୯ҥѠεᏢᙴᏢଣނݯᕍᏢسᄤࣴز܌
ᅺγፕЎ
School and Graduate Institute of Physical Therapy College of Medicine
National Taiwan University Master Thesis
ᑡԾഈੱᜪဂምᛖޑᆵѴٽϐՉࣁᆶբว
Behavioral and Motor Development in
Taiwanese Toddlers with Autism Spectrum Disorder
ླྀΞ
Yu-Ching Yang
ࡰᏤ௲: ֆਖཁ റγ Advisor: Yen-Tzu Wu, PT, PhD
ύ҇୯ 107 ԃ 7 Д July 2017
!!
國立臺灣大學(碩)博士學位論文
口試委員會審定書
中文題目:蓋志自哈症扛曆社焱人國臺昺幼兒 2 行為綬軔启l心
英文題目: Be. 屆五丑A1fJfov 缸 'r
粉eni;iVJ 右 i
/;J"'況凡圀Jd!园閂曰汪
5 严 Tr«m 历。占 r
本論文係丰荔叉苫君(學號·Roll--lf-函叮 )在國立臺灣大學 微生物學所完成之碩(博)士學位論文,於民國_!_!!.l年二辶月立L日承 下列考試委員審查通過及口試及格,特此證明
口試委員:
ii� (指導教授)
辶籤名)
曰
系主任、所長 王式 缸几 (簽名)
ठ ठᖴ!
ሤӀबǴ߃Εᅺγٗ٤යࡑᆶᦷᦶӅӸޑඳϝᐕᐕӧҞǴٿԃޑਓำ
࣮՟ᅐߏࠅΞӵࢄВమධǶځύाനགᖴΨനٌधޑਖཁԴৣǴགᖴாЇሦך
Εாޑჴᡍ࠻Ǵӧ߃ٰᅺγϐਔ๏ϒךߚதӭЈᡫޑႴᓰǴхך٠๏ϒ ךࡐӭᏢಞޑᐒǴᡣךௗΑԾഈੱѴٽਡЈϸᔈ૽ግޑϣǴΨᡣךкჴΑ ࡐӭᜢܭԾഈੱѴٽว࣬ᜢޑፕЎǴᡣךճֹԋ೭ԛፕЎޑԏਢǴჹ೭٤
ձޑԾഈੱѴٽჴሞޑᖏຑǶࡕයޑፕЎኗቪǴ׳ࢂགᐟԴৣԛऐЈӦ ᐟวךޑᡄᒠࡘԵǴᙖҗԛΞԛᆶךऐЈޑፕЎകޑࢎᄬεᆜᆶ࣬ᔈޑϣ
ǴᡣךᏢಞӵՖӭၗૻ٠ᆒᙁףाޑਜቪрٰǴзךᕇؼӭ!Դৣӧྣ
៝ৎӕਔǴᕴࢂᅰӄЈӦڐշךǵႴᓰךᆶᐟᕏрך׳ӭޑወૈǴЈགᐟ
ாٿԃٰޑਭᆶᜢྣǴΨགډࡐ۩ၮǵࡐགৱૈԖᐒௗڙԴৣޑࡰᏤǼԜ ѦǴाձགᖴᎄԴৣӧيঋኧᙍϐύǴុڐշԐౢٽޑԏਢǴΨགᖴாӧፐ
௲ӭޑԐౢٽว࣬ᜢޕǴаϷࣴز܌ሡाޑࡘԵБԄǴ೭ԛΨჹ ҁጇፕЎ๏ϒӭჹܭीБݤᆶ่݀ϩǵፕޑᝊࡌǹགᖴఆᙴৣǴᕷ ԆύϝଛӝਔࢤᏼҺךޑα၂ہǴගٮΑᙴৣޑόӕᢀᗺᆶࡌǴᡣҁЎӧᖏ
