Risk of carotid atherosclerosis is associated with low serum paraoxonase (PON1) activity among arsenic exposed residents in Southwestern Taiwan
Wan-Fen Lia, Chien-Wen Suna, Tain-Junn Chengb,c, Kuang-Hsi Changa, Chien-Jen Chend, Shu-Li Wanga,e,⁎
aDivision of Environmental Health and Occupational Medicine, National Health Research Institutes, Zhunan, Taiwan
bDepartment of Neurology, Chimei Medical Center, Tainan, Taiwan
cDepartment of Environmental and Occupational Health, Medical College, National Cheng Kung University, Tainan, Taiwan
dGenomics Research Center, Academia Sinica, Taipei, Taiwan
eInstitute of Environmental Medicine, College of Public Health, China Medical University Hospital, Taichung, Taiwan
a b s t r a c t a r t i c l e i n f o
Article history:
Received 5 November 2008 Revised 23 January 2009 Accepted 30 January 2009 Available online 5 February 2009
Keywords:
Arsenic Atherosclerosis Cardiovascular disease Paraoxonase Polymorphism
To understand whether human paraoxonase 1 (PON1) would modulate the risk for arsenic-related atherosclerosis, we studied 196 residents from an arseniasis-endemic area in Southwestern Taiwan and 291 age- and sex-matched residents from a nearby control area where arsenic exposure was found low. Carotid atherosclerosis was defined by a carotid artery intima-media wall thickness (IMT) of N1.0 mm. Prevalence of carotid atherosclerosis was increased in the arseniasis-endemic area as compared to the control area after adjustment for conventional risk factors (OR = 2.20, pb0.01). The prevalence was positively associated with cumulative arsenic exposure (mg/L-year) in a dose-dependent manner. Multiple logistic regression analysis showed that in the endemic group, low serum PON1 activity was an independent risk factor for atherosclerosis (OR = 4.18 low vs. high, pb0.05). For those of low PON1 activity and high cumulative arsenic exposure, the odds ratio for the prevalence of atherosclerosis was further increased up to 5.68 (pb0.05). No significant association was found between atherosclerosis and four polymorphisms of the PON gene cluster (PON1−108C/T, PON1 Q192R, PON2 A148G, PON2 C311S). However, genetic frequencies of certain alleles including PON1 Q192, PON2 G148 and PON2 C311 were found increased in the endemic group as compared to the controls and a general Chinese population, indicating a possible survival selection in the endemic group after a long arsenic exposure history. Our results showed a significant joint effect between arsenic exposure and serum PON1 activity on carotid atherosclerosis, suggesting that subjects of low PON1 activity may be more susceptible to arsenic-related cardiovascular disease.
© 2009 Elsevier Inc. All rights reserved.
Introduction
Arsenic exposure through drinking water is a global public health issue. Epidemiologic evidence has demonstrated an association between arsenic exposure and increased risk for vascular diseases.
Arsenic is the most possible cause of blackfoot disease, a peripheral vascular disease in Southwestern Taiwan that is characterized by severe arteriosclerosis and subsequent dry gangrene of affected extremities (Tseng et al., 1996). In addition to peripheral vascular disease, arsenic exposure has been related to cardio- and cerebrovas- cular dysfunction as well. Increased mortality from ischemic heart disease (Chen et al., 1996) and stroke (Chiou et al., 1997) was reported in residents of a blackfoot disease-endemic area. A study byWang et
al. (2002) using the same population has further shown a strong dose–response relationship between carotid atherosclerosis and long- term arsenic exposure.
The exact mechanisms by which arsenic induces atherosclerosis are not clear. One potential pathway is that arsenic increases oxidative stress by producing reactive oxygen species (ROS) like hydrogen peroxide, hydroxyl radicals and superoxide radicals (Wang et al., 1996;
Barchowsky et al., 1999). ROS induced by arsenic was shown to enhance endothelial cell proliferation (Barchowsky et al., 1999) and apoptosis (Wang et al., 1996; Chen et al., 1998), both leading to endothelial cell damage. Arsenic exposure increased the expression of cytokines that are involved in monocyte penetration and migration, a critical step of plaque formation, in lymphocytes of exposed individuals (Wu et al., 2003) and in culture of vascular smooth muscle cells (Lee et al., 2005). These effects were blocked by modulators of oxidative stress, indicating that arsenic exposure increased the generation of ROS and subsequently enhanced the expression of related cytokines (Lee et al., 2005). Findings in human studies also suggest a role of oxidative stress in arsenic toxicity. Blood levels of arsenic was found associated with increased level of reactive Abbreviations: BFD, Black foot disease; BMI, Body mass index; HDL, High density
lipoprotein; LDL, Low density lipoprotein; Paraoxonase 1, 2, PON1, PON2.
⁎ Corresponding author. Division of Environmental Health and Occupational Medicine, National Health Research Institutes, No. 35, Keyan Road, Zhunan Town, Miaoli County 350, Taiwan. Fax: +886 37 587 406.
E-mail address:[email protected](S.-L. Wang).
0041-008X/$– see front matter © 2009 Elsevier Inc. All rights reserved.
doi:10.1016/j.taap.2009.01.019
Contents lists available atScienceDirect
Toxicology and Applied Pharmacology
j o u r n a l h o m e p a g e : w w w. e l s ev i e r. c o m / l o c a t e / y ta a p
oxidants in Taiwanese (Wu et al., 2001) and with increased level of lipid peroxides in residents of Inner Mongolia, China (Pi et al., 2002).
Human paraoxonases (PONs) are a family of proteins including PON1, PON2 and PON3, which provide significant protection from physiological oxidative stress. PON1 is thought to attenuate the oxidation of low-density lipoprotein (LDL) and therefore protect against the development of atherosclerosis. PON1-knockout mice were prone to develop atherosclerotic plaques when fed a high-fat diet (Shih et al., 1998), while PON1-overexpressing mice showed a reduction in atherosclerotic lesion formation (Tward et al., 2002).
PON2 possesses similar anti-oxidant functions to those of PON1, as shown by a recent study in which PON2-knockout mice develop larger atherosclerotic lesions compared to their wild-type littermates (Ng et al., 2006).
Epidemiologic studies also support a role of PON1 in cardiovascular disease. A coding region polymorphism (Q192R) of the human PON1 gene (Wheeler et al., 2004), as well as low serum PON1 activity levels (Jarvik et al., 2000; Mackness et al., 2001; Mackness et al., 2003), were both associated with increased incidence of coronary heart disease.
Evidence of the association between PON2 polymorphisms and cardiovascular disease is less conclusive. However, several studies have linked a coding region polymorphism at residue 311 (S311C) to the disease in both Chinese (Pan et al., 2002; Su et al., 2005) and European Whites (Leus et al., 2001; Chen et al., 2003). Another amino acid substitution at codon 148 (A148G) was found associated with variations in total and LDL cholesterol (Hegele et al., 1998) and fasting plasma glucose levels (Hegele et al., 1997).
