ŀ
1A Open-Label, Multicentre Study of Levocetirizine for the Treatment of
Allergic Rhinitis and Urticaria in Taiwanese Patients
Sheen-Yie Fang1,2,*, Diahn-Warng Perng3, J. Yu-Yun Lee4, Ding-Yu Lin5*, Chih-Yang Huang5,6,*
1
Department of Otolaryngology, National Cheng Kung University Hospital, Tainan, Taiwan
2
Department of Otolaryngology, Chiali Hospital, Tainan, Taiwan
3
Department of Chest Medicine, Taipei Veterans General Hospital, Taipei, Taiwan; School of medicine, National Yang-Ming University, Taipei, Taiwan
4
Department of Dermatology, College of Medicine, National Cheng Kung University, Tainan, Taiwan
5
Graduate Institute of Basic Medical Science, Graduate Institute of Chinese Medical Science, China Medical University, Taichung, Taiwan
6
Department of Health and Nutrition Biotechnology, Asia University, Taichung, Taiwan
Correspondence author Sheen-Yie Fang, MD
Department of Otolaryngology
National Cheng Kung University Hospital Tainan, Taiwan 704
Republic of China
Fax: 886 6 2377404
E-mail: [email protected]
* These authors contributed equally to this paper. This study was sponsored by UCB (Taiwan) Ltd.
Abstract
Levocetirizine has been shown in observational studies in the west as an effective and satisfactory therapy for patients with allergic respiratory and skin disease. An open-label, multicentre observational study to investigate the patients’ perception of levocetirizine in the treatment of allergic rhinitis (AR) and urticaria in Taiwanese patients. Three hundred and thirty-three patients (236 AR and 97 urticaria patients) attending out-patient clinics of
medical centres across Taiwan. Patients were treated with levocetirizine 5mg once daily (AR patients for 2-4 weeks and urticaria patients for 2-6 weeks) and at the end of treatment evaluated for symptoms of disease, perception of change in symptoms, global efficacy and tolerability, global preference over previous antiallergic treatment, change in quality of sleep/daily activities, and safety and adverse events (AEs). Levocetirizine markedly improved the symptoms of AR and urticaria; with 70%-75% of AR patients and 60%-80% of urticaria patients reporting complete or marked improvements in individual symptoms. Asthma symptoms were completely or markedly improved in 44% of patients with AR and
concomitant asthma. The majority of patients were satisfied with levocetirizine therapy and 50%-70% indicated preference for levocetirizine over previous therapy. Overall, 50%-74% of all patients perceived improvements in quality of sleep/daily activities and 50%-65% of the patients rated the onset of action for levocetirizine as very rapid or rapid. Somnolence was the most common AE, reported by 7.4% of AR and 7.0% of urticaria patients. The results of this study indicated Levocetirizine is an effective and satisfactory therapy for the management of allergic respiratory and skin disease in Taiwanese subjects.
Key words: allergic rhinitis, urticaria, levocetirizine, patient perception, persistent allergic rhinitis, intermittent allergic rhinitis
Introduction
The worldwide increase in the prevalence of allergic disease, particularly allergic rhinitis (AR) and allergic skin disease such as chronic urticaria, over the last two to three decades has been well documented by the World Health Organization (WHO). Estimates indicate that 10-25% of the population worldwide is affected by AR (1, 2), whereas chronic urticaria is reported to affect as many as 25% of people at some point in their lives (3). While chronic idiopathic urticaria (CIU) is estimated to affect between 0.1-3% of the population in Europe and the USA, it is thought that the worldwide lifelong prevalence of CIU is 0.5% across different populations (4).
