國立臺灣大學醫學院病理學研究所 博士論文
Graduate Institute of Pathology College of Medicine National Taiwan University
Doctoral Dissertation
TERT 啟動子突變與 GATA3、CK20、CK5/6 及 p53 之 表現於膀胱泌尿上皮腫瘤之生物學意義
Biological Significance of TERT Promoter Mutation and Expression of GATA3, CK20, CK5/6 and P53 in
Urothelial Neoplasm of the Urinary Bladder
王中傑
Chung-Chieh Wang
指導教授:鄭永銘教授
Advisor: Yung-Ming Jeng, Professor
中華民國 109 年 1 月
January, 2020
口試委員會審定書
致謝
猶記八年前剛入學時,我才剛升任主治醫師不久。當時雖然已經習慣於病理 診斷工作,對於研究領域卻仍相當陌生。經過張逸良前主任的鼓勵,我報考並就 讀了病理學研究所;在鄭永銘教授不厭其煩的指導下,我從對於病理研究完全外 行的門外漢,一點一滴地產生了心得與興趣。
這八年來,研究之路其實走得跌跌撞撞。在職場上,出國進修與分院支援讓 我一度中斷學業;身體健康的問題,也讓我不得不二度休學。此外,不論是診斷 工作還是病理研究,都需要投注相當大量的時間與精力;兩者之間的優先順序安 排,常帶給我不小的考驗。我之能夠寫成論文,首先必須感謝鄭永銘教授;除了 提供研究的方向與充沛的資源,在計畫撰寫、研究技術與論文寫作方面,鄭教授 也給了我全面性的援助與教導。由於論文內容涉及臨床應用,黃昭淵醫師與蔡育 傑醫師等臨床先進的指導,對於這篇論文的完成相當重要。此外,感謝賴寶蓮小 姐協助切片與蠟塊借調;感謝莊郁琳小姐等研究助理協助進行 DNA 萃取、PCR 與 定序工作;感謝切片室與免疫組織化學室同仁在免疫染色的支援;感謝張晉豪博 士與統計諮詢團隊在生物統計上的指導。如果沒有各位的努力,這篇論文也不可 能完成。
研究的路或許稱不上辛勞,但苦悶與挫折總是在所難免。感謝愛妻柏瑩支持 著家庭,讓我能有溫暖而安穩的歸宿;感謝愛女恆音的笑容,在每天的開始帶給 我奮鬥的動力。感謝父母的勸勉與鼓勵,幫助我面對各種人生的挑戰;感謝吾弟 中瑋與吾友重佑,時時為我分憂解悶。最後,將我的感謝與讚美獻給天父上帝;
願此研究成果能使醫學進步,造福人類,榮耀祢的名。
中文摘要
膀胱泌尿腫瘤是泌尿科的常見疾病,而其治療主要依據為腫瘤分期與形態學 上的分化程度。近期分子病理研究發現了不少重要的腫瘤生物標記,但它們尚未 被整合到臨床的治療指引中。本篇論文包含兩部分,分別闡述相關標記於兩類膀 胱泌尿腫瘤中的生物學意義:早期的低度非侵襲性泌尿上皮腫瘤,以及晚期的肌 肉侵犯性膀胱癌(MIBC)。
在第一部分,我們在低度非侵襲性泌尿上皮腫瘤檢測 TERT、FGFR3 及 HRAS 三種基因的突變狀態,並分析其預後意義。TERT 基因之啟動子突變在膀胱癌頗為 常見,但是在低惡性度乳突狀泌尿上皮腫瘤(PUNLMP)的相關資料並不多。本研究 中,我們收集了 21 例良性之倒生性乳突瘤、30 例 PUNLMP,以及 34 例低度非侵 襲性乳突狀泌尿上皮癌(NIPUC)。TERT 基因之啟動子突變出現於 10 (33%)例之 PUNLMP 與 17 (50%)例之低度 NIPUC,但未出現於倒生性乳突瘤。相對於倒生性 乳突瘤,PUNLMP 與低度 NIPUC 較常出現 FGFR3 基因之突變(p = 0.009),HRAS 基因突變則較為少見(p < 0.001)。在預後方面,PUNLMP 病例有 TERT 啟動子突變 者較容易復發(p = 0.024),但是低度 NIPUC 並無此現象(p = 0.530)。此外,PUNLMP 病例有 TERT 啟動子突變者,其復發率與低度 NIPUC 無顯著差異(p = 0.487)。
在第二部分,我們分析了 GATA3、CK20、CK5/6 及 p53 在 MIBC 的表現與其 生物學意義。近期基因研究將 MIBC 區分為數種子分類,而上述之免疫組織化學 染色(IHC)標記與這些子分類有關。其中,GATA3 與 CK5/6 分別被視為管腔型與類 基底-鱗狀型的代表性標記;p53 染色常被用於代替 TP53 基因突變檢測,而傳統上 一般將細胞核染色比例高者視為異常。本研究共收集了 91 名 MIBC 病人的膀胱全 切除術組織檢體。在這些病例中,GATA3 表現量較低及 CK20 陰性者,其 Ki-67 增殖指數較高(p 值分別為 0.006 與 0.002)。相對地,CK5/6 呈廣泛性表現者,Ki-67 增殖指數較高(p = 0.001)。P53 染色則有三種類型與高 Ki-67 指數相關:完全陰性、
廣泛的細胞核強染色,以及廣泛的細胞質強染色。此外,CK20 與 CK5/6 的染色結 果通常呈現互補關係,但 91 例中的 13 例(14.29%)同時有廣泛的 GATA3 與 CK5/6 表現。在 78 名未接受術前化學治療的病人裡,GATA3 表現量較低者於單變項與多 變項分析均有顯著較高的復發率(p 值分別為 0.008 與 0.002)。CK20、CK5/6 及 p53
的表現則與預後無關。
總結來說,根據我們的研究結果,TERT 基因的啟動子突變可做為 PUNLMP 病人的預後標記。在 MIBC 病患,GATA3 的表現量則可做為膀胱切除術後的復發 危險性指標。此外,由 Ki-67 增殖指數的關聯性來看,以前述三種染色類型做為判 斷 p53 染色異常的標準,應比傳統上的核染色比例準則更佳。
關鍵詞:膀胱癌;泌尿上皮腫瘤;TERT 啟動子;GATA3;CK20;CK5/6;p53
Abstract
Clinical management of bladder urothelial neoplasm depends mainly on the tumor stage
and grade. Recent advances in molecular pathology discovered several essential
biomarkers, and their value in clinical application warrants investigation. In our study,
we focused on the relevant biomarkers in two separate fields of bladder tumors: the
early low-grade noninvasive papillary urothelial neoplasm, and the advanced
muscle-invasive bladder cancer (MIBC).
In the first part, we investigated the mutation status of the TERT promoter, FGFR3
gene, and HRAS gene in low-grade papillary urothelial neoplasms and evaluated their
prognostic significance. Mutations in the promoter region of the TERT gene have been
frequently found in urothelial carcinoma of the urinary bladder, but related data for
papillary urothelial neoplasm of low malignant potential (PUNLMP) are limited. In our
study, we included 21 cases of inverted papillomas, 30 PUNLMPs, and 34 low-grade
noninvasive papillary urothelial carcinomas (NIPUCs). TERT promoter mutations were
observed in 10 (33%) PUNLMPs and 17 (50%) low-grade NIPUCs, but not in any
inverted papilloma. FGFR3 mutations were more frequently observed in PUNLMP and
low-grade NIPUC than in inverted papillomas (p = 0.009), whereas the opposite trend
was noted for HRAS mutations (p < 0.001). Regarding the clinical outcome, TERT
but not in low-grade NIPUC (p = 0.530). Notably, PUNLMP cases with TERT promoter
mutations had a similar recurrence rate to that in low-grade NIPUC cases (p = 0.487).
Our results suggest that the status of the TERT promoter mutation may serve as a
biomarker of prognostic stratification in patients with PUNLMP.
In the second part, we investigated the biological and prognostic significance of
GATA3, cytokeratin (CK) 20, CK5/6 and p53 in MIBCs from 91 patients who
underwent radical cystectomy. Genetic profiling studies on muscle-invasive bladder
cancers (MIBCs) have discovered several subtypes with different biological
characteristics, and these markers were found to be associated with the molecular
subtypes. According to our results, high Ki-67 indices were associated with negative
CK20 (p = 0.002) and diffuse CK5/6 (p = 0.001) staining. By contrast, tumors with
diffuse GATA3 expression had low Ki-67 index (p = 0.006). Regarding p53, three
staining patterns were associated with a high Ki-67 index: (1) complete absence, (2)
diffusely strong nuclear reactivity, and (3) diffusely strong cytoplasmic staining (p <
0.001 compared with other patterns). CK5/6 and CK20 expression was typically present
in a reciprocal fashion; however, diffuse GATA3 and CK5/6 coexpression was observed
in 13 (14.29%) cases. Among 78 chemotherapy-naïve patients, low GATA3 staining was
associated with worse recurrence-free survival in both univariate (p = 0.008) and
multivariate analyses (p = 0.002). CK20, CK5/6, or p53 expressionwas not associated
with clinical outcome. Based on our results, IHC staining for GATA3 may help risk
stratification in patients with MIBC receiving radical cystectomy. In addition, the
differences in Ki-67 indices suggested that aberrant p53 expression was better defined
by the three aforementioned patterns, rather than percentage of nuclear staining alone.