Due to the strong implication of oxidative stress in arsenic-induced atherosclerosis, the present study was to investigate whether the polymorphisms of two anti-oxidant proteins, PON1 and PON2, as well as the serum activity level of PON1, may modulate the individual risk for atherosclerosis in residents of arseniasis-endemic area. For this purpose, we determined carotid artery intima-media wall thickness (IMT) in long-term residents of the endemic area, and in age- and sex- matched subjects living in a nearby control area where arsenic exposure was found low. IMT has been widely used as a surrogate marker for atherosclerosis (de Groot et al., 2004) and a strong predictor of future cardiovascular disease (Lorenz et al., 2007). Results of this study may help us understand a possible interaction between arsenic exposure and PON genes that are known to be involved in regulation of atherosclerosis.
Methods
Study areas. This study included a community-based cohort with previous high-level arsenic exposure, recruited from an arseniasis- endemic area in Southwestern Taiwan in 2002, and a non-exposed population recruited from a control area in 2004. The arseniasis- endemic area included Homei, Fuhsin and Hsinming villages in Putai Town, where the prevalence of blackfoot disease was the highest in Taiwan (9.6–13.6%). Residents of this area had a history of long-term exposure to arsenic through consumption of high-arsenic artesian well water (median = 0.7–0.93 mg/L, as measured during 1940s to 1960s) since 1910s, although well water was no longer used for drinking or cooking after the implementation of tap water in the mid- 1970s (Kuo, 1964; Lo et al., 1977). The non-exposed control area was Chiali Town where the arsenic concentration of well water was very low, according to the results of surveys conducted in 1960s and 1970s (Kuo, 1964; Lo et al., 1977). Climate, ethnic background (Han Chinese), urbanization degree and socioeconomic status were similar between Putai and Chiali.
Study subjects. A cohort that consisted of 898 subjects who were over 30 years old and lived in the arseniasis-endemic area was established between 1989 and 1990 as described before (Chen et al., 1995). In January 2002, approximately 490 subjects who still resided in the area were invited to participate in this study and 291 subjects were recruited for assessment of carotid atherosclerosis measured by Doppler carotid ultrasound scan. Their blood pressure, fasting plasma glucose and fasting serum lipids were also measured. Among 291 subjects who underwent Doppler carotid ultrasound scan, 40 subjects were those whose original ID code were missing, 45 subjects did not have DNA samples and 10 subjects did not have complete blood biochemical parameters, and therefore 196 subjects were included in thefinal statistical analysis forTables 1 and 2. Among these subjects, 19 of them did not have serum samples for PON1 activity assay and therefore a total of 177 subjects were listed inTables 5and 6. All subjects who had both carotid atherosclerosis and genotype data available, regardless of their blood biochemical parameters, were presented inTable 3, and subjects who also had serum PON1 activity measured were listed inTable 4. Residents in the non-exposed area were selected as controls. Age- and gender-stratified (from 35- to 85- year-old, every 5-year as a group) subjects were randomly drawn
Table 1
Characteristics of subjects from the arseniasis-endemic area and non-exposed control area
Characteristics Arseniasis-endemic area (n = 196) Non-exposed control area (n = 291) p-value
Age 61.6 ± 8.71 61.5 ± 10.07 0.897a
Male (%) 88 (44.9) 114 (39.2) 0.209c
BMI (kg/m2) 25.4 ± 3.78 24.3 ± 3.20 0.002a
Waist/hip ratio 0.86 ± 0.10 0.86 ± 0.08 0.996a
Smoking (current or ever) (%) 46 (23.5) 38 (13.1) 0.003c
Alcohol (current or ever) (%) 18 (9.3) 25 (8.7) 0.826c
SBP (mm Hg) 137.1 ± 20.6 138.9 ± 18.1 0.313a
DBP (mm Hg) 81.3 ± 14.0 83.7 ± 10.7 0.039a
Glucose (mg/dL) 106.8 ± 36.8 110.5 ± 30.2 b0.001b
Cholesterol (mg/dL) 203.2 ± 36.8 201.6 ± 37.6 0.560b
Triglycerides (mg/dL) 129.3 ± 86.3 132.2 ± 89.9 0.747b
HDL (mg/dL) 40.3 ± 12.4 44.6 ± 12.5 b0.001b
LDL (mg/dL) 142.3 ± 36.3 124.5 ± 36.0 b0.001b
Total urinary Arsenic (μg/g)d,e 40.3 (36.6–44.5) 41.7 (38.8–44.8) 0.810b
Inorganic Arsenic (μg/g)d,e 5.2 (4.6–5.9) 3.6 (3.3–3.9) b0.001b
Organic Arsenic (μg/g)d,e 32.7 (29.3–36.6) 37.0 (34.3–39.9) 0.171b
IMTN1 mm (%) 41 (20.9) 32 (11.0) 0.003c
Data were presented as mean ± S.D. or geometric mean (95% CI).
SBP: Systolic blood pressure; DBP: Diastolic blood pressure.
aDifferences were analyzed by Student's t-test.
b Differences were analyzed by Mann–Whitney test.
c Differences were analyzed by Chi-square test.
d Urinary arsenic was adjusted by urinary creatinine and presented asμg/g of creatinine.
e Numbers of subjects who had urinary arsenic measured were 168 (n = 168) for the endemic area and 287 (n = 287) for the control area.
according to the age distribution of the exposed group. Subjects were asked not to consume any seafood 3 days before urine collection in order to limit the organic arsenic exposure from foods. This protocol was approved by the institutional review board of National Health Research Institutes and informed consent was obtained from each subject before the study.
Assessment of arsenic exposure. An index of cumulative arsenic exposure from drinking artesian well water was derived as described previously (Chen et al., 1996) to represent the overall arsenic exposure for each subject. Briefly, the individual cumulative arsenic exposure (mg/L-year) was defined as the sum of products, derived by multiplying the arsenic concentration in well water (mg/L) by the years of consuming the well water (year) during consecutive periods of living in different villages. Because the consumption of well water by a subject was not limited to a single well, the arsenic concentration in well water was represented by the median arsenic level in well water of the village where the subject had lived. Urinary samples were collected from each subject for measurement of current arsenic exposure. Four arsenic species in urine including arsenite (AsIII), arsenate (AsV), monomethylarsonic acid (MMA) and dimethylarsinic acid (DMA) were quantified. Urinary arsenic was analyzed using high- performance liquid chromatography (HPLC) coupled with flow injection atomic absorption spectrometry. The HPLC system consisted
of a solvent delivery pump (PU-1580, Jasco, Tokyo, Japan) and a silica- based anion-exchange column (Nucleosil 10 SB, 250 mm × 4.6 mm;
Phenomenex, CA, USA) with a guard column packed with the same material. Aflow injection analysis system (FIAS-400, PerkinElmer, CT, USA) was designed as the on-line interface to the continuous hydride generation system (Analyst 100, PerkinElmer, CT, USA) used in this study. With this method, the within-day and between-day precision (coefficient of variance, CV%) for AsIII, AsV, MMA, and DMA determinations ranged from 1.0 to 3.7% were observed. Furthermore, the recoveries for AsIII, AsV, MMA, and DMA were 99.0, 98.9, 99.0, and 99.0% while the detection limits were 0.75, 1.47, 1.19, and 0.76μg/L, respectively. Inorganic arsenic was the sum of AsIII and AsV, organic arsenic was the sum of MMA and DMA, and total urinary arsenic was the sum of four arsenic species.