Several studies have demonstrated that both AR and urticaria are debilitating
conditions which adversely impact the quality of life (QOL) of affected individuals and add substantially to the socioeconomic burden (3, 5, 6, 7, 8). As mechanistic studies have
demonstrated histamine to be a major mediator involved in the development of symptoms of AR and urticaria, this has led to the recommendation for the use of oral H1 receptor
antagonists (H1 antihistamines) as the first-line pharmacotherapy for both these conditions, by
national and international guidelines (1, 9, 10).In this respect several well-controlled clinical trials have demonstrated that levocetirizine, one of the latest commercially available H1
-antihistamines, is significantly more efficacious than placebo in improving the symptoms of disease and QOL of life in children and adults with seasonal (SAR) or perennial (PAR) allergic rhinitis (11, 12, 13, 14)and adults with CIU (15, 16).Recently, levocetirizine has also been shown to significantly improve the symptoms and QOL in subjects classified as
“persistent” AR (PER) patients (17, 18),according to the ARIA (Allergic Rhinitis and its Impact on Asthma) guidelines (1); which are more applicable to modern day AR patients as classification of “intermittent” AR (IAR) or PER is based on the duration of symptoms rather than on the time of occurrence during the year and the nature of the allergen triggering the
symptoms, as is the case for SAR and PAR. Importantly, evidence from observational studies investigating real-life experience of levocetirizine in primary-care patients has also indicated that levocetirizine led to significant/complete improvement in nasal and skin symptoms in 80-90% of allergic patients, including SAR/PAR (19, 20, 21)and CIU patients (20, 21, 22). Moreover, over 75% of the patients indicated a preference for levocetirizine over their previous medications, including other antihistamines, corticosteroids, and dermatologic and ophthalmic preparations (19, 20, 21).
The observational studies, however, have investigated the effects of levocetirizine in mostly Caucasian subjects and to date there is no information on whether or not the effects of levocetirizine might be influenced by ethnic/genetic differences, as been shown to be the case for the pharmacokinetics of loratadine in Chinese subjects (23). The aim of our study was therefore to investigate the patients’ perception of the efficacy and safety of levocetirizine in Taiwanese patients with AR or urticaria, in real-life clinical practice setting. The study further aimed to evaluate the incidence of intermittent (IAR) and persistent (PER) AR in Taiwan, using the ARIA guidelines for classification of disease.
Material and Materials
Patients
Male and female subjects aged 11 to 92 years (mean age = 45 years) with a history of AR or CIU were recruited into the study. All patients provided written informed consent to
participate in the study and to be treated with levocetirizine as part of their physician’s normal practice. Patients with a history of sensitization to any of the components of Xyzal® (levocetirizine) and those already being treated with levocetirizine were excluded from the study.
Study Design
This was an open-label, multicentre observational study, conducted between May 2006 to March 2007. Subjects attending out-patient clinics in ENT, chest and dermatology
departments at six medical centres across Taiwan were assessed for demographic
characteristics and indications of AR and urticaria were confirmed by testing for allergic sensitization (skin prick tests or specific IgE), duration and persistence of symptoms, and co-morbidities according to the ARIA classification (1). Subjects with AR were supplied levocetirizine 5 mg tablets for a planned observational phase of 2-4 weeks and subjects with an indication of urticaria, levocetirizine 5 mg tablets for a planned observational phase of 2-6 weeks. The patients were instructed to take levocetirizine 5 mg tablet per day instead of their previous medication at the inception of trial and to rate their symptoms according to pre-determined scales. The patients returned to the clinic at the end of treatment and were evaluated for the symptoms of their disease and additionally for their perception of any change in their symptoms, global efficacy and tolerability, global preference over previous antiallergic treatment, change in quality of sleep/daily activities, and safety and adverse events following treatment with levocetirizine.
The study was approved by the Ethics Committee or the Institutional Review Board of each participating centre and conducted according to globally accepted standards of good clinical practice; as defined in the International Conference on Harmonization (ICH) E6 Guideline for Good Clinical Practice, 1 May 1996; in agreement with the Declaration of Helsinki, and in keeping with local laws and regulations.
ǒ
Patients with AR evaluated the severity of the five main symptoms of rhinitis, including runny nose, nasal and ocular pruritus, sneezing and nasal obstruction on a 4-point scale of 0 to 3; with 0= absent, 1= mild, 2= moderate, and 3= severe. The sum of each symptom score was also calculated as the total 5 Symptoms Score (T5SS), ranging between 0-15. The recorded symptoms of AR were further classified as being either intermittent or persistent, based on the ARIA criteria (1).
Patients with co-morbid asthma additionally rated asthma symptoms as either mild (>1x /wk, <1x /day), moderate (daily), or severe (continuous), according to the GINA guidelines (24).
