Syncope as First Presentation in an Old Man with Follicle Stimulating Hormone-secreting
Non-functioning Pituitary Macroadenoma:
A Case Report and Review of the Literature
Bao-Mei Wang
2, Vinchi Wang
3,4, Chin-Yao Lin
4,5, Sio-Long Chang
6, and Wen-Ya Ma
1,41
Division of Endocrinology,
2Department of Internal Medicine,
3
Neurological Center, Cardinal Tien Hospital, Xindian;
4
School of Medicine, Fu-Jen Catholic University;
5
Department of Pathology,
6Department of Neurosurgery, Cardinal Tien Hospital Yung-Ho Branch,
Yung-Ho District, New Taipei City, Taiwan
Abstract
Non-functioning pituitary adenoma (NFPA) is the most prevalent type of pituitary tumor. However, it could be a diagnostic challenge due to the lack of clinical signs and symptoms. The diagnosis has mainly made by incident and frequently been delayed until macroadenoma causing mass effect or the appearance of panhypopituitarism. Most of NFPA are gonadotrophinomas. Herein we reported a pituitary macroadenoma in an 84-year-old man with unusual presentation of syncope without focal neurological signs or symptoms of pituitary hormones excess. Hyponatremia, however, was a significant clue of panhypopituitarism even when the clinical appearance could be missed by the old age. Visual field examination revealed bitemporal hemianopia. Computed tomography and magnetic resonance imaging of brain discovered a huge tumor of 3.3x2.0x1.9 cm in the pituitary gland with suprasellar extension. Hormone profile showed reduced cortisol, free T4, and testosterone concentrations, compatible with panhypopituitarism. However, serum FSH level was increased unexpectedly while the LH level was normal, suggesting FSH-secreting NFPA. Endoscopic transnasal-transsphenoidal adenomectomy was performed for tumor removal. Microscopically, the tumor cells revealed immunoreactivity to FSH staining. Focal area revealed extensive hemorrhage without necrosis, suggesting pituitary apoplexy. After the surgery, he was given glucocorticoids and thyroxine for replacement and was followed regularly under stable condition. (J Intern Med Taiwan 2012; 23: 367-373)
Key Words: Nonfunctioning pituitary adenoma, Gonadotrophinoma, Syncope, Transnasal- transsphenoidal surgery
Reprint requests and Correspondence:Dr. Wen-Ya Ma
Address:Department of Internal Medicine, Cardinal Tien Hospital, No. 362, Zhongzheng Rd. Xindian District, New Taipei City, 231 Taiwan, R.O.C.
Introduction
Non-functioning pituitary adenoma (NFPA) is the most common type which accounts for 15-45%
of pituitary tumor
1,2. However, the true prevalence is difficult to estimate since the discovery of pituitary incidentaloma (PI) is increasing with the wide use of diagnostic imaging techniques. NFPA could be diagnostic challenging due to the lack of clinical signs and symptoms of hormone excess.
Large NFPA can be diagnosed from appearance of panhypopituitarism caused by its mass effect on surrounding tissue. Herein we reported a case of pituitary macroadenoma with unusual presentation of syncope. The diagnostic procedure and clinical course of the patient were described.
Case Presentation
An 84-year-old man was brought to our emergency department for syncope. He had history of coronary artery disease and had undergone percutaneous coronary intervention without stenting. He also had spondylosis of thoracolumbar spines but his daily activity was unaffected.
Sudden onset of syncope occurred when he was at home. His family did not find convulsions or focal weakness of limbs during the episode. The patient gained his consciousness spontaneously on arrival.
He reported a blurred vision, especially on the left eye. He also felt light-headed prior to the episode.
Otherwise, no chest pain, dyspnea, vertigo, tinnitus, visual loss, urinary or bowel incontinence was mentioned. He was an ex-smoker and he denied alcohol consumption. His family history was irrelevant.
At presentation, his consciousness was clear and oriented with an arterial blood pressure of 128/54 mmHg and a heart rate of 70 beats/min. He did not have fever and had no signs of respiratory distress. Physical examination and a comprehensive neurological examination were normal except a
possibly defect in lateral visual fields at both sides.
His eye movements were free and full.Eye brows were slightly thinner. His neck was supple without jugular vein engorgement or carotid bruits. Heart sounds were regular and absence murmurs. The lungs were clear in both sides.The pigmentation of areola was diminished.The abdomen was soft and non-tender. There were sparse axillary and pubic hairs. The extremities showed no edema or clubbing. The peripheral pulsations were normal.
Muscle powers and the deep tendon reflexes of all four limbs were intact and symmetrical. No Romberg signs or ataxic gaits were observed.
