Effect of Auricular Acupressure on Peri- and Early Post-Menopausal Wome n
with Anxiety: A Double-Blinded, Randomized, and Controlled Pilot Study
Ching-Ling Kaoa,b, Chao-Hsun Chenc, Wei-Yun Lin b, Yu-Ching Chiaod, Ching- Liang
Hsiehe,f,g*
a
Department of Adult Psychiatry , Tsao-Tun Psychiatric Center, Department of Health,
Executive Yuan, Nan-Tou, 54249 ,Taiwan
b
College of Chinese Medicine, Graduate institute of Integrated Medicine, China
Medical University, Taichung, 40402, Taiwan
c
Department of Chinese Medicine, Chang-Hua Hospital, Department of Health,
Chang-Hua, 51341, Taiwan
d
Department of Business Administration, National Chung Hsing University, Taichung,
40227, Taiwan
e
College of Chinese Medicine, Graduate Institute of Acupuncture Science, China
Medical University, Taichung, 40402, Taiwan
f
Acupuncture Research Center, China Medical University, Taichung, 40402, Taiwan
g
Department of Chinese Medicine, China Medical University Hospital, Taichung,
* Correspondence: Ching- Liang Hsieh M.D., Ph.D. College of Chinese Medicine,
Graduate Institute of Acupuncture Science, China Medical University. 91 Hsueh-Shih
Road, Taichung, 40402, Taiwan
Running title: Auricular acupressure improves women with menopausal anxiety
Abstract
We tested effects of auricular acupressure on peri- and early post- menopausal women
with anxiety (PPWA). Fifty PPWA were randomly assigned to the auricular
acupressure group (AG) or the sham group (SG). After 3 meals and before sleep every
day for 4 weeks, the AG received auricular acupressure on the bilateral ear shenmen
and subcortex points for 3 min per point on alternating ears. The SG received sham
auricular acupressure. The Alprazolam was reduced from 0.5 mg/day at baseline to
0.3 mg/day 4 weeks after auricular acupressure (4W) in the AG (P < .05) whereas
Alprazolam maintained at 0.5 mg/day in the SG (P > .05). The Zolpidem was reduced
from 3.0 mg/day at baseline to 1.5 mg/day at 4 W (P < .05), whereas Zolpidem was
reduced from 2.4 mg/day at baseline to 1.9 mg/day at 4W in the SG (P > .05),
Introduction
In menopausal women, anxiety and accompanying insomnia generate a domino effect
that can multiply symptoms associated with menopause and depression. These
burdens last for more than a few months or even several years, and such conditions
often affect quality of life. According to the American Psychiatric Association
Diagnostic and Statistical Manual Fourth Edition (DSM-IV, TR) [1], anxiety is
classified as an ongoing concern, worry, or sense of impending disaster, a feeling of
tension, and an inability to relax. Anxiety disorders are a large group of conditions,
including panic disorder, phobia, obsessive-compulsive disorder, generalized anxiety
disorder, post-traumatic stress disorder, and anxiety secondary to general medical
conditions. Insomnia is defined as difficulty falling asleep or maintaining sleep, early
awakening, or not feeling rested after sleep along with fatigue, distress, or functional
decline.
Menopause is when women permanently stop menstruating. Peri- menopause
usually occurs in 5 to 7 years before menopause, and is the transitional phase from the
regular ovarian menstrual cycle to complete cessation of ovarian functions. The
epidemiology of natural menopause is defined as a lack of menstruation for 12
months in the absence of other causes such as pregnancy or breastfeeding [2];
characterized by irregular menstrual cycles or less than 12 months without
menstruation, but the only index in the first 2 or 3 days of the menstrual cycle is an
elevation in the follicle stimulating hormone (FSH) [3]. According to Stages of
Reproductive Aging Workshop (STRAW) criteria, FSH plasma concentrations of
more than 2 standard deviations more than the normal 14 IU/ L above the early
follicular phase concentration of FSH indicates peri- menopause.
The most common symptoms of menopause are hot flashes, night sweats,
vaginal dryness, problems with decreased sexual function, sleep disorders, headaches,
heart palpitations, inability to concentrate, and fatigue; in addition, weight gain, joint
pain, short-term memory problems, urinary problems, skin itching, and intestinal
discomfort are common symptoms [4]. For middle-aged women, numerous sources of
stress may worsen the anxiety of the situation, such as "empty nest" syndrome, care
for elderly parents, spouse death, or divorce. Epidemiological research shows that
numerous menopausal women have more symptoms of irritability and depression, and
are prone to mild to severe depression. A cohort study by a Harvard research team
found that significant new depressive symptoms in menopausal women have at least
twice the possibility of leading to depression than in the pre- menopausal stage [5].
Anxiety and insomnia can be predictors of depression for women in this period [6].
sleep disturbance, physical and mental symptoms, muscle and joint pain, and other
symptoms at different stages of menopause may affect women's quality of life [8];
however, early treatment of anxiety can improve menopause-related symptoms,
depression, and quality of life.