Evaluation of Urticaria Symptoms
Patients with urticaria evaluated pruritus severity and duration, wheal number, size and duration, and frequency of symptoms. The severity of pruritus was rated on a 4-point scale, where as all other symptoms were rated as mild, moderate or severe, as shown:
i. severity of pruritus was rated on a scale of 0-3 with 0= absent, 1= mild, 2= moderate, and 3= severe
ii. duration of pruritus was rated as mild (< 1h/day), moderate (1-6h/day), or severe (> 6h/day)
iii. number of wheals was rated as mild (1-10 wheals), moderate (10-20 wheals), or severe (> 20 wheals)
iv. size of wheals was rated as mild (≤ 1.5cm); moderate (1.5cm and ≤ 3cm), or severe (> 3cm)
vi. frequency of symptoms was rated as mild (< every other day), moderate (every other day), or severe (daily).
Global Satisfaction and Preference for Levocetirizine
All patients and investigators evaluated global satisfaction with treatment on a visual
analogue scale (VAS) ranging from 0 cm (very dissatisfied) to 10.0 cm (very satisfied) at the end-of-treatment. The patients also indicated their preference for levocetirizine over their previous medication as being much better, somewhat better, as good as, somewhat worse, or much worse.
The onset of action for levocetirizine was rated as being very rapid (≤30min), rapid (≤30min, <1hr), or moderately rapid (≥1hr).
Effect of Treatment on Quality of Sleep and Daily Activities
The patients rated any change in the quality of sleep and daily activities as being much better, somewhat better, as good as, somewhat worse, or much worse.
Evaluation of Safety
Safety was evaluated according to the frequency, severity, nature and duration of any adverse events (AEs) experienced over the course of the study.
The sample size was estimated on the basis of how many patients would be expected to be recruited within the projected time frame for the centres involved, and in consideration of the number of patients not being too large to interfere with normal practice of the recruiting investigator. This sample size was also expected to provide a preliminary estimation of the prevalence of PER in Taiwan.
Changes in the various parameters investigated were analyzed using descriptive statistics; calculating arithmetic means and standard deviation values.
Results
Overall 333 patients (236 patients with AR and 97 patients with urticaria were enrolled into the study). A total of 217 (92%) patients with AR and 95 (98%) patients with urticaria completed the study. The 19 AR patients (8%) and 2 urticaria patients were lost to follow-up due to AEs, none of which were serious.
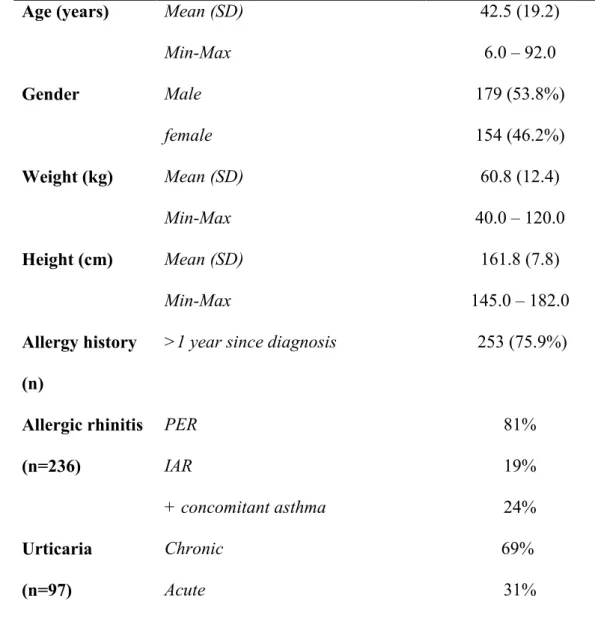
Baseline characteristics indicated that the mean ± SD age of the study cohort was 45 ± 21 years. There were approximately equal numbers of males and females, over 75% of whom had a > 1 year history of allergic disease (Table 1). Diagnosis of disease in patients with AR, using the ARIA criteria, further showed that 81% (n=191) of these patients suffered from PER and 19% (n= 45) from IAR. Furthermore, 24% (n=56) of these patients additionally suffered from concomitant asthma. Similarly, diagnosis of disease in patients with urticaria showed that 69% (n=67) of these patients suffered from chronic urticaria and 31% (n=30) from acute urticaria.