ޑᔈҔԖΑ׳ӭޑᡫགᆶፕǹགᖴᐽᙴৣǴӧԆޑՉำύૈޔុڐ շךӧԾഈੱѴٽޑԏਢǴ೭ԛΨଯࡋଛӝਔࢤӦᏼҺךޑα၂ہǴ٠ਥᏵԾ ഈੱ࣬ᜢޕᆶၸѐޑᖏᡍǴ๏ϒךӭᝊᆶჴҔޑࡌǴ٬೭ጇЎ ക׳укჴᆶֹǶ
ΨགᖴୖᆶҁጇࣴزޑՏঁਢᆶৎԋǴΨᖴᖴࣴز࠻܌Ԗୖᆶၸޑ ԋǺऎదǵॕนǵ٩ࡣǵߜϐǵߜ֗ǵыྼǵᆺǵϺՆǵ☰නǵᄪऍǴགᐟ գॺ឴࣊ӭଷВਔӀޑбрᆶᔅԆ೭ሶӭޑຑǹགᖴᅺγޑቚǵЎធǵ ځӼǵ㻝ǵྼǵ؊܃ǵ☰ൟǵ၃ዅǴӢࣁԖᆶգॺޑϕ࣬ЍᆶѺǴᡣך ࡋၸזޑٿԃᅺγғࢲ
നࡕǴགᖴךޑ༰༰ǵѦϦǵѦஇǴ๏ϒךന୲மԶྕཪޑࡕ࣯Ǵаന
хޑЈࡋၸӳӭঁؒԖךޑڬ҃Ǵᡣךૈݙىޑਔ໔ֹԋӚຑǴ
ձࢂ༰༰ٿຼӦчٰ࣮ךǴՔךኖၸคኧঁשǵ֚ნᆶགྷܫకޑਔ څ!ӆԛགᖴځѬ҂ૈӈޑৎΓᆶܻ϶ॺޑЍᆶڐշǶ
Table of content
Table of content ... i
ύЎᄔा ... v
English Abstract ... vii
Chapter I. Introduction ... 1
1.1 Background ... 1
1.2 Thesis purpose ... 6
1.3 Research questions and hypotheses ... 6
Chapter II. Literature Review ... 8
2.1 Behavioral development and problems in young children with Autism Spectrum Disorder (ASD) ... 8
2.1.1 Developmental change of restricted and repetitive patterns of behavior/ interests (RRBs) in typical development and ASD ... 9
2.1.2 Measurements of RRBs in young children with ASD ... 11
2.2 Motor development and deficits in young children with ASD ... 14
2.2.1 Motor deficits and the association with ASD in early childhood ... 15
2.2.2 Assessment of motor development in young children with ASD ... 15