Although estrogen therapy has an effect on vasomotor symptoms, depression,
anxiety, and insomnia in menopausal and postmenopausal women, the Women's
Health Initiative (WHI) reported an increase in cases of coronary heart disease, stroke,
venous thrombosis, and dementia cases after hormone therapy [9]. Although all these
studies are conducted on post- menopausal women, and the time before termination of
hormone treatment is at least 5 years, they have caused misgivings on the safety of
long-term hormone therapy. Some studies show that the drugs of choice for insomnia
in menopausal and post-menopausal women, such as the non-benzodiazepines
Zolpidem and Eszopiclone, are effective for the short-term, and improve sleep, mood,
quality of life, and menopause-related symptoms within 4 weeks [10, 11]; however,
long-term use of these drugs may still cause psychological or physical dependence.
Typical clinical anxiety disorders such as generalized anxiety disorder, panic disorder,
obsessive-compulsive disorder, and post-traumatic stress disorders require serotonin
reuptake inhibitors, serotonin and norepinephrine reuptake inhibitors, and other
physical condition are treatable with low doses of anti-anxiety agents.
As a treatment for generalized anxiety disorders, acupuncture has relatively
similar effects as traditional medicine, and can be used in combination with traditional
medicine to reduce the side effects of serotonin reuptake inhibitors. Acupuncture
reduces anxiety through the regulation of neurotransmitters by reducing the platelet
5-hydroxytryptamine (5-HT) concentration and plasma adrenocorticotrophic hormone
(ACTH) [12]. Some randomized controlled studies showed that ear acupuncture
before surgery can reduce anxiety related to surgery [13], and can improve anxiety in
everyday life for healthy participants [14]. As opposed to acupuncture focused on
parts of the body, auricular acupuncture therapy can easily be mapped to the body's
acupuncture points, and is convenient for patients because treatment does not require
the removal of clothing. Acupuncture covers a variety of techniques. Apart from
needle insertion, one approach is to paste magnetic beads on corresponding
acupuncture points and pressing several times to reduce local congestion, redness, or
heat. This approach is called acupressure.
We used evidence-based methods to review the history and research of the
effects of ear acupuncture on anxiety [15-17]. No previous study has explored the
therapeutic effect of a combination of auricular acupressure and drug treatment for
we designed this protocol in an attempt to provide convenient and effective treatment
and to reduce dependence on sedatives, thereby improving quality of life for
Materials and methods
Participants
Ninety-one peri-and early post- menopausal women with anxiety (PPWA) were
recruited at the Department of Psychiatry, Chang-Hua Hospital, Department of Health
from January 1, 2010 to December 31, 2010. Forty-one patients were excluded from
the study prior to signing informed consent: 12 patients had experienced menopause
for more than 10 years, 1 had a serious medical disease, 3 had major psychiatric
illnesses, 2 had recently used hormones, 1 regularly used Chinese herbs, and 3 refused
the trial. The inclusion criteria were 1) between 40 and 60 years of age; 2) irregular
menstruation for less than 12 months or menopause for less than 10 years; 3) FSH
plasma concentrations of ≧ 14 IU / L ; and 4) anxiety secondary to peri- menopause
or early post- menopause. Participants provided written informed consent after a full
explanation of the purpose and process of the study. Exclusion criteria were 1) serious
medical disorders (for example, asthma; epilepsy; or heart, liver, or renal failure); 2)
substance dependence or abuse (for example, alcohol, drugs, hypnotics, and
analgesics); 3) contraindications to sedatives and hypnotic drugs; 4) contraindications
to acupuncture treatment; 5) suicidal and violent tendencies; 6) existence of primary
anxiety disorders and other major axis I psychiatric diagnoses ( for example,
standard type and dosage of the drugs set in this study; 8) use of hormone therapy for
menopausal symptoms; 9) use of traditional Chinese medicine for mental conditions;
and 10) refusal to sign the informed consent form. The plan was reviewed and
approved before the trial by the China Medical University Hospital Institutional
Review Board (CMUH IRB No. DMR98-IRB-291-1).
Design and sample size
The present study is a randomized double-blind control pilot study of a combination
of modern medicine and complementary therapy of auricular acupressure to research
the change in anxiety symptoms in peri-and early post- menopausal women.
Remission of anxiety is defined as a reduction in score on the Hamilton Anxiety
Rating Scale (HAMA) [18] ≧ 50% and Clinical Global Impression-severity/Clinical
Global Impression-Improvement/ (CGI-S/CGI-I)[19]≦ 2; and improvement of
menopausal symptoms is defined as a reduction in score on the Menopause Rating
Scale (MRS)[20]≧ 50%.
Because the present study was a pilot study, no bas is existed on which to calculate
power or sample size.