Effect of Levocetirizine on Symptoms and Perception of Overall Efficacy and Tolerability
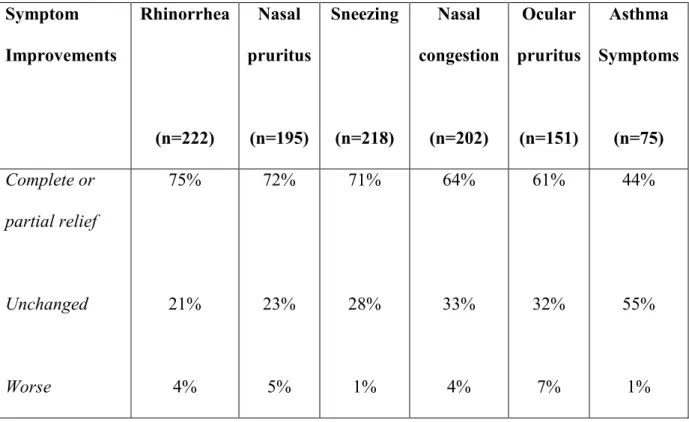
T5SS improved by 56%, from 10 (±3.3) at baseline to 4.4 (±2.3) in patients with AR at end of treatment. Assessment of improvements in individual symptoms showed that rhinorrhoea, nasal pruritus and sneezing was relieved either completely or partially in 70-75% of all patients where as nasal congestion and ocular pruritus was relieved in over 60% of the patients. Overall, 44% of all patients with concomitant asthma also achieved relief from asthma symptoms (Table 2). In contrast, <5% of all patients reported worsening of nasal
symptoms. Moreover, 58.7% and 66% of the patients assessed overall efficacy and tolerability, respectively, to be “excellent/good” (Figure 1).
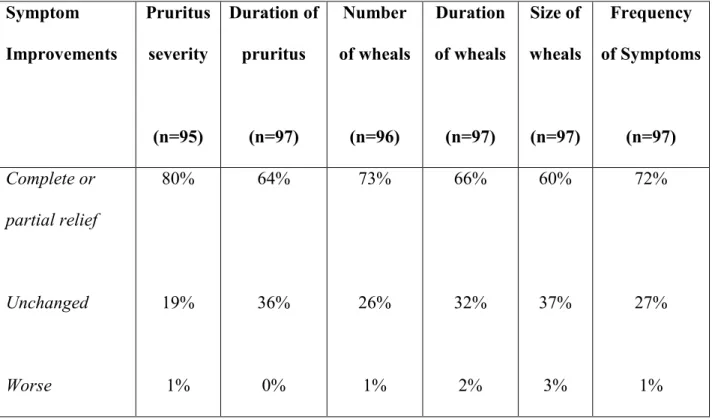
Overall, 60%-80% of all patients with urticaria also reported complete recovery or marked improvement of any individual symptom, compared with only 1%-3% of patients reporting worsening of any symptom (Table 3). The overall efficacy and tolerability were also assessed as “excellent/good” by 75% and 68% of patients, respectively (Figure 1).
Global Satisfaction and Preference for Levocetirizine
Figure 2 shows the patient’s and investigator’s global satisfaction VAS scores following treatment with levocetirizine for 2-4 and 2-6 weeks’ in patients with AR and urticaria, respectively. Global satisfaction with levocetirizine treatment was high for both sets of patients; as indicated by VAS scores of 6.9 and 7.4 for patients with AR and patients with urticaria, respectively. The physicians treating these individuals also expressed high global satisfaction with levocetirizine, by scoring similarly.
Assessment of the patients’ preference for levocetirizine indicated that 53.4% and 72% of patients with AR and urticaria, respectively, rated levocetirizine as better than their previous therapy, compared to 9.4% and 4.3% of the patients, respectively, rating
levocetirizine as worse (Figure 3).
Onset of Action Following Treatment with Levocetirizine
Overall, 50%-65% of all patients rated the onset of action as very rapid or rapid, with nearly twice as many patients with urticaria as with AR (28% vs 15%) attaining very rapid relief of their symptoms (Figure 4).
Effect of Levocetirizine on Quality of Sleep and Daily Activities
Treatment with levocetirizine improved the quality of sleep in 50%-61% of all patients and daily activities in 53%-74% of all patients (Figure 5). This was in marked contrast to less than 10% of the patients reporting any worsening in the quality of sleep or daily activities.
Safety Assessment
Overall, 32/333 patients (9.6%) reported several treatment-emergent AEs of moderate to severe intensity; of which somnolence (n= 24; 7.2%), fatigue (n= 15; 4.5%), dry mouth (n= 6; 1.8%), headache (n= 2; 6%), and asthenia (n= 2; 6%); were the most commonly occurring in >0.5% of the patients. Assessment of drug-related AEs showed that somnolence was the most common study drug-related AE, reported by 5.9% and 6.2% of the patients with AR and urticaria, respectively; followed by fatigue reported by 3.8% and 3.1% of the patients with AR and urticaria, respectively. No serious treatment-emergent adverse events (SAEs) were reported over the course of the study.