Assessment of carotid atherosclerosis. Carotid artery imaging was performed by high-resolution B-mode ultrasound scans using a hand- carried model SonoSite™180 (SonoSite Inc., Bothell, WA, USA) equipped with a 7.5 MHz transducer. Each examination cycle included sequential longitudinal and transverse views of the common carotid artery (CCA), the carotid bifurcation and the internal carotid artery (ICA) bulb. All ultrasound images were recorded and then digitalized and transferred to a computer for further analysis. Images were performed and analyzed by one neurologist and confirmed by Table 2
Multiple logistic regression analysis of risk factors associated with carotid atherosclerosis
Risk factors N ORa(95%C.I.) ORb(95%C.I.) ORc(95%C.I.) ORd(95%C.I.)
Age b55 140 1
55–65 160 3.01 (1.17–7.77)⁎
N65 187 7.71 (3.20–18.62)⁎⁎⁎
Gender Male 202 1
Female 285 0.53 (0.32–0.88)⁎
BMI b24 205 1
24–26 121 1.26 (0.66–2.42)
N26 161 1.65 (0.93–2.94)
Smoking status No 403 1
Yes or ever 84 2.06(1.12–3.68)⁎
LDL (mg/dL) b130 256 1 1
≥130 231 1.72 (1.04–2.85)⁎ 1.74 (1.01–3.00)⁎
HDL (mg/dL) b35 142 1 1
35 345 0.81 (0.48–1.39) 1.19 (0.64–2.21)
Triglycerides (mg/dL) b130 307 1 1 1 1
≥130 180 1.40 (0.85–2.32) 1.17 (0.68–2.00) 1.15 (0.64–2.03) 0.95 (0.52–1.72)
Total cholesterol (mg/dL) b220 340 1 1 1 1
≥220 147 1.77 (1.06–2.96)⁎ 1.85 (1.07–3.22)⁎ 1.76 (0.86–3.63) 1.53 (0.73–3.21)
Hypertensione No 236 1 1 1
Yes 251 2.30 (1.36–3.91)⁎⁎ 1.65 (0.93–2.94) 1.71 (0.95–3.05)
Diabetesf No 396 1 1 1
Yes 91 4.04 (2.35–6.93)⁎⁎⁎ 2.66 (1.47–4.82)⁎⁎ 2.70 (1.48–4.91)⁎⁎
Area Non-exposed 291 1 1 1 1
Arseniasis 196 2.14 (1.29–3.54)⁎⁎ 2.12 (1.22–3.68)⁎⁎ 1.91 (1.08–3.39)⁎ 2.20 (1.22–3.99)⁎⁎
Cumulative As exposure (mg/L-year) b0.1 345 1 1 1 1
0.1–15.0 71 1.40 (0.68–2.88) 2.14 (0.96–4.77) 1.95 (0.86–4.39) 2.20 (0.95–5.09)
N15.0 71 3.42 (1.88–6.25)⁎⁎⁎ 2.62 (1.37–5.01)⁎⁎ 2.38 (1.20–4.71)⁎ 2.74 (1.34–5.60)⁎⁎,g
Years of drinking b1 313 1 1 1 1
1–20 70 1.53 (0.73–3.19) 2.70 (1.16–6.28)⁎ 2.46 (1.04–5.78)⁎ 2.79 (1.15–6.78)⁎
N20 103 3.06 (1.75–5.37)⁎⁎⁎ 2.28 (1.25–4.18)⁎⁎ 2.11 (1.13–3.97)⁎ 2.32 (1.22–4.43)⁎
As level in well water (ppb) Low:b1 345 1 1 1 1
Median: 1–700 72 2.73 (1.47–5.08)⁎⁎ 3.00 (1.53–5.89)⁎⁎ 2.71 (1.35–5.43)⁎⁎ 3.04 (1.48–6.24)⁎⁎
High:N700 70 1.91 (0.97–3.73) 1.91 (0.92–3.99) 1.71 (0.80–3.67) 1.99 (0.90–4.37)
aModel A: crude OR (95% CI).
b Model B: adjusted for age, gender, BMI and smoking.
c Model C: adjusted for age, gender, BMI, smoking, LDL and HDL.
d Model D: adjusted for age, gender, BMI, smoking, LDL, HDL, hypertension and diabetes.
eHypertension was defined as (1) an average systolic blood pressure ≧140 mm Hg, (2) an average diastolic blood pressure ≧90 mm Hg or 3) regularly treated with anti- hypertensive agents.
f Diabetes was defined as 1) fasting glucose level ≧126 mg/dL or 2) regularly treated with oral hypoglycemic agents or insulin.
g Trend analysis, p = 0.003.
⁎ pb0.05.
⁎⁎ pb0.01.
⁎⁎⁎ pb0.001.
another; both were blinded to subjects' status. The intima-media thickness (IMT) was measured in the far wall of two segments of carotid arteries on both sides. Two segments were identified on each side: the distal 1.0 cm of CCA to the bifurcation, and the proximal 1.0 cm of ICA to the bifurcation. A total of four measurements were determined for each subject. Carotid atherosclerosis was defined as the mean of four measurementsN1 mm.
Laboratory examinations. Fasting total serum cholesterol, triglycerides, and HDL and LDL cholesterol-level were determined using Beckmen SYNCHRON LX20 System (Beckmen Coulter, CA, USA).
Genotype analysis of PON polymorphisms. Genomic DNA was extracted from buffy coat using a commercial kit (PUREGENE®, Gentra, Minneapolis, MN, USA). All genotyping was conducted by polymerase chain reaction (PCR) amplification followed by polymorphism-specific restriction enzyme digestion and gel analysis.
The PON1 Q192R polymorphism was determined following a protocol developed byHumbert et al. (1993)and the−108C/T polymorphism by Brophy et al. (2001). The protocol for determining the PON2 polymorphisms were described previously (Mochizuki et al., 1998).