Keywords: Bladder cancer; urothelial neoplasm; TERT promoter; GATA3; cytokeratin
20; cytokeratin 5/6; p53
目錄
口試委員會審定書 ... i
致謝 ... ii
中文摘要 ... iii
Abstract ... v
1. Introduction ... 1
1.1 Classification of urothelial neoplasm of the urinary bladder ... 1
1.2 Clinical management on different categories of the bladder tumors ... 1
1.3 Current problem in management of PUNLMP... 3
1.4 Common gene mutations in low-grade urothelial neoplasms ... 3
1.4.1 TERT promoter mutations ... 4
1.4.2 FGFR3 mutations ... 5
1.4.3 HRAS mutations ... 6
1.5 Molecular classification of MIBC ... 7
1.5.1 Lund and MDA Classification Systems ... 7
1.5.2 Consensus Molecular Classification System ... 8
1.5.3 Possible surrogate markers for molecular subtypes of MIBC ... 9
1.6 TP53 mutation and p53 IHC staining ... 10
1.7 Aims of our study ... 11
2. Materials and Methods ... 12
2.1 Patients and specimens ... 12
2.2 DNA extraction and sequencing ... 13
2.3 IHC staining ... 14
2.4 Clinicopathological correlation and survival analysis ... 15
3. Results ... 17
3.1 Mutation status in each histological entity of low-grade noninvasive papillary
urothelial neoplasms ... 17
3.2 Prognostic significance of the mutation status in PUNLMP and low-grade NIPUC ... 18
3.3 Prognostic grouping by combination of histological classification and mutation status of TERT promoter ... 19
3.4 Demographic and clinicopathological data regarding patients with MIBC .. 20
3.5 Association among GATA3, CK20 and CK5/6 staining in MIBC ... 20
3.6 Association of Ki-67 index with GATA3, CK20, CK5/6 and p53 expression in MIBC ... 21
3.7 Intratumoral heterogeneity in MIBC ... 23
3.8 Prognostic significance of the IHC markers in MIBC ... 24
4. Discussion ... 25
4.1 Biological significance of TERT promoter mutation in papillary urothelial neoplasm of low malignant potential ... 25
4.2 Biological significance of GATA3, cytokeratin 20, cytokeratin 5/6 and p53 expression in MIBC ... 29
5. Conclusion ... 33
Reference ... 34
圖目錄
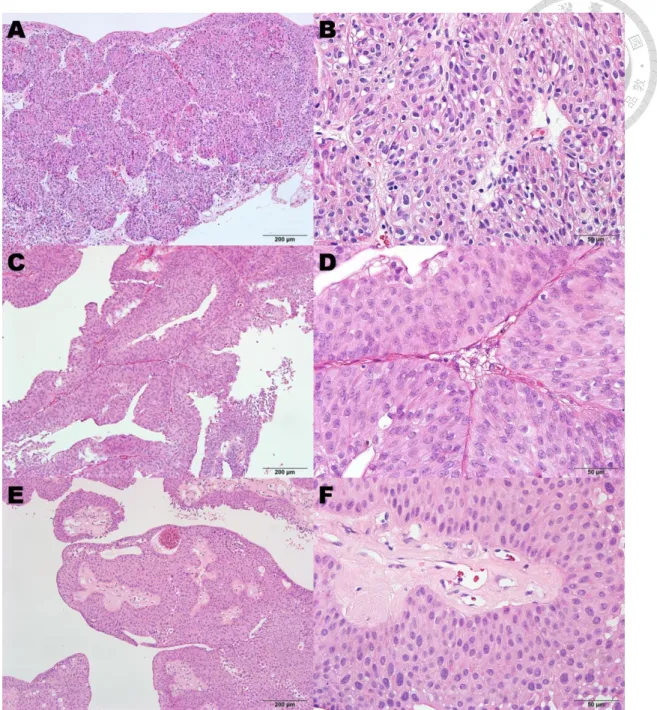
Figure 1. Representative histological images of inverted papilloma, PUNLMP, and
low-grade NIPUC. ... 44 Figure 2. Scoring criteria for p53 IHC staining ... 45 Figure 3. Common point mutations in the TERT promoter region, FGFR3 gene, and
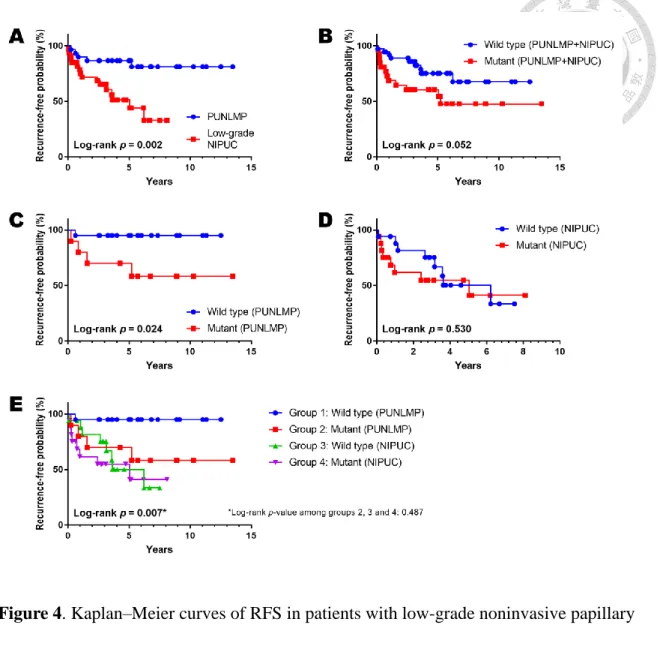
HRAS gene. ... 46 Figure 4. Kaplan–Meier curves of RFS in patients with low-grade noninvasive papillary
urothelial neoplasms ... 47 Figure 5. (A) Two examples showing reciprocal staining patterns of CK20 and CK5/6
in MIBC. (B) Two examples showing diffuse coexpression of GATA3 and CK5/6 ... 48 Figure 6. Intratumoral heterogeneity in case RC01-22 ... 49 Figure 7. Kaplan–Meier curves regarding the 78 patients with chemotherapy-naïve
MIBC. ... 50
表目錄
Table 1. Primer sequences for mutation analysis ... 51 Table 2. Immunoreactive score (IRS) by Remmele and Stegner’s criteria ... 52 Table 3. Clinical characteristics and mutation status of patients with inverted papilloma,
PUNLMP, and low-grade NIPUC ... 53 Table 4. Detailed mutation status of inverted papilloma, PUNLMP, and low-grade
NIPUC ... 54 Table 5. Clinicopathological features of the 91 patients who received radical
cystectomy ... 55 Table 6. Correlation among GATA3, CK20, CK5/6, and Ki-67 index ... 56 Table 7. Association between Ki-67 and other IHC markers ... 57 Table 8. Cox regression analysis of clinical outcomes in the 78 chemotherapy-naïve
patients with MIBC using tumor staging and percentages of IHC staining .. 58 Table 9. Cox regression analysis of clinical outcomes in the 78 chemotherapy-naïve
patients with MIBC using tumor staging and immunoreactive scores (IRS) of GATA3, CK20 and CK5/6 staining ... 59
1. Introduction
1.1 Classification of urothelial neoplasm of the urinary bladder
Urothelial neoplasm of the urinary bladder, or simply bladder tumor, is a major disease
entity commonly encountered by physicians in urology and genitourinary pathology.
This entity encompasses a wide spectrum from the totally benign urothelial papilloma to
advanced bladder cancer. According to the general concept of pathology, the current
version of World Health Organization (WHO) Tumor Classification roughly divides
urothelial neoplasms into the infiltrating urothelial carcinoma and noninvasive
urothelial lesions [1, 2]. The noninvasive neoplasms can be further divided into flat and
papillary lesions by their growth pattern, and the latter includes four categories by the
ascending order of aggressiveness: (1) urothelial papilloma, (2) papillary urothelial
neoplasm of low malignant potential (PUNLMP), (3) low-grade noninvasive papillary
urothelial carcinoma (NIPUC), and (4) high-grade NIPUC [2, 3].
1.2 Clinical management on different categories of the bladder tumors
Clinical management on the urothelial neoplasms depends mainly on the tumor stage
and the histologic grade for noninvasive lesions [4]. From the clinical point of view,
invasion of the bladder tumor into or beyond muscularis propria (stage T2 or more)
warrants aggressive treatment such as radical cystectomy. These advanced tumors are
also known as muscle-invasive bladder cancers (MIBCs) in the clinical usage and
treatment guidelines [4]. Systemic chemotherapy prior to operation, or neoadjuvant
chemotherapy, may be required in some MIBC patients. By contrast, treatment of
infiltrating urothelial carcinomas limited to the lamina propria (stage T1) is similar to
that of high-grade NIPUC. Although these tumors have potential in progression to
MIBC, most patients require only limited tumor resection, intravesical chemotherapy,
and close clinical follow-up [4].