Discussion
The main objective of this observational study was to evaluate and confirm the beneficial effects of levocetirizine therapy in Taiwanese patients with AR and urticaria in ordinary clinical practice, as has been shown for Caucasian patients in the west (19, 20, 21, 22).Our study demonstrated that treatment with levocetirizine markedly improved the symptoms of AR and urticaria; with 70%-75% of all patients with AR and 60%-80% of all patients with urticaria reporting complete or marked improvements in individual symptoms of
“moderate/severe” intensity. Moreover, levocetirizine also markedly improved asthma symptoms in patients with AR and concomitant asthma, with 44% of the patients perceiving complete or marked improvements in individual symptoms of “moderate/severe” intensity. However, the finding that a comparatively short treatment period with levocetirizine led to marked or complete improvements in a substantial proportion of patients with relatively severe symptoms at baseline (as indicated by T5SS of 10 for AR patients, 81% of whom had PER, and with 69% of urticaria patients having chronic urticaria), suggests that it may be possible to achieve even greater symptom improvements in these patients, as has been shown to be the case with longer treatment with levocetirizine (17).
Our findings are nevertheless in accordance with the findings of one large study by Klimek and colleagues (20), who investigated the effect of treatment with levocetirizine 5 mg once daily for 4-6 weeks in 17,638 patients with any allergic disease. The authors
demonstrated that 80%-90% of all patients with allergic airway disease (including, SAR, PAR and asthma) and 80%-90% of all patients with allergic skin disease (including chronic urticaria, eczema, and neurodermatitis) were either symptom-free or had marked
improvements in symptoms by the end of treatment. More recently, sub-analysis of data for 1,829 patients with CIU from this large study cohort also demonstrated that levocetirizine resulted in complete or partial improvements of individual symptoms in 80%-90% of these patients (22), thus suggesting that the effect of levocetirizine in symptoms improvement was likely to be universal and similar in different allergic skin conditions. One recent study evaluated the effect of levocetirizine 5 mg once daily for 4 weeks in 1,290 primary-care patients with SAR (19). Levocetirizine significantly improved the Total 4 Symptoms Scores (T4SS; for sneezing, runny nose, itchy nose and itchy eyes) by 68%, which was further reflected as significant improvements in the global clinical condition of >90% of the patients, as indicated by the investigators’ change in the Clinical Global Impression (CGI-c) scores.
Our study additionally demonstrated that the majority of investigators and patients with AR or urticaria were satisfied with levocetirizine therapy. It is feasible that this expression of satisfaction with levocetirizine therapy is based on the findings of global satisfaction assessments and additionally the preference for levocetirizine over previous therapy, indicated by 50%-70% of the patients. These findings are also in accordance with the findings of previous studies outlined above, which have reported global satisfaction with levocetirizine in 91.7% of SAR patients and preference for levocetirizine over previous medication in 84% of SAR patients (19). Indeed, comparison with cetirizine, loratadine and desloratadine indicated levocetirizine to be preferred to these other commonly employed
antihistamines by 75%-90% of the patients with SAR (19).While 57% of the patients with allergic airway and skin disease investigated by Klimek and colleagues (20) rated
levocetirizine as better than their previous medication, subsequent analysis of data according to diagnostic grouping further indicated that about 75% of the patients with either respiratory allergies or skin allergies rated levocetirizine to be better than their previous medication (21). Moreover, most patients with allergic airway or skin diseases rated the onset of action by levocetirizine as being very rapid or rapid (20, 21, 22),as was found to be the case in the present study. Although, levocetirizine has also been shown to significantly improve the QOL of life in children and adults with AR (11, 14, 17, 18)and adults with CIU (15, 16)in several clinical trials, to our knowledge this has not been investigated in a real-life observational study. In this regard, the findings from the present observational study also confirm the beneficial effects of levocetirizine on improvements in the quality of sleep and daily activities in Taiwanese patients with AR or urticaria.