Complete blood count and serum chemistry tests were unremarkable except hyponatremia. The data were summarized in Table 1. Urine analysis was within normal limits.Plain films on chest and KUB showed nonspecific findings including tortuosity of the thoracic aorta with mild cardiomegaly,
Table 1. Laboratory test results and hormone profiles Result Reference range Complete blood counts
White blood cells ,x109/L 7.11 4-10x109
Hemoglobin, g/L 11.1 13.5-17.5
Hematocrit, % 33.1 41-53
Platelet,x109/L 208 150-450 109
Biochemistry
BUN, mg/dL 21 7-18
Creatinine, mg/dL 1.39 0.8-1.3
Sodium,mmol/L 131 136-145
Potassium, mmol/L 3.76 3.5-5.1
Glucose, mg/dL 83 70-99
Hormone profiles
Cortisol (8 A.M), μg/dL 3.84 5-23
ACTH ,pg/mL 12.3 0-46
TSH, µIU/mL 2.658 0.35-5.5
Free T4, ng/dL 0.72 0.89-1.76
Growth hormone, ng/mL 0.101 0.003-0.97
Prolactin, µg/L 15.58 2.1-17.7
Total testosterone, ng/dL 191.89 241-827
FSH, mIU/mL 32 1-12
LH, mul/mL 6.11 1-12
reticulonodular infiltrates over both lungs with hypoinflation, widening of superior mediastinum and spondylosis of thoracolumbar spine with spur formation and residual fecal material.A 12-lead electrocardiogram at rest showed normal sinus rhythm. There was no evidence of orthostatic hypotension.
A 24 hour holter monitoring showed infrequent atrial premature complexes (APC) and frequent ventricular premature complexes (VPC). Supra- ventricular tachycardia (SVT) was found on one occasion and sinus bradycardia was on another.
Cardiac Doppler ultrasound revealed normal chamber size and systolic function of left ventricle with moderate aortic regurgitation, moderate tricuspid regurgitation, mild mitral regurgitation and mild pulmonary regurgitation.
Computed tomography (CT) of brain revealed a huge tumor mass of 3.3x2.0x1.9 cm over the pituitary gland with suprasellar extension (Figure 1). The lesion showed mildly contrast-enhancing, suggesting a pituitary adenoma. Calcified foci were noted over pineal gland, bilateral basal ganglia and choroid plexus. Magnetic resonance imaging
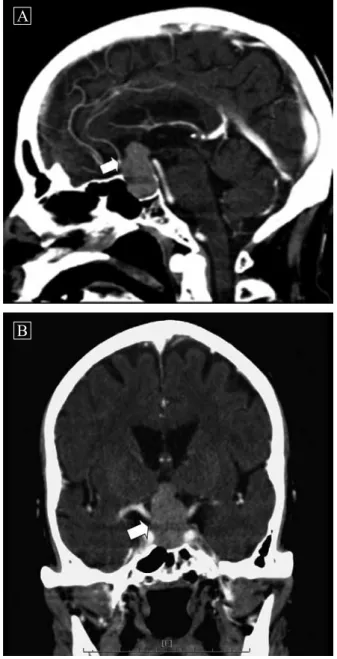
(MRI) of sella (T1-weighted images with contrast) showed a homogeneous enhanced and lobular mass of 3.5x1.8 cm in size located within the sella and suprasellar region (Figure 2). No evidence of parasellar tumor extension or mass effect to the ventricles and sulci were identified. T2-weighted images showed scattered tiny hyper-intense spots at the bilateral corona radiata and subcortical white matter, suggesting lacunar infarcts and subcortical
Figure 1. Axial view of computed tomography of brain revealed a huge tumor mass of 3.3x2.0x1.9 cm over the pituitary gland with suprasellar extension (white arrow).
Figure 2. Magnetic resonance imaging (MRI) of sella, T1-weighted image with contrast medium, showed a homogeneous enhanced and lobular mass of 3.5x1.8 cm in size located within the sella and suprasellar region (white arrow). (A, sagittal view; B coronal view).
B
A
arteriosclerotic encephalopathies (SAE). Visual filed examination showed bitemporal hemianopia.
The hormone profiles were summarized in table 1.The reduced morning cortisol, free thyroxine (Free T4) and total testosterone were compatible with panhypopituitarism resulted from tumor compression. However, serum FSH concentration was elevated while LH was not, suggesting possibly FSH-secreting adenoma.
Transnasal-transsphenoidal pituitary tumor removal was performed smoothly. Microscopically, the tumor cells appeared in diffuse pattern and focally papillary features. They possessed chromophobic cytoplasm with fine chromatic nuclei. Focal area revealed extensive hemorrhage without necrosis (Figure 3).These cells also revealed immunoreactivity to FSH staining (Figure 4). The diagnosis of FSH-secreting pituitary adenoma with pituitary apoplexy was made.
