The Role of Cyclooxygenase 2 Functional Polymorphisms in Renal Cell Carcinoma
Wen-Shin Chang
1,2,*, Cheng-Hsi Liao
3,*, Chia-En Miao
2,*, Hsi-Chin Wu
4, Lin- Lin Hou
2, Chieh-Lun Hsiao
2, Hong-Xue Ji
2, Chia-Wen Tsai
2and Da-Tian Bau
1,21
Graduate Institute of Clinical Medical Science, China Medical University, Taichung, Taiwan;
2
Terry Fox Cancer Research Laboratory and
4Department of Urology, China Medical University Hospital, Taichung, Taiwan.
3
Department of Urology, Taichung Armed Forces General Hospital, Taichung, Taiwan.
* These Authors contributed equally to this work
Correspondence to: Da-Tian Bau, Terry Fox Cancer Research Lab, China Medical
University Hospital, 2 Yuh-Der Road, Taichung, 404 Taiwan, Tel: +886 422052121 Ext 7534, e-mail: [email protected]/[email protected]
Running title: Chang et al: COX-2 in Renal Cell Carcinoma
Abstract. Renal cell carcinoma (RCC) accounts for about 3% of all cancer-related mortalities all over the world and the risk factors for the development of RCC remain not elucidated. Mounting evidence showed that over-expression of cyclooxygenase 2 (COX-2) are commonly found in malignant tumors including RCC. However, the contribution of genotypic variations for COX-2 to RCC was never studied. We hypothesized that variant in COX-2 gene was associated with the susceptibility risk of RCC in Taiwan. In the hospital-based case–control study, 92 RCC patients and 580 age- and gender-matched cancer-free controls were recruited and the associations of COX-2 A-1195G, G-765C, T+8473C, intron 1, intron 5, and intron 6 polymorphisms with RCC risk in a Taiwanese population were examined. The results showed that compared with the wild-type GG genotype, the CG genotype at COX-2 G-765C had a significantly decreased risk of RCC [odds ratio (OR)=0.61, 95% confidence interval (CI) = 0.26–1.46, p=0.0082]. As for other polymorphic sites, no obvious association was found. There was also an obvious enhanced association of COX-2 G-765C genotype with RCC risk among those without family cancer history (p=0.0331). The evidence indicated that COX-2 G-765C genotype involved in the etiology of RCC and may serve as a novel genetic marker for susceptibility of RCC.
Key Words: COX-2; genotype; polymorphism; renal cell carcinoma;
Taiwan
Renal cell carcinoma (RCC) has a worldwide incidence with more than 270,000 new cases and 100,000 deaths annually (1). The incidence of RCC has kept its increasing step in the world (2). After Japan, Taiwan has the second-highest prevalence rate of end-stage renal disease in the world. Epidemiological investigations have showed that cigarette smoking, hypertension, obesity, occupational exposures, diet, and family history of cancer are associated with RCC (3-5). However, only few exposed individuals develop RCC during their lifetime, suggesting that genomic factor may be involved in the etiology of RCC. For urologists, RCC remains unpredictable of its behavior, and tumor stage and grade are not satisfying parameters for prognosis of RCC patients.
Cyclooxygenase-2 (COX-2) is an inducible enzyme for the
conversion of arachidonic acid to prostanoid, prostaglandin and
throboxane (6). Typically, COX-2 is often undetectable in normal tissues,
whereas overexpression of COX-2 has been observed in neoplastic cells
of canine (7) and human RCC (8-10). It is reported that overexpression of
COX-2 contributes to carcinogenesis via increasing cell proliferation,
suppressing apoptosis, enhancing invasiveness, and inducing chronic
activation of immune responses and angiogenesis (11, 12). In several
animal and clinical studies, COX-2 specific inhibitors have both
preventive and therapeutic effects as anticancer drugs for breast, bladder,
lung and pancreas cancers (13-16). However, the association of COX-2
genotypes with RCC has never been investigated.
2 gene may affect the quantity of COX-2 protein through altered self- regulated transcriptional activity or alternative splices resulting from polymorphic variations at promoter region or introns, respectively (17).
To clarify the hypothesis that the polymorphic variants at promoter or intron regions of COX-2 may be associated with the risk of RCC, we analyzed the genotypes for six COX-2 single nucleotide polymorphisms, including A-1195G (rs689466), G-765C (rs20417), T+8473C (rs5275), intron 1 (rs2745557), intron 5 (rs16825748), and intron 6 (rs2066826), in a Taiwanese population. To the best of our knowledge, this is the first study to evaluate the association between the COX-2 genotypes and RCC susceptibility in Taiwan.