An increasing body of evidence has suggested that the traditional classifications of SAR or PAR, based on the time and the nature of major allergen/s triggering the symptoms are no longer valid, especially as the majority of AR patients have a mixed aetiology involving polysensitization to several allergens and manifestation of intermittent and persistent symptoms (25).Moreover, epidemiological studies have indicated that patients with intermittent and persistent symptoms are distinct groups of patients, and that about 40-45% of patients previously classified as SAR or PAR actually have persistent- or
intermittent-symptoms, respectively (26, 27, 28, 29, 30).Furthermore, several studies have indicated that the prevalence of PER, as defined by the ARIA guidelines, ranges from about 20% to about 55% across several countries in Europe (26, 27, 30, 33).One cross-sectional study in 591 patients consulting ENT or allergy specialists for AR across France, however, demonstrated that as many as 73% of all AR patients could be classified as suffering from
mild or moderate/severe PER, when their diagnosis was based on a specific allergic rhinitis scoring scheme and examination of allergic sensitization (skin prick tests or specific IgE) and co-morbidities according to the ARIA classification (28). To our knowledge the present study is the first to have estimated the prevalence of PER in Taiwanese patients and the finding of an 81% prevalence of PER in AR patients consulting ENT, chest and dermatology specialists is clearly in accordance with the findings of Bousquet and colleagues (28)investigating the prevalence of PER in AR patients consulting specialists in France. However, our findings are preliminary for this cohort of patients and need to be confirmed in larger population-based studies specifically designed to address this issue. This is especially important as redefining the incidence and severity of PER in Taiwanese patients is likely to have important
socioeconomic and treatment implications.
In conclusion, our study has confirmed that levocetirizine is an effective and
satisfactory therapy for the management of allergic respiratory and skin disease in Taiwanese subjects. Furthermore, the similarity in the beneficial effects of levocetirizine observed in Taiwanese and Caucasian subjects, suggests that the effects of levocetirizine are universal and unlikely to be influenced by the ethnicity of the patients.
Acknowledgements
This study was sponsored by UCB (Taiwan) Ltd. who was involved in the design and conduct of the study.
Appendix
Investigators: National Taiwan University Hospital, Taipei, Taiwan- Yang-Hsia Tai, Chia-
Ming Liu, Jih-Shuin Jerng; Taipei Veterans General Hospital, Taipei, Taiwan - Diahn-Warng
Perng, Wen-Jen Wang, Shih Hsiang Lin; Mackay Memorial Hospital, Taipei, Taiwan- Yi-
Shing Leu, Yang-Chih Lin, Chien-Liang Wu; Taicung Veterans General Hospital, Taichung,
Taiwan- Yi-Hsing Chen, Jeng-Yuan Hsu, Jui-Lung Shen; China Medical University Hospital,
Taichung, Taiwan- Chih-Jann Tai, Liang-Wen Hang, Meng-Tsi Wu; National Cheng Kung
References
1. Bauchau V. and Durham S.R. Epidemiological characterization of the intermittent and persistent types of allergic rhinitis. Allergy 60: 350-353, 2005.
2. Bauchau V. and Durham S.R. Prevalence and rate of diagnosis of allergic rhinitis in Europe. Eur. Respir. J. 24: 758–764, 2004.
3. Bachert C, Bousquet J, Canonica GW, Durham SR, Klimek L, Mullol J, Van Cauwenberge PB, Van Hammée G; XPERT Study Group. Levocetirizine improves quality of life and reduces costs in long-term management of persistent allergic rhinitis. J.
Allergy Clin. Immunol. 114: 838-844, 2004.
4. Bachert C., van Cauwenberge P., Olbrecht J.and van Schoor J. Prevalence, classification and perception of allergic and nonallergic rhinitis in Belgium. Allergy 61: 693-698, 2006.
5. Bateman ED, Hurd SS, Barnes PJ, Bousquet J, Drazen JM, FitzGerald M, Gibson P, Ohta K, O'Byrne P, Pedersen SE, Pizzichini E, Sullivan SD, Wenzel SE, Zar HJ., Global strategy for asthma management and prevention: GINA executive summary. Eur. Respir.
J. 31(1):143-78, 2008.
6. Bousquet J., Annesi-Maesano I., Carat F., Léger D., Rugina M., Pribil C., El Hasnaoui A. and Chanal I. Characteristics of intermittent and persistent allergic rhinitis: DREAMS study group. Clin. Exp. Allergy 35: 728-732, 2005.