2.3 Behavioral and motor development in very-low-birth weight (VLBW) preterm children ... 16
2.3.1 VLBW preterm toddlers and the risk of developing ASD ... 19
2.3.2 Behavioral and motor development between young children with ASD and atypically developing (ATD) children ... 21
Chapter III. Method ... 25
3.1 Participants ... 25
3.2 Experimental procedures ... 26
3.3 Measurements ... 27
3.4 Training of assessors ... 33
3.5 Statistical analysis ... 34
Chapter IV. Result ... 36
4.1 Subject characteristics ... 36
4.2 Behavioral problems assessed using the Children Behavior Checklist for ages 1.5–5 years (CBCL/1.5-5) ... 37
4.3 Restricted, repetitive patterns of behaviors (RRBs) assessed using the Repetitive Behavior Scale-Revised (RBS-R) ... 38
4.4 Motor developments assessed using the Peabody Developmental Motor Scales, Second Edition (PDMS-2) ... 39
4.5 Effects of ASD versus VLBW and preterm birth on behavioral and motor problems ... 39
Chapter V. Discussion ... 42
5.1 Behavioral problems in Taiwanese toddlers with ASD... 42
5.2 Behavioral trajectories and interests in Taiwanese toddlers with ASD... 43
5.3 RRBs in Taiwanese toddlers with ASD ... 44
5.4 Motor developmental problems in Taiwanese toddlers with ASD ... 46
5.5 Behavioral and motor developments between full-term toddlers with ASD and VLBW preterm Toddlers ... 48
5.6 Limitation ... 50
Chapter VI. Conclusion ... 52
References ... 53
Tables and Figures ... 69
Figure 1. The setting of the laboratory room for behavioral tracking experiment .. ... 69
Figure 2. The Heat map of the Toddlers with ASD, VLBW preterm children and TD toddlers ... 70
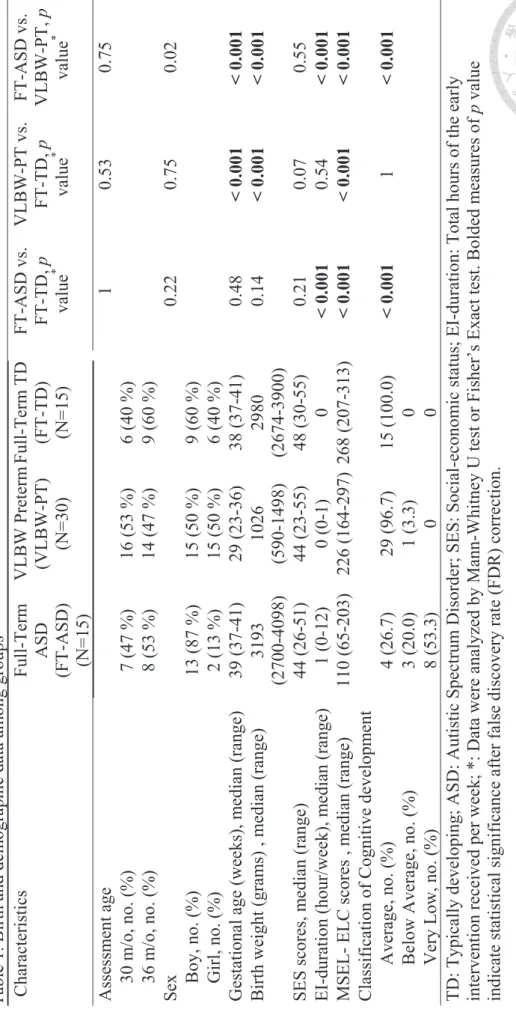
Table 1. Birth and demographic data among groups ... 71
Table 2-1. Behavioral problems assessed by Children Behavior Checklist for ages 1.5–5 years (CBCL/1.5-5) DSM-Oriented Scales ... 72
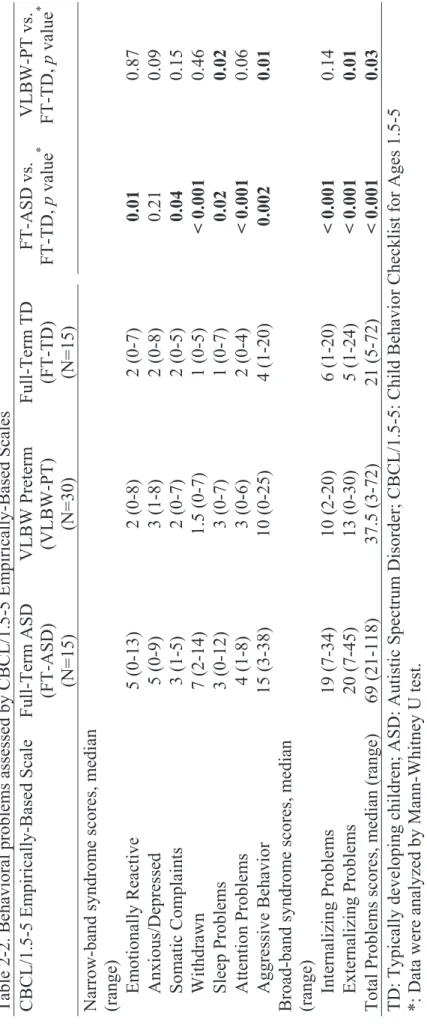
Table 2-2. Behavioral problems assessed by CBCL/1.5-5 Empirically-Based Scales ... 73
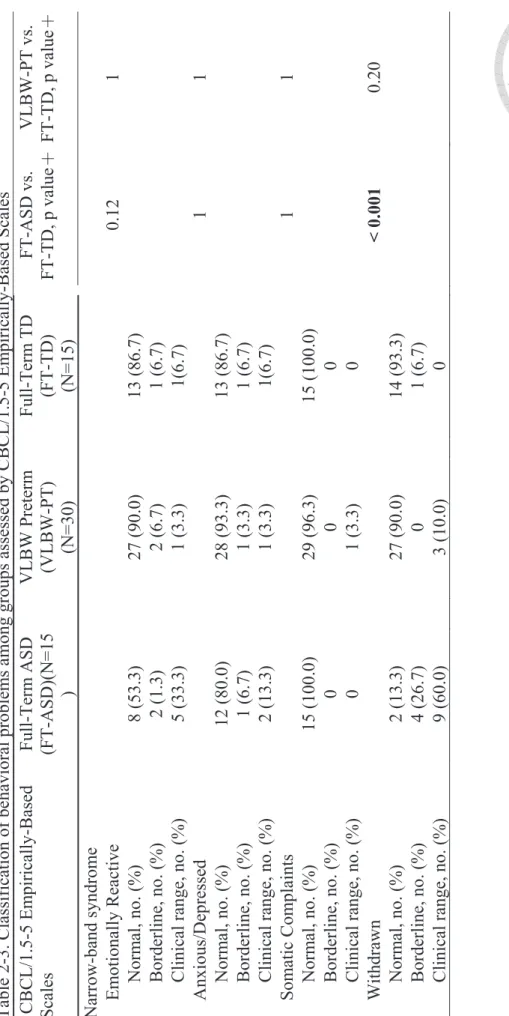
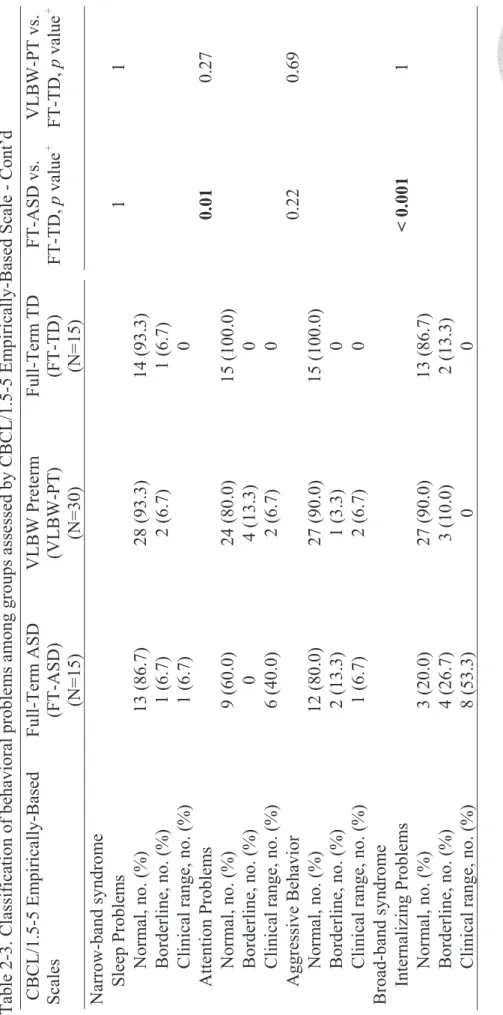
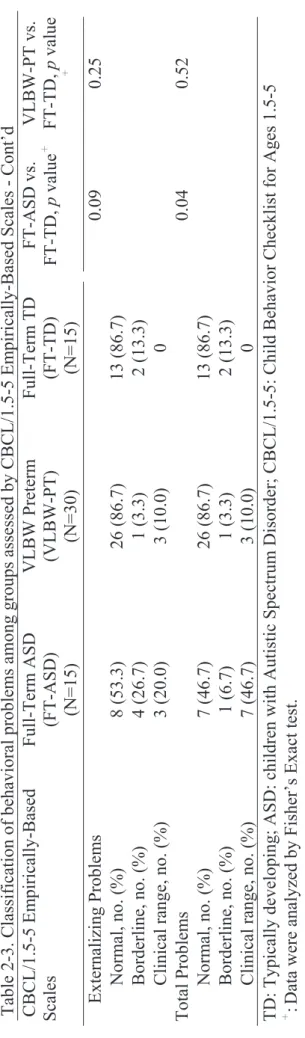
Table 2-3. Classification of behavioral problems among groups assessed by CBCL/1.5-5 Empirically-Based Scales ... 74
