對多重利益相關者之意義提升是臨床醫療服務典範轉移的原因—以某區域教學醫院主動脈瘤支架手術迅速普及之經驗為例 - 政大學術集成
75
0
0
全文
(2) 治 Patients Dedicate政 to my 大. 立. ‧. ‧ 國. 學. n. er. io. sit. y. Nat. al. Ch. engchi. 2. i n U. v.
(3) Acknowledgement Having been a cardiac and vascular surgeon for 14 years, it‘s not easy for me to look at things without a surgeon‘s point of view. During the past couple of months, I tried hard to avoid my surgeon‘s prejudice and to look at things with different point of views in preparing the thesis. Professor Yuan‘s inspiring lectures on service science and innovation opened a door for me to the beauty of service science. Studies and preparation for the thesis offered me with the opportunity to regurgitate what I‘ve learnt in the class. Also, supports from my families, colleagues, and patients can never be overemphasized. Lastly, I offer my regards and blessings to all of those who supported me in any respect during the completion of the project.. 立. 政 治 大. ‧. ‧ 國. 學. n. er. io. sit. y. Nat. al. Ch. engchi. 3. i n U. v.
(4) 中文摘要 在現代外科實務中,我們今天認為是標準作業程序的手術,追溯到初期可能 是激進創新。多年來,外科技術雖然已經有頻繁的修改,但往往是漸進式地。心 臟和血管外科領域中的大多數創新並沒有導致日常實踐劇變。然而,在過去的幾 年中,在我服務的醫院和全世界,我看到了治療腹主動脈瘤 (AAA) 的典範轉移, 亦即主動脈腔內修復 (EVAR)。 相對於傳統開腹手術修復 (OSR),主動脈腔內修復較傳統開腹手術修復有 顯著較低的手術死亡率。不過,長遠來說,總死亡率或動脈瘤相關死亡率並無差 異;而主動脈腔內修復有較高的植入物相關併發症和必須再次手術的機率,且成 本更高。然而,主動脈腔內修復還是成為腹主動脈瘤治療的支柱。這是為什麼? 除了是激進的技術創新,主動脈腔內修復也是技術頓悟。傳統上,醫療服務 是典型的技術輔助服務情境,其中包含兩個單獨的、然而是密切相關的溝通系統:. 政 治 大. 一個是產業與醫師之間,另一個是醫師與病人之間。醫師居於樞紐地位,不僅確 保治療之執行,而且還要評估結果。由於現代資訊與通信技術的發達,病人可以 方便地搜尋輔助醫療文獻資訊、線上資訊和個人社會網絡的意見。這就像是詮釋 者的作用。這詮釋者的解釋對病人、外科醫生、和醫療產業界產生了實質上重大 的影響,反之亦然。以前在這服務體系中互相分離的部分現在可以緊密地互相配. 立. ‧ 國. 學. ‧. 合了,這與服務導向邏輯中價值共同創造的概念是不謀而合的。. sit. n. al. er. io. 相關者之意義提升。. y. Nat. 總之,對多重利益相關者之意義提升是臨床醫療服務典範轉移的原因。在醫 療行業中引入服務導向邏輯的概念的重要性,不論是在日常實務和創新策略上的 意義都是不容忽視的。醫療服務中,多重利益相關者比以前更涉及共同創造價值 的過程。未來的創新者除了專注在技術和科技上,更必須考慮該創新對多重利益. Ch. engchi. 4. i n U. v.
(5) Abstract In modern surgical practice, what we consider as standard procedures today may be radical innovations dated back to the early days. Over the years, there has been frequent modification of surgical techniques, often incremental though, and most innovations in the field of cardiac and vascular surgery didn‘t result in drastic changes in the daily practice. However, during the past several years, I have been witnessing a paradigm shift in the treatment of abdominal aortic aneurysm (AAA) in my hospital and worldwide towards endovascular aortic repair (EVAR). In comparison to the traditional open surgical repair (OSR), EVAR was associated with a significantly lower operative mortality than OSR. However, no differences were seen in total mortality or aneurysm-related mortality in the long term, and EVAR was associated with increased rates of graft-related complications and. 政 治 大. reinterventions and was more costly. Nevertheless, EVAR is becoming the mainstay of AAA treatment. Why is this? Except for being a radical technology innovation, EVAR is also a technology epiphany. Traditionally, medical service is a typical technology-assisted service encounter, consisting of two separate, however, closely inter-related communication. 立. ‧ 國. 學. ‧. systems: one between the industry and the physician, and the other one between the physician and the patient. The physician is of the pivot role that not only ensures the execution of treatment but also evaluates the results. With modern information and communication technologies, patients can easily search information from paramedical literatures, online information, and opinions from personal social network. This serves. er. io. sit. y. Nat. al. n. the emerging role of an interpretor. This interpretors‘ interpretation has substantial influence on patients, surgeons, industry, and payers and vice versa. Previously separated parts in the service system now can be closely inter-related. This is in concordance with the concept of co-creation of value in service-dominant logic. It is concluded that newly defined meanings to multiple stakeholders are the. Ch. engchi. i n U. v. reasons for paradigm shift in clinical medical service. The importance of introduction of the concept of service-dominant logic into the medical industry, both in daily practice and in innovation strategy can never be over-emphasized. Multiple stakeholders are being involved much more than before in the process of co-creation of value in medical service. Future innovators must concentrate on meanings to multiple stakeholders as well on techniques and technologies.. 5.
(6) Table of Contents Title page .............................................................................................................................. 1 Dedication ............................................................................................................................ 2 Acknowledgement................................................................................................................ 3 Abstract (Chinese) ................................................................................................................ 4 Abstract ................................................................................................................................ 5 List of tables ......................................................................................................................... 9 List of figures ...................................................................................................................... 10. 政 治 大. Chapter I Introduction ..................................................................................................... 11. 立. 1.1 Motivation of the Study ..................................................................................... 11. ‧ 國. 學. 1.2 Research Objectives and Questions .................................................................... 12 1.3 Research Flow and Chapter Description ............................................................. 12. ‧. 1.4 Research Scope and Limitation ........................................................................... 13. ............................................................................14. sit. y. Nat. Chapter II Review of Literature. io. al. n. 2.1.1 Introduction of Abdominal Aortic Aneurysm. Ch. engchi U. er. 2.1 Abdominal Aortic Aneurysm (AAA) .................................................................... 14 ........................................ 14. v ni. 2.1.2 Open Surgical Repair (OSR) ..................................................................... 17 2.1.3 Endovascular Aortic Repair (EVAR) .......................................................... 19 2.2 Evaluation of Different Treatment Modalities ...................................................... 21 2.2.1 Clinical Results of Different Treatment Modalities .................................. 21 2.2.2 Cost-effectiveness of Different Treatment Modalities .............................. 25 2.3 Factors Influencing Choice of Treatment ............................................................ 26 2.3.1 Shared Decision Making Model ............................................................... 26 2.3.2 Impact of Online Information on Decision Making .................................. 28 2.3.3 Service-dominant Logic and Co-creation of Value ................................... 30 2.4 Innovation— the EVAR Experience and Design-Driven Innovation....................... 33 2.4.1 History of Early Innovation and Development of EVAR ............................. 33 6.
(7) 2.4.2 Future Perspective of Technological Innovation in EVAR ........................ 34 2.4.3 Technology Epiphany: the Interplay between Technology Push and Design-Driven Innovation ........................................................................ 35 2.5 Dissemination of Medical Innovation ................................................................. 37 2.5.1 History of Development of EVAR .............................................................. 37 2.5.2 Adoption of EVAR .................................................................................... 39 2.6 Summary of Literature Review ........................................................................... 40 2.6.1 Abdominal aortic aneurysm is a serious disease. .................................... 40 2.6.2 Endovascular aortic repair is becoming the mainstream of AAA treatment. .................................................................................................................. 40. 政 治 大. 2.6.3 EVAR is not as cost-effective as we expect. ............................................. 41. 立. 2.6.4 Patient participation should be encouraged and facilitated to co-create. ‧ 國. ..................................................................................................... 41. 學. value.. 2.6.5 EVAR Is a Technology Epiphany? .............................................................. 43 ................................................................................. 45. ‧. Chapter III Research Methodology. 3.1 Research Methodology......................................................................................... 45. y. Nat. io. sit. 3.1.1 Research Design and Interview Guidelines .............................................. 45. n. al. er. 3.1.2 Information Collection .............................................................................. 46. Ch. i n U. v. Chapter IV Case Description and Analysis ......................................................................... 48. engchi. 4.1 Current Features of Medical Service in Taiwan 4.2 Current Status and Strategy of the Case Hospital. ................................................. 48 ............................................. 49. 4.3 Endovascular Aortic Repair (EVAR) in the Case Hospital ..................................... 52 4.3.1 Introduction of EVAR into the Department of Cardiovascular Surgery .... 52 4.3.2 Conduct of EVAR in Regional Hospitals (including the case hospital) in Taiwan ..................................................................................................... 53 4.4 Paradigm shift in surgical treatment of abdominal aortic aneurysm .................. 56 4.5 Analysis of In-depth Review ............................................................................... 58 4.6 Decision Making Process .................................................................................... 61 Chapter V Research findings ............................................................................................. 62 7.