7. Bousquet J., Neukirch F., Bousquet P.J, Gehano P., Klossek J.M., Le Gal M. and Allaf B. Severity and impairment of allergic rhinitis in patients consulting in primary care. J.
Allergy Clin. Immunol. 117: 158-162, 2006.
8. Bousquet J., van Cauwenberge P. and Khaltaev N. Allergic rhinitis and its impact on asthma. J. Allergy Clin. Immunol. 108(5 Suppl.):S147-S334, 2001.
9. Canonica GW, Bousquet J, Van Hammee G, Bachert C, Durham SR, Klimek L, Mullol J, Van Cauwenberge PB; The XPERT study group. Levocetirizine improves health-related quality of life and health status in persistent allergic rhinitis. Respir. Med. 100: 1706-1715, 2006.
10. De Blic J., Wahn U., Billard E., Alt R. and Pujazon M.C. Levocetirizine in children: evidenced efficacy and safety in a 6-week randomized seasonal allergic rhinitis trial.
Pediatr. Allergy Immunol.16: 267-275, 2005.
11. Demoly P., Allaert F-A, Lecasble M., Bousquet J. and PRAGMA. Validatioof the classification of ARIA (allergic rhinitis and its impact on asthma) Allergy 58: 672-675, 2003.
12. Greaves M.W. Chronic idiopathic urticaria. Curr. Opin. Allergy Clin. Immunol. 3: 363-368, 2003.
13. Jorissen M., Bertrand B., Stiels B. and Vandenbulcke K. Levocetirizine as treatment for symptoms of seasonal allergic rhinitis. B-ENT. 2: 55-62, 2006.
14. Kapp A. and Pichler W.J. Levocetirizine is an effective treatment in patients suffering from chronic idiopathic urticaria: a randomized, double-blind, placebo-controlled, parallel, multicenter study. Int. J. Dermatol. 45: 469-474, 2006.
15. Klimek L. and Hundorf I. Levocetirizine in allergic diseases: An open multicentre practice study of efficacy and tolerability. Allergologie 25 (Suppl. 1): S1–S7, 2002.
16. Klimek L, Wrede, H, Schott BC, Hansen I. Patients’ perception of the value of levocetirizine in allergic diseases. Clin. Drug Invest. 25: 609-614, 2005.
17. Kozel MMA and Sabroe R.A. Chronic urticaria: aetiology, management and current and future treatment options. Drugs 64: 2515-2536, 2004.
18. Leynadier F., Mees K., Arendt C. and Pinelli M.E. Efficacy and safety of levocetirizine in seasonal allergic rhinitis. Acta Otorhinolaryngol Belg. 55: 305-312, 2001.
19. Leynaert B., Neukirch C., Liard R., Bousquet J. and Neukirch F. Quality of life in allergic rhinitis and asthma. A population based study of young adults. Am. J. Respir. Crit. Care
Med. 162: 1391-1396, 2000.
20. Mösges R. and Klimek . Today's allergic rhinitis patients are different: new factors that may play a role. Allergy 62: 969-975, 2007.
21. Nettis E., Colanardi M.C., Barra L., Ferrannini A., Vacca A.and Tursi A.. Levocetirizine in the treatment of chronic idiopathic urticaria: a randomized, double-blind, placebo-controlled study. Br. J. Dermatol. 154: 533-538, 2006.
22. Pfaar O., Wrede H., Barth C., Hansen I. and Klimek L. Levocetirizine in patients with chronic idiopathic urticaria: results of a multicenter clinical practice study. Int. J. Clin.
Pharmacol. Ther. 44: 191-192, 2006.
23. Poon E., Seed P.T., Greaves M.W. and Kobza-Black A. The extent and nature of disability in different urticarial conditions. Br. J. Dermatol, 140: 667-671, 1999.
24. Potter P.C. Efficacy and safety of levocetirizine on symptoms and health-related quality of life of children with perennial allergic rhinitis: a double-blind, placebo-controlled randomized clinical trial. Ann. Allergy Asthma Immunol. 95:175-180, 2005.
25. Potter P.C. Levocetirizine is effective for symptom relief including nasal congestion in adolescent and adult (PAR) sensitized to house dust mites. Allergy 58: 893-899, 2003.
26. Settipane R.A. and Lieberman P. Update on nonallergic rhinitis. Ann. Allergy Asthma
Immunol. 86: 494-507, 2001.
