P
Puurrppoossee.. Hematuria can be a sign of urinary tract disorders; therefore, it is necessary to arrange complete imaging studies to evaluate the entire urinary system. Our purpose is to elucidate the efficacy of retrograde pyelography (RP) for evaluating patients who present with hematuria.
M
Meetthhooddss.. From 2000 to 2002, a total of 634 patients underwent RP procedures because of hematuria. After excluding the 378 patients with urothelial carcinoma, stone disease, and urinary tract infection, 256 patients were included in this study. Patients were divided into two groups based on renal function: Group I: normal renal function (n = 156); Group II: poor renal function (Cr > 2.0) (n = 100). Patients in Group I were further classified into either group Ia: gross hematuria (n = 104) or Ib: microscopic hematuria (n = 52). Patients in Group II were further subdivided into either Group IIa uremia (n = 39) or IIb: chronic renal function impairment (n = 61).
R
Reessuullttss..Patients in Group II (50.0%) were more likely to have malignancy (OR = 4.2, 95% CI = 2.5 to 7.0, p < 0.001) than those in Group I (19.2%). In Group II, uremia (74.3%) was most closely associated with urothelial carcinoma (OR = 5.5, 95% CI = 2.3 to 13.1, p < 0.05). The rate of stone disease was significantly higher for Group II (OR = 2.0, 95% CI = 1.1 to 3.8, p < 0.005).
C
Coonncclluussiioonnss. Patients with impaired renal function are more likely to have urinary stone disease and urothelial cancer than those with normal renal function. Thus, RP is more valuable for evaluating hematuria in patients with impaired renal function than in those with normal renal function. Among the patients with impaired renal function, uremic patients are at highest risk of having urothelial cancer in Taiwan. Therefore, it is crucial to perform RP and cystoscopy for patients with impaired renal function, especially for those with uremia. ( Mid Taiwan J Med 2007;12:14-9 )
K
Keeyy wwoorrddss
hematuria, retrograde pyelography, renal function impairment, urothelial carcinoma
IINNTTRROODDUUCCTTIIOONN
Hematuria can arise from disease in any part of the urinary tract. Both gross and microscopic hematuria are likely to be indicative
of clinically significant disease, such as stone, infection or malignant tumors [1,2]. If a patient is at risk for malignancy, such as having a history of smoking [3], analgesic abuse [4], residing in a arseniasis-endemic area in Taiwan [5-8], and exposure to chemicals agents [9,10], a complete urologic evaluation including intravenous pyelography (IVP), cystoscopy or urine cytology
Received : 30 June 2006. Revised : 15 August 2006.
Accepted : 5 September 2006.
Address reprint requests to : Wen-Chi Chen, Department of Urology, China Medical University Hospital, 2 Yuh-Der Road, Taichung 404, Taiwan.
The Role of Retrograde Pyelography for Evaluation of Hematuria in Patients
with Normal and Impaired Renal Function
Wayne Young Liu, Hsi-Chin Wu, Chao-Hsiang Chang, Chin-Chong Yeh, Chieh- Lung Chou, Kuo-Liang Chen, Wen-Chi Chen
Department of Urology, China Medical University Hospital, Taichung, Taiwan.
is necessary. However, the initial imaging studies might not provide a definitive diagnosis.
Therefore, a second diagnostic procedure should be performed.
Retrograde pyelography (RP) has been used as an alternative imaging study in urology for many years, escepically for patients with contrast medium allergy, or unsatisfactory image of IVP in the initial diagnosis of hematuria. RP is always performed in association with cystoscopic examination for providing complete urinary tract study. It has been questioned whether RP is useful for all patients with hematuria or just for patients with renal funtion impairment. We performed this study to evaluate the role for this relatively invasive procedure for patients with impaired renal function.
M
MAATTEERRIIAALLSS AANNDD MMEETTHHOODDSS From 2000 to 2002, a total of 634 patients who underwent RP procedures because of hematuria (either microscopic or gross hematuria) in this hospital were retrospectively reviewed.
