press, 1996; 772-93.
13 Beasley
RP.
Hepatitis B virus: The major etiology of hepatocellular carcinoma. Cancer 1985; 61: 1942-56. 14 m e n CJ,Yu MW, Wang CJ, Huang
HY, Lin WC.Multiple risk factors of hepatocellular carcinoma: A
cohort study of 13737 male adults in Taiwan. J. Gastroenterol. Hepawl. 1993; 8: S83-7.
9 69-7 6.
R ~ s . 1987; 41: 4967-72.
15 Lu SN, Lin TM, Chen CJ er ul. A case-control study of primary hepatocellular carcinoma in Taiwan. Cancer
16 Chen CJ, Liang KY, Chang AS et al. Effects of hepatitis B virus, alcohol drinking, cigarette smoking and familial tendency of hepatocellular carcinoma. Hepawbgy 199 1; 13: 398-406.
17 Chung WK, Sun HS, Park DH, Minuk GY, Hoofnagle
JH. Primary hepatocellular carcinoma and hepatitis B
virus in Korea. J . Med. Virol. 1983; 11: 99-104.
18 Lam KC, Yu MC, h u n g JWC, Henderson BE. Hepatitis B virus and cigarette smoking: Risk factors for hepatocellular carcinoma in Hong Kong. Cancer Res.
19 Yeh FS, Mo CC, Luo S, Henderson BE, Tong MJ, Yu MC. A serological case-control study of primary hepatocellular carcinoma in Guanxi, China. Cancer Res.
20 Trichopoulos D, Day NE, Kaklamani E et al. Hepatitis B virus, tobacco smoking and ethanol consumption in the etiology of hepatocellular carcinoma. Int. J. Cancer
21 Prince AM, Szmuness W, Michon J, Demaille J. A case- control study of association between primary liver cancer and hepatitis B infection in Senegal. Int. J. Cancer 1975; 16: 376-83.
22 Lingao AL, Doming0 EO, Nishioka K. Hepatitis B virus profile of hepatocellular carcinoma in the Philippines. Cancer 1981; 48: 1590-5.
23 Tsukuma H, Hiyama T, Oshima A et al. A case-control study of hepatocellular carcinoma in Osaka, Japan. Int.
J. Cancer 1990; 45: 231-6.
24 Tokudome S, Ikeda M, Matsushita K et al. Hepatocellular carcinoma among HBsAg positive blood donors in Fukuoka, Japan. Eur. J. Cancer Clin. Oncol,
25 Oshima A, Tsukuma H, Hiyama T, Fujimoto I, Yamano H, Tanaka M. Follow-up study of HBsAg- positive blood donors with special reference to effect of drinking and smoking on development of liver cancer. Int. J. Cancer 1984; 34: 775-9.
26 Val1 Mayans My Calvet X, Bruix J et al. Risk factors for hepatocellular carcinoma in Catalonia, Spain. Int. J.
Cancer 1990; 46: 378-81.
27 Watanabe Y, Harada S, Saito I, Miymura T. Prevalence of antibody against the core protein of hepatitis C virus in patients with hepatocellular carcinoma. Znt.
3.
Cancer28 Tanaka K, Hirohata T, Koga S et al. Hepatitis C and hepatitis B in the etiology of hepatocellular carcinoma in the Japanese population. Cancer Res. 1991; 51: 29 Hasan F, Jeffers LJ, De Medina M et al. Hepatitis C- associated hepatocellular carcinoma. Hepatology 1990; 30 Di Bisceglie AM, Order SE, Klein JL et al. The role of chronic viral hepatitis in hepatocellular carcinoma in the United States. Am. J. Gastroenterol. 1991; 86: 335-8. 31 Vargas V, Castells L, Esteban JI. High frequency of
antibodies to the hepatitis C virus among patients with hepatocellular carcinoma. Ann. Intern. Med. 1990; 112: 32 Bruix J, Barrera JM, Calvet X et al. Prevalence of
1988; 62: 205 1-5. 1982; 42: 5246-8. 1985; 45: 872-3. 1987; 39: 45-9. 1988; 24: 235-9. 1991; 48: 340-3. 2842-7. 12: 589-91. 232-3.
antibodies to hepatitis C virus in Spanish patients with hepatocellular carcinoma and hepatic cirrhosis. Lancet
1989; ii: 1004-6.
33 Kew MC, Houghton My Choo QL, Kuo G. Hepatitis C virus antibodies in southern African blacks with hepatocellular carcinoma. Lancet 1990; 335: 873-4. 34 Chen DS, Kuo GC, Sung JL et al. Hepatitis C virus
infection in an area hyperendemic for hepatitis B and chronic liver disease: The Taiwan Experience. J. Infect.
35 Chuang WL, Chang WY, Lu SN et al. The role of hepatitis B and C viruses in hepatocellular carcinoma in hepatitis B endemic area: A case-control study. Cancer
1992; 69: 2052-4.
36 Yu MW, You SLY Chang AS, Lu SN, Liaw YF, Chen CJ. Association between hepatitis C virus antibodies and hepatocellular carcinoma in Taiwan. Cancer Res.