(8) 5.1 Reasons for Paradigm Shift ................................................................................. 62 5.1.1 Newly Defined Meanings to Multiple Stakeholders Are the Reasons for Paradigm Shift in Clinical Medical Service — Patient Perspective. .......... 62. 5.1.2 Newly Defined Meanings to Multiple Stakeholders Are the Reasons for Paradigm Shift in Clinical Medical Service — Provider Perspective ......... 64 5.2 Innovation Model in the Transformation Process from Traditional Open Surgery to Modern Less Invasive Surgery ........................................................................ 66 Chapter VI Conclusions and Future Perspectives .............................................................. 69 References: ....................................................................................................................... 72. 立. 政 治 大. ‧. ‧ 國. 學. n. er. io. sit. y. Nat. al. Ch. engchi. 8. i n U. v.
(9) List of Tables. Table 2.1 Service-dominant logic foundational premise modifications and additions ........ 32 Table 3.1 Interviewees’ background and interview methods ............................................. 47 Table 4.1 Patient data......................................................................................................... 57. 立. 政 治 大. ‧. ‧ 國. 學. n. er. io. sit. y. Nat. al. Ch. engchi. 9. i n U. v.
(10) List of figures. Figure 2.1 Illustration of abdominal aortic aneurysm. ........................................................ 15 Figure 2.2 Operative techniques of trasnperitoneal abdominal aortic aneurysm repair with a straight or a bifurcated prosthetic graft. ......................................................... 18 Figure 2.3 Techniques of endovascular aortic repair. ......................................................... 21 Figure 2.4 Kaplan–Meier Estimates for Total Survival and Aneurysm-Related Survival during 8 Years of Follow-up. .............................................................................. 22. 治 政 大 Reintervention during 8 Years of Follow-up....................................................... 23 立 Figure 2.6 Innovation Strategies ......................................................................................... 36 Figure 2.5 Kaplan–Meier Estimates for the Time to the First Graft-Related Complication or. ‧ 國. 學. Figure 2.7 User-Centered Design and Design-Driven Innovation ........................................ 37. ‧. Figure 4.1 Abernathy and Clark (1985) Innovation types .................................................... 49 Figure 4.2 Business model of the traditional surgery melieu .............................................. 54. y. Nat. io. sit. Figure 4.3 Business model of the EVAR melieu ................................................................... 56. n. al. er. Figure 4.4 Numbers of EVAR and OSR ................................................................................ 57 Figure 5.1 A. Technology-assisted service encounter.. Ch. engchi. i n U. v. B. Technology-assisted service encounter with the presence of interpretor.... 64. Figure 5.2 Business model of the combined SDL and Design-driven innovation milieu. ...................................................................................................... 68. 10.
(11) Chapter I Introduction. 1.1 Motivation of the Study The author has been a cardiovascular surgeon for 14 years. I do a lot of surgeries in my daily practice, including coronary artery bypass surgery, heart valve surgery, peripheral vascular surgery, and aortic surgery. What we consider as standard procedures today may be radical innovations dated back to the early days. Take. 政 治 大. cardiopulmonary bypass which is a routine and essential part of modern open heart. 立. surgery as an example. Between March 26, 1954 and July 19, 1955, C. Walton. ‧ 國. 學. Lillehei and colleagues operated upon 45 infants and children with previously uncorrectable cardiac anomalies using cross-circulation with a human donor. The. ‧. concept of cross-circulation represented "the dawn of open-heart surgery" (Moller,. y. Nat. n. al. er. io. machine (cardiopulmonary bypass) that soon followed.. sit. Shumway, & Gott 2009). This concept contributed to the invention of heart-lung. i n U. v. Over the years, there has been frequent modification of surgical techniques, often. Ch. engchi. incremental though. Of course, there were major radical innovations, like off-pump coronary artery bypass surgery, robotic mitral valve repair, and etc. Not any one of them has gained wide acceptance. For example, since its advent some 20 years ago, only 20% of patients were operated on with off-pump technique, while the remaining 80% of patients accepted traditional surgery. Most innovations in the field of cardiac and vascular surgery didn‘t result in drastic changes in the daily practice. During the past two years, I have been witnessing a paradigm shift in the treatment of abdominal aortic aneurysm in my hospital. Endovascular aortic repair (EVAR) is a new and less invasive surgery in comparison to open surgical repair 11.
(12) (OSR) as a treatment modality to abdominal aortic aneurysm. In my hospital, we started EVAR program in 2009, and amazingly it soon became the mainstay of treatment within 1 year. This rapid acceptance and dissemination of EVAR not only has been observed in my hospital, but also it has been a worldwide trend. What are the underlying reasons for this phenomenon of radical innovation? It‘s the aim of this study to figure them out.. 1.2 Research Objectives and Questions. 政 治 大 endovascular aortic repair (EVAR) technique to treat abdominal aortic aneurysm 立 This study is focused on the process of rapid adoption of an innovatively new. within one year in a 750-bedded regional hospital in New Taipei City. At the same. ‧ 國. 學. time span, the numbers of traditional open aortic repair procedures decreased. ‧. dramatically. Since most innovations in surgical techniques are incremental, this. sit. y. Nat. observed phenomenon is quite unique and exceptional. The research objectives are. io. The author tried to answer the following questions:. al. v i n What is the reason for theCparadigm shift in theUtreatment of abdominal aortic hengchi n. 1.. er. therefore to explore the underlying contributing reasons for this phenomenon.. aneurysm in this certain period of time? 2.. Is there a specific innovation model in the transformation process from. traditional open surgery to modern less invasive surgery?. 1.3 Research Flow and Chapter Description This study flow started with the research motivation and objectives, followed by literature review. Related research works and literatures from both the medicine and the business study field were reviewed to formulate the theoretical bases of this service and innovation study. There were two parts of the following case study. First 12.
(13) part of the case study consisted of an analysis of medical records of all patients with abdominal aortic aneurysm treated either with traditional open surgery or with EVAR in the case hospital in the study period. The results concerning the medical and the financial aspects were analyzed. The second part of the case study consisted of an in-depth interview of two surgeons and seven industry persons. The interview results were analyzed for meanings. Compiling the results from the literatures reviewed and conjectures deduced from those observed facts in the case study, an explanatory conclusion was achieved.. 政 治 大 research methodology, case description and analysis, and conclusions and future 立 This thesis is divided into five chapters: the introduction, review of literatures,. perspectives.. ‧ 國. 學 ‧. 1.4 Research Scope and Limitation. sit. y. Nat. The author intends to figure out the reasons underlying the process of a certain. io. er. radical innovation in the case hospital through case study and in-depth interview. The conclusions are theoretically valid only concerning the case hospital in this limited. al. n. v i n C h and innovation U period of time. However, as a service study, I hope there is a category engchi effect — the conclusions could be extrapolated to similar categories of medical service and innovations. Of course, there must be imperfections in the analysis and conclusions. Future studies are needed to answer those remaining questions.. 13.
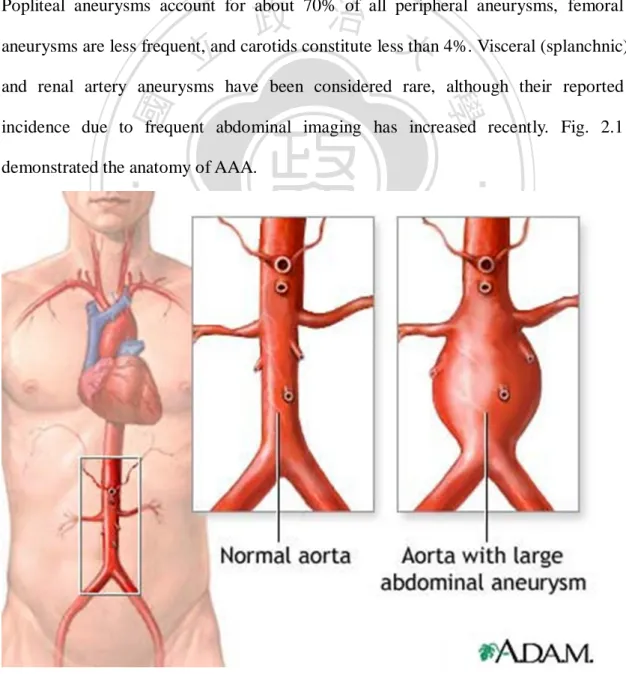
(14) Chapter II Review of Literature. This is a service and innovation study in which conclusions are deduced from facts directly observed in daily medical practice or from comprehensive review of literatures. Related research works and literatures from both the medicine and the business study field were reviewed to formulate the theoretical bases of this service. 政 治 大 We first briefly introduced the pathophysiology of abdominal aortic aneurysm 立. and innovation study.. and choices of treatment, focusing on the traditional open surgical repair and the. ‧ 國. 學. innovative endovascular repair (2.1), followed by comparison of the two different. ‧. treatment modalities concerning clinical results and cost-effectiveness (2.2). How. sit. y. Nat. patients make decision on treatment modality can be found from review of literatures. io. er. on patients‘ decision-making process (2.3). In section 2.4 and 2.5, the innovation and dissemination process of endovascular repair are thoroughly discussed about.. n. al. Ch. engchi. i n U. v. 2.1 Abdominal Aortic Aneurysm (AAA) 2.1.1 Introduction of Abdominal Aortic Aneurysm Gloviczki, and Ricotta, (2011) wrote in Textbook of Vascular Surgery that the term aneurysm is derived from the Greek word aneurysma which means ―widening‖ and can be defined as a permanent and irreversible localized dilation of a blood vessel, having at least a 50% increase in diameter compared with the expected normal diameter. Ectasia is defined as a dilation less than 50% of the normal diameter. Normal diameter of the aorta and the arteries depends on age, gender, body size, and 14.