Materials and methods
Study population. The hospital-based case-control study
recruited 92 RCC patients and 580 cancer-free controls frequency
matched by age and sex, and none of the subjects are relatives to each
other with any biological relationship. All the RCC patients were
diagnosed and histopathologically confirmed and without any prior
history of other cancers. All the age- and gender-matched cancer-free
controls were genetically unrelated to the RCC patients and had no
individual history of cancer. Extra exclusion criteria of the controls were
that if they had symptoms suggestive of RCC, such as hematuria. Each
patient donated 3-5 ml venous blood after providing a written informed
consent. The study was approved by the institutional review board of
China Medical University. The details of the characteristics for all the
participants are summarized and compared in Table I.
Genotyping protocol. The total genomic DNA of each
subject was extracted from the leucocytes of peripheral blood and stored as previously published (18-20). The polymerase chain reaction (PCR) cycling conditions were: one cycle at 94
°C for 5 min; 35 cycles of 94
°C for 30 sec, 55
°C for 30 sec, and 72
°C for 30 sec, and a final extension at 72
°C for 10 min. Pairs of PCR primer sequences and restriction enzyme for each DNA product of COX-2 genotyping work are all listed in Table II. The PCR products were cut by proper restriction enzymes and the reaction was incubated for 2 h at 37
°C. Then, 10 l of product was loaded into a 3% agarose gel for electrophoresis.
Statistical analyses. To ensure that the controls used were
representative of the general population and to exclude the possibility of
genotyping error, the deviation of the genotype frequencies of COX-2
single nucleotide polymorphisms in the control subjects from those
expected under the Hardy-Weinberg equilibrium was assessed using the
goodness-of-fit test. Pearson’s Chi-square test or Fisher’s exact test
compare the distribution of the COX-2 genotypes between cases and controls. The associations between the COX-2 polymorphisms and RCC risk were estimated by computing odds ratios (ORs) and their 95% confidence intervals (CIs) from unconditional logistic regression analysis with the adjustment for possible confounders. p < 0.05 was considered statistically significant, and all statistical tests were two-sided.
Results
Basic Characteristics compared between the case and control groups.
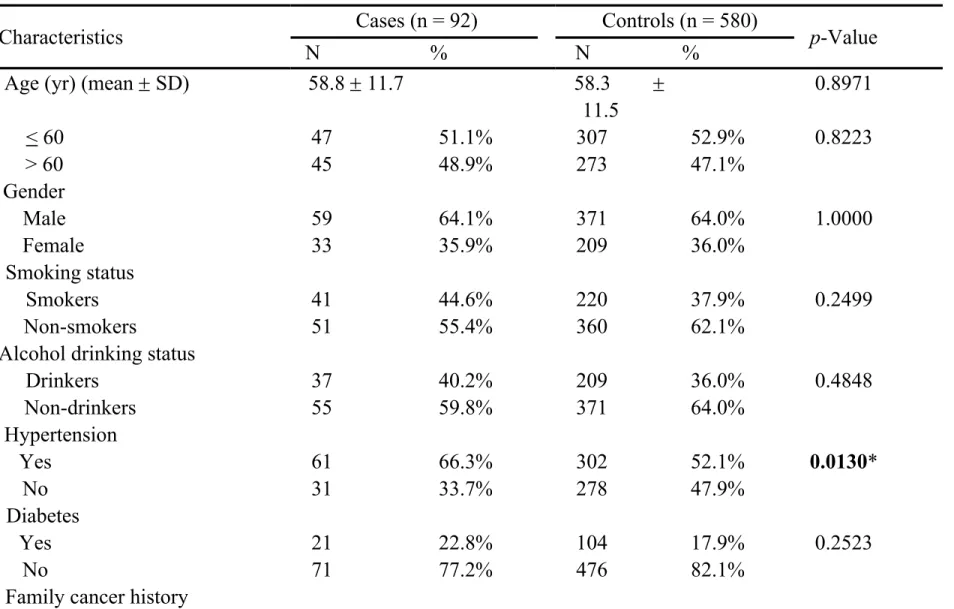
The frequency distributions of the characteristics for the control and case subjects are summarized in Table I. There were no difference between the case and control group on age, gender, smoking or alcohol drinking status, diabetes or family history of cancer (p>0.05). However, there were more subjects with hypertension (66.3%) among the RCC cases than the controls (52.1%), and the difference was statistically significant (p=0.0130).
