Findings of 2-fluoro-2-deoxy-
d
-glucose positron
emission tomography in hemorrhoids
Shih-Chuan Tsai,
1Long-Bin Jeng,
2,7Jun-Jun Yeh,
3,7Cheng-Chieh Lin,
4,7Jin-Hua Chen,
5Wan-Yu Lin,
1,7,8Chia-Hung Kao
6,71
Department of Nuclear Medicine, Taichung Veterans General Hospital, Taichung, Taiwan
2
Organ Transplantation Center, China Medical University Hospital, Taichung, Taiwan
3
Pingtung Christian Hospital, Meiho University, Pingtung, Taiwan
4
Department of Community Medicine and Health Examination Center, China Medical University Hospital, Taichung, Taiwan
5
Biostatistics Center and Graduate Institute of Biostatistics, China Medical University, Taichung, Taiwan
6
Department of Nuclear Medicine and PET Center, China Medical University Hospital, Taichung, Taiwan
7
School of Medicine, China Medical University, Taichung, Taiwan
8
Institute of Radiological Science, Central Taiwan University of Science and Technology, Taichung, Taiwan
Abstract
Background: Hemorrhoids are very common in adults. The data regarding the incidence of high 2-fluoro-2-deoxy-d-glucose (FDG) uptake in hemorrhoids is
incom-plete. In this study, we evaluated FDG uptake in hemorrhoids and calculated the rate of high FDG uptake in these lesions.
Methods: One hundred and seventy six subjects who undertook whole body FDG–PET for health screening examination were investigated retrospectively. All pa-tients had colonoscopy and 156 subjects were found to have hemorrhoids and 20 had no hemorrhoids. Quanti-tative analysis of FDG uptake in the anal region was performed by calculating the maximum standard uptake value (SUVmax).
Results:The SUVmax ranged from 1.8 to 4.1 (2.8 ± 0.6)
for normal subjects and ranged from 1.4 to 8.3 (2.9 ± 0.8) for patients with hemorrhoids. No statistical difference was noted between these two groups using a Student’s t-tests. If the highest SUVmax, which was 4.1 in
normal subjects, was used as a cutoff, 5.1% (8/156) hemorrhoid patients had a SUVmaxgreater than 4.1.
Conclusion: Hemorrhoids can be one possible cause of focal high FDG uptake in the rectum.
Key words: 2-Fluoro-2-deoxy-d-glucose
(FDG)—Positron emission tomography
(PET)—Hemorrhoid—Maximum standard uptake value (SUVmax)—Health screening examination
Hemorrhoids are one of the most common conditions and they frequently affect the adult population. Over half of the population has hemorrhoids by age 50. Hemorrhoids are swollen blood vessels around the anus or lower rectum. Thrombosis, inflammation and neo-vascularization are usually associated with the swollen blood vessels [1]. High fluorodeoxyglucose (FDG) up-take has been documented with thrombotic lesions, inflammation and neovascularization [2–5]. Therefore, a high FDG uptake in an inflamed hemorrhoid is possi-ble. In 2006, Basu et al. [6] reported avid 18F-FDG uptake in rectal hemorrhoids in a patient with meta-static medullar carcinoma of the thyroid. He assumed intense inflammation and hyperemia associated with the hemorrhoid might be responsible for avid FDG uptake. In the same year, Lu et al. reported another case of hemorrhoids with high FDG uptake [7]. To our sur-prise, these are the only two cases which have been reported with high FDG uptake in hemorrhoid patients. We are curious of the incidence of high FDG uptake in hemorrhoids?
The purpose of this study was to investigate FDG uptake in hemorrhoids and to realize the incidence of high FDG uptake in these lesions.
W.-Y. Lin and C.-H. Kao contributed equally to this work.
Correspondence to:Chia-Hung Kao; email: [email protected]
ª Springer Science+Business Media, LLC 2010
A
bdominal
I
maging
Abdom Imaging (2010) DOI: 10.1007/s00261-010-9670-0
Materials and methods
A total of 487 charts of healthy people, referred from the department of family medicine, examined by whole body FDG positron emission tomography (PET) for health screening examination from January 2007 to December 2009, were reviewed retrospectively. One hundred and seventy six subjects (71 females and 105 men, age ranging between 29 and 80 with an average of 53.2) undertook coloscopy within 3 months. Of the 176 subjects with re-ports of coloscopy, 20 had no evidence of hemorrhoids and 156 were found to have hemorrhoids including three external hemorrhoids, 149 internal hemorrhoids and four mixed type of hemorrhoids. This study was approved by the ethics committee of our hospital (DMR-99-IRB-010).