(15) other factors. In men, the infrarenal aorta is normally between 14 and 24 mm, and in women, it is between 12 and 21 mm. Therefore, an abdominal aortic aneurysm (AAA) is diagnosed if the diameter is 3 cm or larger in a man or 2.6 cm or larger in a woman. The most frequent site of extracranial arterial aneurysms is the infrarenal aorta. In one large autopsy series of patients with aortoiliac aneurysms, the most frequent location was the abdominal aorta alone (65%), followed by the thoracic aorta alone (19%), the abdominal aorta and iliac arteries (13%), the thoracoabdominal aorta (2%) and iliac arteries alone (1%). Peripheral arterial aneurysms are much less common.. 政 治 大 aneurysms are less frequent, and carotids constitute less than 4%. Visceral (splanchnic) 立 Popliteal aneurysms account for about 70% of all peripheral aneurysms, femoral. and renal artery aneurysms have been considered rare, although their reported. ‧ 國. 學. incidence due to frequent abdominal imaging has increased recently. Fig. 2.1. ‧. demonstrated the anatomy of AAA.. n. er. io. sit. y. Nat. al. Ch. engchi. i n U. v. Figure 2.1 Illustration of abdominal aortic aneurysm. (source: “MedlinePlus‖) 15.
(16) The natural history of AAAs is continuous expansion. Rupture is the most frequent and lethal complication of AAAs. In the United States, aneurysm rupture is the cause of death in 1.2% of men and 0.6% of women. About 15,000 deaths each year are caused by ruptured AAAs, making AAA the 13th leading cause of death in the United States. It is the 10th leading cause of death in men. In a study of 231 ruptured aneurysms, 71% of patients did not know before rupture that they had an aneurysm. Most ruptures occur into the retroperitoneal space, but free rupture of the anterior wall can result in herald bleeding into the abdominal cavity; rupture into. 政 治 大 stula, whereas rupture into the duodenum results in massive gastrointestinal bleeding 立. the inferior vena cava or iliac vein causes aortocaval or aortoiliac arteriovenous fi. due to a primary aortoduodenal fistula.. ‧ 國. 學. After rupture of an AAA, only half of patients arrive at the hospital alive. In one. ‧. study, 50% reached the hospital alive, 7% died before surgery, 17% died during the. sit. y. Nat. operation, and 37% died within 30 days of surgery for an overall mortality rate for. io. er. open surgical repair of 45%. Although initial results of EVAR for ruptured AAA have been encouraging, about 25% to 30% of patients with a ruptured AAA will eventually. al. n. v i n Clead survive. Occasionally, AAAs can and limb-threatening conditions because U h etonlifei h gc. of acute thromboembolism.. The larger the aneurysm diameter is, the greater the risk for rupture is. The annual risk for rupture of an AAA between 4 and 5.4 cm in size is about 0.5% to 1%. For AAAs between 5.5 and 6 cm, the annual rupture risk is estimated between 5% and 10%. AAAs between 6 and 7 cm have an estimated yearly rate of rupture of 10% to 20%. In 2003, a consensus statement was issued by the Society for Vascular Surgery regarding screening for AAAs. It recommended baseline ultrasound screening for AAA in men aged 60 to 85 years, women 60 to 85 years with cardiovascular risk 16.
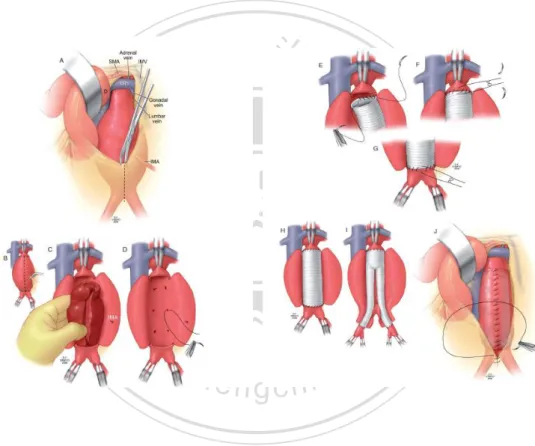
(17) factors, and men and women older than 50 years with a family history of AAA. Subsequent ultrasound is recommended annually for AAAs 4.0 to 4.5 cm and every 6 months for AAAs larger than 4.5 cm. The United States approved the Screening Abdominal Aortic Aneurysms Very Efficiently (SAAAVE) Act to provide AAA screening at age 65, for male ever-smokers and men and women with a family history of AAA, as recommended by the U.S. Preventive Services Task Force. For patients with low-risk AAAs (small diameter without other risk factors for rupture) being followed with serial size measurements, attempts are made to reduce. 政 治 大 modifications, including smoking cessation, blood pressure control, and reduction of 立. expansion rate and rupture risk. This can be accomplished with risk factor. cholesterol, triglycerides, and lipoproteins.. ‧ 國. 學. The goal of elective AAA repair is to prevent rupture and prolong life. Careful. ‧. assessment of factors that influence rupture risk, operative mortality, and life. er. io. sit. y. Nat. expectancy is essential, and patient preference receives increasing importance.. 2.1.2 Open Surgical Repair (OSR). al. n. v i n C h can be used,Ueach with its own merits and For open repair, several exposures engchi. disadvantages. Options include a transperitoneal approach, through a long midline incision or through a mini-laparotomy, or the retroperitoneal approach through a left. flank incision. Though the incisions and exposures may vary, the aim of the operation is to exclude or resect the aneurysmally dilated abdominal aorta and to replace it with a straight or a bifurcated graft. If the iliac arteries are not aneurysmal, a straight collagen or gelatin-coated zero porosity polyester (Dacron) graft is used for repair, usually 16 or 18 mm in diameter. Both proximal and distal anastomoses are performed with 3-0 polypropylene running sutures. When the common iliac arteries are involved, a 16- or 18-mm bifurcated graft 17.
(18) is used and sutured to the distal common iliac arteries in an end-to-end fashion, using 4-0 polypropylene running sutures (Fig. 2.2). Early mortality for open elective AAA repair has greatly improved during the past 2 decades because of improvements in preoperative evaluation, intraoperative techniques, and perioperative care. Mortality rates of elective open infrarenal AAA repair in good-risk patients can be expected to be less than 5%; in high-volume centers, the mortality rate is between 1% and 3%. (Rutherford 2004). 立. 政 治 大. ‧. ‧ 國. 學. n. er. io. sit. y. Nat. al. Ch. engchi. i n U. v. Figure 2.2 Operative techniques of trasnperitoneal abdominal aortic aneurysm repair with a straight or a bifurcated prosthetic graft. (source: Sabiston Textbook of Surgery, 18th Edition). 18.
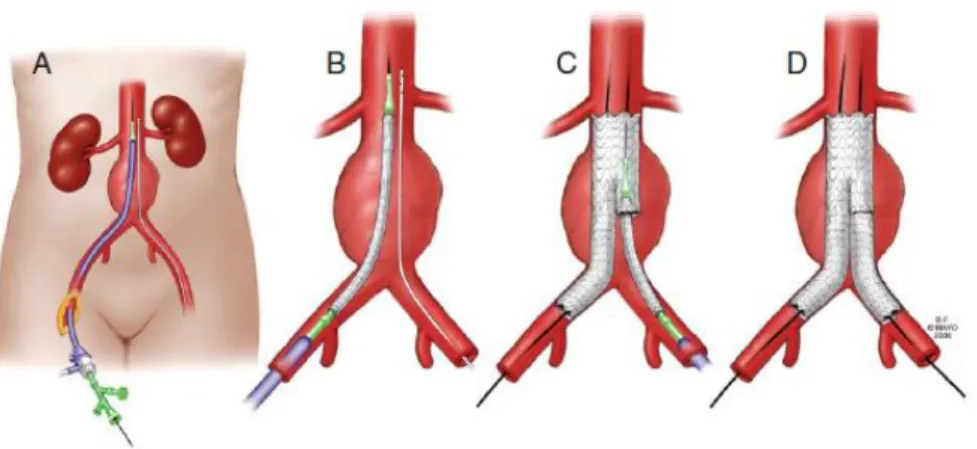
(19) The 2003 Guidelines for the treatment of abdominal aortic aneurysms published by the Joint Council of the Vascular Societies noted that treatment of AAAs is individualized and recommended operative repair for AAAs with a diameter of 5.5 cm or greater in men. Those aneurysms that expand at a rate of more than 1 cm/year or that are symptomatic must be repaired. However, subsets of younger, low-risk patients, with long projected life expectancy, may prefer earlier repair. If the surgeon‘s operative mortality rate is low, repair may be indicated at smaller sizes (4.5-5.4 cm) if that is the patient‘s preference. For women and patients with a greater than average. 政 治 大 repair. Atypical aneurysms (dissecting, pseudoaneurysms, mycotic, saccular, and 立. rupture risk, an AAA diameter of 4.5 to 5.0 cm is an appropriate threshold for elective. penetrating ulcers) may be an indication for surgical treatment regardless of size. For. ‧ 國. 學. high-risk patients, delay in repair until larger diameter is warranted, especially if. ‧. EVAR is not possible. The guidelines recommended EVAR as the most appropriate. y. Nat. option for patients at increased risk with conventional open repair. EVAR is preferred. er. io. sit. for older, high-risk patients; those with ―hostile‖ abdomens; and patients with other clinical circumstance likely to increase the risk of open repair, if their anatomy is. al. n. v i n appropriate. It was emphasized C that patient preferenceU h e n g c h i is of great importance.. It is essential that the patients be well informed to make such choices.. 2.1.3 Endovascular Aortic Repair (EVAR) In contrary to open surgical repair, in which the aneurysm is resected and the aorta was replaced with a prosthesis graft through a generous laparotomy or a flank incision, during EVAR, the stent-graft of which the mechanism of treatment is to exclude the blood from flowing into the aneurysm sac is introduced into the aneurysm through the femoral arteries and fixed in place to the nonaneurysmal aortic neck and iliac arteries with self-expanding or balloon-expandable stents. Some of the 19.