Patients with urothelial carcinoma, urolithiasis, urinary tract infection, or other urologic diseases were excluded from the study. A total of 256 patients with unknown causes of hematuria were enrolled in our study. The patients were divided into two groups according to their renal function:
Group I: normal renal function (n = 156); Group II: poor renal function (Cr > 2.0) (n = 100). The patients in Group I who had undergone IVP (intravenous pyelography) before RP were further classified into group Ia: gross hematuria (n = 104); Ib: microscopic hematuria (n = 52). The patients in Group II who had undergone RP with
cystoscopy instead of IVP because of poor renal function were subdivided into: IIa uremia (n = 39) and IIb: chronic renal function impairment (CRI) (n = 61). Abnormal RP findings were further evaluated by ureteroscopy and computed tomography (CT). Suspicious upper urinary tract tumors were analyzed by pathologic examination of ureteroscopic biopsy or surgical specimens.
RP findings between the two groups were analyzed by the chi-square test with odds ratio evaluation. All p values < 0.05 were considered statistically significant. Calculations were performed using commercial statistical software (SPSS®).
R
REESSUULLTTSS
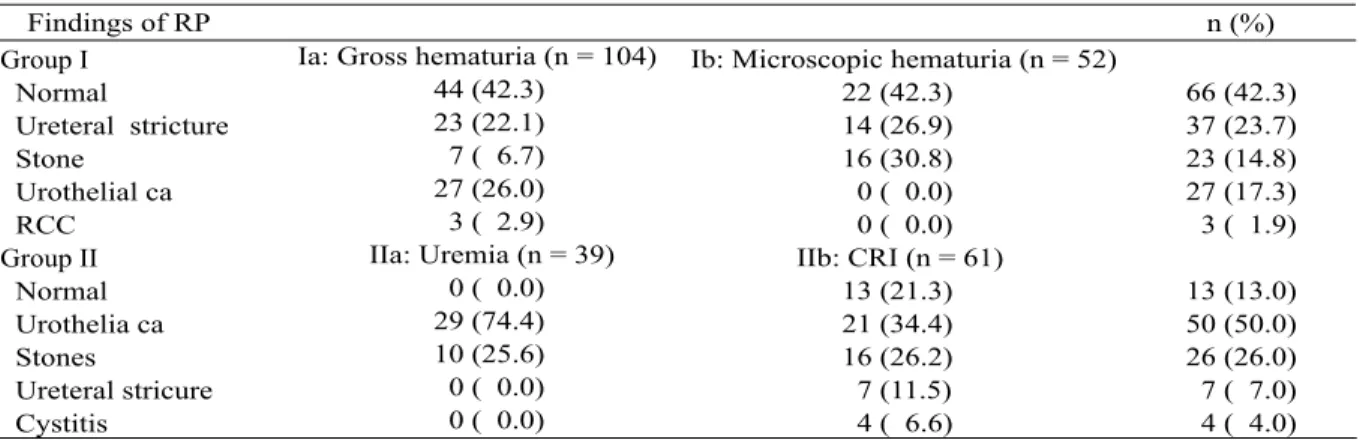
The characteristics of patients are listed in Table 1. In Group I, there were normal findings in 66 patients (42.3%), ureteral stricture in 37 patients (23.7%), urothelial carcinoma in 27 patients (17.3%), urinary stones in 23 patients (14.8%), and renal cell carcinoma (RCC) in 3 patients (1.9%) (Table 2). In Group Ia, there were normal findings in 44 patients (42.3%), ureteral stricture in 23 patients (22.1%), urothelial carcinoma in 27 patients (26.0%), stones in 7 patients (6.7%), and 3 RCC (2.9%). In Group Ib, there were normal findings in 22 patients (42.3%), ureteral stricture in 14 patients (26.9%), and stones in 16 patients (30.7%). All of the tumors were found in Group Ia, and included urothelial cancers (n = 27) and RCC (n = 3).
In Group II, 13 patients had normal findings (13.0%); 7 patients had ureteral stricture (7.0%); 50 patients had positive findings of urothelial cancer (50.0%); 26 patients had urinary stones (26.0%), and 4 had cystitis (4.0%)
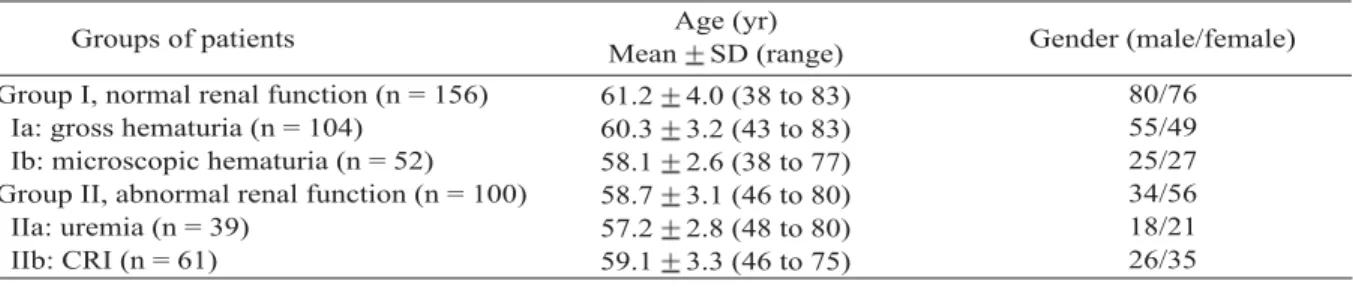
Table 1. Patient characteristics
CRI = chronic renal function impairment.