27. Schoenwetter W.F., Dupclay L., Appajosyula S., Botteman M.F. and Pashos C.L.
Economic impact and quality of life burden of allergic rhinitis. Curr. Med. Res. Opin. 20: 305-317, 2004.
28. Thompson A.K., Juniper E. and Meltzer E.O. Quality of life in patients with allergic rhinitis. Ann. Allergy Asthma Immunol. 85: 338-347, 2000.
29. Todo-Bom A., Loureiro C., Almeida M.M., Nunes C., Delgado L., Castel-Branco G. and Bousquet J. Epidemiology of rhinitis in Portugal: evaluation of the intermittent and the persistent types. Allergy 62: 1038-1043, 2007.
30. Van Cauwenberge P, Bachert C, Passalacqua G, Bousquet J, Canonica GW, Durham SR,Fokkens WJ, Howarth PH, Lund V, Malling HJ, Mygind N, Passali D, Scadding GK, Wang DY. Consensus statement on the treatment of allergic rhinitis. Allergy, 55: 116-134, 2000.
31. Van Hoecke H., Vastesaeger N., Dewulf L., Sys L.and van Cauwenberge P. Classification and management of allergic rhinitis patients in general practice during pollen season.
Allergy 61: 705-711, 2006.
32. Yin O.Q., Shi X.J., Tomlinson B.and Chow M.S. Effect of CYP2D6*10 allele on the pharmacokinetics of loratadine in Chinese subjects. Drug Metab. Dispos. 33: 1283-1287, 2005.
33. Zuberbier T., Bindslev-Jensen C., Canonica W., Grattan C.E., Greaves M.W., Henz B.M., et al. EAACI/GA2LEN/EDF. EAACI/GA2LEN/EDF guideline: management of urticaria.
Tables
Table 1. Patient characteristics
IAR (intermittent allergic rhinitis): Duration of symptoms < 4 days/week or ≦ 4 weeks PER (persistent allergic rhinitis): Duration of symptoms ≥4 days/week and 4 weeks.
Age (years) Mean (SD)
Min-Max 42.5 (19.2) 6.0 – 92.0 Gender Male female 179 (53.8%) 154 (46.2%) Weight (kg) Mean (SD) Min-Max 60.8 (12.4) 40.0 – 120.0 Height (cm) Mean (SD) Min-Max 161.8 (7.8) 145.0 – 182.0 Allergy history (n)
>1 year since diagnosis 253 (75.9%)
Allergic rhinitis (n=236) PER IAR + concomitant asthma 81% 19% 24% Urticaria (n=97) Chronic Acute 69% 31%
Table 2. Proportion of patients with AR perceiving improvements in symptoms of disease Symptom Improvements Rhinorrhea (n=222) Nasal pruritus (n=195) Sneezing (n=218) Nasal congestion (n=202) Ocular pruritus (n=151) Asthma Symptoms (n=75) Complete or partial relief Unchanged Worse 75% 21% 4% 72% 23% 5% 71% 28% 1% 64% 33% 4% 61% 32% 7% 44% 55% 1%
Table 3. Proportion of patients with urticaria perceiving improvements in symptoms of disease. Symptom Improvements Pruritus severity (n=95) Duration of pruritus (n=97) Number of wheals (n=96) Duration of wheals (n=97) Size of wheals (n=97) Frequency of Symptoms (n=97) Complete or partial relief Unchanged Worse 80% 19% 1% 64% 36% 0% 73% 26% 1% 66% 32% 2% 60% 37% 3% 72% 27% 1%
Figure legends
Figure.1. Perception of overall efficacy and tolerability to levocetirizine treatment in patients with allergic rhinitis (AR) and patients with urticaria.
Figure. 2. Patient and physician Global satisfaction with levocetirizine treatment in patients with allergic rhinitis (AR) and patients with urticaria.
Figure. 3. Preference for levocetirizine over previous treatment in patients with allergic rhinitis (AR) and patients with urticaria.
Figure. 4. Onset of effect of levocetirizine treatment in (a) patients with allergic rhinitis (AR) (Dot bar: very rapid; Open bar: rapid) and (b) patients with urticaria (very rapid: ≤30min; rapid: ≥30min, <1hr; moderate: ≥1 hr)
Figure. 5. Perception of change in quality of sleep and daily activities in patients with allergic rhinitis (AR) and patients with urticaria, following treatment with levocetirizine.