(20) stent-grafts have barbs, pins, or hooks to secure the stent, whereas some others have suprarenal fixation with self-expanding stents. A major abdominal incision is thus avoided, and procedure-related morbidity is reduced. An endovascular stent-graft excludes the aneurysm from blood flow and extends from the infrarenal aorta to both common iliac arteries, preserving flow to the internal iliac arteries. This procedure can be performed in a surgery-capable catheterization laboratory or a surgical suite equipped with a fixed or mobile angiography C-arm. This can be performed under general, regional, spinal, or local anesthesia. Both common femoral. 政 治 大 cutdowns. Vascular sheaths are placed over guidewires under fluoroscopic guidance 立. arteries are cannulated either percutaneously or more commonly with femoral artery. into both external iliac arteries. The patient is systemically heparinized, and a. ‧ 國. 學. diagnostic aortogram is performed through a marker pigtail catheter placed just above. ‧. the renal arteries. Appropriate measurements are taken. Super-stiff guidewires are. sit. y. Nat. then inserted into the thoracic aorta through both femoral sheaths. The endograft. io. er. device is advanced into the aorta, usually through its own deployment sheath. A multi-sidehole catheter is advanced from the contralateral side to mark the level of the. al. n. v i n Cdevice renal arteries, and the main body deployed just below the lowest renal artery. U h e nis g i h c. Distally, it is deployed to just above the iliac bifurcation, taking care not to cover the hypogastric artery unless preoperatively planned. The contralateral limb gate is then cannulated, and an appropriately chosen contralateral iliac limb endograft device is deployed from within the main device to just above the iliac bifurcation. Balloon dilation is performed of all attachment sites, and completion angiogram is done with attention paid to position and sealing of the graft attachment sites.. 20.
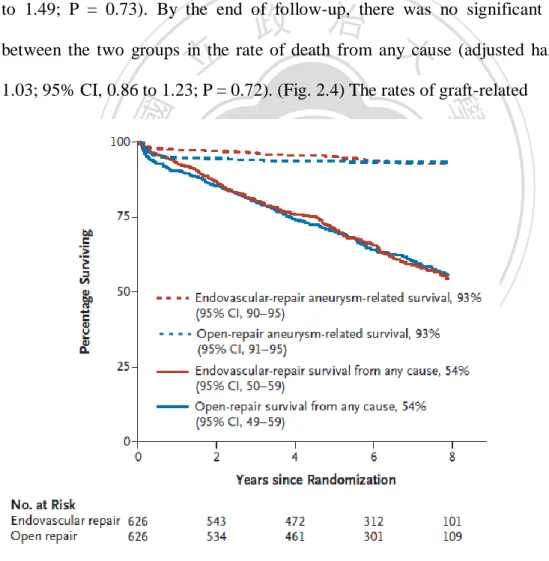
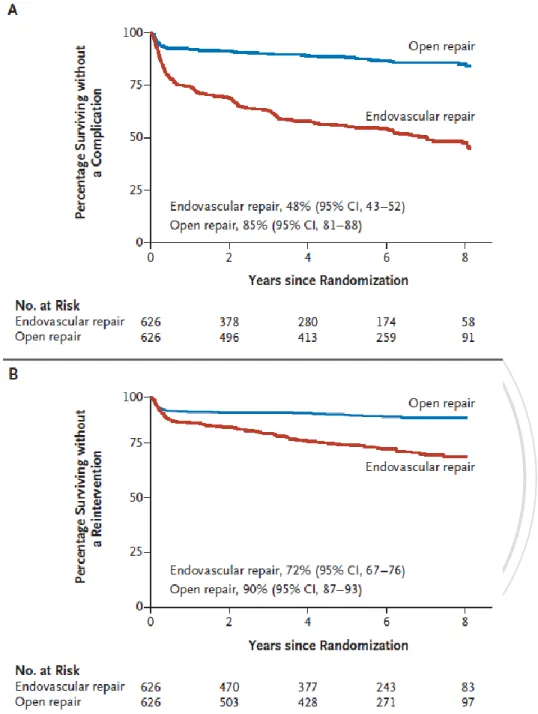
(21) Figure 2.3 Techniques of endovascular aortic repair. (source: Sabiston Textbook of Surgery, 18th Edition). 立. 政 治 大. 2.2.1 Clinical Results of Different Treatment Modalities. 學. ‧ 國. 2.2 Evaluation of Different Treatment Modalities. Since the advent of endovascular aortic repair techniques for surgical treatment. ‧. of abdominal aortic aneurysm in the early 1990‘s, many meticulous amendments of. y. Nat. io. sit. the implantation techniques and a lot of technological improvement of endovascular. n. al. er. stentgrafts have been observed. There are many clinical studies focusing on the. i n U. v. short-term and long-term results of EVAR in comparison to OSR.. Ch. engchi. Within 10 years, Seelig (1999) reported in Mayo Clinic Procedings that in light of the potential to reduce morbidity and mortality associated with open surgical repair, endoluminal grafting offers therapeutic options to patients who are not surgical candidates because of comorbidities. The United Kingdom EVAR Trial Investigators published the trial result in New England Journal of Medicine in 2010. From 1999 through 2004 at 37 hospitals in the United Kingdom, they randomly assigned 1252 patients with large abdominal aortic aneurysms (≥5.5 cm in diameter) to undergo either endovascular or open repair; 626 patients were assigned to each group. Patients were followed for rates of death, 21.
(22) graft-related complications, reinterventions, and resource use until the end of 2009. Logistic regression and Cox regression were used to compare outcomes in the two groups. The 30-day operative mortality was 1.8% in the endovascular-repair group and 4.3% in the open-repair group (adjusted odds ratio for endovascular repair as compared with open repair, 0.39; 95% confidence interval [CI], 0.18 to 0.87; P = 0.02). The endovascular repair group had an early benefit with respect to aneurysm-related mortality, but the benefit was lost by the end of the study, at least partially because of fatal endograft ruptures (adjusted hazard ratio, 0.92; 95% CI, 0.57. 政 治 大 between the two groups in the rate of death from any cause (adjusted hazard ratio, 立. to 1.49; P = 0.73). By the end of follow-up, there was no significant difference. 1.03; 95% CI, 0.86 to 1.23; P = 0.72). (Fig. 2.4) The rates of graft-related. ‧. ‧ 國. 學. n. er. io. sit. y. Nat. al. Ch. engchi. i n U. v. Figure 2.4 Kaplan–Meier Estimates for Total Survival and Aneurysm-Related Survival during 8 Years of Follow-up. (source: United Kingdom EVAR Trial Investigators 2010.) 22.
(23) 立. 政 治 大. ‧. ‧ 國. 學. n. er. io. sit. y. Nat. al. Ch. engchi. i n U. v. Figure 2.5 Kaplan–Meier Estimates for the Time to the First Graft-Related Complication or Reintervention during 8 Years of Follow-up. (source: United Kingdom EVAR Trial Investigators 2010.). complications and reinterventions were higher with endovascular repair, and new complications occurred up to 8 years after randomization, contributing to higher overall costs. (Fig. 2.5) They concluded in this large, randomized trial, that 23.
(24) endovascular repair of abdominal aortic aneurysm was associated with a significantly lower operative mortality than open surgical repair. However, no differences were seen in total mortality or aneurysm-related mortality in the long term. Endovascular repair was associated with increased rates of graft-related complications and reinterventions and was more costly. The United Kingdom EVAR Trial Investigators also published in New England Journal of Medicine in 2010 data on the question of whether endovascular repair reduces the rate of death among patients who were considered to be physically. 政 治 大 United Kingdom, they randomly assigned 404 patients with large abdominal aortic 立. ineligible for open surgical repair. From 1999 through 2004 at 33 hospitals in the. aneurysms (≥5.5 cm in diameter) who were considered to be physically ineligible for. ‧ 國. 學. open repair to undergo either endovascular repair or no repair; 197 patients were. ‧. assigned to undergo endovascular repair, and 207 were assigned to have no. sit. y. Nat. intervention. Patients were followed for rates of death, graft-related complications and. io. er. reinterventions, and costs until the end of 2009. Cox regression was used to compare outcomes in the two groups. The 30-day operative mortality was 7.3% in the. al. n. v i n endovascular-repair group. The C overall rate of aneurysm h e n g c h i U rupture in the no-intervention group was 12.4 (95% confidence interval [CI], 9.6 to 16.2) per 100 person-years.. Aneurysm-related mortality was lower in the endovascular-repair group (adjusted hazard ratio, 0.53; 95% CI, 0.32 to 0.89; P = 0.02). This advantage did not result in any benefit in terms of total mortality (adjusted hazard ratio, 0.99; 95% CI, 0.78 to 1.27; P = 0.97). A total of 48% of patients who survived endovascular repair had graft-related complications, and 27% required reintervention within the first 6 years. During 8 years of follow-up, endovascular repair was considerably more expensive than no repair (cost difference, £9,826 [U.S. $14,867]; 95% CI, 7,638 to 12,013 [11,556 to 18,176]). The concluded that patients who were physically ineligible for 24.