As their designation implies, patients with low-grade noninvasive papillary lesions
usually follow an indolent clinical course. Urothelial papillomas are totally benign and
do not recur after resection [2]. Low-grade NIPUC has potential of recurrence and even
progression, but most patients require only surgical resection and follow-up [4].
Between them is the entity of PUNLMP, which is characterized by thickening of the
urothelium with minimal cytological atypia [2, 3]. This entity is specific to the urinary
tract and not equivalent to any certain premalignant lesion in other organs. Although it
is associated with a better clinical outcome compared to low-grade NIPUC, it still has
low potential of recurrence. In addition, the differential diagnosis between PUNLMP
and low-grade NIPUC depends only on the degree (minimal versus mild) of nuclear
atypia [2, 3], and this can be subjective in clinical practice. Therefore, WHO Tumor
Classification recommends that patients with PUNLMP should be managed in the same
manner as those with low-grade NIPUC [2].
1.3 Current problem in management of PUNLMP
Although we already have well-established treatment guidelines for the bladder
urothelial neoplasms, there are still problems to be solved. Current recommendation for
management of PUNLMP is resection and clinical follow-up, but most cases of
PUNLMP never recur or progress (hence the name “low malignant potential”) [2, 3]. In
my speculations, PUNLMP may be further divided into two groups: (1) benign
papillomatous tumors with thickened urothelium, and (2) low-grade NIPUC with
minimal nuclear atypia. Identification of the first group can avoid unnecessary clinical
follow-up in these patients, but these two groups cannot be distinguished by
morphology alone. Genetic studies may provide clues for classification, and knowledge
about the common genetic changes in PUNLMP becomes important in design of our
studies.
1.4 Common gene mutations in low-grade urothelial neoplasms
As the evidence from genetic studies suggests, urothelial neoplasms are likely to
develop through two different routes: high-grade and low-grade pathways [1, 5].
Histologic characteristics of the tumors are often parallel to their genetic changes, as
inactivating mutations of the TP53 gene and subsequent genomic instability are more
commonly seen in tumors with high-grade features [1, 5]. By contrast, mutations
involving the tyrosine kinase receptor gene FGFR3 and the oncogene HRAS are mainly
associated with the more indolent low-grade papillary urothelial neoplasms [1, 2, 5]. In
addition to these grade-specific alterations, TERT promoter mutations were found in a
considerable percentage of tumor samples regardless of the tumor stage and histologic
grade [6–9]. Details about the three frequently-mutated genes in low-grade urothelial
neoplasms (TERT, FGFR3, and HRAS) are described in the following sections.
1.4.1 TERT promoter mutations
The TERT gene encodes the human telomere reverse transcriptase, which maintains the
telomere length in tumor cells. Mutations in the promoter region of the TERT gene have
been found in not only bladder cancer but also other types of human cancers, including
malignant melanoma, thyroid carcinoma, and glioma [6]. In bladder cancer, C228T was
reported to be the most common mutation pattern in the TERT promoter [7]. In the two
series included by Allory et al., TERT promoter mutations were identified in 70% and
79% of the bladder cancer samples, respectively [7]. Vinagre et al. found TERT
promoter mutations in 67% and 56% of low-grade and high-grade tumors, respectively
[6]. Hosen et al. reported that the rate of the TERT promoter mutation was 66.5% in 158
NIPUC cases, which is similar to a mutation rate of 65.4% in 327 combined cases of all
stages of bladder cancer [8]. Allory et al. also found that TERT promoter mutations
were not significantly associated with the histologic grade, tumor stage, or clinical
outcome [7].
The data of TERT promoter mutations described above included samples with
different grades and stages, and studies focused on low-grade papillary urothelial
neoplasms are limited. Cheng et al. reported the presence of TERT promoter mutations
in PUNLMP (15 of 35 cases), benign urothelial papilloma (12 of 26 cases) [10], and
inverted papilloma (4 of 26 cases) [9]. Rodriguez Pena et al. collected 30 de novo cases
of PUNLMP and found TERT promoter mutations in 19 (63%) of them. In addition,
there was no association between TERT promoter mutations and the recurrence rate [11].
Taken together, the biological significance of TERT promoter mutations in these
low-grade urothelial lesions remains elusive according to current evidence.
1.4.2 FGFR3 mutations
FGFR3 gene encodes the human fibroblast growth factor receptor 3, and mutations
in this gene are found in both urothelial carcinoma [12, 13] and benign urothelial
papillomas [14, 15]. FGFR3 mutations occur mainly in the exons 7, 10, and 15, and the most common form is S249C (g. C746G) close to the 3’ end of the exon 7 [12–17].
These mutations are associated with lower grade and lower stage bladder cancers and
are thus considered a favorable prognostic marker [1, 16, 17]. Furthermore, a previous
study demonstrated a correlation between FGFR3 mutations and improved
progression-free survival (PFS) [17]. In contrast to their well-established role in
urothelial carcinoma, evidence about FGFR3 mutations in PUNLMP is limited. One
recent study showed 60% of cases with mutated FGFR3 gene in a series of PUNLMP,
and no significant association with clinical outcome was found [11]. The value of
FGFR3 mutations in stratification of PUNLMP may need further investigation.
1.4.3 HRAS mutations
Mutations in another mitogen-activated protein kinase pathway-related gene,
HRAS, have been observed in some urothelial carcinomas [18, 19]. One large-scale
study showed an overall RAS mutation rate of 4% to 15% cases in MIBC depending on
the molecular subtype [20] (see section 1.5 for details). HRAS mutations are more
common in the benign inverted papillomas, as the percentage reached 81% (13/16) in
two separate studies [21, 22]. The most common form of HRAS mutations was Q61R,
which occurred in exon 3 of this gene [18, 21, 22]. Evidence about HRAS mutations is
other low-grade papillary urothelial neoplasms was more limited; the percentages of
mutation were 18% (2/11) and 3% (1/30) in urothelial papilloma and PUNLMP,
respectively, according to two separate studies [11, 22]. The association of HRAS
mutations and malignant potential in urothelial neoplasms is uncertain under current
evidence.
1.5 Molecular classification of MIBC
While tumor recurrence is the main issue in management of low-grade papillary
urothelial neoplasms, MIBC could result in systemic metastasis and mortality. The
current treatment guidelines for MIBC are based on the tumor stage, overall clinical
condition, and the patient’s response to treatment [4]. In the recent decade, several
independent studies have revealed distinct molecular subtypes by analyzing mRNA
expression profiles in bladder UC specimens [23–26]. The concept of molecular
classification in bladder UC is similar to that in breast cancers [27, 28], and
immunohistochemical (IHC) staining for the breast cancer subtype-associated markers
has been incorporated in the treatment guidelines [29, 30]. Based on the achievements
in breast cancer studies, surrogate IHC markers for molecular subtypes of MIBC may
aid clinical management of the disease.
1.5.1 Lund and MDA Classification Systems
Before proceeding, we first take a brief review of the evolution in the molecular
classification systems. In 2012, a research group from Lund University (Sjödahl et al.)
revealed five distinct subtypes by analyzing the mRNA expression profiles in bladder
urothelial carcinomas. They named these subtypes as (1) urobasal A, (2) genomically
unstable, (3) infiltrated, (4) urobasal B, and (5) squamous cell carcinoma (SCC)-like,
according to their histologic or genetic characteristics [23]. Another group from MD
Anderson Cancer Center (Choi et al.; abbreviated as MDA) described three subtypes
including (1) luminal, (2) basal, and (3) p53-like [24]. Along with the study by Cancer
Genome Atlas Research Network [25], each classification system could demonstrate the
significant association with the clinical outcome [23–25]. For example, the MDA basal
subtype is associated with a higher metastatic rate and shorter disease-specific survival
(DSS) [24]. However, the subtypes among these classification systems are not
interchangable because the gene sets for mRNA profiling are different. To be more confusing, the MDA “basal” subtype has a totally different meaning from the Lund
“urobasal” subtypes [23, 24, 31].
1.5.2 Consensus Molecular Classification System
Because of the diversity among these classification systems, researchers from different groups held a consensus meeting and described a “basal/squamous-like (BASQ)”
phenotype in the bladder urothelial carcinoma [31]. This BASQ phenotype is featured
by (1) high levels of cytokeratin (CK) 5/6 and CK14 expression, (2) low levels of
FOXA1 and GATA3 expression, (3) enrichment (higher percentage) of squamous
differentiation, and (4) worse clinical outcome. Compared to other subtypes, the BASQ
phenotype is more constantly defined among different classification systems; it is
roughly equivalent to the MDA basal subtype, the Lund SCC-like subtype, and the
TCGA cluster III and IV [31].
After the consensus meeting, the researchers organized a multi-national study
using 1750 MIBC transcriptomes and analysis of independent molecular classification
systems [32]. The described a “consensus” set of six molecular classes: (1) luminal
papillary, which is enriched in noninvasive papillary components, (2) luminal
non-specified, (3) luminal unstable, (4) stroma-rich, (5) basal/squamous, which is
similar to the concept of BASQ phenotype, and (6) neuroendocrine-like, in the
descending order of overall survival (OS). These “consensus” subtypes differ in not
only histologic and clinical characteristics but also possibly underlying oncogenic
mechanisms [32].