Association of COX-2 genotypes and RCC risk. The genotypic
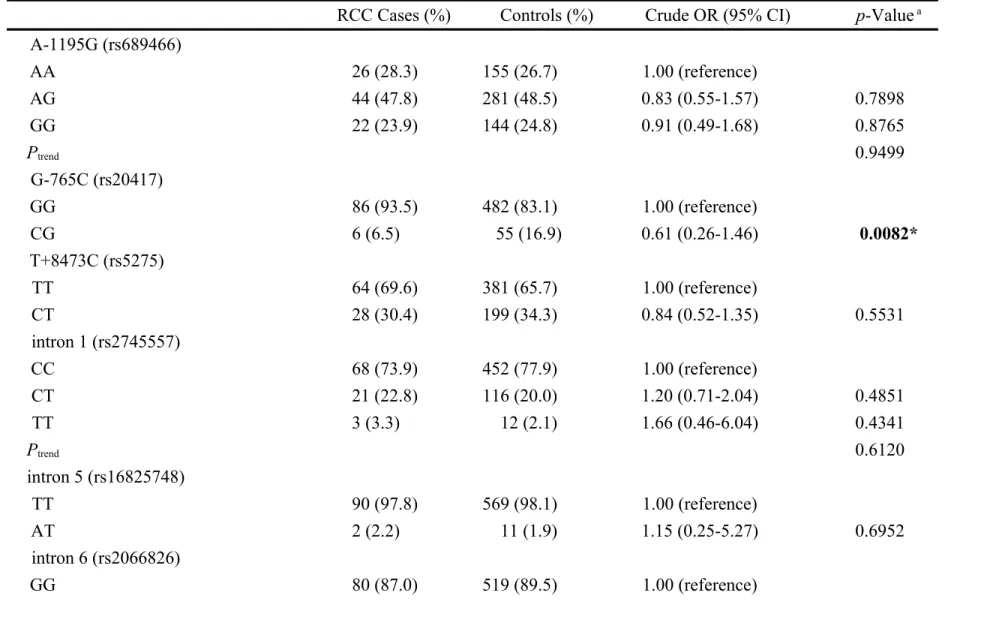
distributions of the COX-2 polymorphisms in the cases and controls are
presented and compared in Table III. The distributions of the genotypes of all the polymorphisms of COX-2 were not significant between the two groups (p>0.05) except that of G-765C (p=0.0082) (Table III). The OR for the people carrying CG genotype at COX-2 G-765C were 0.61 (95%
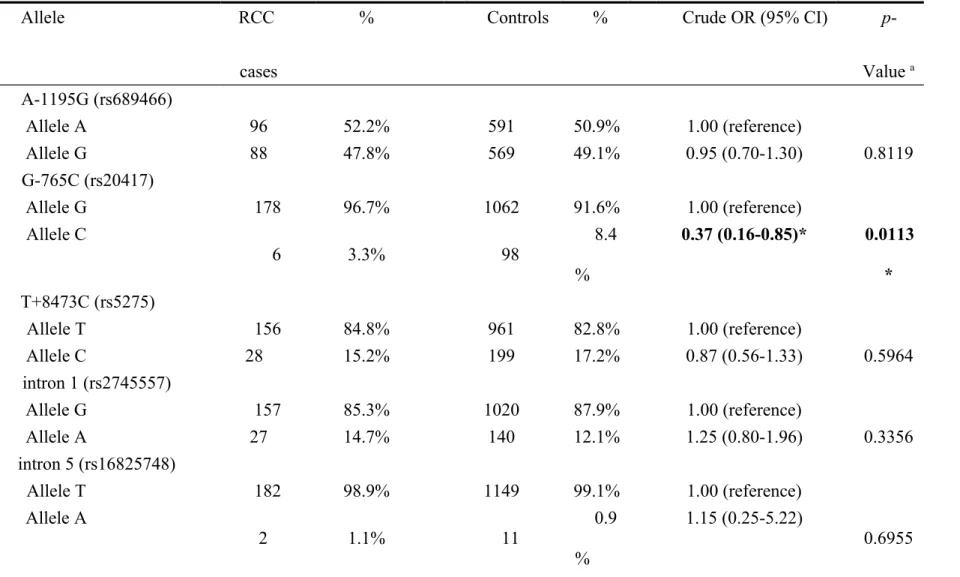
CI = 0.26-1.46) compared to those carrying GG wild-type genotype. The frequencies of the alleles for COX-2 polymorphisms in controls and RCC patients are shown in Table IV. Neither of the allele of the COX-2 of the polymorphisms were found to be associated with RCC (p>0.05) except that of G-765C (p=0.0113). The percentages of allele C were 3.3% and 8.4% among RCC patients and controls, and the OR for the people carrying C allele at COX-2 G-765C were 0.37 (95% CI = 0.16-0.85) compared to those carrying G wild-type allele. To sum up, these data indicated that individuals carrying variant C allele at promoter G-765C may have a lower risk of RCC.