(25) open repair, endovascular repair of abdominal aortic aneurysm was associated with a significantly lower rate of aneurysm-related mortality than no repair. However, endovascular repair was not associated with a reduction in the rate of death from any cause. The rates of graft-related complications and reinterventions were higher with endovascular repair, and it was more costly.. 2.2.2 Cost-effectiveness of Different Treatment Modalities We know from the previous section on clinical result that endovascular aortic. 政 治 大 cost-effectiveness and quality of life issue. 立. repair is more costly that open surgical repair. Yet, we still don‘t know the. Young (2010) reported in the Journal of Vascular surgery an evaluation of the. ‧ 國. 學. cost-effectiveness of endovascular repair (EVAR) for small abdominal aortic. ‧. aneurysms (AAA). Outcomes were reported as quality-adjusted life-years (QALYs).. sit. y. Nat. The model demonstrated that early EVAR for 4.0 cm-5.4 cm AAAs led to fewer. io. er. QALYs at greater costs when compared with observational management with elective repair at 5.5 cm. With a >70% probability, observational management until AAA. al. n. v i n Ch diameter is 5.5 cm will be the cost-effective option. However, EVAR for small AAAs engchi U may become cost-effective when differences in quality of life and mortality are considered.. When EVAR was compared with OSR, Blackhouse‘s group reported in 2008 and 2009 that based on commonly quoted willingness-to-pay thresholds, EVAR was not found to be cost-effective compared to OSR. EVAR may be a cost-effective strategy compared with OSR for high-risk patients. Longer-term data are needed to decrease the uncertainty associated with the results. In Chambers‘ review paper (2009), they concluded that open repair is more likely to be cost-effective than EVAR on average in patients considered fit for open 25.
(26) surgery. EVAR is likely to be more cost-effective than open repair for a subgroup of patients at higher risk of operative mortality. These results are based on extrapolation of mid-term results of clinical trials. Evidence does not currently support EVAR for the treatment of ruptured aneurysms. Further follow-up of the existing UK trials should be undertaken and the relative costs of procedures and devices should be investigated further.. 2.3 Factors Influencing Choice of Treatment. 政 治 大 the first priority. Can this aim be always achieved? This has been and still will be true 立. Every clinician has been taught and trained to consider a patient‘s best benefit as. for a certain percentage of clinical scenarios: one ill, one pill, and one bill. A patient. ‧ 國. 學. was prescribed with a pill to treat a disease by a physician who was compensated for. ‧. the treatment. However, as medical knowledge and technology are progressing. sit. y. Nat. explosively, not only patients but also clinicians are more frequently encountering. io. er. puzzling clinical situations that can oftentimes be managed with more than one treatment modalities, of which each treatment modality carries its specific anticipated. al. n. v i n C side-effects results, at the tradeoff of potential of course. h e n g candh complications, i U. Is there always a straight forward best solution? If there is, who‘s going to make. the decision out of the complex clinical situation? Is it easy for a patient to choose the best treatment modality for him/herself? Is it EVAR, OSR, or watchful waiting?. 2.3.1 Shared Decision Making Model Shared decision making is an approach where clinicians and patients communicate together using the best available evidence when faced with the task of making decisions, where patients are supported to deliberate about the possible attributes and consequences of options, to arrive at informed preferences in making a 26.
(27) determination about the best action and which respects patient autonomy, where this is desired, ethical and legal. One of the first instances where the term ‗shared decision making‘ was used was in a report entitled the ‗President's Commission for The Study of Ethical Problems in Medicine and Biomedical Research. (President's Advisory Commission on Consumer Protection and Quality in the Health Care Industry, 1998). This work built on the increasing interest in patient-centredness and an increasing emphasis on recognising patient autonomy in health care interactions since the 1970s.. 政 治 大 decision-making in the medical encounter. The particular decision-making context 立 Shared decision-making is increasingly advocated as an ideal model of treatment. that we focus on is potentially life threatening illnesses, where there are important. ‧ 國. 學. decisions to be made at key points in the disease process, and several treatment. ‧. options exist with different possible outcomes and substantial uncertainty. Charles et. sit. y. Nat. al. (1997) suggested as key characteristics of shared decision-making (1) that at least. io. er. two participants—physician and patient be involved; (2) that both parties share information; (3) that both parties take steps to build a consensus about the preferred. al. n. v i n C his reached on theUtreatment to implement. treatment; and (4) that an agreement engchi. In December 2010 a Salzburg Global Seminar focused on "The Greatest. Untapped Resource in Healthcare? Informing and Involving Patients in Decisions about Their Medical Care." Powerful conclusions emerged among the 58 participants from 18 countries: not only is it ethically right that patients should be involved more closely in decisions about their own medical care and the risks involved, it is practical – through careful presentation of information and the use of decision aids/pathways – and it brings down costs. Unwarranted practice variations - where one area may have many more interventions than another, but with no better outcomes – are reduced, sometimes dramatically. 27.
(28) Do patients really want to participate in decision making? Levinson et al. (2004) reported in their population-base study that people vary substantially in their preferences for participation in decision making. Physicians and health care organizations should not assume that patients wish to participate in clinical decision making, but must assess individual patient preferences and tailor care accordingly. Patients may wish to participate in a variety of ways including seeking and exchanging information, discussing options in care, and making the final decisions about treatment. Patients who are active participants in the process of their care may. 政 治 大 organizations alike encourage patients to engage in making decisions in collaboration 立. have improved medical outcomes. To this end, consumer groups and medical. with their physicians.. ‧ 國. 學. Yet, not all patients want to participate to the same degree. Some may wish to. ‧. be active in discussing treatment options but may ultimately want to rely entirely on. sit. y. Nat. their physicians to make decisions on their behalf. Nearly all respondents (96%). io. er. preferred to be offered choices and to be asked their opinions. In contrast, half of the respondents (52%) preferred to leave final decisions to their physicians and 44%. n. al. preferred to rely on. i n C hfor medical knowledge physicians engchi U. v. rather than seeking out. information themselves. Women, more educated, and healthier people were more likely to prefer an active role in decision making. African-American and Hispanic respondents were more likely to prefer that physicians make the decisions. Preferences for an active role increased with age up to 45 years, but then declined.. 2.3.2 Impact of Online Information on Decision Making When diagnosed with an abdominal aortic aneurysm (AAA), patients are confronted with a complex decision: whether or not to undergo invasive treatment for an asymptomatic but potentially fatal condition. Effective communication of this 28.
(29) information during the informed consent process can be challenging because of the volume and complexity of the information involved as well as the emotional impact of the potentially life-changing alternatives being considered. Many patients neither appreciated the scope of their options before AAA repair nor felt adequately informed prior to making a decision. The internet has the potential to provide patients with information and support as an adjunct to direct communication with the surgeon. Nevertheless, Goldberg, Berman, and Gusberg, (2010) suggested that websites frequently accessed by patients. 政 治 大 was mortality, which was reported by less than one-third of sites as a risk for open 立. lack important information regarding surgical risk. The most common risk reported. repair and less than 10% of sites as a risk for EVAR. Within the discussion of risks,. ‧ 國. 學. few sites quantified the probability that a complication would occur. When EVAR was. ‧. presented as an alternative to open surgery, they found that websites tended to present. sit. y. Nat. more information about the benefits and less information about the risks of EVAR.. io. er. Less than 20% reported a risk of reintervention after EVAR. Although 40% of sites alluded to the concept of increased follow-up after EVAR, only 18.5% specified the. al. n. v i n C h of surgical risk was need for annual CT scans. Reporting even lower among industryengchi U sponsored websites.. The lack of information available to patients has important implications for the physician-patient encounter. Even proactive patients who are seemingly wellinformed may lack important information about health risk. Patients who form treatment preferences based on information obtained online are likely to have based these preferences on incomplete and possibly misleading information about the treatment options and their risks, potentially leaving them with unrealistic expectations of outcomes. Assessing the degree to which patients are making informed choices requires an understanding of the adequacy of information obtained from the internet 29.
(30) and patients‘ ability to interpret this information. Surgeons and other physicians who regularly discuss AAA management options with their patients should be aware of the potential for patients to arrive with preconceived notions based on what they have read online and be prepared to provide more complete information on risk and outcomes.. 2.3.3 Service-dominant Logic and Co-creation of Value Can the medical society borrow any idea from the business world?. 政 治 大 its dominant logic away from the exchange of tangible goods (manufactured things) 立. Vargo and Lusch (2004) suggested ―increasingly, marketing has shifted much of. and toward the exchange of intangibles, specialized skills and knowledge, and. ‧ 國. 學. processes (doing things for and with), which we believe pints marketing toward a. ‧. more comprehensive and inclusive dominant logic, one that integrates goods with. y. sit. io. er. and practice.‖. Nat. services and provides a richer foundation for the development of marketing thought. The service-centered view of marketing implies that marketing is a continuous. al. n. v i n C h that is largelyU focused on operant resources series of social and economic processed engchi. with which the firm is constantly striving to make better value propositions than its competitors. In a free enterprise system, the firm primarily knows whether it is making better value propositions from the feedback it receives from the marketplace in terms of firm financial performance. Because firms can always do better at serving customers and improving financial performance, the service-centered vie of marketing perceives marketing as a continuous learning process (directed at improving operant resources). The service-centered viewed can be stated as follows: 1. Identify or develop core competences, the fundamental knowledge and skills 30.