After the operation, the patient was given with oral glucocorticoids (prednisolone 5 mg in the morning and 2.5 mg in the evening) and thyroxine (100 μg once daily) for replacement of secondary hypocortisolism and secondary hypothyroidism, respectively. Serum FSH concentration 3 months after operation was 17.81 mIU/L. His condition was
stable and he was followed regularly at OPD.
Discussion
In the absence of symptoms and signs of hormone excess, early detection of NFPA is difficult unless incidentally found by imaging study.
Therefore, NFPA mainly presents as macroadenoma (>10mm in diameter) at diagnosis
3. Most common presentations of NFPA were headache and visual symptoms such as visual field defect or ocular paresis. Other manifestations include vomiting, mental disturbances, seizure and rarely, syncope
2,4.
NFPA may also present with pituitary insuffi- ciency, which is due to compression of the pituitary stalk or destruction of normal pituitary tissue by the tumor
3. Hypopituitarism may be suspected in the presence of clinical signs of target hormone deficiency. Hyponatremia can be associated with both hypocortisolism and hypothyroidism.
Hypogonadism is detected in up to 96% of patients with pituitary macroadenomas and is usually associated with inappropriately normal or decreased serum gonadotropin levels, indicating secondary (central) hypogonadism. Patients of reproductive age may present clinical hormonal symptoms such as amenorrhea, decreased libido or impotence
2. The etiology of hypogonadism in this setting may be multifactorial:
Figure 3. The tumor cells are arranged in diffuse and focally papillary patterns (white arrow), with prominent chromophobic cytoplasm, fine chromatin, indistinctive nucleoli and extensive hemorrhage (H). (Hematoxylin and Eosin stain, 200 X).
Figure 4. Photomicrograph showing immunoreactivity
for FSH in tumor cells (Immunohistochemistry
stain, 200X).
1. insufficient LH and FSH secretion by normal gonadotrophs due to tumor compression;
2. gonadotroph deficiency resulted from the associated hyperprolactinemia;
3. secretion of bioinactive gonadotropin monomer subunits instead of the intact bioactive heterodimers, resulting in inadequate gonadotropin stimulation of the gonads by these subunits.
About 80-90% of NFPA are gonadotroph cell adenomas (gonadotrophinomas)
3. They can synthesize FSH and/or LH, or the alpha or beta subunits of these heterodimers. Among gonadotropin secreting tumors, FSH secretion is more predominant than LH
1. Pure FSH-secreting pituitary adenoma was uncommon. It was more frequently seen in men and was increasing with age
5. Overproduction of FSH in men seldom causes clinical symptoms
6.
In this case, a huge pituitary tumor (macroa- denoma) was found on brain CT and MRI.To arrange brain imaging in a patient with syncope is necessary when neurological lesion should be excluded. In this case, clinical signs of pituitary hormones deficit including visual field defect, hypopigmentation of areola, thinning eyebrows, scanty axillary and pubic hair were present but they could be missed by old age. Hyponatremia could be a hint for hypopituitarism. In fact, the assessment of serum cortisol and thyroid function is helpful to differentiate the cause of hyponatremia. Ophthalmologic evaluation for visual field assessment showed the typical presentation of bitemporal hemianopia caused by tumor compression of optic chiasma. The morning cortisol concentration was low without elevation of adrenocorticotropin (ACTH), suggesting secondary adrenal insufficiency. Similarly, free T4 concentration was below normal range and the TSH concentration was not elevated, which was also compatible with secondary hypothyroidism.
The low total testosterone concentration suggested
hypogonadism but the FSH concentration was unexpectedly elevated while the LH was not, suggesting FSH-secreting pituitary adenoma. There was no relevant symptom or sign of hormonal hyper-secretion syndrome in this case. Therefore, we believed the secreted FSH is immune-reactive rather than bioactive.
Syncope in patient with pituitary tumor has been reported but the cause is unknown and rarely discussed
4. Pituitary apoplexy, resulting from acute infarction of pituitary adenoma, may cause symptoms such as headache (63%), visual field defect (61%), vomiting (50%), ocular paresis (40%), mental deterioration (13%), hyponatremia (13%) and rarely, syncope (5%)
7. In this case, the pathology findings highly suggested the presence of pituitary apoplexy since extensive hemorrhage without necrosis was found. Autonomic failure with syncope has been described in a patient with macroprolactinoma
8. Trigemino-cardiac reflex (TCR), an autonomic reflex of brainstem, were occasionally occurred during surgical procedures involving pituitary fossa
9. It is defined as sudden onset of parasympathetic activity, sympathetic hypotension, apnea, or gastric hyper-motility during central or peripheral stimulation of any of the sensory branches of the trigeminal nerve. Whether a large pituitary tumor triggers TCR is unknown.