Interaction of COX-2 G-765C genotype with personal characteristics.
We have stratified the controls and RCC cases according to their personal
characteristics and evaluated the interactions of COX-2 G-765C genotype
and these characteristics on the risk of RCC (Table V). As shown in
Table V, the association between COX-2 G-765C genotype and RCC risk did not vary by age, gender, smoking, alcohol drinking, hypertension status or diabetes stratification. However, the association appeared to be stronger in subgroups without family history (p=0.0331, OR=0.24, 95%CI=0.06-1.02).
Discussion
RCC is a highly heterogeneous tumor, and the cancer cells did not respond well to radiotherapy or chemotherapy, but partially to targeted therapies. Although it seems targeted therapies for advanced RCC is promising, the development of specific prognostic biomarkers for RCC is still lacking and in an urgently need (21-23). In the present study, the association of COX-2 genotypes and RCC risk was examined in Taiwan, where the prevalence of end-stage renal disease was second-highest all over the world after Japan. After performing the genotyping and analysis, we found that individuals carrying the CG genotype were of lower risk of RCC compared with those carrying GG genotype on COX-2 G-765C.
Regarding the other five polymorphic sites, A-1195G, T+8473C, intron 1,
intron 5, and intron 6, no association was found (Table III and IV). In
addition, we have also investigate the interactions of COX-2 G-765C genotype with personal characteristics on RCC risk, finding that the protective effects of COX-2 G-765C genotype was stronger among those without family cancer history (Table V). To the best of our knowledge, this is the first study of the role of COX-2 genotype in RCC in Taiwan.
The single nucleotide polymorphism COX-2 G-765C is a functional one at promoter region, determining the transcriptional activity of COX-2.
Many epidemiological studies have demonstrated the genotypes of COX- 2 G-765C to be associated with altered risk for human cancers such as
gastric cancer (24), colorectal cancer (25), prostate cancer (26, 27),
bladder cancer (28), and childhood leukemia (29). However, some other
studies showed that COX-2 G-765C genotype was not observed to be
associated with cancer risk (30, 31). The above evidence could be
interpreted to suggest the concept that immuno-regulating gene and
protein may play a role in the initiation of cancer development in
different carcinogenesis. However, the contribution of COX-2 genotypes
to RCC risk has never been studied. From the viewpoint of protein level,
there were several studies focused on the COX-2 expression levels in
RCC cells. In 2004, Chen et al have reported that COX-2 is overexpressed in OS-RC-2 RCC cell line and may play an important role in tumorigenesis. It is noticeable that regarding other RCC cell lines, SMKT-R4 and ACHN, the COX-2 was not overexpressed in the cells (32). Similar findings were reported by Miyata’s and Mungan’s groups (8, 10). In 2008, Dirim et al have reported that COX-2, PCNA and VEGF were observed primarily in the cytoplasm of RCC tumor cells and about half of 99 samples examined showed immunoreactivity for COX-2 (33).
In 2010, Kankuri-Tammilehto et al have reported that higher COX-2 expression may associate with longer metastasis-related survival (34).
The present study has some limitations to be improved
in the near future. First, our sample size is moderate,
which may restrict the reliability and feasibility of
stratification and interaction analyses. For instance, the
interaction findings such as stronger association of COX-2 G-
765C genotype with RCC risk in subgroups without family history
should be validated with enlarged population. Second,
more clinical and behavioral information, such as
occupational exposure, daily diet and physical exercise habits, metastasis and survival may strengthen our capacity of performing further risky factor analysis. Last, the transcriptional (mRNA) and translational (protein) studies, especially the comparison of those tissues from people with the CG and GG genotypes on COX-2 G-765C, should be further validated in both tumor tissues and normal adjacent tissues.