PET imaging
The PET studies were performed using Advance NXi PET scanner (General Electric Medical Systems, Mil-waukee, WI) 40 min to 1 h after the intravenous injec-tion of 370 MBq (10 mCi) of 18F-FDG. The serum glucose levels of all subjects were checked to ensure the readings were less than 150 mg/dL. Before PET scan-ning, patients were encouraged to void to minimize activity in the bladder due to renal excretion of 18 F-FDG. The scanning was performed from the head to the upper thigh in 2D mode 4 min per bed position. Trans-mission scans were acquired with 68Ge rod sources for attenuation correction. Reconstruction of both trans-mission and etrans-mission scans used ordered-subset expec-tation maximization. The images were reconstructed and displayed in 3D and axial, sagittal and coronal recon-structions for interpretation. Quantitative analysis of
18
F-FDG uptake in the anal region was performed and maximum standard uptake value (SUVmax) was
calcu-lated. The highest SUVmax of the normal subjects was
used as a cutoff value.
Statistical analysis
Statistical analysis of the results was made with the Statistica for Windows Release 4.5 package (StatSoft, Inc., OK, US) using Student’s t-tests and Mann–Whitney U-tests. Results are expressed as mean ± STD. A P value less than 0.05 was considered statistically sig-nificant.
Results
Table1shows the demographic characteristics of normal subjects and patients with hemorrhoids. There was no statistical difference for age and gender between these two groups. Table2 showed the SUVmax in normal
subjects and patients with hemorrhoids. The SUVmax
ranged from 1.8 to 4.1 with a mean value of 2.8 for normal subjects and ranged from 1.4 to 8.3 with a mean
value of 2.9 for patients with hemorrhoids (Fig.1). There was no statistical difference of the SUVmaxbetween these
two groups using Student’s t tests. In the hemorrhoid group, the mean SUVmax was 2.7 for patients with
external hemorrhoids, 2.9 for patients with internal hemorrhoids, and 2.7 for patients with mixed type of hemorrhoids. No statistical differences were noted among these three groups using Mann–Whitney U-tests. The highest SUVmax in the normal subjects was 4.1.
Of the 156 subjects with hemorrhoids, eight (5.1%) sub-jects had SUVmax greater than 4.1 (Fig.2).
Discussion
Hemorrhoids are present in healthy individuals. The main observations of hemorrhoids are hemorrhage, thrombosis, and prolapse. Several theories have been proposed for the mechanisms of hemorrhoidal develop-ment including the varicose vein theory, the sliding anal-lining theory and the vascular hyperplasia theory, and the neovascularization theory [8, 9]. These pathological changes result in prolapsed anovascular cushions, which subsequently interfere with venous return. Decreased venous return, thought to be the mechanism of action, induces dilation of the venous plexus, venous stasis, and/ or thrombosis [1]. Thrombosis in the venous plexus may elicit an inflammatory response. Moreover, vascular proliferation has been reported to cause an important pathologic change in hemorrhoids, which might be due to thrombosis formation [1]. Therefore, thrombosis, inflammation, and vascular proliferation should be considered in the pathogenesis of hemorrhoids.
In our study, eight (5.1%) subjects with hemorrhoids had SUVmax higher than 4.1, which was the highest
Table 1. Demographic characteristics of normal subjects and patients with hemorrhoids
No. Age Sex
Mean ± STD Male Female Normal 20 53.7 ± 11.2 11 9 Hemorrhoid 156 53.2 ± 9.6 94 62
External 3 51 ± 2.6 0 3
Internal 149 53 ± 9.6 92 57
Mixed 4 60.2 ± 12.7 2 2
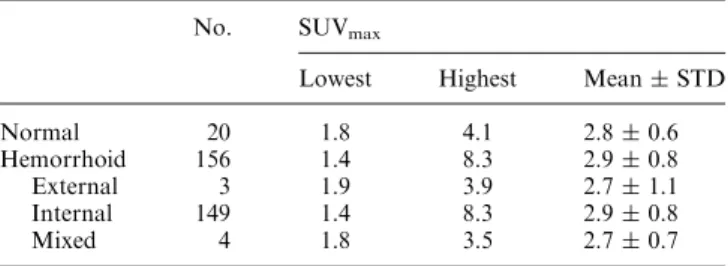
Table 2. The FDG uptake (SUVmax) in normal subjects and patients
with hemorrhoids
No. SUVmax
Lowest Highest Mean ± STD Normal 20 1.8 4.1 2.8 ± 0.6 Hemorrhoid 156 1.4 8.3 2.9 ± 0.8 External 3 1.9 3.9 2.7 ± 1.1 Internal 149 1.4 8.3 2.9 ± 0.8 Mixed 4 1.8 3.5 2.7 ± 0.7
SUVmax for the anal region in the normal group. The
highest SUVmax in the hemorrhoid was 8.3 (Fig. 1),
which was similar to the case reported by Lu et al. In her report, the SUVmax in the hemorrhoids was 8.0 [7]. In
Basu et al.’s study, the intensity of FDG uptake in the hemorroids was also quite high (higher than that of liver uptake) although no SUVmax of the lesion was
men-tioned.