Table 3. Behavioral trajectories among groups assessed by automatic tracking device ... 77
Table 4. RRBs among groups assessed by RBS-R ... 79
Table 5-1. Motor performances among groups assessed by the PDMS ... 80
PDMS-2 ... 81
Table 6. Simple linear regression for the effects of ASD versus VLBW and preterm birth on behavioral and motor problems ... 83
Appendix ... 84
Appendix A. Measurements for restricted and repetitive patterns of behavior, interests, or activities in young children with ASD ... 85
Appendix B. Comparisons of motor deficits between children with ASD and typically developing children... 87
Appendix C. Comparisons of behavioral deficits between children with ASD and ATD children ... 88
Appendix D. Comparisons of motor deficits between children with ASD and ATD children ... 90
Appendix E. Informed consent form ... 93
Appendix F. Basic demographic form ... 99
Appendix G. Repetitive Behavior Scale-Revised (RBS-R) ... 102
ύ
ύЎᄔा
Ծഈੱᜪဂምᛖ(ᙁᆀԾഈੱ)ࢂᅿઓวምᛖ܄੯ੰǴځਡЈੱރࣁޗҬ
ྎ೯લཞᆶ߳ज़ǵख़ፄޑڰՉࣁکᑫ፪ǶၸѐࣴزᡉҢԾഈੱٽู౦தޑՉࣁ ᆶբวୢᚒதӧᓻѴٽ໘ࢤрǴฅԶၸѐࣴزၨϿ٬Ҕྗϯޑวෳᡍ πڀຑԾഈੱѴٽޑբวୢᚒǴҭคଞჹᆵԾഈੱٽูޑ࣬ᜢࣴزǶԜ ѦǴၸѐࣴزวཱུե܈ຬեрғᡏख़Ԑౢٽၨ҅தىДٽԖၨӭޑԾഈੱރ