In conclusion, our present study indicate that the functional COX-2 G-765C polymorphism is associated with Taiwan RCC susceptibility, and this COX-2 polymorphic site may serve as both novel biomarker for RCC and potential target for anticancer drug development. Functional assays are warranted to reveal the role of COX-2 G-765C in RCC carcinogenesis.
Acknowledgements
This study was supported by research grants from Terry Fox Cancer
Research Foundation and Taiwan Ministry of Health and Welfare
Clinical Trial and Research Center of Excellence (MOHW103-TDU-B-
212-113002). The assistance from Tsai-Ping Ho in data collection
together with that from Hong-Xue Ji, Yi-Kai Huang, and Ding-Hao Sun
in genotyping was highly appreciated by the authors.
References
1 Remon J, Lianes P and Martinez S: Brain metastases from renal cell carcinoma. Should we change the current standard? Cancer Treat Rev 38: 249-257, 2012.
2 Salehipoor M, Khezri A, Behzad-Behbahani A, Geramizadeh B, Rahsaz M, Aghdaei M and Afrasiabi MA: Role of viruses in renal cell carcinoma. Saudi J Kidney Dis Transpl 23: 53-57, 2012.
3 Lipworth L, Tarone RE and McLaughlin JK: The epidemiology of renal cell carcinoma. J Urol 176: 2353-2358, 2006.
4 Murai M and Oya M: Renal cell carcinoma: etiology, incidence and epidemiology. Curr Opin Urol 14: 229-233, 2004.
5 Lindblad P: Epidemiology of renal cell carcinoma. Scand J Surg 93: 88-96, 2004.
6 DeWitt DL: Prostaglandin endoperoxide synthase: regulation of enzyme expression. Biochim Biophys Acta 1083: 121-134, 1991.
7 Khan KN, Stanfield KM, Trajkovic D and Knapp DW: Expression of cyclooxygenase-2 in canine renal cell carcinoma. Vet Pathol 38:
116-119, 2001.
8 Mungan MU, Gurel D, Canda AE, Tuna B, Yorukoglu K and
kidney, renal intraepithelial neoplasia, and renal cell carcinoma.
Eur Urol 50: 92-97; discussion 97, 2006.
9 Ristimaki A, Nieminen O, Saukkonen K, Hotakainen K, Nordling S and Haglund C: Expression of cyclooxygenase-2 in human transitional cell carcinoma of the urinary bladder. Am J Pathol 158:
849-853, 2001.
10 Miyata Y, Koga S, Kanda S, Nishikido M, Hayashi T and Kanetake H: Expression of cyclooxygenase-2 in renal cell carcinoma: correlation with tumor cell proliferation, apoptosis, angiogenesis, expression of matrix metalloproteinase-2, and survival. Clin Cancer Res 9: 1741-1749, 2003.
11 O'Byrne KJ and Dalgleish AG: Chronic immune activation and inflammation as the cause of malignancy. Br J Cancer 85: 473-483, 2001.
12 Kanaoka S, Takai T and Yoshida K: Cyclooxygenase-2 and tumor biology. Adv Clin Chem 43: 59-78, 2007.
13 Davies G, Salter J, Hills M, Martin LA, Sacks N and Dowsett M:
Correlation between cyclooxygenase-2 expression and
angiogenesis in human breast cancer. Clin Cancer Res 9: 2651-
2656, 2003.
14 Levitt RJ and Pollak M: Insulin-like growth factor-I antagonizes the antiproliferative effects of cyclooxygenase-2 inhibitors on BxPC-3 pancreatic cancer cells. Cancer Res 62: 7372-7376, 2002.
15 Mizutani Y, Kamoi K, Ukimura O, Kawauchi A and Miki T:
Synergistic cytotoxicity and apoptosis of JTE-522, a selective cyclooxygenase-2 inhibitor, and 5-fluorouracil against bladder cancer. J Urol 168: 2650-2654, 2002.
16 Sanchez-Alcazar JA, Bradbury DA, Pang L and Knox AJ:
Cyclooxygenase (COX) inhibitors induce apoptosis in non-small cell lung cancer through cyclooxygenase independent pathways.
Lung Cancer 40: 33-44, 2003.