PON1 activity assay. Serum PON1 activity was measured using 1.2 mM paraoxon in 0.1 M Tris–HCl, pH 8.5, 2 mM CaCl2and 2 M NaCl at 37 °C. Reaction was monitored at 405 nm and an extinction coefficient of 18 mM− 1cm− 1was used for activity calculation. PON1 activity was expressed as units/liter (units =μmol of hydrolysis product formed per min). The assay was performed in a Molecular Devices 96-well microplate spectrophotometer SPECTRAMax 190 (Sunnyvale, CA, USA).
Statistical analysis. Differences in demographic characteristics between groups were analyzed using Students' t-test, Mann–Whitney test or chi-square test. To evaluate the association between risk factors and the prevalence of carotid atherosclerosis, a multiple logistic regression analysis was performed to calculate the odds ratios (ORs) and 95% confidence intervals (CIs). Multiple logistic regression analysis, after adjusting for traditional risk factors, was used to test the association between PON genotypes, PON1 activity and prevalent atherosclerosis. Trend analysis was derived from logistic regression models, showing dose-dependent effects of risk factors. Allele frequency, genotype distribution and deviation from Hardy–Weinberg equilibrium were evaluated using chi-square test. Attributable risk (AR) adjusted for confounding factors was estimated by the following:
AR = 1−ΣΣρij/ RRijwhere the quantityρijrepresents the proportion of diseased individuals with exposure at i level and confounding at j level, while RRijrepresents the relative risk for level i of exposure given level j of adjusting factors (Bruzzi et al., 1985; Benichou, 2001).
All analyses were performed using SPSS statistical software (Version 10.0, SPSS Inc., Chicago, USA).
Results
A total of 196 long-term residents living in the arseniasis-endemic area and 291 subjects from the control area were included in this study. All subjects had a complete questionnaire and IMT measured.
No differences were found in age and gender, although the subjects of the endemic area had higher body mass index (BMI) and higher smoking rate than the control group (Table 1). Because residents in the endemic area have ceased the consumption of well water for over 20 years, the current arsenic exposure was comparable between two groups, as shown by total arsenic level in urine (Table 1). However, the level of urinary inorganic arsenic was higher in the endemic group than the control group (pb0.001).
The prevalence of carotid atherosclerosis, defined as IMTN1 mm, was significantly higher in the endemic group compared to controls (20.9% vs. 11.0%, p = 0.003) (Table 1). Traditional risk factors for atherosclerosis such as systolic blood pressure, triglycerides and total cholesterol level, were not different between two groups. Subjects of the endemic group even had lower diastolic blood pressure and fasting plasma glucose than controls. However, the endemic group had worse lipoprotein profile as compared to controls, with both LDL- Table 3
Distribution of PON1 and PON2 polymorphisms in the arseniasis-endemic area and non-exposed control area
Arseniasis area N (%) Non-exposed area N (%) Reference populationa p-value
PON1 Q192R QQ 35 (18.5) 32 (12.8) 0.083b
QR 88 (46.6) 108 (43.0)
RR 66 (34.9) 111 (44.2)
Allele frequency Q 0.42 0.34 0.35 0.022c
R 0.58 0.66 0.65
PON1-108C/T CC 45 (21.8)d 66 (22.6) 0.113b
CT 120 (58.3) 146 (50.0)
TT 41 (19.9) 80 (27.4)
Allele frequency C 0.51 0.48 0.55 0.295c
T 0.49 0.52 0.45
PON2 A148G AA 109 (53.9) 210 (71.4) b0.001b
AG 85 (42.1) 75 (25.5)
GG 8 (4.0) 9 (3.1)
Allele frequency A 0.75 0.84 0.83 b0.001c
G 0.25 0.16 0.17
PON2 C311S CC 18 (9.3)d 10 (3.6) 0.025b
CS 52 (26.8) 68 (24.6)
SS 124 (63.9) 198 (71.8)
Allele frequency C 0.23 0.16 0.17 0.009c
S 0.77 0.84 0.83
aAllele frequencies of PON1 and PON2 polymorphisms in a reference Chinese Han population (Wang et al., 2003).
b Chi-square test for differences in genotype distribution between the arseniasis endemic area and non-exposed control area.
c Chi-square test for differences in allele frequency between the arseniasis endemic area and non-exposed control area.
d Significantly deviated from Hardy–Weinberg equilibrium by Chi-square test (pb0.05).
Table 4
Serum PON1 activity level of subjects from the arseniasis-endemic area and non- exposed control area
PON1 Q192R Serum PON1 activity (units/L)a p-valueb
Arseniasis area (N) Non-exposed area (N)
QQ 668.2 ± 372.1 (29) 340.7 ± 87.5 (32) b0.001
QR 844.6 ± 399.1 (76) 730.0 ± 149.6 (108) 0.024
RR 1067.0 ± 463.2 (55) 1048.9 ± 231.1 (110) 0.668
aPON1 activity was measured using paraoxon as substrate.
b Significant differences were analyzed by Mann–Whitney test.
and HDL-cholesterol reaching the borderline risk level (Table 1).
Logistic regression analysis revealed that, after adjusting for age, gender, BMI, smoking, HDL, LDL, hypertension and diabetes, subjects living in the endemic area had significantly higher risk (OR=2.20, pb0.01) for developing atherosclerosis than residents of the control area (Table 2). Prevalence of atherosclerosis was associated with cumulative arsenic exposure (defined as “arsenic level of well water”
multiplied by “drinking years”, mg/L-year) in a dose-dependent manner (p = 0.003 for trend analysis) (Table 2). Compared to subjects with the cumulative arsenic exposure less than 0.1 mg/L-year, those who had highest arsenic exposure (N15 mg/L-year) showed a significantly increased risk for carotid atherosclerosis (OR=2.74, pb0.01). The significantly positive association was also found for drinking years although the dose-dependence was less clear (Table 2).
Table 3showed the distribution of PON1 and PON2 polymorphisms in two study groups, as well as a reference Chinese population (Wang et al., 2003). For the control group, the genotype distribution of the four polymorphisms was in Hardy–Weinberg equilibrium and the allele frequencies were similar to those found in the reference Chinese population. However, the distribution of these polymorphisms in the endemic group was significantly different from it was in the control group or the reference population. For PON1 Q192R, PON2 A148G and PON2 C311S polymorphisms, the allele frequencies were significantly different between two study groups. The frequencies of the risk alleles that have been linked to atherosclerosis or increased cholesterol levels, including the PON1 R192 allele, the PON2 S311 allele and the PON2 A148 allele, were found decreased in the endemic group compared to the control or reference group. Although the allele frequency of the PON1−108C/T polymorphism was similar between two groups, the genotype distribution in the endemic group was significantly deviated from Hardy–Weinberg equilibrium, with more heterozygotes and less TT homozygotes found than expected.