Fifty peri- and early post- menopausal women with anxiety were assigned to 1 of 2
groups by a computerized random numbers table, as follows: 1) In the auricular
acupressure group (AG), participants received ear adhesive tape with magnetic beads
(200 Gauss, Xiang Yu International Co., Ltd., Taiwan) on the ear shenmen (MA-TF1)
and subcortex (MA- AT1) points for both ears from a Chinese medicine physician with
more than 8 years of experience in auricular acupressure. Acupressure was applied to
each acupoint on alternating ears for 3 min at each point after 3 meals and before
bedtime every day for 4 weeks. The ear adhesive tape with magnetic beads was
changed twice a week; thus, they were changed 8 times in the 4 weeks; 2) In the sham
acupressure group (SA), the methods were identical to AG, but the ear adhesive tape
had no magnetic beads. All participants were allowed to receive doses of Alprazolam
0 to 2 mg/day and Zolpidem 0 to 10 mg/day, gradually tapering the dosage of each
drug during the period of treatment.
Assessment and outcome measure
The assessment was performed by a psychiatric specialist who was blind to the group.
The participants were evaluated at baseline (before auricular acupressure) and 4
weeks after auricular acupressure (4W). The type and dosage of medication were also
Primary outcome measures focused on the difference in dosage of Alprazolam or
Zolpidem between the baseline and at 4W and the difference in HAMA, MRS, CGI-S,
and CGI-I scores between baseline and at 4W. The secondary outcome measure was
the difference in quality of life according to Short Form Health Survey (SF-36) scores
and its sub-scores between baseline and at 4W.
The HAMA contains 14 items measured with a 5-point Likert scale. The score is
from 0 (no symptoms) to 4 (extremely severe). The present study calculated only the
total scores. The higher the total score was, the more serious the symptoms of anxiety.
The MRS includes 11 items that can be divided into 3 subscales: the urogenital,
somatic, and psychological domains. It uses a 5-point Likert scale from 0 (no
symptoms) to 4 (extremely severe). The study calculated only the total scores. The
higher the total score, the more serious the symptoms of menopause are. The SF-36
contains 36 items to assess physical and mental health, divided into 8 subscales:
physical function (PF), social function (SF), role limitations caused by physical
problems (RP), role limitations caused by emotional problems (RE), mental health
(MH), energy/vitality (VT), body pain (BP), and general perception of health (GH).
This study assessed each subscale; higher scores presented a better health status. The
CGI-S contains 7 items from 1 to 7 points. A higher score indicates greater severity.
degree of improvement.
Statistical Analysis
The data were analyzed using statistical software SPSS 18.0 version. The categorical
data was analyzed using Pearson x2 tests or Fisher ’s exact tests. Independent t tests
(two-tailed) were used to analyze the variables between the AG and SG groups, and
paired t tests (two-tailed) were used to analyze the intra-group variables. Significance
Results
Baseline characteristics of demographic data
Of the 50 PPWA enrolled in the present study, 27 participants were assigned to the AG
and 23 to the SG. Only 25 participants in the AG completed the trial. One stopped
because of dizziness, and 1 stopped because of other reasons. N ineteen participants
completed the trial in the SG; 2 stopped because they felt no effect, and 2 could not
adhere to the times in the study. Therefore, 44 participants completed the trial (Fig. 1).
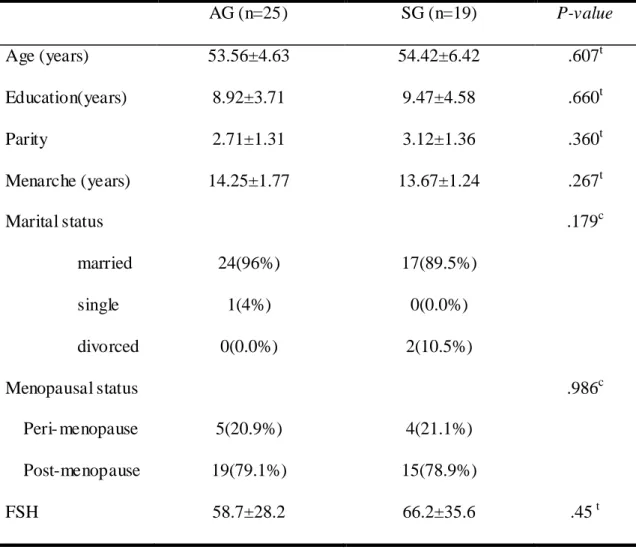
The baseline characteristics of the AG and SG participants, which comprised age,
education, parity, age at menarche, marital status, menopausal status (peri- menopause
and post- menopause), and levels of FSH were similar between the 2 groups (all P
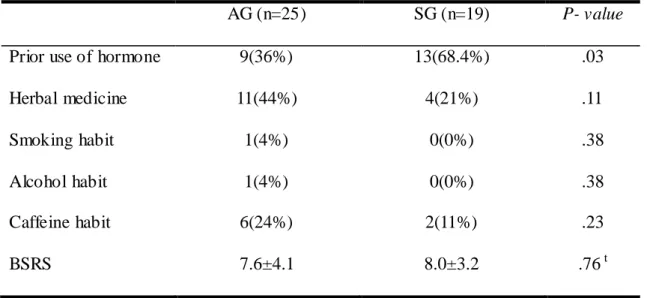
> .05; Table 1). In addition, factors influencing anxiety investigated prior to the trial,
namely use of herbal medicine, smoking habits, alcohol habits, caffeine habits, and
Brief Symptom Rating Scale (BSRS), were similar between the AG and the SG (all P
> .05; Table 2). The exception was that prior use of FSH was greater in the SG than in
the AG (P = .03; Table 2).