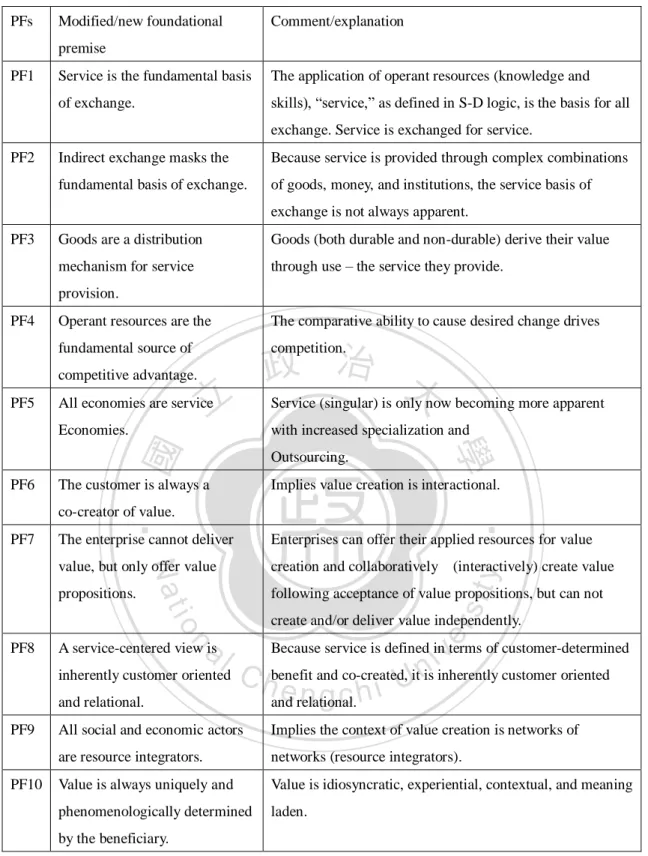
(31) of an economic entity that represent potential competitive advantage. 2. Identify other entities (potential customers) that could benefit from these competences. 3. Cultivate relationships that involve the customers in developing customized, competitively compelling valve propositions to meet specific needs. 4. Gauge marketplace feedback by analyzing financial performance from exchange to learn how to improve the firm‘s offering to customers and improve firm performance.. 政 治 大 original foundational premises (PFs‘). 立. Later on in their 2008 work, Vargo and Lusch (2008) made some modifications and additions to their. (Table 2.1) They. addressed that service is the fundamental basis of exchange, operant resources are the. ‧ 國. 學. fundamental source of competitive advantage, and all economies are service. ‧. economies. The customer is always a co-creator of value, and the enterprise cannot. sit. y. Nat. deliver valve, but only offer value propositions. A service-centered view is. io. er. inherently customer-oriented and relational. All social and economic actors are resource integrators and value is always uniquely and phenomenologically determined. n. al. by the beneficiary.. Ch. engchi. i n U. v. The last two PFs‘ add some NPO (non-profit organization) flavor to the service-dominant logic. And in addition, we are surprised to find out the similarity of value propositions between the shared decision making model from the medical society and the service dominant logic from the business world.. 31.
(32) PFs. Modified/new foundational. Comment/explanation. premise PF1. Service is the fundamental basis. The application of operant resources (knowledge and. of exchange.. skills), ―service,‖ as defined in S-D logic, is the basis for all exchange. Service is exchanged for service.. PF2. Indirect exchange masks the. Because service is provided through complex combinations. fundamental basis of exchange.. of goods, money, and institutions, the service basis of exchange is not always apparent.. PF3. Goods are a distribution. Goods (both durable and non-durable) derive their value. mechanism for service. through use – the service they provide.. provision. PF4. Operant resources are the fundamental source of. 立. All economies are service. with increased specialization and Outsourcing.. The customer is always a. 學. PF6. ‧ 國. Economies.. 政 治 大 Service (singular) is only now becoming more apparent competition.. competitive advantage. PF5. The comparative ability to cause desired change drives. Implies value creation is interactional.. The enterprise cannot deliver. Enterprises can offer their applied resources for value. Nat. creation and collaboratively (interactively) create value. propositions.. following acceptance of value propositions, but can not. io. sit. y. value, but only offer value. create and/or deliver value independently.. al. er. PF7. ‧. co-creator of value.. n. v i n inherently customer oriented C benefit and co-created, it is inherently customer oriented hengchi U and relational. and relational.. PF8. A service-centered view is. Because service is defined in terms of customer-determined. PF9. All social and economic actors. Implies the context of value creation is networks of. are resource integrators.. networks (resource integrators).. Value is always uniquely and. Value is idiosyncratic, experiential, contextual, and meaning. phenomenologically determined. laden.. PF10. by the beneficiary.. Table 2.1 Service-dominant logic foundational premise modifications and additions (Vargo and Lusch 2008). 32.
(33) 2.4 Innovation— the EVAR Experience and Design-Driven Innovation 2.4.1 History of Early Innovation and Development of EVAR The first EVAR was performed by Parodi and associates using a Dacron graft sutured onto balloonexpandable Palmaz stents at the Instituto Cardiovascular de Buenos Aires (ICBA) on September 7, 1990 . (Parodi 1991) Since then, a number of commercially manufactured stent-graft devices have been developed and tested. Much work, experimentation and design preceded the launch of the clinical program. Parodi (1997) wrote that he was a resident in vascular surgery at the. 政 治 大 the results of therapy—even the most advanced—were sometimes dismaying. To 立 Cleveland Clinic in 1976, where he learned a sad truth: in aged and very sick patients,. counter this, Parodi began to think of less traumatic ways to overcome the drawbacks. ‧ 國. 學. of a major operation and dreamed of a day when patients with aneurysms could be. ‧. treated under local anesthesia in the outpatient department. Taking advantage of the. sit. y. Nat. large arterial lumens found in most aortic aneurysm patients, he conceived the idea of. io. er. introducing a polyester graft into the artery from a remote site under fluoroscopic guidance. When the target area was reached, the graft could be anchored and both. al. n. v i n ends sealed by means of a metalC component, which wound h e n g c h i U replace suture.. The first two projects failed. Parodi met Julio Palmaz in Washington DC in 1988. and realized that his stent was the component He needed to achieve good anchoring and sealing of an endoluminal graft. After completing 62 canine experiments, they performed the first successful human case as mentioned earlier. Criado (2010) listed the perceived critical milestones that made it possible for Parodi to develop an entirely new treatment solution for AAA patients and do so before anyone else. 1. First and foremost, it was Juan Parodi who provided the indispensable creativity, inventiveness, requisite focus, and perseverance to follow through (for 33.
(34) many years) until his dream was complete. 2. Much of the work and development took place in Argentina, mostly away from the then-prevailing power centers of medical technology. At the same time, the ability and rapidity of transitioning from concept to bench and then to animal experimentation and on to human application was undeniably helped by the less constraining regulatory environment. 3. Meeting Julio Palmaz in 1988 was groundbreaking: his stent turned out to be the ‗‗missing link‘‘ that completed Parodi‘s concept.. 政 治 大 and/or procured some of the most important components of the Parodi-Palmaz system, 立 4. Hector Barone, a most capable industrialist and inventor, who manufactured. supporting each and every procedure performed during the initial phase of their. ‧ 國. 學. experience.. ‧. 5. Meeting John Bergan (in Miami) in June of 1991 led to the prompt publication. sit. y. Nat. of the first English-language report before the end of that year and at a time when no. io. er. one else was listening!. 6. Treatment of the first AAA patient in the US (on November 23, 1992) was. al. n. v i n C h dissemination inUthis country and beyond and instrumental in assuring large-scale engchi providing further ‗‗validation‘‘ to the procedure and its potential.. 2.4.2 Future Perspective of Technological Innovation in EVAR Endovascular devices have been designed by trial and error, with bench and animal testing followed by human clinical trials to determine whether the devices are safe and effective. Despite remarkable advances over the past 15 years, there are persistent concerns regarding the long-term durability of endovascular devices. This may be due to deficiencies in device design, which has lagged behind other industries in adopting 34.