The exact cause of high FDG uptake in the hemor-rhoids remains unclear. We considered inflammation, thrombosis, and vascular proliferation in the
pathogen-esis of hemorrhoids could have contributed to the high FDG uptake. It is well known that FDG not only accumulates in malignant tissue but also in pyogenic infectious foci, granulomatous and non-infectious inflammatory diseases [2]. Furthermore, FDG–PET has been used for the diagnosis and follow-up of large vessel vasculitis with good sensitivity (77%–92%) and high specificity (89%–100%) [3, 10–13]. FDG–PET has also been reported to be useful for the evaluation of throm-bosis. In 2004, Kikuchi et al. [14] found marked accu-mulation of FDG in internal and external jugular vein thrombosis. In addition, Miceli et al. [15] reported that FDG–PET may be useful in evaluating response to treatment. In 2010, Khosa et al. [16] reported an in-creased FDG uptake not only within the vein but also the thrombus itself and concluded FDG–PET/CT appropriately shows venous thrombosis and might play a prominent role in the future. Recently, the relationship between angiogenesis and FDG uptake has been dis-cussed [17,18]. In an animal study, Calcagno et al. found a positive correlation between neovessel count in ath-erosclerotic plaques and 18F-FDG uptake. They con-cluded that FDG–PET could be used as a clinical tool in the evaluation of lesion prognosis and monitoring of anti-angiogenic therapies [17]. Strauss et al. investigated patients with primary colorectal tumors with FDG–PET before surgery. Tissue specimens were obtained from the tumor during surgery, and gene expression was assessed using gene arrays. They found that FDG kinetics are modulated by angiogenesis-related genes. The transport rate for FDG is higher in tumors with a higher expres-sion of VEGF-A and angiopoietin-2. The regresexpres-sion functions for the PET parameters provide the possibility to predict gene expression of VEGF-A and angiopoietin-2. They concluded that angiogenesis is a determining parameter for FDG kinetics in primary colorectal tu-mors [18].
Physiological FDG uptake in the intestines is fre-quently observed [19]. Typical sites of FDG accumula-tion in the intestinal tract include the gastroesophageal junction, gastric fundus, and colon (cecum, proximal ascending colon, and the recto-sigmoid colon). In re-search by Soyka et al. [20], they reported physiological FDG uptake with an SUVmax of 2.6 in the small
intes-tine, 2.3 in ascending colon, 1.8 in transverse colon, 1.9 in descending colon, and 2.8 in recto-sigmoid colon. Recto-sigmoid colon had the highest mean SUVmax for the
intestines. In our study, the mean SUVmax of the anal
region was 2.8, which was the same as the SUVmax of
recto-sigmoid colon in Soyka’s study. Of 20 normal subjects, 13 (65%) had SUVmax greater than 2.5 for the
anal region, 6 (30%) greater than 3.0 and 2 (10%) greater than 3.5. The exact mechanism and cause of the intestinal FDG uptake are still unclear. However, smooth-muscle activity, sphincter activity, constipation, and the presence of lymphoid tissue may be the causes [21,22].
Fig. 1. Scattergram of SUVmax in 20 normal subjects and
156 subjects with hemorrhoids. The solid lines represent the highest SUVmax(4.1) in normal subjects.
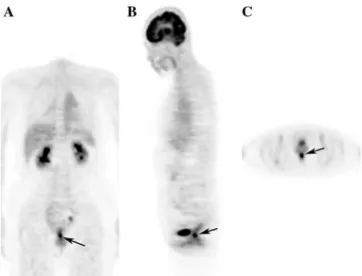
Fig. 2. The FDG-PET images show an area of increased FDG uptake in the anal region (arrows). A coronal view, B sagittal view, and C transverse view. The maximum SUV of the lesion is 8.3. A sigmoidoscopy was performed and internal hemorrhoids of the rectum was the final diagnosis.
In conclusion, hemorrhoids may be considered as one possible cause of focal high FDG uptake in the rectum.
Acknowledgments.We want to thank the grant support of the study projects (DMR-96-065) in our hospital and Taiwan Department of Health, Cancer Research Centers for Excellence (DOH99-TD-C-111-005).