Effect of auricular acupressure on PPWA
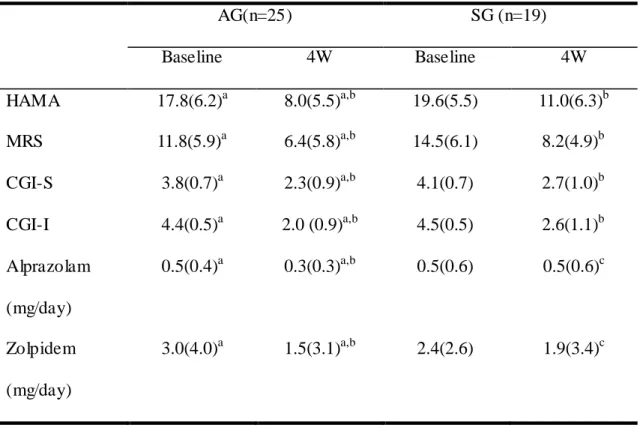
The HAMA scores at baseline and at 4W were similar between the AG and the SG
AG and in the SG (both P < .05; Table 3), and the difference in HAMA score between
baseline and 4W was similar between the 2 groups (P > .05; Table 3).
The MRS scores at baseline and at 4W were similar for the AG and the SG (both
P > .05; Table 3). The MRS scores were higher at baseline than at 4W in the AG and
in the SG (both P < .05; Table 3), and the difference in MRS score between baseline
and 4W was similar for the 2 groups (P > .05; Table 3).
The CGI-S scores at baseline and at 4W were similar for the AG and the SG
(both P > .05; Table 3). The CGI-S scores were higher at baseline than at 4W in the
AG and in the SG (both P < .05; Table 3), and the difference between CGI-S score at
baseline and at 4W was similar for the 2 groups (P > .05; Table 3).
The CGI-I scores at baseline and at 4W were similar for the AG and the SG (both
P > .05; Table 3). The CGI-I scores were higher at baseline than at 4W in the AG and
in the SG (both P < .05; Table 3), and the difference between CGI-I score at baseline
and at 4W was similar for the 2 groups (P > .05; Table 3).
The Alprazolam doses at baseline and at 4W were similar for the AG and the SG
(both P > .05; Table 3). The Alprazolam doses were greater at baseline than at 4W in
the AG (both P < .05; Table 3), but not in the SG (P > .05; Table 3). The difference in
Alprazolam doses between baseline and 4W was similar for the 2 groups (P > .05;
The Zolpidem doses at baseline and at 4W were similar for the AG and the SG
(both P > .05; Table 3). The Zolpidem doses were higher at baseline than at 4W in the
AG (both P <.05; Table 3), but not in the SG (P > .05; Table 3). The difference
between Zolpidem doses at baseline and at 4W was similar for the 2 groups (P > .05;
Table 3).
Effect of auricular acupressure on sub-scores of SF-36 in PPWA
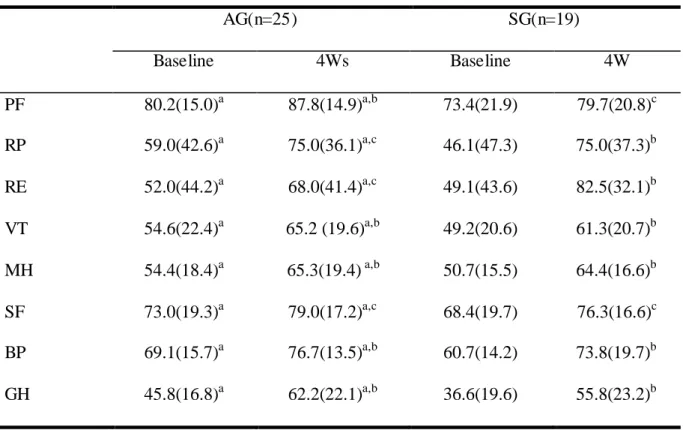
The PF sub-score of SF-36 at baseline and at 4W were similar for the AG and the
SG (both P > .05; Table 4). The PF sub-scores of SF-36 were higher at 4W than at
baseline in the AG (both P < .05; Table 4), but not in the SG (P > .05; Table 4). The
difference between PF sub-scores of SF-36 at baseline and at 4W was similar for the 2
groups (P > .05; Table 4).