Group I, normal renal function (n = 156) Ia: gross hematuria (n = 104)
Ib: microscopic hematuria (n = 52) Group II, abnormal renal function (n = 100)
IIa: uremia (n = 39) IIb: CRI (n = 61)
61.2 4.0 (38 to 83) 60.3 3.2 (43 to 83) 58.1 2.6 (38 to 77) 58.7 3.1 (46 to 80) 57.2 2.8 (48 to 80) 59.1 3.3 (46 to 75)
Age (yr)
Mean SD (range) Gender (male/female) Groups of patients
80/76 55/49 25/27 34/56 18/21 26/35
(Table 2). In Group IIa, there were 29 patients with urothelial cancers (74.4%) and 10 patients with urinary stones (25.6%). In Group IIb, 13 patients had normal findings (21.3%); 7 had ureteral stricture (11.5%); 21 had urothelial cancers (34.4 %);16 had urinary stones (26.2%), and 4 had cystitis (6.6%).
There was a higher percentage of malignancy in Group II than in Group I, (chi- square test, p < 0.001). The odds ratio (OR) was 4.2 in Group II (95% CI = 2.5 to 7.0) (Table 3). In comparing the rates of malignancy between subgroups IIa and IIb, the OR for subgroup IIa was 5.5 (95% CI = 2.3 to 13.1). Patients in Group II had a significantly higher rate of stone disease than patients in Group I (OR = 2.0, 95% CI = 1.1 to 3.8, p < 0.05) (Table 3). There was no significant differnce in stone disease between subgroups IIa and IIb (p = 0.947). Patients with impaired renal function were more likely to have urinary stone disease and urothelial cancer than those with normal renal function.
D
DIISSCCUUSSSSIIOONN
The marked difference between gross and microscopic hematuria is that patients with gross hematuria are at higher risk for malignancy than those with microscopic hematuria [1-3]. For patients with impaired renal function, RP is helpful in diagnosing the cause of gross hematuria [12,13]. In Group I, RP showed that patients with gross hematuria were more likely to have malignancy (27 urothelial cancer, 3 RCC) compared with those with microscopic hematuria;
no malignancies were diagnosed in patients with microscopic hematuria (Table 1). Our study is compatible with other series in which gross hematuria was shown to be a symptom of urinary tract malignancy [13-16]. Contrary to gross hematuria, RP has little diagnostic value in the evaluation of microscopic hematuria.
The results of RP revealed that gross hematuria in patients with impaired renal function was more closely related to malignancy than that in patients with normal renal function. There was a higher incidence of tumor in Group II (50.0%)
Table 2. Results of the study by retrograde pyelography in patients in Group I and Group II
RCC = renal cell carcinoma. CRI = chronic renal function impairment.
Group I Normal
Ureteral stricture Stone
Urothelial ca RCC
Group II Normal Urothelia ca Stones
Ureteral stricure Cystitis
Ia: Gross hematuria (n = 104) 44 (42.3)
23 (22.1) 7 ( 6.7) 27 (26.0) 3 ( 2.9) IIa: Uremia (n = 39)
0 ( 0.0) 29 (74.4) 10 (25.6) 0 ( 0.0) 0 ( 0.0)
Ib: Microscopic hematuria (n = 52) 22 (42.3)
14 (26.9) 16 (30.8) 0 ( 0.0) 0 ( 0.0) IIb: CRI (n = 61)
13 (21.3) 21 (34.4) 16 (26.2) 7 (11.5) 4 ( 6.6)
n (%) Findings of RP
66 (42.3) 37 (23.7) 23 (14.8) 27 (17.3) 3 ( 1.9)
13 (13.0) 50 (50.0) 26 (26.0) 7 ( 7.0) 4 ( 4.0)
Table 3. Comparisons of the percentages of tumors and urinary stones between group I and II from RP studies (chi-square test)
*p < 0.05, p < 0.01.