1.5.3 Possible surrogate markers for molecular subtypes of MIBC
As stated in the previous section, four IHC markers are associated with the BASQ
phenotype described by Lerner et al.: CK5/6, CK14, FOXA1, and GATA3 [31]. Choi et
al. also reported consistency between the results of IHC staining and mRNA expression
profiles in basal (CK5/6-positive) and luminal (CK20-positive) subtypes [24]. Dadhania
et al. further proposed that IHC study on GATA3 and CK5/6 may sufficiently identify
these two subtypes with more than 90% accuracy [33]. Among these IHC markers,
GATA3, CK20, and CK5/6 are frequently used in the practice of diagnostic pathology.
The prognostic significance of GATA3 has been investigated in previous studies, but the
results were controversial. Miyamoto et al. revealed poor clinical outcome in MIBC
with negative or decreased GATA3 expression [34], but three other studies
demonstrated no prognostic significance of GATA3 staining in bladder UC [35–37].
Similarly, negative GATA3 staining in upper-tract UC (UTUC) was associated with
poor clinical outcome in one study [38] but not in another [39]. The potential
importance of these IHC markers in MIBC warrants further investigation.
1.6 TP53 mutation and p53 IHC staining
In addition to subtype-specific genetic changes, TP53 mutation is common in bladder
urothelial carcinoma. In the practice of diagnostic pathology, IHC expression of p53 is
commonly used as a surrogate marker for TP53 mutations. This is based on the finding
that missense mutations in TP53 increase the half-life of p53, thereby increasing the
percentage of positive IHC staining for p53 [40–42]. Traditionally, a positive p53
staining is defined as nuclear reactivity over a certain cut-off percentage, whereas the
absence of p53 staining indicates a negative result [43, 44]. By using this criterion, the
correlation of p53 IHC staining with clinical outcome may be controversial [43].
Studies on ovarian and endometrial carcinoma have reported two patterns related to
TP53 mutation–associated aberrant p53 staining: diffusely strong nuclear reactivity and
complete absence of staining [45, 46]. The cut-offs for diffuse nuclear staining were
60% and 75% for ovarian [45] and endometrial [46] carcinoma, respectively. A bladder
cancer study also demonstrated that abnormal (negative or ≥50%) p53 staining was
correlated with significantly worse recurrence-free survival (RFS) [44]. Therefore, the
clinical significance of p53 IHC staining in bladder cancers also requires further
investigation.
1.7 Aims of our study
In order to improve clinical management of bladder tumors, we investigated the
mutation status of the TERT promoter, FGFR3 gene, and HRAS gene in cases of
low-grade papillary urothelial neoplasms, including inverted papilloma, PUNLMP, and
low-grade NIPUC. We then analyzed the association between the mutation status and
the clinical outcome in these cases. In addition, we evaluated the IHC expression of
GATA3, CK20, CK5/6 and p53 in a series of MIBC cases and correlated them with the
associated clinical outcome, Ki-67 proliferative index, and other clinicopathological
parameters to investigate their clinical significance.
2. Materials and Methods
2.1 Patients and specimens
The patients included in our study were retrieved from the database of pathological
diagnosis in the Department of Pathology, National Taiwan University Hospital
(NTUH). For cases of low-grade noninvasive papillary urothelial neoplasm, we
recruited all 66 patients diagnosed as PUNLMP of the urinary bladder from 2005 to
2014 and collected their tissue specimens of initial diagnosis. Four patients with the initial diagnosis of “transitional cell carcinoma, grade I” from 2000 to 2004 were also
added to our study cohort. In addition, we randomly selected 26 patients with inverted
papilloma from 2005 to 2014 for comparison. Hematoxylin and eosin (H&E)-stained
sections of all cases were reviewed and reclassified according to the WHO 2016 tumour
classification (Figure 1). Cases without adequate tumor contents for DNA extraction
were excluded from the analysis. After confirming the histologic diagnosis of each case,
the patients’ age, sex, and follow-up data (status and periods of tumor recurrence and
progression) were recorded. Tumor progression was defined as recurrence as high-grade
NIPUC, urothelial carcinoma in situ, or invasive urothelial carcinoma. One
representative section with an adequate tumor part and the corresponding formalin-fixed
paraffin-embedded (FFPE) tissue block were selected for each case. This part of study
th
201508043RIND; revised on Dec 30th, 2016).
For MIBC cases, we included all 109 patients who underwent radical cystectomy
from 2010 to 2016 and collected their clinical data. Patients with a history of UTUC
were excluded to avoid confounding prognostic analysis. In each patient who received
neoadjuvant chemotherapy, the latest resection specimen prior to cystectomy was
selected for this study. In this group, those who did not have a preoperative specimen
available at NTUH were excluded from this study. In patients without neoadjuvant
chemotherapy, the cystectomy specimens were selected. Alternatively, the latest
resection specimen before cystectomy was selected if no adequate tumor cells were
present in the cystectomy specimen. H&E-stained sections of all cases were reviewed
and re-staged by the TNM classification system defined in the AJCC Cancer Staging
Manual (8th edition). Cases without definite muscularis propria invasion were excluded
at this point. One representative section with an adequate tumor part and the
corresponding FFPE tissue block were selected for each case. This part of study was
approved by the Research Ethics Committee of NTUH on Oct 16th, 2017 (No.
201708055RIND; revised on Aug 17th, 2018).
2.2 DNA extraction and sequencing
For each case with low-grade noninvasive papillary urothelial neoplasm, five 10-μm
unstained slides were sectioned from the representative tissue block. DNA was extracted
using the QiaAmp DNA FFPE Tissue Kit (Qiagen, Hilden, Germany) following the
manufacturer’s instructions. The mutation hotspots in the promoter region of the TERT
gene, 3 exons of coding regions in the FGFR3 gene, and 1 exon in the HRAS gene were
amplified through polymerase chain reaction (PCR). The amplicons of the FGFR3 gene
included codons 248 and 249 in exon 7, codons 372 and 375 in exon 10, and codon 652
in exon 15. A similar assay in the HRAS gene focused on codon 61 in exon 3. We
selected these exons of the target genes based on previous reports showing the frequent
mutated genes in urothelial neoplasms and their mutational hot spots [6–19]. The
primers for PCR are listed in Table 1, and the Sanger method was used to sequence the
PCR products.
2.3 IHC staining
For each case with MIBC, 5-μm sections were taken from the representative tissue
block for IHC staining. The staining procedures were conducted with a Ventana
Benchmark XT autostainer (Ventana Medical Systems, Tucson, AZ, USA) according to
the manufacturer’s instructions. Primary antibodies against p53 (clone DO-7, dilution
1:1000, Dako Denmark A/S, Glostrup, Denmark), GATA3 (clone L50-823), CK20
(clone SP33), CK5/6 (clone D5/16B4), and Ki-67 (clone 30-9) were included. All
antibodies other than anti-p53 antibody were purchased from Ventana Medical Systems
and were ready to use. The antibody reactivity was visualized with a Ventana OptiView
DAB IHC Detection Kit. Finally, the slides were counterstained with hematoxylin.
All IHC results were examined under a light microscope and scored under the
following criteria. The percentage and intensity of tumor cells stained with GATA3
(nuclear staining), CK20, and CK5/6 (membranous-type or cytoplasmic staining) were
recorded for each case and their immunoreactive scores (IRS) were calculated using
Remmele and Stegner’s criteria [47, 48] (Table 2). According to the cut-offs used in
IRS, their staining percentage was also classified as negative (<10%), partial
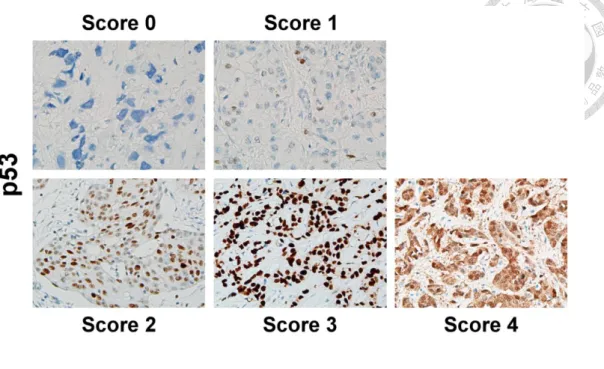
(10%–80%), and diffuse (>80%). The standards for p53 scores are demonstrated in
Figure 2 by combining the criteria used in prior studies of bladder [44] and ovarian [45,
49] cancers. The Ki-67 indices were evaluated by following the recommendations from
the International Ki67 in Breast Cancer Working Group [50]. In brief, at least three
400× fields containing 500 or more invasive tumor cells were selected for each case.
Tumor cells with nuclear staining were considered positive regardless of the staining
intensity. The Ki-67 index was calculated as the percentage of the positive cells among
the total number of tumor cells in the scored area.
2.4 Clinicopathological correlation and survival analysis
Student t test and one-way analysis of variance (ANOVA) were used to evaluate
differences in the continuous parameters between or among comparable groups.