17 Szczeklik W, Sanak M and Szczeklik A: Functional effects and gender association of COX-2 gene polymorphism G-765C in bronchial asthma. J Allergy Clin Immunol 114: 248-253, 2004.
18 Chang WS, Ke HL, Tsai CW, Lien CS, Liao WL, Lin HH, Lee
MH, Wu HC, Chang CH, Chen CC, Lee HZ and Bau DT: The role
of XRCC6 T-991C functional polymorphism in renal cell
carcinoma. Anticancer Res 32: 3855-3860, 2012.
19 Chang CH, Chiu CF, Liang SY, Wu HC, Chang CL, Tsai CW, Wang HC, Lee HZ and Bau DT: Significant association of Ku80 single nucleotide polymorphisms with bladder cancer susceptibility in Taiwan. Anticancer Res 29: 1275-1279, 2009.
20 Wang HC, Liu CS, Chiu CF, Chiang SY, Wang CH, Wang RF, Lin CC, Tsai RY and Bau DT: Significant association of DNA repair gene Ku80 genotypes with breast cancer susceptibility in Taiwan.
Anticancer Res 29: 5251-5254, 2009.
21 Angevin E, Lopez-Martin JA, Lin CC, Gschwend JE, Harzstark A, Castellano D, Soria JC, Sen P, Chang J, Shi M, Kay A and Escudier B: Phase I study of dovitinib (TKI258), an oral FGFR, VEGFR, and PDGFR inhibitor, in advanced or metastatic renal cell carcinoma. Clin Cancer Res 19: 1257-1268, 2013.
22 Figlin RA, Kaufmann I and Brechbiel J: Targeting PI3K and mTORC2 in metastatic renal cell carcinoma: new strategies for overcoming resistance to VEGFR and mTORC1 inhibitors. Int J Cancer 133: 788-796, 2013.
23 Motzer RJ, Escudier B, Bukowski R, Rini BI, Hutson TE, Barrios
CH, Lin X, Fly K, Matczak E and Gore ME: Prognostic factors for
survival in 1059 patients treated with sunitinib for metastatic renal cell carcinoma. Br J Cancer 108: 2470-2477, 2013.
24 Zhang XM, Zhong R, Liu L, Wang Y, Yuan JX, Wang P, Sun C, Zhang Z, Song WG and Miao XP: Smoking and COX-2 functional polymorphisms interact to increase the risk of gastric cardia adenocarcinoma in Chinese population. PLoS One 6: e21894, 2011.
25 Andersen V, Ostergaard M, Christensen J, Overvad K, Tjonneland A and Vogel U: Polymorphisms in the xenobiotic transporter Multidrug Resistance 1 (MDR1) and interaction with meat intake in relation to risk of colorectal cancer in a Danish prospective case- cohort study. BMC Cancer 9: 407, 2009.
26 Balistreri CR, Caruso C, Carruba G, Miceli V, Campisi I, Listi F, Lio D, Colonna-Romano G and Candore G: A pilot study on prostate cancer risk and pro-inflammatory genotypes:
pathophysiology and therapeutic implications. Curr Pharm Des 16:
718-724, 2010.
27 Wu HC, Chang CH, Ke HL, Chang WS, Cheng HN, Lin HH, Wu
CY, Tsai CW, Tsai RY, Lo WC and Bau DT: Association of
cyclooxygenase 2 polymorphic genotypes with prostate cancer in taiwan. Anticancer Res 31: 221-225, 2011.
28 Chang WS, Tsai CW, Ji HX, Wu HC, Chang YT, Lien CS, Liao WL, Shen WC, Tsai CH and Bau DT: Associations of cyclooxygenase 2 polymorphic genotypes with bladder cancer risk in Taiwan. Anticancer Res 33: 5401-5405, 2013.
29 Wang CH, Wu KH, Yang YL, Peng CT, Wang RF, Tsai CW, Tsai RY, Lin DT, Tsai FJ and Bau DT: Association study of cyclooxygenase 2 single nucleotide polymorphisms and childhood acute lymphoblastic leukemia in Taiwan. Anticancer Res 30: 3649- 3653, 2010.
30 Liu CJ, Hsia TC, Wang RF, Tsai CW, Chu CC, Hang LW, Wang CH, Lee HZ, Tsai RY and Bau DT: Interaction of cyclooxygenase 2 genotype and smoking habit in Taiwanese lung cancer patients.