The RP and RE sub-scores of SF-36 at baseline and at 4W were similar for the
AG and the SG (both P > .05; Table 4). The RP and RE sub-scores of SF-36 were
greater at 4W than at baseline in the SG (both P < .05; Table 4), but not in the AG
(both P > .05; Table 4). The difference between the RP and RE sub-scores of SF-36 at
baseline and at 4W was similar for the 2 groups (both P > .05; Table 4).
The VT, MH, BP, and GH sub-scores of SF-36 at baseline and at 4W were
sub-scores of SF-36 were greater at 4W than at baseline in the AG and in the SG (all
P < .05; Table 4), whereas the difference between VT, MH, BP, and GH sub-scores of
SF-36 at baseline and at 4W were similar for the 2 groups (all P > .05; Table 4).
The SF sub-score of SF-36 at baseline and at 4W were similar for the AG and the
SG (both P > .05; Table 4). The SF sub-score of SF-36 was similar at baseline and at
4W in the AG and in the SG (both P < .05; Table 4). The difference in SF sub-score of
Discussion
The results of the present study indicate that the difference between HAMA,
MRS, CGI-S, and CGI-I scores at baseline and at 4W was similar for the AG and the
AG. The doses of Alprazolam and Zolpidem were reduced from baseline to 4W in the
AG, but not in the SG. Therefore, we suggest that auricular acupressure improved
PPWA. Both Alprazolam and Zolpidem are sedative drugs widely used to treat PPWA
or insomnia [10, 11], and HAMA, MRS, CGI-S, and CGI-I scores can be used to
evaluate menopausal anxiety [20]. This is the first study showing that auricular
pressure with low-dose Alprazolam and Zolpidem improves anxiety symptoms,
menopausal symptoms, and quality of life in PPWA. The results also show that the
dosage of drugs can be gradually reduced during the course of treatment to help avoid
long-term drug use that could induce dependence. Adding auricular acupressure to a
treatment of anti-anxiety drugs will not increase adverse side effects or decrease
safety. However, participants in the AG and the SG could not predict which group
would show significant improvements. The results are consistent with those of
previous studies that found auricular pressure effective for treating anxiety [21] and
anxiety before surgery [22] and for improving quality of life [23]. Evidence-based
studies on the efficacy of acupuncture have compared the efficacy of real and control
women [24], including primary dysmenorrhea [25], insomnia [26], and weight loss
[27], finding improvement in real and control acupuncture, and showing no statistical
difference between the 2 groups. However, most of the studies did not design a
treatment group without intervention as a control, instead using a noninvasive method
as the control group; therefore, the placebo effect may have contributed to their results.
Some scholars have indicated that sham acupuncture does not exist because true
acupuncture and sham acupuncture could have similar effects on the central nervous
or endocrine systems [28, 29].
The choice of the ear shenmen and subcortex acupoints was based on the
meridian theory of traditional Chinese medicine with a sedative mechanism to
regulate cortical excitation and inhibit brain function. Auricular acupressure on these
acupoints may alleviate the stimulating effect of anxiety, which promotes blood
circulation through the nerve channels. It may also stimulate the small myelinated
nerve in the spinal cord, midbrain, pituitary, and hypothalamus, causing the release of
endorphins into the bloodstream [30].
At the end of this study, the average Alprazolam dosage in the AG was 0.3
mg/day and in the SG was 0.5 mg/day. No statistically significant difference between
the groups was reached; however, in the AG, the difference in drug use between the
showed that 1.5 to 3 mg of Alprazolam per day can improve moderate to severe
anxiety and has antidepressant effects [31]. Our participants entered the study with
mild to moderate anxiety. However, the average dosage remains lower than the
general therapeutic dose in clinical use. Further research is required to adjust the
experimental design using a fixed dosage of combination drugs to distinguish the
difference between the 2 groups.
The present study has several limitations: 1) The sample size was small. With
the first error set to 0.05 and the second error set to 0.2, the power of this study was
0.9; for the study to detect a significant difference in therapeutic effect, each group
requires at least 30 participants; 2) The participants are all from a hospital in a rural
area, and therefore, the results may not be representative of other areas; 3) If the
participants were interested in auricular acupressure or held a positive view of it
before the study, this was likely to affect the results of the study; 4) We had no
untreated group as a control. As mentioned, sham acupuncture had a similar effect,
but a design considering this cannot be a double-blind experimental design. Previous
studies did not directly compare the efficacy of auricular acupressure with different
methods such as rapeseed, Vaccaria son, mustard seed, and magnetic beads in
reducing anxiety; therefore, future studies might consider them; 5) The therapeutic
anxiety or less distressed, consciously or unconsciously driven by the hope of
achieving clinical improvement; and 6) The timeframe for our study is only 4 weeks.
We cannot predict whether the therapeutic effect would be maintained over a longer
period. In the future, we could design a study that, after using a combination of drugs
and auricular pressure for 4 weeks, uses auricular acupressure alone as treatment for a
set time. This could avoid drug dependency and assess whether auricular acupressure
alone can maintain beneficial effects.