Chi-square test and Spearman rank correlation test were applied to analyze the
association among categorical and continuous parameters, respectively. For cases of
PUNLMP and low-grade NIPUC, we calculated the cumulative recurrence-free survival
(RFS) and PFS from the point of initial diagnosis by using the Kaplan–Meier method.
In chemotherapy-naïve MIBC patients, we calculated OS and DSS after radical
cystectomy in addition to RFS. The differences in survival time were determined using
log-rank tests. For MIBC patients, Cox regression was used to determine the association
between continuous parameters and clinical outcomes. Multivaraite analyses were also
performed using Cox regression. P < 0.05 was considered statistically significant. Cox
regression was performed with SAS (version 9.4; SAS Institute Inc., Cary, NC, USA)
with the assistance of the Department of Medical Research, NTUH, and the other
statistical analyses were conducted using Microsoft Excel 2007 and Prism (version 7.03;
GraphPad Software, Inc., La Jolla, CA, USA).
3. Results
3.1 Mutation status in each histological entity of low-grade noninvasive papillary
urothelial neoplasms
After review of all 96 cases with low-grade noninvasive papillary urothelial neoplasms,
4 were reclassified as high-grade NIPUC and excluded from our study. Four additional
cases were excluded because the tissue specimens of initial diagnosis were not available
or limited in amount. In the mutation analyses, PCR for TERT promoter sequences were
unsuccessful in 3 cases after two repeated experiments. These 3 cases were also
excluded. The 85 cases finally included in this study comprised 21 inverted papillomas,
30 PUNLMPs, and 34 low-grade NIPUCs. The clinical characteristics of patients and
the results of the mutation status in each entity were summarized in Table 3.
TERT promoter mutations were found in 33% (10 of 30) of PUNLMP, 50% (17 of
34) of low-grade NIPUC and none of the 21 inverted papillomas. The rates of FGFR3
mutations were also much higher in PUNLMP (30%, 9 of 30) or low-grade NIPUC
(50%, 17 of 34) than in inverted papilloma (10%, 2 of 21) (p = .009). Conversely, HRAS
mutations were more frequently observed in inverted papilloma (76%, 16 of 21) than in
PUNLMP (10%, 3 of 30) or low-grade NIPUC (15%, 5 of 34) (p < .001). We compared
the mutation frequency between PUNLMP and low-grade NIPUC groups and found no
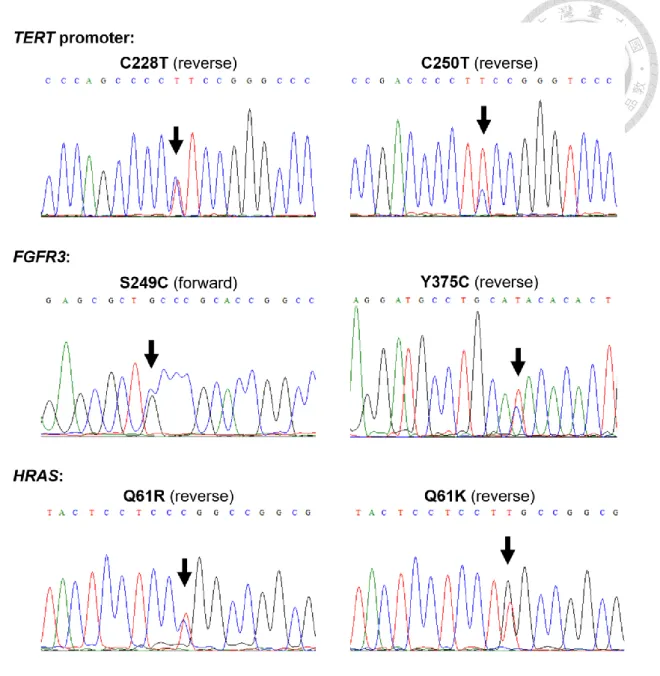
Regarding mutation patterns, the most frequent point mutation in the TERT
promoter region was C228T (19 of all 27 mutated cases), followed by C250T (6 of 27
cases) and C228A (2 of 27 cases) (Figure 3, upper panel). The most common mutation
in FGFR3 was S249C (16 of all 28 mutated cases), followed by Y375C (7 of 28 cases)
(Figure 3, middle panel). Other mutations in FGFR3 included G372C (1 case), S373C
(1 case), K652E (1 case), and K652T (2 cases). Mutations in the HRAS gene included
Q61R (14 of all 24 mutated cases), Q61K (7 cases), and Q61L (3 cases) (Figure 3,
lower panel) (Table 4).
3.2 Prognostic significance of the mutation status in PUNLMP and low-grade
NIPUC
The PUNLMP and low-grade NIPUC patients were followed at our outpatient clinics
with a median follow-up period of 5.7 years, and most (61 of 64, 95.3%) cases have
been followed for more than 2 years. We first analyzed the clinical outcomes of all
patients with PUNLMP or low-grade NIPUC. Patients with low-grade NIPUC had
shorter RFS than those with PUNLMP (p = 0.002, Figure 4A), and the TERT promoter
mutation status had borderline significance regarding RFS in these patients (p = 0.052,
Figure 4B). We then separately analyzed the survival data of 30 patients with PUNLMP
and 34 patients with low-grade NIPUC. In the PUNLMP group, patients with TERT
promoter mutations had shorter RFS than those without mutations (p = 0.024, Figure
4C). In contrast, the TERT promoter mutation status was not related to RFS in the
low-grade NIPUC group (p = 0.530, Figure 4D).
Tumor progressions occurred in only three patients. One patient progressed from
PUNLMP to high-grade NIPUC and then high-grade invasive urothelial carcinoma. The
other patient initially diagnosed as PUNLMP progressed to high-grade invasive
urothelial carcinoma directly. The third patient progressed from low-grade NIPUC to
high-grade NIPUC and then high-grade invasive urothelial carcinoma. Neither the
histologic entity nor the TERT promoter mutation status had significant impact on PFS.
In addition, mutation status of the FGFR3 gene has no prognostic association in
PUNLMP, low-grade NIPUC, or combined. Analysis of the association between
survival and the mutation status of HRAS was not performed due to the limited number
of mutated cases in each group.
3.3 Prognostic grouping by combination of histological classification and mutation
status of TERT promoter
Because of the prognostic significance of the TERT promoter mutation in PUNLMP, we
further categorized PUNLMP and low-grade NIPUC cases into 4 groups based on the
mutation status of the TERT promoter. Group 1 was defined as PUNLMP cases without
TERT promoter mutations, and group 2 represented those with the mutations.
Low-grade NIPUC cases with wild-type and mutated TERT promoter regions were
referred to as groups 3 and 4 respectively. We then compared the Kaplan-Meier curves
of RFS among these groups, and the result was shown in Figure 4E. The recurrence rate
of PUNLMP without TERT promoter mutations (group 1) was significantly lower than
other groups (overall p = 0.007). Moreover, there was no significant difference in RFS
among PUNLMP with TERT promoter mutations (group 2) and low-grade NIPUC cases
(groups 3 and 4; p = 0.487).
3.4 Demographic and clinicopathological data regarding patients with MIBC
Among the 109 patients recruited for our MIBC study, definite muscularis propria
invasion (i.e. stage pT2 or higher) was not identified in 9, the microscopic slides were
unavailable in 7, a history of UTUC was noted in 1, and loss to follow-up after radical
cystectomy was noted in 1; these 18 cases were all excluded. Finally, we included 91
patients (median age: 67 years [range: 39–89 years]; male-to-female ratio: 2.37:1). Of
them, 13 (14.3%) received neoadjuvant chemotherapy. In patients not receiving
neoadjuvant chemotherapy, the median follow-up time was 2.46 years. The
demographic and clinicopathological data of these patients are summarized in Table 5.
3.5 Association among GATA3, CK20 and CK5/6 staining in MIBC
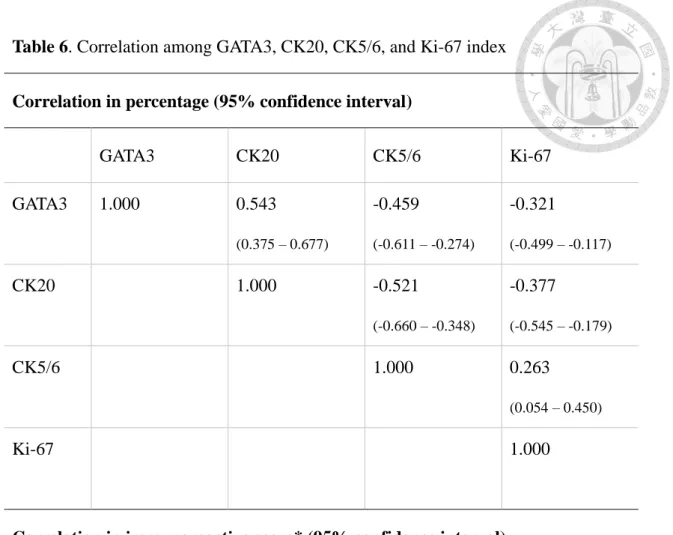
After completion of IHC, we evaluated the correlation of the staining results among
each marker. The results are summarized in Table 6. First, CK20 and GATA3
demonstrated a positive correlation in terms of both percentage and IRS score. The
percentage of GATA3 staining tended to be higher than that of CK20, and CK20
staining was stained on GATA3-positive tumor cells in most cases. By contrast, a
negative correlation was observed between CK20 and CK5/6. In cases with both CK20
and CK5/6 reactivity, the staining patterns of these two markers were generally
reciprocal. Although they were not completely mutually-exclusive, CK20 tended to be
stained on CK5/6-negative tumor cells and vice versa. Figure 5A illustrates two
examples of such a reciprocal pattern. Of the 21 (23.08%) tumors with minimal
(1%–9%) CK5/6 staining, 5 (5.49%) demonstrated basal alignment in the aggregates of
tumor cells. Because the case number was limited, analyzing the biological significance
of such a pattern is unfeasible.