37 Zavitsanos X, Hatzakis A, Kaklamani E et al. Association between hepatitis C virus and hepatocellular carcinoma using assays based on structural and nonstructural hepatitis C virus peptides. Cancer Res.
1992; 52: 5364-7.
38 Coursaget P, Leboullew D, Le Cann P, Bao 0, Coll- Seck AM. Hepatitis C virus infection in cirrhosis and primary hepatocellular carcinoma in Senegal. Trans. R. SOC. Tmp. Med. Hygiene 1992; 86: 552-3.
39 Dazza M, Meneses LV, Girard P er al. Absence of a relationship between antibodies to hepatitis C virus and hepatocellular carcinoma in Mozambique. Am. J Tmp. Med. Hygiene 1993; 48: 23742.
40 Tsai JF, Jeng JE, Ho MS, Chang WY, Lin ZY, Tsai
JH.
Hepatitis B and C virus infection as risk factors for hepatocellular carcinoma in Chinese: A case-control study. Int. J. Cancer 1994; 56: 619-21.
41 Sun CA, Fanadegan H, You SL et al. Mutual confounding and interactive effects between hepatitis C and hepatitis B viral infections in hepatocellular carcinogenesis: A population-based case-control study in Taiwan. Cancer Epidemwl. Biomark. fiev. 1996; 5: 42 Chang CC, Yu MW, Lu CF, Yang CS, Chen CJ. A nested case-control study on association between hepatitis C virus antibodies and primary liver cancer in a cohort of 9775 men in Taiwan. J. Med. Virol. 1994; 43 Yu MC, Tong MJ, Coursaget P, Ross RK, Govindarajan S, Henderson BE. Prevalence of hepatitis B and C viral markers in black and white patients with hepatocellular carcinoma in the United States. J. Natl Cancer Znst.
1990; 82: 1038-4 1.
44 Kalamani E, Trichopoulos D, Tzonou A et al. Hepatitis
B and C viruses and their interaction in the origin of hepatocellular carcinoma. J A M 1991; 265: 1974-6. 45 Stroffolini T, Chiaramonte My Tiribelli C et al.
Hepatitis C virus infection, HBsAg carrier state and hepatocellular carcinoma: Relative risk and population attributable risk from a case-control study in Italy. J.
Hepawl. 1992; 16: 36&3.
46 Cordier S, Le Thi Bich Thuy, Verger P et al. Viral infection and chemical exposures as risk factors for hepatocellular carcinoma in Vietnam. Int. J. Cancer
1993; 55: 196-201.
D ~ s . 1990; 162: 817-22.
1991; 51: 5621-5.
173-8.
47 Tanaka K, Ikematsu H, Hirohata T, Kashiwagi S. Hepatitis C virus infection and risk of hepatocellular carcinoma among Japanese: Possible role of type 1 b (II) infection. 3; Natl Cancer Inst. 1996; 88: 742-6.
48 Van Rensburg SJ, Cook-Mozaffari P, Van Schalkwyk DJ, Van Der Watt JJ, Vincent TJ, Purchase IF. Hepatocellular carcinoma and dietary aflatoxin in Mozambique and Transkei. Br. J. Cancer 1985; 51: 49 Peers F, Bosch X, Kaldor J, Linsell A, Pluijman M. Matoxin exposure, hepatitis B virus infection and liver cancer in Swaziland. Inr. J. Cancer 1987; 39: 545-53. 50 Autrup H, Seremet T, Wakhisi J, Wasunna A. Matoxin
exposure measured by urinary excretion of aflatoxin B1-guanine adduct and hepatitis B virus infection in areas with different liver cancer incidence in Kenya. Cancer Res. 1987; 47: 3430-3.
5 1 Yeh FS, Yu MC, Mo CC, Luo S, Tong MJ, Henderson BE. Hepatitis B virus, aflatoxins, and hepatocellular carcinoma in southern Guangxi, China. Cancer Res.
1989; 4 9 2506-9.
52 Campbell TC, Chen J, Liu C, Parpia B. Nonassociation of aflatoxin with primary liver cancer in a cross- sectional ecological survey in the People’s Republic of China. Cancer Res. 1990; 50: 6882-93.
53 Ross RK, Yuan JM, Yu MC et al. Urinary aflatoxin biomarkers and risk of hepatocellular carcinoma. Lancet
54 Hatch MC, Chen CJ, Levin B et al. Urinary aflatoxin levels, hepatitis-B virus infection and hepatocellular carcinoma in Taiwan. Int. 3; Cancer 1993; 5 4 931-4. 55 Chen CJ, Wang LY, Lu SN er ul. Elevated aflatoxin
exposure and increased risk of hepatocellular carcinoma. Hepawlogy 1996; 2 4 38-42.
56 Wang LY, Hatch M, Chen CJ ez al. Matoxin exposure and risk of hepatocellular carcinoma in Taiwan. Int. 3;
Cancer 1996; 67: 620-5.