In conclusion, no direct support was found for our hypothesis that auricular
acupressure is better than sham acupressure for improving anxiety, menopausal
symptoms, and quality of life. Participants improved whether receiving real or sham
acupressure. The dosage of medication decreased significantly in the auricular
acupressure group, but not the sham acupressure group. This may be indirect evidence
of the benefit of such alternative therapy. Research to develop more safe and effective
interventions using integrated complementary therapy and Western treatment should
Acknowledgme nts
This study is supported by a research fund from Chang-Hua hospital (CHH No. 94-4) ,
and also is supported in part by the Taiwan Department of Health Clinical Tria l and
References
[1]American Psychiatric Association, Diagnostic and Statistical Manual of Mental
Disorders, Fourth Edition, Text Revision.: Washington, DC, 2000.
[2] N.E. Avis and S.M. McKinlay, “A longitudinal analysis of women's attitudes
toward the menopause: results from the Massachusetts Women's Health Study,”
Maturitas, vol. 13, no. 1, pp. 65-79, 1991.
[3]N.E. Avis and S.M. McKinlay, “The Massachusetts Women's Health Study: an
epidemiologic investigation of the menopause,” Journal of the American
Medical Women's Association, vol. 50, no. 2, pp. 45-49, 63, 1995.
[4]C.A. Morse, A. Smith, L. Dennerstein, A. Green, J. Hopper, and H. Burger, “The
treatment-seeking woman at menopause,” Maturitas, vol. 18, no. 3, pp. 161-173,
1994.
[5]L.S. Cohen, C.N. Soares, A.F. Vitonis, M.W. Otto, and B.L. Harlow, “Risk for
new onset of depression during the menopausal transition: the Harvard study of
moods and cycles,” Archives of General Psychiatry, vol. 63, no. 4, pp. 385-390,
2006.
[6] A.F. Polisseni, D.A. de Araújo, F. Polisseni, C.A. Mourão Junior, J. Polisseni, E.S.
Fernandes, and O. Guerra Mde, “Depression and anxiety in menopausal women:
Federação Brasileira das Sociedades de Ginecologia e Obstetrícia, vol. 31, no. 1,
pp. 28-34, 2009.
[7] M.S. Hunter, P. Gupta, A. Papitsch-Clark, and D.W. Sturdee, “Mid-Aged Health
in Women from the Indian Subcontinent (MAHWIS): a further quantitative and
qualitative investigation of experience of menopause in UK Asian women,
compared to UK Caucasian women and women living in Delhi,” Climacteric,
vol. 12, no. 1, pp. 26-37, 2009.
[8]H. Waidyasekera, K. Wijewardena, G. Lindmark, and T. Naessen, “Menopausal
symptoms and quality of life during the menopausal transition in Sri Lankan
women,” Menopause (New York, N.Y.), vol. 16, no. 1, pp. 164-170, 2009.
[9]J.E. Rossouw, G.L. Anderson, R.L. Prentice, A.Z. LaCroix, C. Kooperberg, M.L.
Stefanick, R.D. Jackson, S.A. Beresford, B.V. Howard, K.C. Johnson, J.M.
Kotchen, and J. Ockene, “Risks and benefits of estrogen plus progestin in
healthy postmenopausal women: principal results From the Women's Health
Initiative randomized controlled trial,” JAMA : the journal of the American
Medical Association, vol. 288, no. 3, pp. 321-333, 2002.
[10] C.M. Dorsey, K.A. Lee, and M.B. Scharf, “Effect of zolpidem on sleep in
women with perimenopausal and postmenopausal insomnia: a 4-week,
therapeutics, vol. 26, no. 10, pp. 1578-1586, 2004.
[11]C.N. Soares, H. Joffe, R. Rubens, J. Caron, T. Roth, and L. Cohen, “Eszopiclone in patients with insomnia during perimenopause and early
postmenopause: a randomized controlled trial,” Obstetrics and Gynecology, vol.
108, no. 6, pp. 1402-1410, 2006.
[12] Q. Yuan, J.N. Li, B. Liu, Z.F. Wu, and R. Jin, “Effect of Jin-3-needling therapy
on plasma corticosteroid, adrenocorticotrophic hormone and platelet 5-HT levels
in patients with generalized anxiety disorder,” Chinese Journal of Integrative
Medicine, vol. 13, no. 4, pp. 264-268, 2007.
[13]M. Karst, M. Winterhalter, S. Münte, B. Francki, A. Hondronikos, A. Eckardt, L.
Hoy, H. Buhck, M. Bernateck, and M. Fink, “Auricular acupuncture for dental
anxiety: a randomized controlled trial,” Anesthesia and Analgesia, vol. 104, no.
2, pp. 295-300, 2007.
[14]S.M. Wang and Z.N. Kain, “Auricular acupuncture: a potential treatment for
anxiety,” Anesthesia and Analgesia, vol. 92, no. 2, pp. 548-553, 2001.