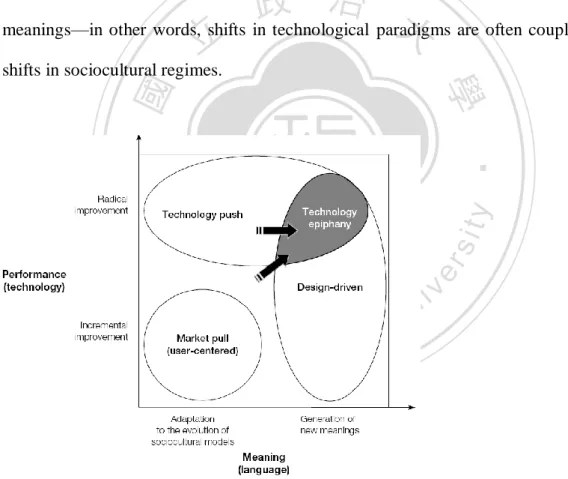
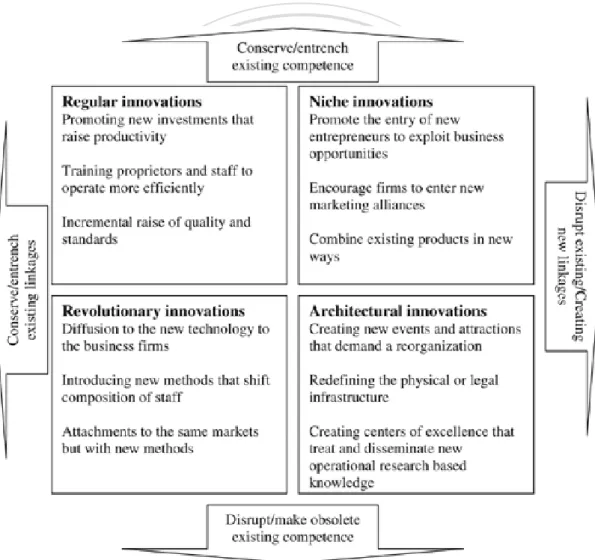
(35) computational methods that are now routinely used to design, develop, and test new aircraft and automobiles. Similar computational design and failure mode simulations that evaluate performance under stress conditions have not been widely applied in the development of endovascular devices. Advances in medical imaging and computational modeling now allow simulation of physiological conditions in patient-specific 3-dimensional vascular models, which can provide a framework to design and test the next generation of endovascular devices. This modeling will allow the prospective design of devices that can. 政 治 大 coughing, and varying degrees of exercise, as well as the extremes encountered during 立. withstand the force variations in the cardiovascular system that occur during bending,. sudden impact in contact sports. Utilization of computational design methodology that. ‧ 國. 學. takes into consideration the physiology of the cardiovascular system will improve. ‧. future endovascular devices so that they are safer and more effective and durable.. er. io. sit. y. Nat. (Zarins & Taylor, 2009). 2.4.3 Technology Epiphany: the Interplay between Technology Push and. n. al. Ch. Design-Driven Innovation. engchi. i n U. v. From the previous discussion we can all agree that scientifically speaking, EVAR is a breakthrough technological innovation. What else can we expect from EVAR? Verganti (2008) specially emphasized product meanings. Market-pull innovation starts from the analysis of user needs and subsequently searches for the technologies and languages that can actually satisfy them. Technology-push innovation is the result of dynamics of technological research. Analysis of design-intensive manufacturers such as Alessi, Artemide, and other leading Italian firms shows that their innovation process hardly starts from a close observation of user needs and requirements. Rather, they follow a different strategy 35.
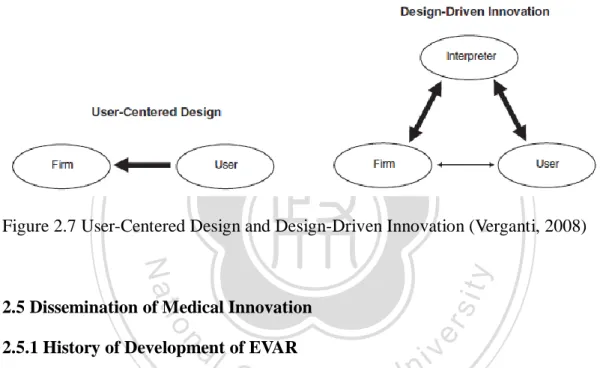
(36) called design-driven innovation. This strategy aims at radically change the emotional and symbolic content of products (i.e., their meanings and languages) through a deep understanding of broader changes in society, culture, and technology. Rather than being pulled by user requirements, design-driven innovation is pushed by a firm‘s vision about possible new product meanings and languages that could diffuse in society. (Verganti 2008). Figur 2.6 highlighted the major areas of action of the three modes of innovation. The overlap between technology push and design-driven innovation in the upper left corner of Figure 2.6 highlights that breakthrough. 政 治 大 meanings—in other words, shifts in technological paradigms are often coupled with 立. technological changes are often associated with radical changes in product. shifts in sociocultural regimes.. ‧. ‧ 國. 學. n. er. io. sit. y. Nat. al. Ch. engchi. i n U. v. Figure 2.6 Innovation Strategies (Verganti, 2008). Verganti proposed a metamodel for investigating design-driven innovation in which a manufacturer‘s ability to understand, anticipate, and influence emergence of new product meanings is built by relying on external interpreters (e.g., designers, 36.
(37) firms in other industries, suppliers, schools, artists, the media) that share its same problem: to understand the evolution of sociocultural models and to propose new visions and meanings. Managing design-driven innovation therefore implies managing the interaction with these interpreters to access, share, and internalize knowledge on product languages and to influence shifts in sociocultural models. (Fig. 2.7). 立. 政 治 大. ‧. ‧ 國. 學. Figure 2.7 User-Centered Design and Design-Driven Innovation (Verganti, 2008). sit. y. Nat. n. al. er. io. 2.5 Dissemination of Medical Innovation 2.5.1 History of Development of EVAR. Ch. engchi. i n U. v. The first EVAR was performed by Parodi and associates in 1991 using a Dacron graft sutured onto balloonexpandable Palmaz stents at the Instituto Cardiovascular de Buenos Aires (ICBA). (Parodi 1991) Since then, a number of commercially manufactured stent-graft devices have been developed and tested. Six years after Parodi‘s initial work, Zarins and Harris (1997) commented in there review paper that in good-risk patients, aneurysms > 5 cm in diameter are best treated by replacement with a prosthetic graft. Operative mortality should be < 5% and 1-year survival > 90%. Aortic endograft techniques must meet or exceed these standards if they are to supplant standard surgical repair. 37.
(38) 15 year after the first implantation, Rutherford (2006) summarized the three major trials, endovascular aneurysm repair (EVAR) 1 and 2 and Dutch Randomized Endovascular Aneurysm Management (DREAM) trials, and addressed that in patients with large AAAs who are fit for OR, EVAR offers an initial mortality advantage over OR, with a persistent reduction in AAA-related death at 4 years. However, EVAR offers no overall survival benefit, is more costly, and requires more interventions and indefinite surveillance with only a brief QOL benefit. It may or may not offer a mortality benefit over nonoperative management in patients with large AAAs who are. 政 治 大 Albuquerque et al. retrospectively analyzed non-suprarenal AAA repairs between 立. unfit for open repair, but the statistical significance of this comparison is inconclusive.. January 1, 1996, and December 31, 2008, performed at a single institution. During a. ‧ 國. 學. 13-year period, 721 patients underwent AAA repair, comprising 410 (56.9%) with. ‧. EVAR and 311 (43.1%) with open repair. A bimodal distribution of EVAR usage was. sit. y. Nat. observed, with initial escalation in the 1990s to 70%. A nadir of EVAR occurred in the. io. er. early 2000s (40%), correlating with more conservative EVAR use after the limitations of first-generation endografts were understood. Between 2005 and 2008, average. al. n. v i n EVAR use increased to 84%. C Open AAA repair became h e n g c h i U more complex during the study period. The average rate for juxtarenal open AAA repair was 17.7% (range,. 6.5%-34.6%) between 1996 and 2002 compared with 55.6% (range, 29.6%-100%) between 2003 and 2008 (P < .05). They concluded that AAA treatment has undergone a profound and sustained paradigm shift, now averaging 84% of repairs performed with EVAR between 2005 and 2008. Overall mortality from AAA repair, including ruptures, was reduced 64% (from 4.9% to 1.8%) during the 13-year study period. Although EVAR and open repair both had improved mortality in the latter half of the series, the primary driver in reduced mortality for AAA repair has been the shift to EVAR. 38.
(39) 2.5.2 Adoption of EVAR Without doubt, we‘ve seen form the previous section that there has been a trend in adopting EVAR as the preferred treatment for AAA repair. Yet, priority setting in health care is a challenge because demand for services exceeds available resources. The increasing demand for less invasive surgical procedures by patients, health care institutions and industry, places added pressure on surgeons to acquire the appropriate skills to adopt innovative procedures. Danjoux et al. conducted a qualitative case study (which is the only one the. 政 治 大 decision to adopt EVAR using a modified thematic analysis of documents and 立. author could have found from the English literature on this issue on PubMed) of the. semi-structured interviews in a Canadian medical center. Accountability for. ‧ 國. 學. Reasonableness was used as a conceptual framework for fairness in priority setting. ‧. processes in health care organizations. (Danjoux et al. 2007) Though this is the only. sit. y. Nat. work on the process of adoption of a new treatment modality, through their. io. er. sophisticated review, the concept can be extrapolated to the majority of hospitals. There were two key decisions regarding EVAR: the decision to adopt the new. al. n. v i n C decision technology in the hospital and the funding. h e n gto cstoph hospital i U. They found that such innovations are often initiated and introduced by surgeons. in the hospital setting. The decision to adopt EVAR was based on perceived improved patient outcomes, safety, and the surgeons' desire to innovate. This decision involved very few stakeholders. The decision to stop funding of EVAR involved all key players and was based on criteria apparent to all those involved, including cost, evidence and hospital priorities. Limited internal communications were made prior to adopting the technology. There was no formal means to appeal the decisions made.. 39.