Anticancer Res 30: 1195-1199, 2010.
31 Chang WS, Yang MD, Tsai CW, Cheng LH, Jeng LB, Lo WC, Lin
CH, Huang CY and Bau DT: Association of cyclooxygenase 2
single-nucleotide polymorphisms and hepatocellular carcinoma in
Taiwan. Chin J Physiol 55: 1-7, 2012.
32 Chen Q, Shinohara N, Abe T, Watanabe T, Nonomura K and Koyanagi T: Significance of COX-2 expression in human renal cell carcinoma cell lines. Int J Cancer 108: 825-832, 2004.
33 Dirim A, Haberal AN, Goren MR, Tekin MI, Peskircioglu L, Demirhan B and Ozkardes H: VEGF, COX-2, and PCNA expression in renal cell carcinoma subtypes and their prognostic value. Int Urol Nephrol 40: 861-868, 2008.
34 Kankuri-Tammilehto MK, Soderstrom KO, Pelliniemi TT, Vahlberg T, Pyrhonen SO and Salminen EK: Prognostic evaluation of COX-2 expression in renal cell carcinoma. Anticancer Res 30:
3023-3030, 2010.
Table I. Distributions of the frequencies of selected characteristics among the RCC cases and healthy controls
Characteristics Cases (n = 92) Controls (n = 580)
p-Value
N % N %
Age (yr) (mean SD) 58.8 11.7 58.3
11.5
0.8971
< 60 47 51.1% 307 52.9% 0.8223
> 60 45 48.9% 273 47.1%
Gender
Male 59 64.1% 371 64.0% 1.0000
Female 33 35.9% 209 36.0%
Smoking status
Smokers 41 44.6% 220 37.9% 0.2499
Non-smokers 51 55.4% 360 62.1%
Alcohol drinking status
Drinkers 37 40.2% 209 36.0% 0.4848
Non-drinkers 55 59.8% 371 64.0%
Hypertension
Yes 61 66.3% 302 52.1% 0.0130*
No 31 33.7% 278 47.9%
Diabetes
Yes 21 22.8% 104 17.9% 0.2523
No 71 77.2% 476 82.1%
Yes 6 6.5% 17 2.9% 0.1125
No 86 93.5% 563 97.1%
Table II. Primer sequences and restriction fragment length polymorphism (RFLP) conditions for COX-2 genotyping and analysis.
Polymorp hism
Primers sequences (5’ to 3’) Restriction enzyme Polymorphic type DNA fragment size (bp)
A-1195G (rs689466)
F: CCCTGAGCACTACCCATGAT R: GCCCTTCATAGGAGATACTGG
Hha I A
G
273 220 + 53 G-765C
(rs20417)
F: TATTATGAGGAGAATTTACCTTTCGC R: GCTAAGTTGCTTTCAACAGAAGAAT
PvuⅡ C
G
100 74 + 26 T+8473C
(rs5275)
F: GTTTGAAATTTTAAAGTACTTTTGAT R: TTTCAAATTATTGTTTCATTGC
Bcl I T
C
147 124 + 23 intron 1
(rs2745557 )
F: GAGGTGAGAGTGTCTCAGAT R: CTCTCGGTTAGCGACCAATT
Taq I C
T
439 353 + 76
intron 5 (rs1682574 8)
F: GCGGCATAATCATGGTACAA R: CAGCACTTCACGCATCAGTT
BsrG I T
A
417 314 + 103
intron 6 (rs2066826
)
F: ACTCTGGCTAGACAGCGTAA R: GCCAGATTGTGGCATACATC
Aci I A
G
327
233 + 94
F and R indicate forward and reverse primers, respectively.