[15]L. Gori and F. Firenzuoli, “Ear acupuncture in European traditional medicine,”
Evidence-based Complementary and Alternative Medicine : eCAM, vol. 4, no.
Suppl 1, pp. 13-16, 2007.
“Acupuncture for anxiety and anxiety disorders--a systematic literature
review,” Acupuncture in Medicine : Journal of the British Medical Acupuncture
Society, vol. 25, no. 1-2, pp. 1-10, 2007.
[17]K. Pilkington,“Anxiety, depression and acupuncture: A review of the clinical
research,” Autonomic Neuroscience : Basic & Clinical, vol. 157, no. 1-2, pp.
91-95, 2010.
[18]M. Hamilton, “The assessment of anxiety states by rating,” The British
Journal of Medical Psychology, vol. 32, no. 1, pp. 50-55, 1959.
[19]W. Guy, ECDEU Assessment Manual for Psychopharmacology. Rockville, MD,
USA: US Department of Health, Education, and Welfare. 1976.
[20]L.A. Heinemann, P. Potthoff, and H.P. Schneider, “International versions of the
Menopause Rating Scale (MRS) ,” Health and Quality of Life Outcomes, vol. 1,
pp. 28, 2003.
[21]A. Kober, T. Scheck, B. Schubert, H. Strasser, B. Gustorff, P. Bertalanffy, S.M.
Wang , Z.N. Kain, and K. Hoerauf, “Auricular acupressure as a treatment for
anxiety in prehospital transport settings,” Anesthesiology, vol. 98, no. 6, pp.
1328-1332, 2003.
[22] S.M. Wang, I. Maranets, M.E. Weinberg, A.A. Caldwell- Andrews, and Z.N. Kain, “Parental auricular acupuncture as an adjunct for parental presence during
induction of anesthesia,” Anesthesiology, vol. 100, no. 6, pp. 1399-1404, 2004.
[23] S.H. Maa, M.F. Sun, K.H. Hsu, T.J. Hung, H.C. Chen, C.T. Yu, C.H. Wang, and
H.C. Lin, “Effect of acupuncture or acupressure on quality of life of patients
with chronic obstructive asthma: a pilot study,” Journal of Alternative and
Complementary Medicine (New York, N.Y.), vol. 9, no. 5, pp. 659-670, 2003.
[24]L. Venzke, J.F. Calvert Jr., and B. Gilbertson, “A randomized trial of
acupuncture for vasomotor symptoms in post- menopausal women,”
Complementary Therapies in Medicine, vol. 18, no. 2, pp. 59-66, 2010.
[25] M.C. Wang, M.C. Hsu, L.W. Chien, C.H. Kao, and C.F. Liu, “Effects of
auricular acupressure on menstrual symptoms and nitric oxide for women with
primary dysmenorrhea,” Journal of Alternative and Complementary Medicine
(New York, N.Y.), vol. 15, no. 3, pp. 235-242, 2009.
[26] M. Sjöling, M. Rolleri, and E. Englund, “Auricular acupuncture versus sham
acupuncture in the treatment of women who have insomnia,” Journal of
Alternative and Complementary Medicine (New York, N.Y.), vol. 14, no. 1, pp.
39-46, 2008.
[27] C.H. Hsieh, “The effects of auricular acupressure on weight loss and serum
lipid levels in overweight adolescents,” The American Journal of Chinese
[28] I. Lund and T. Lundeberg, “Are minimal, superficial or sham acupuncture
procedures acceptable as inert placebo controls?,” Acupuncture in Medicine :
Journal of the British Medical Acupuncture Society, vol. 24, no. 1, pp. 13-15,
2006.
[29]T. Lundeberg, I. Lund, J. Näslund, and M. Thomas, “The Emperors sham -
wrong assumption that sham needling is sham,” Acupuncture in Medicine :
Journal of the British Medical Acupuncture Society, vol. 26, no. 4, pp. 239-242,
2008.
[30] K.K. Hui, J. Liu, N. Makris, R.L. Gollub, A.J. Chen, C.I. Moore, D.N. Kennedy,
B.R. Rosen, and K.K. Kwong, “Acupuncture modulates the limbic system and
subcortical gray structures of the human brain: evidence from fMRI studies in
normal subjects,” Human Brain Mapping, vol.9, no. 1, pp. 13-25, 2000.
[31] K. Davison, R.G. Farquharson, M.C. Khan, and A. Majid, “A double blind
comparison of alprazolam, diazepam and placebo in the treatment of anxious
Table 1. Demographic characteristics at baseline AG (n=25) SG (n=19) P-value Age (years) 53.56±4.63 54.42±6.42 .607t Education(years) 8.92±3.71 9.47±4.58 .660t Parity 2.71±1.31 3.12±1.36 .360t Menarche (years) 14.25±1.77 13.67±1.24 .267t Marital status .179c married 24(96%) 17(89.5%) single 1(4%) 0(0.0%) divorced 0(0.0%) 2(10.5%) Menopausal status .986c Peri- menopause 5(20.9%) 4(21.1%) Post-menopause 19(79.1%) 15(78.9%) FSH 58.7±28.2 66.2±35.6 .45 t
Data are expressed as mean ± standard deviation (SD). AG: auricular acupressure group; SG: sham group; FSH: follicle stimulating hormone; t: Student’s t test; c: Pearson chi-square or Fisher ’s exact test.