I: normal renal function (n = 156 ) II: abnormal renal function (n = 100 )
IIa: uremia (n = 39) IIb: CRI (n = 61)
126 (80.8) 50 (50.0) 10 (25.7) 40 (65.6)
RP findings
30 (19.2) 50 (50.0) 29 (74.3) 21 (34.4) Non-tumors
n (%)
Tumors n (%)
133 (85.3) 74 (64.9) 29 (74.4) 45 (73.8)
RP findings
OR OR
23 (14.7) 26 (35.1) 10 (25.6) 16 (26.2) 1.0
4.2 5.5 1.0
1.0 2.0*
0.9 1.0 Non-stones
n (%)
Stones n (%) Groups of patients
than in Group I (19.2%), (OR = 4.2, p < 0.001) (Table 3). Furthermore, uremic patients with gross hematuria were more likely to have malignancy than any other patients. RP revealed 29 urothelial cancers (74.3%) in 39 uremic patients in comparison with 21 urothelial cancers (34.4%) in 61 patients with impaired renal function (OR = 5.5, p < 0.001) indicating that uremic patients with hematuria are at high risk for urothelial cancer.
It has been reported that patients with chronic renal failure have a high incidence of malignant tumor [17]. According to many reports, gross hematuria in uremic patients in Taiwan is associated with urothelial cancer [12-14,18,19].
Our study confirmed the above findings. We strongly recommend that uremic patients undergo complete urologic imaging study including RP and cystoscopy because urothelial cancer tends to be multifocal and has a high rate of recurrence [13-15,20]. In contrast to ureteroscopy, RP and cystoscpoy are less invasive and can be managed with regional urethral anesthesia, which is suitable for patients at high risk for anesthesia [11]. Furthermore, ureteroscopy can confirm the positive RP findings.
In addition to malignancy, hematuria can also be a sign of urolithiasis. Our study showed that urinary stones occur more frequently in patients with impaired renal function than in patients with normal renal function. RP showed that 26 (26.0%) in Group II had urolithiasis in comparison with 23 (14.8%) in Group I (OR = 2.0, p = 0.025). Stone formation in patients with renal failure may be due to metabolic factors such as high urinary oxalate and due to iatrogenic factors, namely vitamin D3 or calcium salt supplementation [21,22]. Therefore, RP is of diagnostic value for patients with impaired renal function whenever hematuria occurs. Once urinary stone has been confirmed, the following ureteroscopy can be arranged.
There was a high percentage of negative findings in Group I (42.3%), indicating that nearly half of the patients with normal renal function unnecessarily underwent the RP
procedure. It is important to improve the quality of IVP or, alternatively perform multi-detector CT urography (MDCTU) to detect urinary tract disease. To date, contrast-enhanced MDCTU performed with a combination of unenhanced, nephorgenic-phase, and excretory- phase can provide better visualization of urinary tract than IVP [23-26]. RP is a valuable diagnostic modality in patients with impaired renal function because more than half of them (61.0%) have urinary tract disease. All uremic patients with gross hematuria in our study had positive RP findings. Thus, RP is an essential and efficacious screening tool to evaluate upper urinary tract for patients with poor renal function.
Our study is limited because of selection bias; most of the patients were referred from local clinics or regional hospitals in central Taiwan.
Our RP findings do not clarify the characteristic of hematuria in Taiwan. Therefore, a large and national multi-center study should be arranged to evaluate the efficacy of RP, especially for uremic patients.
In conclusion, our study indicated that gross hematuria is a cardinal sign of urinary tract disorders. For patients with poor renal function, RP and cystoscopy play an important role because disease is more frequently seen in those patients than in patients with normal renal function.
Furthermore gross hematuria in uremic patients is more strongly related to urothelial cancer in Taiwan than in other countries. Therefore, it is crucial to perform RP and cystoscopy for patients with impaired renal function, especially for those with uremia.
R
REEFFEERREENNCCEESS
1. Grossfeld GD, Litwin MS, Wolf S, et al. Evalution of asymptomatic microscopic hematuria in Adults: The American urological association best practice policy-- part I: definition, detection, prevalence, and etiology.
Urology 2001;57:599-603.
2. Sutton JM. Evaluation of hematuria in adults. JAMA 1990;263:2475-80.
3. McLaughlin JK, Silverman DT, Hsing AW, et al.
Cigarette smoking and cancers of the renal pelvis and ureter. Can Res 1992;52:254-7.