A genotype-dependent difference in serum PON1 activity was also found between the endemic and control group (Table 4). Subjects who were PON1 QQ192 or PON1 QR192 genotype and lived in the endemic area had significantly higher PON1 activity compared to those of the
same genotype but from the control area. Subjects of PON1 RR192 genotype, however, had similar serum PON1 activity no matter where their residential area was.
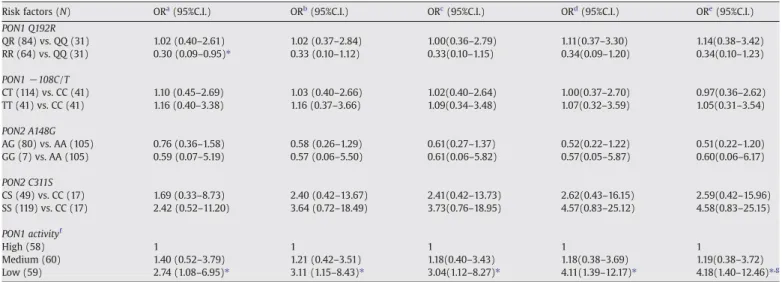
Multiple logistic regression analysis was carried out to examine the relationship between carotid atherosclerosis and PON polymorphisms in the endemic group (Table 5). Only the polymorphism of PON1 Q192R showed a slight association which became insignificant after adjustment for other risk factors. None of other polymorphisms were associated with atherosclerosis. Interestingly, a significantly negative association with atherosclerosis was found for serum PON1 activity in the endemic group (p = 0.009 for trend analysis) (Table 5). Subjects were divided into tertiles and assigned as low, medium, and high group, based on their serum PON1 activity. The odds ratio for atherosclerosis comparing subjects in the low vs. high group was 4.11 (pb0.05) after adjustment for other conventional risk factors including age, sex, BMI, smoking, LDL, HDL, hypertension and diabetes (Model D,Table 5). The negative association with decreasing PON1 activity was even more evident after adjusted for cumulative arsenic exposure (OR = 4.18, Model E), indicating that low serum PON1 activity was an independent risk factor for atherosclerosis.
We further analyzed the joint effect between PON1 activity and cumulative arsenic exposure on atherosclerosis. Subjects of the endemic area were divided into four sub-groups, with the sub-group of high serum PON1 activity and low cumulative arsenic exposure as the reference group (Table 6). A clear and significant trend for athero- sclerosis risk was found when PON1 activity decreasing while cumulative exposure increasing (p = 0.036 for trend analysis). Subjects who had low PON1 activity and high exposure showed the greatest risk for atherosclerosis compared to others (OR = 5.68, pb0.05).
Discussion
This study confirmed the association between long-term arsenic exposure and carotid atherosclerosis, which has been reported previously by Wang et al. (2002). In this study we included an external cohort as the control group and showed that living in the Table 5
Multiple logistic regression analysis of polymorphisms and PON1 activity associated with carotid atherosclerosis in subjects of arseniasis-endemic area
Risk factors (N) ORa(95%C.I.) ORb(95%C.I.) ORc(95%C.I.) ORd(95%C.I.) ORe(95%C.I.)
PON1 Q192R
QR (84) vs. QQ (31) 1.02 (0.40–2.61) 1.02 (0.37–2.84) 1.00(0.36–2.79) 1.11(0.37–3.30) 1.14(0.38–3.42)
RR (64) vs. QQ (31) 0.30 (0.09–0.95)⁎ 0.33 (0.10–1.12) 0.33(0.10–1.15) 0.34(0.09–1.20) 0.34(0.10–1.23)
PON1−108C/T
CT (114) vs. CC (41) 1.10 (0.45–2.69) 1.03 (0.40–2.66) 1.02(0.40–2.64) 1.00(0.37–2.70) 0.97(0.36–2.62)
TT (41) vs. CC (41) 1.16 (0.40–3.38) 1.16 (0.37–3.66) 1.09(0.34–3.48) 1.07(0.32–3.59) 1.05(0.31–3.54)
PON2 A148G
AG (80) vs. AA (105) 0.76 (0.36–1.58) 0.58 (0.26–1.29) 0.61(0.27–1.37) 0.52(0.22–1.22) 0.51(0.22–1.20)
GG (7) vs. AA (105) 0.59 (0.07–5.19) 0.57 (0.06–5.50) 0.61(0.06–5.82) 0.57(0.05–5.87) 0.60(0.06–6.17)
PON2 C311S
CS (49) vs. CC (17) 1.69 (0.33–8.73) 2.40 (0.42–13.67) 2.41(0.42–13.73) 2.62(0.43–16.15) 2.59(0.42–15.96)
SS (119) vs. CC (17) 2.42 (0.52–11.20) 3.64 (0.72–18.49) 3.73(0.76–18.95) 4.57(0.83–25.12) 4.58(0.83–25.15)
PON1 activityf
High (58) 1 1 1 1 1
Medium (60) 1.40 (0.52–3.79) 1.21 (0.42–3.51) 1.18(0.40–3.43) 1.18(0.38–3.69) 1.19(0.38–3.72)
Low (59) 2.74 (1.08–6.95)⁎ 3.11 (1.15–8.43)⁎ 3.04(1.12–8.27)⁎ 4.11(1.39–12.17)⁎ 4.18(1.40–12.46)⁎,g
aModel A: crude OR (95% CI).
b Model B: adjusted for age, gender, BMI and smoking.
c Model C: adjusted for age, gender, BMI, smoking, LDL and HDL.
d Model D: adjusted for age, gender, BMI, smoking, LDL, HDL, hypertension, diabetes.
eModel E: adjusted for age, gender, BMI, smoking, LDL, HDL, hypertension, diabetes and cumulative As exposure.
f PON1 activity: Low (55.1–608 U/L), Medium (616.5–1074 U/L), High (1090–2005 U/L).
g Trend analysis, p = 0.009.
⁎ pb0.05.
arseniasis-endemic area would increase risk for atherosclerosis considerably (OR = 2.20;Table 2). Most subjects from the endemic area had a previous arsenic exposure history and therefore, using an external cohort would help increase the sample size of non-exposed controls. Meanwhile, a possible selection survival may exist in the endemic group, and the use of an external control group could avoid the bias that may cover up the otherwise existed link between arsenic exposure and risk of atherosclerosis. The risk for development of atherosclerosis was increasing with the cumulative arsenic exposure in a dose-dependent manner, and a 2.74-fold risk was found for subjects whose exposure level was more than 15 mg/L-year (Table 2).
It is comparable to the data reported by Wang et al, where they found the odds ratio was 3.1 for those who had cumulative arsenic exposure of≥20 mg/L-year. We must point out that in our study, carotid IMT was measured in different time for two study groups, with the endemic group measured in 2002 while the control group in 2004.
Due to the lag of 2 years between measurements, it is possible that new cases of atherosclerosis in the endemic group would be identified if the assessment were carried out in 2004 along with the control group. Therefore, there is a possibility that we underestimate the prevalence of atherosclerosis in the endemic group, and the magnitude of risk due to arsenic exposure might be even greater than our result showed.