In our case, we have excluded common causes of syncope with a serial of examinations. Since the blood pressure change and heart rate response were not available when the patient experienced the syncope, we cannot clarify the relationship between pituitary tumor and TCR. Taken together, pituitary apoplexy is most likely the cause of syncope in this case.
Surgical intervention is indicated for macroa-
denomas to relieve the mass effects. Our patient
received endoscopic transnasal transsphenoidal
adenomectomy for tumor removal. Cumulating
evidences showed that the endoscopic transnasal,
nontransseptal, transsphenoidal pituitary surgery is preferred than the traditional sublabial transseptal approach
10. With the improvement of the technique, transnasal procedure provides a rapid and safe route to the sella turcica with superior visualization, potentially more complete tumor resection, shorter hospital stay, less complications and more cost-effectiveness
11-13. For residual or recurrent tumors, stereotactic radiosurgery or conventional radiotherapy are the treatment of choice
14. Long-term pituitary hormone replacement is inevitable.
In conclusion, FSH-secreting NFPA is rare. The diagnosis of NFPAs depends on clinical suspicion especially in patients with unusual presentation.
Early detection may improve the clinical outcome and reducing risks of complications.
References
1. Hanson PL, Aylwin SJ, Monson JP, Burrin JM. FSH secretion predominates in vivo and in vitro in patients with non-functioning pituitary adenomas. Eur J Endocrinol 2005;
152: 363-70.
2. Ho DM, Hsu CY, Ting LT, Chiang H. The clinicopathological characteristics of gonadotroph cell adenoma: a study of 118 cases. Hum Pathol 1997; 28: 905-11.
3. Chanson P, Brochier S. Non-functioning pituitary adenomas.
J Endocrinol Invest 2005; 28: 93-9.
4. Penín A M, Araújo AR, Rodríguez FR, Sesma SP. Syncope in a 57 year old male. Rev Clin Esp 2006; 206: 153-4.
5. Kwekkeboom DJ, de Jong FH, Lamberts SW. Gonadotropin
release by clinically nonfunctioning and gonadotroph pituitary adenomas in vivo and in vitro: relation to sex and effects of thyrotropin-releasing hormone, gonadotropin- releasing hormone, and bromocriptine. J Clin Endocrinol Metab 1989; 68: 1128-35.
6. Dahlqvist P, Koskinen LO, Brannstrom T, Hagg E. Testicular enlargement in a patient with a FSH-secreting pituitary adenoma. Endocrine 2010; 37: 289-93.
7. Lubina A, Olchovsky D, Berezin M, Ram Z, Hadani M, Shimon I. Management of pituitary apoplexy: clinical experience with 40 patients. Acta Neurochir (Wien) 2005;
147: 151-7.
8. Seiler L, Braune S, Borm K, et al. Autonomic failure mimicing dopamine agonist induced vertigo in a patient with macroprolactinoma. Exp Clin Endocrinol Diabetes 2002;
110: 364-9.
9. Schaller B, Cornelius JF, Prabhakar H, et al. The trigemino- cardiac reflex: an update of the current knowledge. J Neurosurg Anesthesiol 2009; 21: 187-95.
10. Yang I, Wang MB, Bergsneider M. Making the transition from microsurgery to endoscopic trans-sphenoidal pituitary neurosurgery. Neurosurg Clin N Am 2010; 21: 643-51.
11. Kabil MS, Eby JB, Shahinian HK. Fully endoscopic endonasal vs. transseptal transsphenoidal pituitary surgery.
Minim Invasive Neurosurg 2005; 48: 348-54.
12. Har-El G. Endoscopic transnasal transsphenoidal pituitary surgery--comparison with the traditional sublabial transseptal approach. Otolaryngol Clin North Am 2005; 38: 723-35.
13. Oosmanally N, Paul JE, Zanation AM, Ewend MG, Senior BA, Ebert CS, Jr. Comparative analysis of cost of endoscopic endonasal minimally invasive and sublabial-transseptal approaches to the pituitary. Int Forum Allergy Rhinol 2011; 1:
242-9.
14. Kim W, Clelland C, Yang I, Pouratian N. Comprehensive
review of stereotactic radiosurgery for medically and
surgically refractory pituitary adenomas. Surg Neurol Int
2012; 3: S79-S89.
以暈厥表現的分泌 FSH 之非功能性腦垂體腺瘤:
病例報告及文獻回顧
王寶妹
2王文奇
3,4林進耀
4,5曾邵勇
6馬文雅
1,4天主教耕莘醫院新店總院
1
新陳代謝內分泌科
2內科
3神經醫學中心
4