Table III. Distributions of COX-2 genotypic frequencies among the RCC cases and controls
RCC Cases (%) Controls (%) Crude OR (95% CI) p-Value
aA-1195G (rs689466)
AA 26 (28.3) 155 (26.7) 1.00 (reference)
AG 44 (47.8) 281 (48.5) 0.83 (0.55-1.57) 0.7898
GG 22 (23.9) 144 (24.8) 0.91 (0.49-1.68) 0.8765
P
trend0.9499
G-765C (rs20417)
GG 86 (93.5) 482 (83.1) 1.00 (reference)
CG 6 (6.5) 55 (16.9) 0.61 (0.26-1.46) 0.0082*
T+8473C (rs5275)
TT 64 (69.6) 381 (65.7) 1.00 (reference)
CT 28 (30.4) 199 (34.3) 0.84 (0.52-1.35) 0.5531
intron 1 (rs2745557)
CC 68 (73.9) 452 (77.9) 1.00 (reference)
CT 21 (22.8) 116 (20.0) 1.20 (0.71-2.04) 0.4851
TT 3 (3.3) 12 (2.1) 1.66 (0.46-6.04) 0.4341
P
trend0.6120
intron 5 (rs16825748)
TT 90 (97.8) 569 (98.1) 1.00 (reference)
AT 2 (2.2) 11 (1.9) 1.15 (0.25-5.27) 0.6952
intron 6 (rs2066826)
AG 10 (10.9) 51 (8.8) 1.27 (0.62-2.61) 0.5556
AA 2 (2.1) 10 (1.7) 1.30 (0.28-6.03) 0.6687
P
trend0.7695
a
the significant p-Value is bolded and marked with a star;
OR: odds ratio; CI: confidence interval
Table IV. Distributions of COX-2 allelic frequencies among the RCC cases and controls
Allele RCC
cases
% Controls % Crude OR (95% CI) p-
Value
aA-1195G (rs689466)
Allele A 96 52.2% 591 50.9% 1.00 (reference)
Allele G 88 47.8% 569 49.1% 0.95 (0.70-1.30) 0.8119
G-765C (rs20417)
Allele G 178 96.7% 1062 91.6% 1.00 (reference)
Allele C
6 3.3% 98 8.4
%
0.37 (0.16-0.85)* 0.0113
* T+8473C (rs5275)
Allele T 156 84.8% 961 82.8% 1.00 (reference)
Allele C 28 15.2% 199 17.2% 0.87 (0.56-1.33) 0.5964
intron 1 (rs2745557)
Allele G 157 85.3% 1020 87.9% 1.00 (reference)
Allele A 27 14.7% 140 12.1% 1.25 (0.80-1.96) 0.3356
intron 5 (rs16825748)
Allele T 182 98.9% 1149 99.1% 1.00 (reference)
Allele A
2 1.1% 11 0.9 1.15 (0.25-5.22)
0.6955
Allele G 170 92.4% 1089 93.9% 1.00 (reference) Allele A
14 7.6% 71
6.1
%
1.26 (0.70-2.29)
0.4171
a
the significant p-Value and odds ratio are bolded and marked with a star
Table V. Stratification analysis between COX-2 G-765C (rs20417) polymorphism and RCC risk among cases and controls
COX-2 G-765C (rs20417) Genotypes
GG CG
Variables Cases/controls n % n % p-Value OR (95%CI)
Age
< 60 47/307 44/274 93.6/89.2 3/33 6.3/10.7 0.4468 0.57 (0.17-1.93)
> 60 45/273 42/251 93.3/91.9 3/22 6.7/8.1 1.0000 0.81 (0.23-2.84)
Gender
Male 59/371 55/333 93.2/89.8 4/38 6.8/10.2 0.4879 0.64 (0.22-1.86)
Female 33/209 31/192 93.9/91.9 2/17 6.1/8.1 1.0000 0.73 (0.16-3.31)
Smoking status
Smokers 41/220 36/183 87.8/83.1 5/37 12.2/16.8 0.6434 0.69 (0.25-1.87)
Non-smokers 51/360 50/342 98.0/95.0 1/18 2.0/5.0 0.4901 0.38 (0.05-2.91)
Alcohol status
Drinkers 37/209 33/173 89.2/82.8 4/36 10.8/17.2 0.4688 0.58 (0.19-1.75)
Non-drinkers 55/371 53/352 96.4/94.9 2/19 3.6/5.1 1.0000 0.70 (0.16-3.09)
Hypertension
Yes 61/302 58/269 95.1/89.1 3/33 4.9/10.9 0.2374 0.42 (0.13-1.42)
No 31/278 28/256 90.3/92.1 3/22 9.7/7.9 0.7267 1.25 (0.35-4.43)
Diabetes
Yes 21/104 18/90 85.7/86.5 3/14 14.3/13.5 0.1393 1.07 (0.28-4.12)
Family history
Yes 6/17 2/12 33.3/70.6 4/5 66.7/29.4 0.1616 4.80 (0.65-35.20)
No 86/563 84/513 97.7/91.1 2/50 2.3/8.9 0.0331* 0.24 (0.06-1.02)
a