(40) 2.6 Summary of Literature Review 2.6.1 Abdominal aortic aneurysm is a serious disease. The most frequent site of extracranial arterial aneurysms is the infrarenal aorta and the natural history of AAAs is continuous expansion. Rupture is the most frequent and lethal complication of AAAs. The larger the aneurysm diameter is, the greater the risk for rupture is. Thus, the goal of elective AAA repair is to prevent rupture and prolong life. The 2003 Guidelines for the treatment of abdominal aortic aneurysms published by the Joint Council of the Vascular Societies noted that treatment of AAAs. 政 治 大 cm or greater in men. For women and patients with a greater than average rupture risk, 立 is individualized and recommended operative repair for AAAs with a diameter of 5.5. an AAA diameter of 4.5 to 5.0 cm is an appropriate threshold for elective repair. For. ‧ 國. 學. high-risk patients, delay in repair until larger diameter is warranted, especially if. ‧. EVAR is not possible. The guidelines recommended EVAR as the most appropriate. io. er. that patient preference is of great importance.. sit. y. Nat. option for patients at increased risk with conventional open repair. It was emphasized. al. n. v i n C his becoming the mainstream 2.6.2 Endovascular aortic repair of AAA treatment. engchi U. The United Kingdom EVAR Trial Investigators published the trial result in New. England Journal of Medicine in 2010. The 30-day operative mortality was 1.8% in the endovascular-repair group and 4.3% in the open-repair group. The endovascular repair group had an early benefit with respect to aneurysm-related mortality, but the benefit was lost by the end of the study. They concluded in this large, randomized trial, that endovascular repair of abdominal aortic aneurysm was associated with a significantly lower operative mortality than open surgical repair. However, no differences were seen in total mortality or aneurysm-related mortality in the long term. Endovascular repair was associated with increased rates of graft-related complications 40.
(41) and reinterventions and was more costly. For high risk patients, they concluded that patients who were physically ineligible for open repair, endovascular repair of abdominal aortic aneurysm was associated with a significantly lower rate of aneurysm-related mortality than no repair. However, endovascular repair was not associated with a reduction in the rate of death from any cause. The rates of graft-related complications and reinterventions were higher with endovascular repair, and it was more costly.. 政 治 大 Open repair is more likely to be cost-effective than EVAR on average in patients 立. 2.6.3 EVAR is not as cost-effective as we expect.. considered fit for open surgery. EVAR is likely to be more cost-effective than open. ‧ 國. 學. repair for a subgroup of patients at higher risk of operative mortality. Evidence does. ‧. not currently support EVAR for the treatment of ruptured aneurysms. Further. io. er. procedures and devices should be investigated further.. sit. y. Nat. follow-up of the existing trials should be undertaken and the relative costs of. al. n. v i n C hbe encouraged and 2.6.4 Patient participation should facilitated to co-create engchi U. value.. Shared decision making is an approach where clinicians and patients communicate together using the best available evidence when faced with the task of making decisions, where patients are supported to deliberate about the possible attributes and consequences of options, to arrive at informed preferences in making a determination about the best action and which respects patient autonomy, where this is desired, ethical and legal. Shared decision-making is increasingly advocated as an ideal model of treatment decision-making in the medical encounter. The particular decision-making context 41.
(42) that we focus on is potentially life threatening illnesses, where there are important decisions to be made at key points in the disease process, and several treatment options exist with different possible outcomes and substantial uncertainty. Yet, not all patients want to participate to the same degree. In Levinson‘s study, nearly all respondents (96%) preferred to be offered choices and to be asked their opinions. In contrast, half of the respondents (52%) preferred to leave final decisions to their physicians and 44% preferred to rely on physicians for medical knowledge rather than seeking out information themselves.. 政 治 大 nor felt adequately informed prior to making a decision. At the same time, the internet 立. Many patients neither appreciated the scope of their options before AAA repair. has the potential to provide patients with information and support as an adjunct to. ‧ 國. 學. direct communication with the surgeon. Nevertheless, websites frequently accessed. ‧. by patients often lack important information regarding surgical risk. Surgeons and. sit. y. Nat. other physicians who regularly discuss AAA management options with their patients. io. er. should be aware of the potential for patients to arrive with preconceived notions based on what they have read online and be prepared to provide more complete information. n. al. on risk and outcomes.. Ch. engchi. i n U. v. In the business encounter, Vargo and Lusch proposed a service-dominant logic and addressed that service is the fundamental basis of exchange, operant resources are the fundamental source of competitive advantage, and all economies are service economies. The customer is always a co-creator of value, and the enterprise cannot deliver valve, but only offer value propositions. A service-centered view is inherently customer-oriented and relational. All social and economic actors are resource integrators and value is always uniquely and phenomenologically determined by the beneficiary. To our surprise, value propositions from different fields should ultimately join 42.
(43) together. That is, the shared decision making model is actually a service-dominant logic model.. 2.6.5 EVAR Is a Technology Epiphany? The first EVAR was performed by Parodi and associates in 1991 using a Dacron graft sutured onto balloonexpandable Palmaz stents at the Instituto Cardiovascular de Buenos Aires (ICBA). During the early development of EVAR technique and technology, first and foremost, it was Juan Parodi who provided the indispensable. 政 治 大 complete. Meeting Julio. creativity, inventiveness, requisite focus, and perseverance to follow through for many years until his dream was. 立. Palmaz in 1988 was. groundbreaking: his stent turned out to be the ‗‗missing link‘‘ that completed Parodi‘s. ‧ 國. 學. concept of anchoring a tube prosthesis to the neck of AAA endoluminally. Hector. ‧. Barone, was a most capable, but least mentioned, industrialist and inventor, who. sit. y. Nat. manufactured and/or procured some of the most important components of the. io. er. Parodi-Palmaz system, supporting each and every procedure performed during the initial phase of their experience. From these facts, we can conclude that EVAR. al. n. v i n C h of technology push— technique and technology is a product breakthrough technology engchi U. innovation.. The very first possibility of dissemination of EVAR should be attributed to John Bergan who in 1991 led to the prompt publication of the first English-language report before the end of that year and at a time when no one else was listening. An important factor affecting the adoption of EVAR was that such innovations were often initiated and introduced by surgeons at the beginning in the hospital setting. The decision to adopt EVAR was based on perceived improved patient outcomes, safety, and the surgeons' desire to innovate. The decision to continue EVAR involved all key players and was based on criteria apparent to all those involved, including cost, evidence and 43.
(44) hospital priorities. In fact, EVAR had already gained wide acceptance before the recent availability of the clinical results of those large-scale trials. The reasons, though, were not thoroughly understood.. 立. 政 治 大. ‧. ‧ 國. 學. n. er. io. sit. y. Nat. al. Ch. engchi. 44. i n U. v.
(45) Chapter III Research Methodology. This research is focused on the process of rapid adoption of an innovatively new endovascular aortic repair (EVAR) technique to treat abdominal aortic aneurysm within one year in a regional hospital in New Taipei City. At the same time span, the numbers of traditional open aortic repair procedures decreased rapidly. The author. 政 治 大 What is the reason for this paradigm shift in the treatment of abdominal aortic 立. tried to answer the following questions:. aneurysm in this certain period of time?. ‧ 國. 學. Is the same reason specific only to this particular disease and its treatment or is it. ‧. applicable to other medical arena as well?. io. 3.1.1 Research Design and Interview Guidelines. n. al. Ch. This is an exploratory and qualitative case. engchi. er. sit. y. Nat. 3.1 Research Methodology. iv n study U comprising. 1) analysis of. patient‘s medical records and hospital‘s financial records and 2) analysis of an in-depth interview. The study started with a quick description of the hospital setting in which these operations were carried out. The process of introduction of the product into the operation room and incorporation of the implantation techniques into their daily practice was also prescribed. Medical records of all those patients undergone either EVAR or open surgery were collected. A brief analysis of the medical records was provided. Each surgeon‘s pre-operative assessment and recommendation and each patient‘s pre-operative 45.
數據

+7
Outline
相關文件
As seen in Table 1 every one of them occurred in male patients; with the exception of one case all large sized sialoliths were located in the submandibular duct (94.4%) and only
This case report demonstrates a case of an unusually sized sialolith and various anatomical and physiological considerations of the duct which contribute to the higher incidence
Winnick, “Salivary gland inclusion in the anterior mandible: report of a case with a review of the literature on aberrant salivary gland tissue and neoplasms,” Oral Surgery,
pylori in pathogenesis of oral mucosal lesions or ulcerations is still unclear, it seems that patients with oral lesions as leukoplakia and oral lichen planus, and concurrent
Our case highlights an enigmatic presentation of oral submucous fibrosis and its coexistence with oral cancer presenting with unusual neurological disturbance of the inferior
Introduction Casereport Abstract Thetreatmentofdiffusesclerosingosteomyelitiswithoralbisphosphonates
A case of SAPHO syndrome with dif- fuse sclerosing osteomyelitis of the mandible treated successfully with prednisolone
Huvos, “Central salivary gland tumors of the maxilla and mandible: a clinicopathologic study of 11 cases with an analysis of the literature, ” Journal of Oral and Maxillofacial
Although AOTs rarely cause impaction of primary teeth, all of the tumors in our case were associated with primary teeth, possibly triggered by the presence of KRAS mutations