Our results also demonstrated that low serum PON1 activity acted as an independent risk factor for carotid atherosclerosis in the endemic group, even after adjustment for cumulative arsenic exposure (Table 5). Thisfinding indicates a possibility of using PON1 activity as a susceptible biomarker to monitor the cardiovascular health for the arsenic exposed group. A major challenge of this proposal is that our study is a cross-sectional study, so it is difficult to establish the causal–effect relationship between low PON1 activity and carotid atherosclerosis. It is arguable that the reduction in PON1 activity may result from the presence of atherosclerosis rather than be a direct cause of the disease. However, previous studies have shown that in two large prospective cohorts, low serum PON1 activity was a successful predictor for cardiovascular diseases such as myocardial infarction and stroke (Mackness et al., 2003; Bhattacharyya et al., 2008). This direct prospective evidence not only confirms the protective role of PON1 in atherosclerosis but supports the proposal of using PON1 activity to predict future cardiovascular outcomes.
Whether serum PON1 activity could be used as a susceptible biomarker for arsenic exposed group, however, needs to be further investigated in a prospective way using a large cohort.
Another major finding of this study is the joint effect between arsenic exposure and low PON1 activity on atherosclerosis in the endemic group. High arsenic exposure together with low PON1 activity would render individuals a 5.68-fold increased risk for developing atherosclerosis (Table 6). To understand the contribution of each factor to the disease, we calculated attributable risk (AR) of cumulative arsenic exposure and PON1 activity after adjusted for other risk factors.
The multivariate-adjusted AR was 27% for arsenic exposure, 35% for PON1 activity and 73% for both factors combined. This information
indicates that for the endemic group, PON1 activity alone contributes to the disease considerably and when combined with arsenic exposure, the contribution to the disease is elevated further.
PON1 is believed to promote the anti-inflammatory and anti- oxidant functions of lipoproteins. A recent study has demonstrated that low PON1 activity is associated with increased systemic oxidative stress in humans as shown by levels of oxidized fatty acids (Bhattacharyya et al., 2008). The most likely mechanism by which PON1 exerts its anti-atherogenic functions is to break down oxidized lipids and to reduce LDL oxidation, although the physio- logical substrates for PON1 remain unclear. It has been proposed that arsenic is involved in the formation of atherosclerosis because it induces oxidative stress, which may in turn increase the levels of cumulated oxidized lipoproteins (Pi et al., 2002; Wang et al., 2007).
A recent article described that atherosclerotic lesions in arsenic- exposed mice showed increased accumulation of malondialdehyde and 4-hydroxy-trans-2-nonenal, two abundant products generated from the oxidation of LDL (States et al., 2009). Ourfinding that low PON1 activity is associated with increased risk provides further support for the oxidation hypothesis of arsenic-induced athero- sclerosis. However, more studies are needed to elucidate the exact role of PON1 in protection against atherosclerosis resulted from arsenic exposure.
An interestingfinding of this study is the distorted distribution of PON1 and PON2 polymorphisms in the endemic group (Table 3). The endemic group and the control group had a similar ethnic background as both groups were composed of Han Chinese. No differences in genotype distribution or allele frequency were found between the control group and a reference Chinese general population, assuring that our genotyping results were accurate and reliable. For the endemic group, we found that either the frequencies of risk alleles were decreased (e.g. the PON1 R192 allele) or more heterozygotes were observed than expected (e.g.−108C/T). These results suggest a possible survival selection for the PON1 and PON2 polymorphisms in the endemic group. Although we did notfind a significant association between the PON1 Q192R polymorphisms and atherosclerosis, which has been suggested by other studies, it could be due to the survival selection of the protective QQ genotype. The fact that subjects carrying the Q192 alleles were over-presented in the endemic group (Table 3) may dilute the effects of the polymorphism on atherosclerosis risk, which may exist otherwise. The impact of PON1 polymorphisms on survival has been reported previously. Christiansen et al. (2004) examined the effects of PON1 polymorphisms on mortality in a Danish population and found that PON1 RR192 homozygosity was associated with increased mortality in women. This relationship between PON1 polymorphisms and survival may explain why the frequencies of protective alleles are increased in the endemic group.
Moreover, the possible survival selection was also found for PON1 activity. For individuals of PON1 QQ192 or QR192 genotypes who were over-presented in the endemic area, they had significantly increased PON1 activity compared to those of the same genotypes but from the control area (Table 4). Modulation of serum PON1 activity by metal exposure, such as lead, has been shown both in vitro (Cole et al., 2002) and in lead workers (Li et al., 2006). Although it is possible that the increase of PON1 activity is a direct result of arsenic exposure by interacting with the protein or inducing the gene expression, evidence so far does not show a modulating effect of arsenic on PON1 activity.
First, no direct interaction was found between arsenic and PON1 protein, as shown by Cole et al. (2002) that arsenic treatment did not inhibit serum PON1 activity. Second, no significant correlation was found between PON1 activity and cumulative arsenic exposure in the endemic group. Third, high arsenic exposure in these subjects was terminated decades ago so the possible effects of arsenic on PON1 protein or gene expression, if any, might no longer exist. Therefore, the increase of PON1 activity found in this study is more likely a result of survival selection. Thisfinding indicates that for subjects carrying the Table 6
Joint effect of PON1 activity and cumulative As exposure on carotid atherosclerosis in subjects of arseniasis-endemic area
PON1 activitya Cumulative Asb N Prevalence (%) ORc(95% CI)
High Low 41 3 (7%) 1
High 46 11 (24%) 4.12 (0.81–21.08)
Low Low 48 10 (21%) 5.15 (1.10–24.04)⁎
High 42 13 (31%) 5.68 (1.20–26.91)⁎,d
aPON1 activity: High (892.6–2005 U/L), Low (55.1–890.5 U/L).
b Cumulative A exposure: Low (0–11.3 mg/L-year), High (11.6–41.5 mg/L-year).
c Adjusted for age, gender, BMI, smoking, HDL, LDL, hypertension and diabetes.
d Trend analysis, p = 0.036.
⁎ pb0.05.
Q192 allele, who have high PON1 activity might be selected over the years.
A significant limitation of our study is the lack of individual assessment of arsenic exposure at the time when exposure was continuous. Instead, the exposure assessment of this study was performed in an ecologic manner as most arsenic researches in general populations (Navas-Acien et al., 2005). Arsenic exposure indexes used in this study were created previously and proved to reflect past arsenic exposure effectively (Chen et al., 1996; Tseng et al., 2005). In fact, we did measure individual arsenic level in urine for both groups but did not find any significant correlation between urinary arsenic and atherosclerosis (data not shown).