Table 2. Influencing factors at baseline
AG (n=25) SG (n=19) P- value
Prior use of hormone 9(36%) 13(68.4%) .03
Herbal medicine 11(44%) 4(21%) .11
Smoking habit 1(4%) 0(0%) .38
Alcohol habit 1(4%) 0(0%) .38
Caffeine habit 6(24%) 2(11%) .23
BSRS 7.6±4.1 8.0±3.2 .76 t
AG: auricular acupressure group; SG: sham group; BSRS: Brief Symptom Rating
Scale.
Table 3. Effect of auricular acupressure on peri-menopausal and early
post-menopausal wome n with anxiety
AG(n=25) SG (n=19) Baseline 4W Baseline 4W HAMA 17.8(6.2)a 8.0(5.5)a,b 19.6(5.5) 11.0(6.3)b MRS 11.8(5.9)a 6.4(5.8)a,b 14.5(6.1) 8.2(4.9)b CGI-S 3.8(0.7)a 2.3(0.9)a,b 4.1(0.7) 2.7(1.0)b CGI-I 4.4(0.5)a 2.0 (0.9)a,b 4.5(0.5) 2.6(1.1)b Alprazolam (mg/day) 0.5(0.4)a 0.3(0.3)a,b 0.5(0.6) 0.5(0.6)c Zolpidem (mg/day) 3.0(4.0)a 1.5(3.1)a,b 2.4(2.6) 1.9(3.4)c
AG: auricular acupressure group; SG: sham group; Baseline: prior to auricular
acupressure; 4W: at 4 week after auricular acupressure; HAMA: Hamilton Anxiety
Rating Scale; MRS: Menopause Rating Scale; CGI-S: Clinical Global
Impression-Severity; CGI-I: Clinical Global Impression-Improvement;
a No significant difference between AG and SG groups (P > .05).
b Significant difference between baseline and 4W (P <= .05).
Table 4. Effect of auricular acupressure on sub-scores of SF-36 in
peri-menopausal and early post-menopausal wome n with anxiety
AG(n=25) SG(n=19) Baseline 4Ws Baseline 4W PF 80.2(15.0)a 87.8(14.9)a,b 73.4(21.9) 79.7(20.8)c RP 59.0(42.6)a 75.0(36.1)a,c 46.1(47.3) 75.0(37.3)b RE 52.0(44.2)a 68.0(41.4)a,c 49.1(43.6) 82.5(32.1)b VT 54.6(22.4)a 65.2 (19.6)a,b 49.2(20.6) 61.3(20.7)b MH 54.4(18.4)a 65.3(19.4) a,b 50.7(15.5) 64.4(16.6)b SF 73.0(19.3)a 79.0(17.2)a,c 68.4(19.7) 76.3(16.6)c BP 69.1(15.7)a 76.7(13.5)a,b 60.7(14.2) 73.8(19.7)b GH 45.8(16.8)a 62.2(22.1)a,b 36.6(19.6) 55.8(23.2)b
AG: auricular acupressure group; SG: sham group; Baseline: prior to auricular
acupressure; 4W: at 4 week after auricular acupressure; SF-36: Short Form Health
Survey; PF: physical function; SF: social function; RP: role limitations due to
physical problems; RE: role limitations due to emotional problems; MH: mental
health; VT: energy/ vitality; BP: body pain; GH: general perception of health;
a No significant difference between AG and SG groups (P > .05).
b Significant difference between baseline and 4W (P <= .05).
Figure 1.
Forty-one patients were excluded More than 65 years of age (n=17)
Menopause for more than 10 years (n=12) Serious medical disease (n=1)
Major psychiatric disorders (n=3) Current use of hormone (n=2) Current use of Chinese herbs (n=3) Refusal of trial (n=3)
Randomized (n=50)
Auricular acupressure group (n=27) 1. Ea r adhesive tape with magnetic beads on ear
shenmen and subcortex points of both ears for 3 min on each point on alternating ears after 3 mea ls and before sleep.
2. Ear adhesive tape changed twice a week for 4 weeks
Sham group (n=23)
1. Ea r adhesive tape without magnetic beads on ear shenmen and subcortex points of both ears for 3 minutes on each point on alternating ears after 3 mea ls and before sleep.
2. Ear adhesive tape changed twice a week for 4 weeks
Complete trial (n=25)
Dropout (n=2): Dizziness (n=1) Word reasons (n=1)
Complete trial (n=19)
Dropout (n=4): feeling no effect (n=2), time reasons (n=2)
Statistical analysis
Peri- menopausal and early post- menopausal women with anxiety were enrolled (n=91)