Similar to CK20, GATA3 showed negative correlation with CK5/6 expression.
However, coexpression of GATA3 and CK5/6 was observed in 44 (48.35%) cases; of
them 13 (14.29%) had diffuse coexpression (staining in >80% of tumor cells for both
markers). Two examples of GATA3/CK5/6 coexpression are illustrated in Figure 5B. In
the 13 double-positive cases, 11 (84.62%) showed completely absent or minimal
staining for CK20. Meanwhile, double-negative tumors for GATA3 and CK5/6
accounted for 3 (3.30%) of the 91 cases, and only one of them showed complete
absence for each marker.
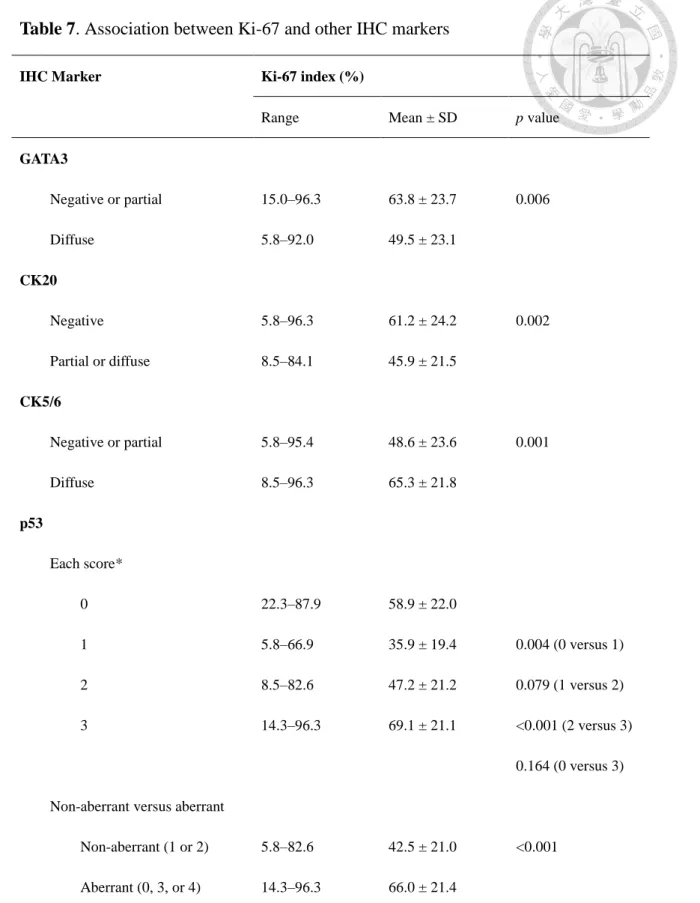
3.6 Association of Ki-67 index with GATA3, CK20, CK5/6 and p53 expression in
MIBC
As presented in Table 6, Ki-67 indices were significantly correlated with staining
percentages of GATA3, CK20, and CK5/6. We further categorized each of the latter
three markers into three groups (negative, partial, and diffuse) and compared their
difference through Ki-67 indices. Differences in Ki-67 indices was also compared
among each group of the p53 score. The results are summarized in Table 7. In brief,
tumors with diffuse GATA3 staining had significantly lower Ki-67 indices. By contrast,
high Ki-67 indices were observed in negative CK20 and diffuse CK5/6 cases. The
difference between negative and partial staining groups of GATA3 (p = 0.616) or CK5/6
(p = 0.565) was nonsignificant. Similarly, no difference was observed between cases
with partial and diffuse CK20 reactivity (p = 0.986).
The association between p53 score and the Ki-67 index was more complex.
Absence of p53 staining (score 0) was associated with a significantly higher Ki-67
index compared with the partial staining group (score 1, p = 0.004). In addition, the
score 2 group had a significantly lower Ki-67 index than the score 3 group (p < 0.001),
but no difference was found between the score 1 and 2 groups (p = 0.079). In addition,
no difference was shown between the p53-absent (score 0) and score 3 groups (p =
0.164). These findings were consistent with the definition of aberrant p53 expression in
ovarian carcinoma [41]. Notably, 1 (1.1%) case in our cohort showed diffuse
cytoplasmic staining with variable nuclear intensity (score 4). This pattern was found to
be associated with TP53 mutation in a previous study on ovarian carcinoma [49] and
considered p53-aberrant. Based on this definition, tumors with aberrant p53 staining had
significantly higher Ki-67 indices (p< 0.001). No difference in GATA3, CK20, or
CK5/6 expression was noted between p53-aberrant and non-p53-aberrant tumors.
3.7 Intratumoral heterogeneity in MIBC
In case RC01-22, a minor component (2% of total tumor area) with significantly
different morphology was observed in the tumor. Although the major part showed
considerable squamous differentiation, this minor component had usual histology of UC
with heavy lymphocytic infiltration. As for the IHC markers, the major part expressed a
typical basal/squamous profile of diffuse CK5/6 staining, minimal GATA3 reactivity,
and a non-aberrant pattern of p53. By contrast, the minor component was partially
positive for both GATA3 and CK5/6 with diffusely strong reactivity to p53 (Figure 6).
This patient demonstrated tumor recurrence after radical cystectomy, but the diagnosis
of recurrence was based on radiologic images without acquisition of tissue specimens.
For analytical purposes, the IHC profile of the major part was used for this case. No
other tumor with apparent intratumoral heterogeneity was noted in our MIBC study
cohort.
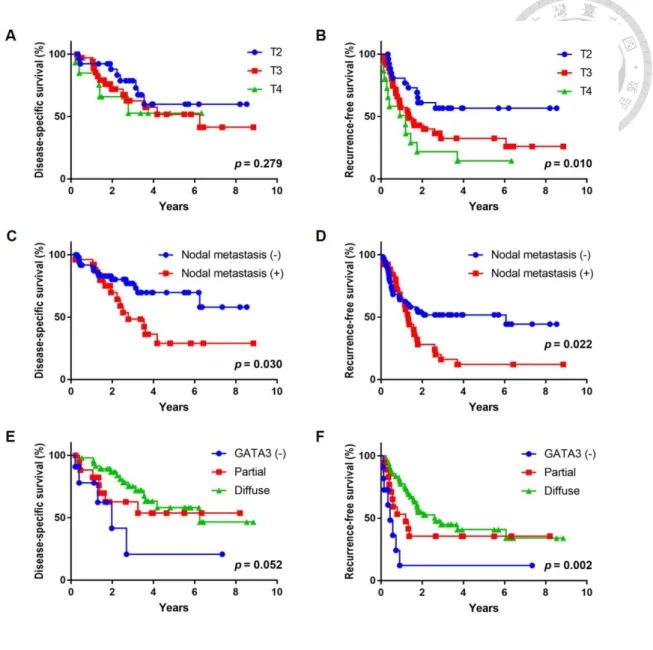
3.8 Prognostic significance of the IHC markers in MIBC
Among the IHC markers (GATA3, CK20, CK5/6, p53 and Ki-67), only GATA3
demonstrated significant correlation with clinical outcomes. In the 78 patients without
neoadjuvant chemotherapy, higher percentage of GATA3 staining was associated with a
significantly better RFS in both univariate (p = 0.008) and multivariate (p = 0.002)
analysis by using Cox regression (Table 8). Analysis by IRS revealed similar results
(Table 9). In the Kaplan-Meier plot, gradual difference in RFS was present among cases
with diffuse, partial, and negative GATA3 staining (p = 0.002). The other significant
prognostic parameters included the T stage (for RFS) and the presence of nodal
metastasis (for DSS and RFS). The Kaplan–Meier plots for GATA3, T stage, and nodal
metastasis are depicted in Figure 7.
4. Discussion
4.1 Biological significance of TERT promoter mutation in papillary urothelial
neoplasm of low malignant potential
In human oncology, urothelial neoplasm is one of the neoplasms with well-established
pathogenetic models. At the genetic level, noninvasive papillary urothelial neoplasms
can be roughly divided into 2 groups: a genetically stable low-grade group and a
genetically unstable high-grade group. High-grade urothelial neoplasms are
characterized by TP53 mutations and exhibit aggressive biological behavior [2, 51–53].
By contrast, low-grade urothelial neoplasms are less likely to result in mortality.