However, this should not be considered a drawback of ourfindings because urinary arsenic represents current exposure only, whereas cardiovascular outcomes are believed to be long-term effects of arsenic exposure.
In conclusion, we found that carotid atherosclerosis is associated with long-term consumption of arsenic-contaminated drinking water and this risk is further increased by low serum PON1 activity. This finding suggests that individuals who are exposed to arsenic, particularly those of low PON1 activity, should be monitored for their cardiovascular health regularly.
Conflict of interest statement
The authors declare that there are no conflicts of interest.
Acknowledgments
We thank Dr. Y.-H. Lu for taking ultrasound carotid artery images, Dr. L.-Y. Tsai for laboratory biochemical analysis, Dr. Y.-L. Hwang for urinary arsenic analysis, Ms. H.-Y. Chen for subject recruitment, and Mr. J.-H. Lu and Ms. M.-C. Chung for technical assistance. This work was supported by the National Health Research Institutes of Taiwan (Grant EO-094-PP-05, EO-095-PP-07).
References
Barchowsky, A., Klei, L.R., Dudek, E.J., Swartz, H.M., James, P.E., 1999. Stimulation of reactive oxygen, but not reactive nitrogen species, in vascular endothelial cells exposed to low levels of arsenite. Free Radic. Biol. Med. 27, 1405–1412.
Benichou, J., 2001. A review of adjusted estimators of attributable risk. Stat. Methods Med. Res. 10, 195–216.
Bhattacharyya, T., Nicholls, S.J., Topol, E.J., Zhang, R., Yang, X., Schmitt, D., Fu, X., Shao, M., Brennan, D.M., Ellis, S.G., Brennan, M.L., Allayee, H., Lusis, A.J., Hazen, S.L., 2008.
Relationship of paraoxonase 1 (PON1) gene polymorphisms and functional activity with systemic oxidative stress and cardiovascular risk. JAMA 299, 1265–1276.
Brophy, V.H., Hastings, M.D., Clendenning, J.B., Richter, R.J., Jarvik, G.P., Furlong, C.E., 2001. Polymorphisms in the human paraoxonase (PON1) promoter. Pharmacoge- netics 11, 77–84.
Bruzzi, P., Green, S.B., Byar, D.P., Brinton, L.A., Schairer, C., 1985. Estimating the population attributable risk for multiple risk factors using case-control data. Am. J.
Epidemiol. 122, 904–914.
Chen, C.J., Chiou, H.Y., Chiang, M.H., Lin, L.J., Tai, T.Y., 1996. Dose–response relationship between ischemic heart disease mortality and long-term arsenic exposure.
Arterioscler. Thromb. Vasc. Biol. 16, 504–510.
Chen, C.J., Hsueh, Y.M., Lai, M.S., Shyu, M.P., Chen, S.Y., Wu, M.M., Kuo, T.L., Tai, T.Y., 1995.
Increased prevalence of hypertension and long-term arsenic exposure. Hyperten- sion 25, 53–60.
Chen, Q., Reis, S.E., Kammerer, C.M., McNamara, D.M., Holubkov, R., Sharaf, B.L., Sopko, G., Pauly, D.F., Merz, C.N., Kamboh, M.I., 2003. Association between the severity of angiographic coronary artery disease and paraoxonase gene polymorphisms in the National Heart, Lung, and Blood Institute-sponsored Women's Ischemia Syndrome Evaluation (WISE) study. Am. J. Hum. Genet. 72, 13–22.
Chen, Y.C., Lin-Shiau, S.Y., Lin, J.K., 1998. Involvement of reactive oxygen species and caspase 3 activation in arsenite-induced apoptosis. J. Cell Physiol. 177, 324–333.
Chiou, H.Y., Huang, W.I., Su, C.L., Chang, S.F., Hsu, Y.H., Chen, C.J., 1997. Dose–response relationship between prevalence of cerebrovascular disease and ingested inorganic arsenic. Stroke 28, 1717–1723.
Christiansen, L., Bathum, L., Frederiksen, H., Christensen, K., 2004. Paraoxonase 1 polymorphisms and survival. Eur. J. Hum. Genet. 12, 843–847.
Cole, T.B., Li, W.F., Richter, R.J., Furlong, C.E., Costa, L.G., 2002. Inhibition of paraoxonase (PON1) by heavy metals. Toxicol. Sci. 66, 312.
de Groot, E., Hovingh, G.K., Wiegman, A., Duriez, P., Smit, A.J., Fruchart, J.C., Kastelein, J.J., 2004. Measurement of arterial wall thickness as a surrogate marker for atherosclerosis. Circulation 109, III33–III38.
Hegele, R.A., Connelly, P.W., Scherer, S.W., Hanley, A.J., Harris, S.B., Tsui, L.C., Zinman, B., 1997. Paraoxonase-2 gene (PON2) G148 variant associated with elevated fasting plasma glucose in noninsulin-dependent diabetes mellitus. J. Clin. Endocrinol.
Metab. 82, 3373–3377.
Hegele, R.A., Harris, S.B., Connelly, P.W., Hanley, A.J., Tsui, L.C., Zinman, B., Scherer, S.W., 1998. Genetic variation in paraoxonase-2 is associated with variation in plasma lipoproteins in Canadian Oji-Cree. Clin. Genet. 54, 394–399.
Humbert, R., Adler, D.A., Disteche, C.M., Hassett, C., Omiecinski, C.J., Furlong, C.E., 1993.
The molecular basis of the human serum paraoxonase activity polymorphism. Nat.
Genet. 3, 73–76.
Jarvik, G.P., Rozek, L.S., Brophy, V.H., Hatsukami, T.S., Richter, R.J., Schellenberg, G.D., Furlong, C.E., 2000. Paraoxonase (PON1) phenotype is a better predictor of vascular disease than is PON1(192) or PON1(55) genotype. Arterioscler. Thromb. Vasc. Biol.
20, 2441–2447.
Kuo, T.L., 1964. Arsenic content of artesian well water in endemic area of chronic arsenic poisoning. Rep. Inst. Pathol. Coll. Med. Natl. Taiwan Univ. 20, 7–13.
Lee, P.C., Ho, I.C., Lee, T.C., 2005. Oxidative stress mediates sodium arsenite-induced expression of heme oxygenase-1, monocyte chemoattractant protein-1, and interleukin-6 in vascular smooth muscle cells. Toxicol. Sci. 85, 541–550.
Leus, F.R., Zwart, M., Kastelein, J.J., Voorbij, H.A., 2001. PON2 gene variants are associated with clinical manifestations of cardiovascular disease in familial hypercholester- olemia patients. Atherosclerosis 154, 641–649.
Li, W.F., Pan, M.H., Chung, M.C., Ho, C.K., Chuang, H.Y., 2006. Lead exposure is associated with decreased serum paraoxonase 1 (PON1) activity and genotypes. Environ.