57 Chen CJ, Yu MW, Liaw YF et ul. Chronic hepatitis B carriers with null genotypes of glutathione S-transferase
M1 and T1 polymorphisms who are exposed to aflatoxin are at increased risk of hepatocellular carcinoma. Am. J. Hum. Genet. 1996; 59: 128-34. 58 Tu J, Gao R, Zhang D et ui. Hepatitis B virus and
primary liver cancer on Chongming Island, People’s Republic of China. Natl Cancer Inst. M m o p . 1985; 69: 59 Hirayama T. A large-scale cohort study on risk factors for primary liver cancer, with special reference to the role of cigarette smoking. Cancer Chemothm Pharmacol.
1989; 23: S114-17.
60 Goodman MT, Moriwaki H, Vaeth M, Akiba S, Hayabuchi H, Mabuchi K. Prospective cohort study of risk factors for primary liver cancer in Hiroshima and Nagasaki, Japan. Epidemwlogy 1995; 6: 36-41.
61 Kono S, Ikeda M, Tokudome S, Nishizumi M, Kuratsune M. Cigarette smoking, alcohol and cancer mortality: A cohort study of male Japanese physicians. 3pn. J. Cancer Res. 1987; 78: 1323-8.
62 Shibata A, Hirohata T, Toshima H, Tashiro H. The role of drinking and cigarette smoking in the excess deaths from liver cancer.
an.
J. Cancer Res. 1986; 17: 287-95. 63 Tanaka K, Hirohata T, Takeshita S. Blood transfusion,alcohol consumption, and cigarette smoking in
71 3-26.
1992; 339 943-6.
2 13-1 5.
causation of hepatocellular carcinoma: A case-control study in Fukuoka, Japan. 3pn. J. Cancer Res. 1988; 79: 64 Yu MC, Mack T, Hanisch R et al. Hepatitis, alcohol
consumption, cigarette smoking, and hepatocellular carcinoma in Los Angeles. Cancer Res. 1983; 43: 65 Yu MC, Harris R, Kabat G et al. Cigarette smoking, alcohol consumption and primary liver cancer: A case- control study in the USA. Int. J. Cancer 1988; 42: 66 Austin H, Delzell E, Grufferman S et al. A case-control
study of hepatocellular carcinoma and the hepatitis B virus, cigarette smoking, and alcohol consumption. Cancer Res. 1986; 46: 962-6.
67 Stemhagen A, Slade J, Altman R, Bill J. Occupational risk factors and liver cancer: A retrospective case- control study of primary liver cancer in New Jersey. Am.
3; Epidemwl. 1983; 117: 44354.
68 Trichopoulos D, MacMahon B, Sparros
L,
Merikas G.Smoking and hepatitis B-negative primary
hepatocellular carcinoma. 3; Natl Cancer Inst. 1980; 65: 69 La Vecchia C, Engri E, Decarli A, D’Avanzo B, Franceschi S. Risk factors for hepatocellular carcinoma in northern Italy. Int. J. Cancer 1988; 42: 872-6. 70 Filippazzo MG, Aragona E, Cottone M et al.
Assessment of some risk factors for hepatocellular carcinoma: A case control study. Stat. Med. 1985; 4: 345-5 1.
71 Hardell L, Bengtsson NO, Jonsson U, Eriksson S, Larsson LG. Aetiological aspects on primary liver cancer with special regard to alcohol, organic solvents and acute intermittent porphyria: An epidemiological investigation. Br. J. Cancer 1984; 5 0 389-97.
72 Kew MC, Di Bisceglie AM, Paterson AC. Smoking as a risk factor in hepatocellular carcinoma: A case-control study in southern African blacks. Cancer 1985; 56: 73 Yu MW, Hsieh
M,
Pan WH, Yang CS, Chen CJ. Vegetable consumption, serum retinol level, and risk of hepatocellular carcinoma. Cancer Res. 1995; 55: 74 Chen CJ, Lin LJ. Human carcinogenicity and atherogenicity induced by chronic exposure to inorganic arsenic. Jn: Nriagu 0, ed. Arsenic in the Enwironment, Part II: Human Heulth and Ecosystem Eflecu. New York John Wiley & Sons Inc, 1994; 109-31.75 Chen CJ, Wu NM, Lee SS, Wang JD, Cheng SH, W u HY. Atherogenicity and carcinogenicity of high-arsenic artesian well water: Multiple risk factors and related malignant neoplasms of blackfoot disease. Arteriosclerosis
76 Chen CJ, Chuang YC, Lin TM, Wu HY. Malignant neoplasms among residents of a blackfoot disease- endemic area in Taiwan: High-arsenic artesian well water and cancers. Cancer Res. 1985; 45: 5895-9. 77 Chen CJ, Kuo TL, Wu NM. Arsenic and cancers.
k n c e t 1988; i: 414-15.
78 Chen CJ, Wang CJ. Ecological correlation between arsenic level in well water and age-adjusted mortality from malignant neoplasms. Cancer Res. 1990; 50: 5470-4. 1075-82. 6077-9. 325-8. 11 1-14. 2315-17. 1301-5. 1988; 8: 452-60.