According to the current WHO tumor classification, low-grade neoplasms include
totally benign urothelial papillomas (including exophytic papillomas and more common
inverted papillomas), PUNLMP, and low-grade NIPUC [2]. Although PUNLMP and
low-grade NIPUC are considered indolent tumors, they are not clinically insignificant
due to their frequent recurrence and the potential of progression to high-grade NIPUC
or invasive carcinoma. Between them, patients with low-grade NIPUC are more likely
to suffer from tumor recurrence than those with PUNLMP [3], and our results are
consistent with this general finding.
According to the current WHO criteria, classification of low-grade urothelial
genetic studies [2]. Some researchers have proposed the concept of “genetic grading”
for urothelial neoplasms [17, 54], but the complexity and cost of genetic studies may
hinder the feasibility of genetic grading in clinical practice. The results of our study
indicated that PUNLMP with wild-type TERT promoter had a lower recurrence rate. In
contrast, PUNLMP cases with TERT promoter mutations had significantly higher risks
of recurrence, which were similar to those in the low-grade NIPUC group. These results
suggest that PUNLMP cases can be stratified by TERT promoter mutation status for
prognostic purposes, and investigation of this mutation status may be of value for
clinical decision when treating patients with PUNLMP.
Compared with PUNLMP, our study did not show prognostic significance for
TERT promoter mutations in patients with low-grade NIPUC. Similarly, a study of
urothelial bladder cancers by Allory et al. found no association of the TERT promoter
mutation status with the clinical outcome [7]. Rachakonda et al. reported that TERT
promoter mutations are associated with poor survival and a higher recurrence rate in
bladder cancer patients without the common polymorphism rs2853669, which is located
in a preexisting Ets2 binding site in the TERT promoter. Such an association was not
found in patients with that polymorphism. The possible mechanism underlying the
association is that TERT promoter mutations affect the clinical outcome by creating de
novo Ets/TCF binding sites, and that common polymorphism may modify such effects
[55]. However, Rachakonda et al. did not include cases of PUNLMP, and further
investigation is necessary to explain the possible mechanisms of the effects of TERT
promoter mutations in PUNLMP.
Our results showed a high prevalence (76%) of HRAS mutation in inverted
papillomas. A previous study also showed HRAS mutations in 10 (91%) of 11 inverted
papillomas, and the authors postulated that isolated RAS mutations might induce cellular
senescence and result in a benign clinical course [22]. In our cohort, the three cases of
PUNLMP with HRAS mutations did not show coexistent TERT promoter or FGFR3
gene mutations. Two of them showed partially inverted growth patterns, and none of
these three tumors recurred after resection. Although these results were inconclusive due
to the limited case number, PUNLMPs with HRAS mutations might have similar
characteristics to the benign inverted papillomas. By contrast, two of the five low-grade
NIPUCs with mutated HRAS also showed TERT promoter mutation, and one additional
case had coexistent HRAS and FGFR3 mutations in our study. None of these tumors had
inverted growth in histology. The different biologic significance of HRAS mutations in
these low-grade urothelial neoplasms may worth further investigation.
Back to the issue of TERT promoter mutation, comparing our results with previous
results is potentially problematic. For survival analysis, many studies evaluating TERT
promoter mutations in bladder tumors have included cases with different grades or
stages [7, 8, 55]. In our study, the prognostic value of TERT promoter mutations fell to
an equivocal level if PUNLMP and low-grade NIPUC cases were mixed (p = .052).
Moreover, and probably more important, the actual cut-off points of histological
classification are subject to interobserver variation [56, 57]. In fact, all of the low-grade
NIPUC cases in our study were originally diagnosed as PUNLMP or even inverted
papilloma. Although our study found no TERT promoter mutation in any case of
inverted papilloma, Cheng et al. reported TERT promoter mutations in 15% (4/26) cases
of inverted papillomas [8]. Such discrepancy might result from the ethnic factor or other
causes; however, the potential interobserver variation may influence the accuracy of
metanalysis among these studies.
There are three potential limitations in our study. First, tumor progression was
uncommon in our study cohort and thereby limiting the analysis of PFS. Secondly, we
met technical problems about TERT promoter mutation analysis in three cases,
including one PUNLMP. This incident did not affect the statistical significance in our
study, but it might hamper the clinical application of TERT promoter mutation analysis.
Finally, to minimize the potential heterogeneity in our study cohort, we only selected
the primary (initial) specimen for each patient with tumor recurrence(s). The recurrent
tumors might exhibit different mutation patterns from their primary counterparts, but
investigations of such difference and possible clinical importance were beyond our
scope in this study.
4.2 Biological significance of GATA3, cytokeratin 20, cytokeratin 5/6 and p53
expression in MIBC
GATA3 is a transcription factor useful in histological diagnosis for UC [35, 58, 59]. It is
also recognized as a marker of luminal subtype(s) in the bladder cancer according to
recent research [20, 24, 33]. In this study, we noted that tumors with decreased GATA3
staining had significantly higher Ki-67 proliferative indices. In addition, IHC staining
for GATA3 was correlated with a clinical outcome in chemotherapy-naïve patients with
MIBC. Cases with diffuse GATA3 staining had the best outcome, and a minor
proportion (12.1%) of GATA3-negative tumors were prone to early recurrence with a
borderline trend of worse DSS. The prognostic significance of GATA3 was independent
to stage and nodal metastasis in RFS. These findings are compatible with the relatively
aggressive behavior observed in the BASQ tumors [24, 26, 32, 33].
The BASQ phenotype described by Lerner et al. included positive CK5/6 and
negative GATA3 in IHC staining [31]. However, we found it difficult to define the
actual BASQ subgroup in our study cohort. In this study, diffusely strong CK5/6
staining was not necessarily associated with negative GATA3. The association of these
two markers with the Ki-67 index might aid in understinaing this problem. Difference in
the Ki-67 index was significant at a 80% cut-off for GATA3, but the tumors with
negative and partial GATA3 staining had similar Ki-67 indices. Similar relationship was
observed between CK5/6 and Ki-67 index. If we use the 80% cut-off to define the
BASQ phenotype (CK5/6 and GATA3 staining in >80% and ≤80% of tumor cells,
respectively), this subgroup would account for 20 (22.0%) cases in our MIBC cohort.
Similar to GATA3 alone, the BASQ cases had a worse RFS (p = 0.027) compared with
others in the chemotherapy-naïve group. Moreover, CK5/6 alone was not prognostically
significant regarding RFS. From the view of prognostication, decrease in GATA3
expression may be a more important component than diffuse CK5/6 staining in the
BASQ phenotype.
Although GATA3 and CK5/6 demosntrated significantly negative correlation in
our study, staining for these two markers showed certain overlap in 44 (48.4%) MIBC
cases. Furthermore, diffuse coexpression was not rarely encountered (14.29%) in our
study. Such a diffuse coexpression phenomenon has not been well-described in previous
studies, and simultaneously high GATA3 and CK5/6 expression on protein level were
uncommon or even absent in the studies by Sjödahl [60] and Hodgson [36]. Dadhania et
al. showed some cases with overlap in GATA3 and CK5/6 staining; however, tumors
with >80% positivity for both markers were absent in their data [33]. A possible
explanation to this phenomenon is the ethnic difference. Further research based on
Asian population is warranted to confirm these findings.
The prognostic significance of GATA3 in bladder UC was controversial in
previous studies [34–37]. Miyamoto et al. reported that loss of GATA3 expression
predicted poor prognosis for patients with MIBC [34], but three other studies showed
that GATA3 expression had no significant influence on either DSS or RFS [35–37]. In
addition to ethnicity, three possible reasons can explain this discrepancy. First, we used
whole slides of the tumor specimens for IHC staining instead of tissue microarrays
(TMAs), which was the case in previous studies [35–37]. Partial staining might lead to
false-negative results in TMA, and this could potentially affect the significance in
survival analyses. Second, Kollberg et al. included 66 (17%) stage T1 tumors along
with MIBC [37], which may influence the results. Finally, in contrast to previous studies
[20, 32], the molecular subtypes in their cohort was not associated with clinical
outcomes [37]. The potential difference in the underlying population might result in
such discrepancy.
As CK20 and CK5/6 are well-established markers related to molecular subtypes
[24, 31, 33, 60], it may appear unreasonable that these markers did not have prognostic
significance. However, the molecular subtypes were defined through hierarchical
analysis with a large panel of markers. Previous studies revealed that the molecular
subtypes were associated with clinical outcomes [24, 31, 33, 60], but each marker
related to the subtypes was not necessarily significant in clinical outcomes. Kollberg et
al. also showed no prognostic significance in any single subtype-associated marker [37].
Therefore, the association of GATA3 expression and clinical outcome merits further
investigation to prove its value in clinical management.
The interpretation of p53 IHC staining is also noteworthy. Although we could not
find the prognostic significance of p53 staining, the differences in the Ki-67 index
suggested that using the same criteria as those used for ovarian carcinoma would be
more suitable when interpreting p53 staining in bladder cancer. Hodgson et al.
discovered that null staining of p53 should be considered an aberrant staining pattern
[44]. Our study further revealed the potential importance of intensity in the diffuse
nuclear staining group. Tumors with diffuse nulcear staining but variable intensity for
p53 (score 2) did not have higher Ki-67 indices than did the partial staining (score 1)
group. However, the differences in the variable-intensity (score 2) and strong-intensity
(score 3) groups were significant. Based on our findings, we plan to correlate these
criteria with the TP53 gene status and verify their superiority over the traditional
overexpression criteria for bladder cancer in the future.