Conflict of interest. The authors have no conflict of interest.
References
1. Nisar PJ, Scholefield JH (2003) Managing haemorrhoids. BMJ 327:847–851
2. Meller J, Sahlmann CO, Gu¨rocak O, Liersch T, Meller B (2009) FDG-PET in patients with fever of unknown origin: the impor-tance of diagnosing large vessel vasculitis. Q J Nucl Med Mol Imaging 53:51–63
3. Bleeker-Rovers CP, Bredie SJ, van der Meer JW, Corstens FH, Oyen WJ (2003) F-18-fluorodeoxyglucose positron emission tomography in diagnosis and follow-up of patients with different types of vasculitis. Neth J Med 61:323–329
4. Chang KJ, Zhuang H, Alavi A (2000) Detection of chronic recur-rent lower extremity deep venous thrombosis on fluorine-18 fluo-rodeoxyglucose positron emission tomography. Clin Nucl Med 25:838–839
5. Tamura M, Unno K, Yonezawa S, et al. (2004) In vivo trafficking of endothelial progenitor cells: their possible involvement in tumor neovascularization. Life Sci 75:575–584
6. Basu S, Nair N (2006) Avid F-18 FDG uptake in rectal hemorrhoid in a patient with metastatic medullary carcinoma of thyroid. Indian J Gastroenterol 25:257
7. Lu YY, Lin WY (2006) Hemorrhoids: a possible cause of high FDG uptake in the rectum. Ann Nucl Med Sci 19:213–217 8. Thomson WH (1975) The nature of hemorrhoids. Br J Surg
62:542–552
9. Chung YC, Hou YC, Pan AC (2004) Endoglin (CD105) expression in the development of haemorrhoids. Eur J Clin Invest 34:107–112 10. Webb M, Chambers A, AL-Nahhas A, et al. (2004) The role of 18F-FDG PET in characterizing disease activity in Takayasu arteritis. Eur J Nucl Med Mol Imaging 31:627–634
11. Kobayashi Y, Ishii K, Oda K, et al. (2005) Aortic wall inflamma-tion due to Takayasu arteritis imaged with 18F-FDG PET coreg-istered with enhanced CT. J Nucl Med 46:917–922
12. Walter MA, Melzer RA, Schindler C, et al. (2005) The value of 18F FDG-PET in the diagnosis of large vessel vasculitis and the assessment of activity and extent of disease. Eur J Nucl Med Mol Imaging 32:674–681
13. Blockmans D, de Ceuninck L, Vanderschueren S, et al. (2006) Repetitive 18F-fluorodeoxyglucose positron emission tomography in giant cell arteritis: a prospective study of 35 patients. Arthritis Rheum 55:131–137
14. Kikuchi M, Yamamoto E, Shiomi Y, et al. (2004) Internal and external jugular vein thrombosis with marked accumulation of FDG. Br J Radiol 77:888–890
15. Miceli M, Atoui R, Walker R, et al. (2004) Diagnosis of deep septic thrombophlebitis in cancer patients by fluorine-18 fluorodeoxy-glucose positron emission tomography scanning: a preliminary re-port. J Clin Oncol 22:1949–1956
16. Khosa F, Otero HJ, Prevedello LM, Rybicki FJ, Di Salvo DN (2010) Imaging presentation of venous thrombosis in patients with cancer. AJR Am J Roentgenol 194:1099–1108
17. Calcagno C, Cornily JC, Hyafil F, et al. (2008) Detection of neo-vessels in atherosclerotic plaques of rabbits using dynamic contrast enhanced MRI and 18F-FDG PET. Arterioscler Thromb Vasc Biol 28:1311–1317
18. Strauss LG, Koczan D, Klippel S, et al. (2008) Impact of angio-genesis-related gene expression on the tracer kinetics of 18F-FDG in colorectal tumors. J Nucl Med 49:1238–1244
19. Engel H, Steinert H, Buck A, et al. (1996) Whole-body PET: physiological and artifactual fluorodeoxyglucose accumulations. J Nucl Med 37:441–446
20. Soyka JD, Strobel K, Veit-Haibach P, et al. (2010) Influence of bowel preparation before FDG PET/CT on physiologic 18F-FDG activity in the intestine. J Nucl Med 51:507–510
21. Cook GJR, Fogelman I, Maisey MN (1996) Normal physiological and benign pathological variants of 18-fluoro-2-deoxyglucose positron emission tomography scanning: potential for error in interpretation. Semin Nucl Med 26:308–314
22. Yasuda S, Takahashi W, Takagi S, et al. (1998) Factors influencing physiological FDG uptake in the intestine. Tokai J Exp Clin Med 23:241–244