Health Perspect. 114, 1233–1236.
Lo, M.C., Hsen, Y.C., Lin, B.K., 1977. Arsenic Content of Underground Water in Taiwan:
Second Report. Taiwan Provincial Institute of Environmental Sanitation, Taichung, Taiwan, pp. 1–17.
Lorenz, M.W., Markus, H.S., Bots, M.L., Rosvall, M., Sitzer, M., 2007. Prediction of clinical cardiovascular events with carotid intima-media thickness: a systematic review and meta-analysis. Circulation 115, 459–467.
Mackness, B., Davies, G.K., Turkie, W., Lee, E., Roberts, D.H., Hill, E., Roberts, C., Durrington, P.N., Mackness, M.I., 2001. Paraoxonase status in coronary heart disease: are activity and concentration more important than genotype? Arter- ioscler. Thromb. Vasc. Biol. 21, 1451–1457.
Mackness, B., Durrington, P., McElduff, P., Yarnell, J., Azam, N., Watt, M., Mackness, M., 2003. Low paraoxonase activity predicts coronary events in the Caerphilly Prospective Study. Circulation 107, 2775–2779.
Mochizuki, H., Scherer, S.W., Xi, T., Nickle, D.C., Majer, M., Huizenga, J.J., Tsui, L.C., Prochazka, M., 1998. Human PON2 gene at 7q21.3: cloning, multiple mRNA forms, and missense polymorphisms in the coding sequence. Gene 213, 149–157.
Navas-Acien, A., Sharrett, A.R., Silbergeld, E.K., Schwartz, B.S., Nachman, K.E., Burke, T.A., Guallar, E., 2005. Arsenic exposure and cardiovascular disease: a systematic review of the epidemiologic evidence. Am. J. Epidemiol. 162, 1037–1049.
Ng, C.J., Bourquard, N., Grijalva, V., Hama, S., Shih, D.M., Navab, M., Fogelman, A.M., Lusis, A.J., Young, S., Reddy, S.T., 2006. Paraoxonase-2 deficiency aggravates athero- sclerosis in mice despite lower apolipoprotein-B-containing lipoproteins: anti- atherogenic role for paraoxonase-2. J. Biol. Chem. 281, 29491–29500.
Pan, J.P., Lai, S.T., Chiang, S.C., Chou, S.C., Chiang, A.N., 2002. The risk of coronary artery disease in population of Taiwan is associated with Cys-Ser 311 polymorphism of human paraoxonase (PON)-2 gene. Zhonghua Yi Xue Za Zhi (Taipei) 65, 415–421.
Pi, J., Yamauchi, H., Kumagai, Y., Sun, G., Yoshida, T., Aikawa, H., Hopenhayn-Rich, C., Shimojo, N., 2002. Evidence for induction of oxidative stress caused by chronic exposure of Chinese residents to arsenic contained in drinking water. Environ.
Health Perspect. 110, 331–336.
Shih, D.M., Gu, L., Xia, Y.R., Navab, M., Li, W.F., Hama, S., Castellani, L.W., Furlong, C.E., Costa, L.G., Fogelman, A.M., Lusis, A.J., 1998. Mice lacking serum paraoxonase are susceptible to organophosphate toxicity and atherosclerosis. Nature 394, 284–287.
States, J.C., Srivastava, S., Chen, Y., Barchowsky, A., 2009. Arsenic and cardiovascular disease. Toxicol. Sci. 107, 312–323.
Su, S.Y., Chen, J.H., Huang, J.F., Wang, X.L., Zhao, J.G., Shen, Y., Qiang, B.Q., Gu, D.F., 2005.
Paraoxonase gene cluster variations associated with coronary heart disease in Chinese Han women. Chin. Med. J. 118, 1167–1174.
Tseng, C.H., Chong, C.K., Chen, C.J., Tai, T.Y., 1996. Dose–response relationship between peripheral vascular disease and ingested inorganic arsenic among residents in blackfoot disease endemic villages in Taiwan. Atherosclerosis 120, 125–133.
Tseng, C.H., Huang, Y.K., Huang, Y.L., Chung, C.J., Yang, M.H., Chen, C.J., Hsueh, Y.M., 2005. Arsenic exposure, urinary arsenic speciation, and peripheral vascular disease in blackfoot disease-hyperendemic villages in Taiwan. Toxicol. Appl.
Pharmacol. 206, 299–308.
Tward, A., Xia, Y.R., Wang, X.P., Shi, Y.S., Park, C., Castellani, L.W., Lusis, A.J., Shih, D.M., 2002. Decreased atherosclerotic lesion formation in human serum paraoxonase transgenic mice. Circulation 106, 484–490.
Wang, C.H., Jeng, J.S., Yip, P.K., Chen, C.L., Hsu, L.I., Hsueh, Y.M., Chiou, H.Y., Wu, M.M., Chen, C.J., 2002. Biological gradient between long-term arsenic exposure and carotid atherosclerosis. Circulation 105, 1804–1809.
Wang, T.S., Kuo, C.F., Jan, K.Y., Huang, H., 1996. Arsenite induces apoptosis in Chinese hamster ovary cells by generation of reactive oxygen species. J. Cell. Physiol. 169, 256–268.
Wang, X., Fan, Z., Huang, J., Su, S., Yu, Q., Zhao, J., Hui, R., Yao, Z., Shen, Y., Qiang, B., Gu, D., 2003. Extensive association analysis between polymorphisms of PON gene cluster with coronary heart disease in Chinese Han population. Arterioscler. Thromb. Vasc.
Biol. 23, 328–334.
Wang, Y.H., Wu, M.M., Hong, C.T., Lien, L.M., Hsieh, Y.C., Tseng, H.P., Chang, S.F., Su, C.L., Chiou, H.Y., Chen, C.J., 2007. Effects of arsenic exposure and genetic polymorphisms of p53, glutathione S-transferase M1, T1, and P1 on the risk of carotid atherosclerosis in Taiwan. Atherosclerosis 192, 305–312.
Wheeler, J.G., Keavney, B.D., Watkins, H., Collins, R., Danesh, J., 2004. Four paraoxonase gene polymorphisms in 11212 cases of coronary heart disease and 12786 controls:
meta-analysis of 43 studies. Lancet 363, 689–695.
Wu, M.M., Chiou, H.Y., Ho, I.C., Chen, C.J., Lee, T.C., 2003. Gene expression of inflammatory molecules in circulating lymphocytes from arsenic-exposed human subjects. Environ. Health Perspect. 111, 1429–1438.
Wu, M.M., Chiou, H.Y., Wang, T.W., Hsueh, Y.M., Wang, I.H., Chen, C.J., Lee, T.C., 2001.
Association of blood arsenic levels with increased reactive oxidants and decreased antioxidant capacity in a human population of northeastern Taiwan. Environ.
Health Perspect. 109, 1011–1017.