5. Conclusion
In conclusion, the first part of our study provided the evidence that the TERT promoter
mutation is related to a higher risk of recurrence in PUNLMP cases. Such an association
was not observed in low-grade NIPUC, although the rates of the TERT promoter
mutation were similar between these two entities. Furthermore, the risk of recurrence in
PUNLMP cases with TERT promoter mutations was similar to that of low-grade NIPUC
cases. Mutation study of the TERT promoter may facilitate risk stratification and assist
the clinical decision when treating patients with PUNLMP of the urinary bladder.
In the second part of our study, decrease in GATA3 staining was significantly
associated with high proliferative activity and poor clinical outcome in MIBC. IHC
staining for GATA3 might facilitate in risk stratification in patients with MIBC
receiving radical cystectomy. Combining CK5/6 and GATA3 for prognostic
stratification has potential problems because coexpression is common. Defining the
“aberrant” p53 staining by using the criteria for ovarian carcinoma (complete
absence,strong nuclear reactivity in ≥60% of tumor cells, or diffuse cytoplasmic
staining) may be more suitable than the traditional overexpressionconcept; however, our
results did not demonstrate the direct association of p53 expression with clinical
outcome.
Reference
1. Grignon DJ, Al-Ahmadie H, Algaba F et al. Infiltrating urothelial carcinoma. In
Moch H, Humphrey PA, Ulbright TM, Reuter VE eds. WHO Classification of
Tumours of the Urinary System and Male Genital Organs, 4th edition. Lyon, France:
IARC, 2016; 81–98.
2. Reuter VE, Algaba F, Amin MB et al. Non-invasive urothelial lesions. In Moch H,
Humphrey PA, Ulbright TM, Reuter VE eds. WHO Classification of Tumours of the
Urinary System and Male Genital Organs, 4th edition. Lyon, France: IARC, 2016;
99–107.
3. Grignon DJ. Tumors of the urinary bladder. In Amin MB, Grignon DJ, Srigley JR,
Eble JN. Urological Pathology. Philadelphia, PA: Lippincott Williams & Wilkins,
2014; 347–348, 360–364.
4. National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in
Oncology: Bladder Cancer (Version 1.2019).
5. Netto GJ. Molecular biomarkers in urothelial carcinoma of the bladder: are we
there yet? Nat Rev Urol. 2012; 9: 41–51.
6. Vinagre J, Almeida A, Pópulo H et al. Frequency of TERT promoter mutations in
human cancers. Nat Commun 2013; 4: 2185.
mutations in bladder cancer: high frequency across stages, detection in urine, and
lack of association with outcome. Eur Urol 2014; 65: 360–366.
8. Hosen I, Rachakonda PS, Heidenreich B et al. Mutations in TERT promoter and
FGFR3 and telomere length in bladder cancer. Int J Cancer 2015; 137: 1621–1629.
9. Cheng L, Davidson DD, Wang M et al. Telomerase reverse transcriptase (TERT)
promoter mutation analysis of benign, malignant and reactive urothelial lesions
reveals a subpopulation of inverted papilloma with immortalizing genetic change.
Histopathology 2016; 69: 107–113.
10. Cheng L, Montironi R, Lopez-Beltran A. TERT promoter mutations occur
frequently in urothelial papilloma and papillary urothelial neoplasm of low
malignant potential. Eur Urol 2017; 71: 497–498.
11. Rodriguez Pena MDC, Tregnago AC, Eich ML et al. Spectrum of genetic mutations
in de novo PUNLMP of the urinary bladder. Virchows Arch. 2017; 471: 761–767.
12. van Rhijn BW, Montironi R, Zwarthoff EC, Jöbsis AC, van der Kwast TH. Frequent
FGFR3 mutations in urothelial papilloma. J Pathol 2002; 198: 245–251.
13. Lott S, Wang M, Zhang S et al. FGFR3 and TP53 mutation analysis in inverted
urothelial papilloma: incidence and etiological considerations. Mod Pathol 2009; 22:
627–632.
14. Lamy A, Gobet F, Laurent M et al. Molecular profiling of bladder tumors based on
the detection of FGFR3 and TP53 mutations. J Urol 2006; 176: 2686–2689.
15. Dodurga Y, Tataroglu C, Kesen Z, Satiroglu-Tufan NL. Incidence of fibroblast
growth factor receptor 3 gene (FGFR3) A248C, S249C, G372C, and T375C
mutations in bladder cancer. Genet Mol Res 2011; 10: 86–95.
16. Neuzillet Y, van Rhijn BW, Prigoda NL et al. FGFR3 mutations, but not FGFR3
expression and FGFR3 copy-number variations, are associated with favourable
non-muscle invasive bladder cancer. Virchows Arch 2014; 465: 207–213.
17. van Rhijn BW, Vis AN, van der Kwast TH et al. Molecular grading of urothelial cell
carcinoma with fibroblast growth factor receptor 3 and MIB-1 is superior to
pathologic grade for the prediction of clinical outcome. J Clin Oncol 2003; 21:
1912–1921.
18. Jebar AH, Hurst CD, Tomlinson DC, Johnston C, Taylor CF, Knowles MA. FGFR3
and Ras gene mutations are mutually exclusive genetic events in urothelial cell
carcinoma. Oncogene 2005; 24: 5218–5225.
19. Castillo-Martin M, Collazo Lorduy A, Gladoun N, Hyun G, Cordon-Cardo C.
H-RAS mutation is a key molecular feature of pediatric urothelial bladder cancer. A
detailed report of three cases. J Pediatr Urol 2016; 12: 91.e1–7.
20. Robertson AG, Kim J, Al-Ahmadie H et al. Comprehensive Molecular
Characterization of Muscle-Invasive Bladder Cancer. Cell 2017; 171: 540–556.e25.
21. McDaniel AS, Zhai Y, Cho KR et al. HRAS mutations are frequent in inverted
urothelial neoplasms. Hum Pathol 2014; 45: 1957–1965.
22. Isharwal S, Hu W, Sarungbam J et al. Genomic landscape of inverted urothelial
papilloma and urothelial papilloma of the bladder. J Pathol 2019; 248: 260–265.
23. Sjödahl G, Lauss M, Lövgren K et al. A molecular taxonomy for urothelial
carcinoma.Clin Cancer Res 2012; 18: 3377–3386.
24. Choi W, Porten S, Kim S et al. Identification of distinct basal and luminal subtypes
of muscle-invasive bladder cancer with different sensitivities to frontline
chemotherapy. Cancer Cell 2014; 25: 152–165.
25. Cancer Genome Atlas Research Network. Comprehensive molecular
characterization of urothelial bladder carcinoma. Nature 2014; 507: 315–322.
26. Damrauer JS, Hoadley KA, Chism DD et al. Intrinsic subtypes of high-grade
bladder cancer reflect the hallmarks of breast cancer biology. Proc Natl Acad Sci U
S A 2014; 111: 3110–3115.
27. Perou CM, Sørlie T, Eisen MB et al. Molecular portraits of human breast tumours.
Nature 2000; 406: 747–752.
28. Sorlie T, Tibshirani R, Parker J et al. Repeated observation of breast tumor subtypes
in independent gene expression data sets. Proc Natl Acad Sci U S A 2003; 100:
8418–23.
29. Allred C, Miller K, Viale G, Brogi E, Isola J. Molecular testing for estrogen
receptor, progesterone receptor, and HER2. In: Lakhani SR, Ellis IO, Schnitt SJ,Tan
PH, van de Vijver MJ, editors. WHO classification of tumours of the breast. 4th ed.
Lyon, France: IARC, 2012; 22–23.
30. National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in
Oncology: Breast Cancer (Version 3.2018).
31. Lerner SP, McConkey DJ, Hoadley KA et al. Bladder Cancer Molecular Taxonomy:
Summary from a Consensus Meeting. Bladder Cancer 2016; 2: 37–47.
32. Kamoun A, de Reyniès A, Allory Y et al. The consensus molecular classification of
muscle-invasive bladder cancer. BioRxiv 2018 Dec 10. doi:
https://doi.org/10.1101/488460.
33. Dadhania V, Zhang M, Zhang L et al. Meta-analysis of the luminal and basal
subtypes of bladder cancer and the identification of signature immunohistochemical
markers for clinical use. EBioMedicine. 2016; 12: 105–117.
34. Miyamoto H, Izumi K, Yao JL et al. GATA binding protein 3 is down-regulated in
bladder cancer yet strong expression is an independent predictor of poor prognosis
in invasive tumor. Hum Pathol 2012; 43: 2033–40.
35. Mohammed KH, Siddiqui MT, Cohen C. GATA3 immunohistochemical expression
in invasive urothelial carcinoma. Urol Oncol. 2016; 34: 432.e9–432.e13.