4. McCredie M, Stewart JH, Carter JJ, et al. Phenacetin and papillary necrosis: indepandent risk factors for renal pelvis cancer. Kidney Int 1986;30:81-4.
5. Mariani AJ. The evaluation of adult hematuria: a clinical update. AUA Update Series 1998;17:186-91.
6. Chiou HY, Chiou ST, Hsu YH, et al. Incidence of transitional Cell carcinoma and arsenic in drinking water: a follow-up study of 8,102 residents in an arseniasis-endemic area in northeastern Taiwan. Am J Epidemiol 2001;153: 411-8 .
7. Chou YH, Huang CH. Unusual clinical presentation of upper urothelial carcinoma in Taiwan. Cancer 1999;
85:1342-4.
8. Chen CJ, Wang CJ. Ecological correlation between arsenic level in well water and age-adjusted mortality from malignant neoplasms. Cancer Res 1990;50:5470- 4.
9. Cartwright RA. Bladder cancer screening in the United Kingdom. J Occup Med 1990;32:878-80.
10. Hanke J, Krajewska B. Acetylation phenotypes and bladder cancer. J Occup Med 1990;32:917-8.
11. Chen GL, El-Gabry EA, Bagley DH. Surveillance of upper urinary tract transitional cell carcinoma: the role of ureteroscopy, retrograde pyelography, cytology and urinalysis. J Urol 2000;164:1901-4.
12. Chen KS, Lai MK, Huang CC, et al. Urologic cancers in uremic patients. Am J Kidney Dis 1995;25:694-70.
13. Wu CF, Shee JJ, Ho DR, et al. Different treatment strategies for end stage renal disease in patients with transitional cell carcinoma. J Urol 2004;171:126-9.
14. Wu CF, Chang PL, Chen CS, et al. The outcome of patients on dialysis with upper urinary tract transitional cell carcinoma. J Urol 2006;176:477-81.
15. Hisataki T, Miyao N, Masumori N, et al. Risk factors for the development of bladder cancer after upper tract urothelial cancer. Urology 2000;655:63-7.
16. Messing EM, Young TB, Hunt VB, et al. Home screening for hematuria: results of a multiclinic study.
J Urol 1992;148:289-92.
17. Cengiz K. Increased incidence of neoplasia in chronic renal failure (20-year experience). Int Urol Nephrol 2002;33:121-6.
18. Jiann BP, Lee YH, Huang JK. Uremia with concomitant urothelial cancer. Br J Urol 1993;72:458- 61.
19. Ou JH, Pan CC, Lin SN. Transitional cell carcinoma in dialysis patient. Euro Urol 2000;37:90-4.
20. Kang CH, Yu TJ, Hsieh HH, et al. The development of bladder tumors and contralateral upper urinary tract tumors after primary transitional cell carcinoma of the upper urinary tract. Cancer 2003;98:1620-6.
21. Daudon M, Lacour B, Jungers P, et al. Urolithiasis in patients with end stage renal failure. J Urol 1992;
147:977-80.
22. Koga N, Nomura G, Yamagata Y, et al. Ureteric pain in patients with chronic renal failure on hemodialysis.
Nephron 1982;31:55-8.
23. Joffe SA, Servaes S, Okon S, et al. Multi-detector row CT urography in the evaluation of hematuria.
RadioGraphics 2003;23:1441-56.
24. Niall O, Russell J, MacGregor R, et al. A comparison of noncontrast computerized tomography with excretory urography in the assessment of acute flank pain. J Urol 1999;161:534-7.
25. Heneghan JP, Kim DH, Leder RA, et al. Compression CT urography: a comparison with IVU in the opacification of the collecting system and ureters. J Comput Assist Tomogr 2001;25:343-47.
26. Wang JH, Lin WC, Wei CJ, et al. Diagnostic value of unenhanced computerized tomography in the evaluation of acute renal colic. Kaohsiung J Med Sci 2003;19:503-9.
404 2
2006 6 30 2006 8 15
2006 9 5
2000 2002 634
378 256
156
100 Ia 104 Ib 52
IIa 39 IIb 61
(OR = 4.2 95% CI = 2.5 to
7.0 p < 0.001) (OR =
5.5 95% CI = 2.3 to 13.1 p < 0.05)
(OR = 2.0 95% CI = 1.1 to 3.8 p < 0.005)
2007;12:14-9