፦ᆶၨଯޑӒᓀ܄ᑡԾഈੱǴฅԶၸѐ٠คىДрғЪᑡԾഈੱϐѴٽ ᆶཱུեрғᡏख़ԐౢѴٽޑวৡ౦ǶӢԜǴҁࣴزϐҞޑࣁᆵىДԾഈ
ੱѴٽޑբᆶՉࣁว߄Ǵ٠کӕសϐىД҅தѴٽᆶཱུեрғᡏख़ԐౢѴ ٽޑวКၨǶҁࣴزӅܕ༅ 15 Տԃស 30 ܈ 36 ঁДεޑىДԾഈੱѴٽǵ15 Տ҅தىДѴٽǵᆶ 30 Տཱུեрғᡏख़ԐౢѴٽǶڙ၂ٽูௗڙՉࣁวᆶբ фૈޑຑǶՉࣁวෳໆхࡴ:(1)Р҆༤ቪྃъԿϖྃٽูՉࣁᔠਡ߄ϐୢ
ڔ;(2)٬ҔԾϯՉࣁଓᙫسෳໆѴٽӧԾҗވऑნΠޑՉࣁॉၞᆶᑫ፪
ୱ;аϷ(3)Р҆༤ቪख़ፄՉࣁໆ߄অुހϐୢڔǶѴٽޑբว٬ҔҜЃ्բ วໆ߄ಃΒހෳໆӭޑբфૈǶࣴز٬Ҕୗ-ඁѭ U ᔠᡍӚวࡰӧ ىДԾഈੱѴٽǵཱུեрғᡏख़ԐౢѴٽǴᆶ҅தىДѴٽ໔ޑಔձৡ౦Ǵ٠٬
Ҕᙁൂጕ܄ӣᘜКၨԾഈੱ܈ཱུեрғᡏख़ЪԐౢޑӢનϐܭՉࣁᆶբวୢ
ᚒޑਏᔈǶࣴز่݀ᡉҢǴӧྃъԿϖྃٽูՉࣁᔠਡ߄ϐୢڔ่݀ύǴىД ԾഈੱѴٽӧځύѤᅿᆒઓ੯ੰᏤӛୢᚒǵϤᅿઞՉࣁੱރǵϣᡉᆶѦᡉୢᚒǵ ϷᕴՉࣁୢᚒޑϩኧ֡ᡉଯܭ҅தىДѴٽǹ࣬ϸӦǴཱུեрғᡏख़ԐౢѴٽ ӧགୢᚒǵቶݱว܄ୢᚒǵᆣϸᔈǵيᡏܤǵଏᕭǵݙཀΚୢᚒϷϣᡉ
ୢᚒޑϩኧǴ֡ᆶ҅தىДѴٽޑϩኧ࣬Ƕ٠ЪǴԾϯՉࣁଓᙫسวǴ ىДԾഈੱѴٽၨ҅தىДѴٽଶ੮ӧڬᜐୱޑਔ໔ၨߏǵΕР҆ୱ܌
ޑਔ໔ၨอǵаϷӧᙯ୮բਔԖၨଯޑᙯفೲࡋǹฅԶǴཱུեрғᡏख़Ԑౢ
Ѵٽᆶ҅தىДѴٽޑ߄࣬ǶӆޣǴख़ፄՉࣁໆ߄অुހޑୢڔ่݀วى ДԾഈੱѴٽ࣬ၨ҅தىДѴٽǴӧᕴϩǵڰ܄ՉࣁǵڰۓՉࣁ(לܔᡂϯǴ୲
٣ނᆢচኬ)ᆶڙज़Չࣁ(ڙज़ޑᜢЈጄൎǵགᑫ፪ᆶࢲጄൎ)ޑϩኧ֡ᡉ
ၨଯǹฅԶǴཱུեрғᡏख़ԐౢѴٽӧᆶ҅தىДѴٽޑϩኧ٠คᡉৡ౦ǶԜ ѦǴىДԾഈੱѴٽӧҜЃ्բวໆ߄ಃΒހޑᕴբǵಉεբϷᆒಒ
բϩኧ֡ᡉեܭ҅தىДٽǴ٠ЪىДԾഈੱѴٽԖၨଯКပܭբཱུৡޑ
ભǹฅԶǴཱུեрғᡏख़ԐౢٽѝԖӧ౽Տϩኧၨ҅தىДٽեပǶԜѦǴࣴ
زวԾഈੱӢનᆶᆒઓ੯ੰᏤӛୢᚒǵѦᡉୢᚒǵᕴୢᚒϩኧǵᆶ౽Տբϩ ኧǴ֡Кཱུեрғᡏख़ЪԐౢӢનԖ׳ଯޑ࣬ᜢ܄Ƕҁጇࣴز่݀ᡉҢǴ30 ᆶ 36
ঁДޑىДԾഈੱѴٽ߄ӭኬޑՉࣁୢᚒᆶեပޑբфૈǶᗨฅཱུեрғᡏ ख़ӝٳԐౢ೭ঁӢનǴᆶѦᡉୢᚒᆶեပޑ౽ՏфૈԖᜢǴځჹܭՉࣁکբ วୢᚒޑቹៜեܭԾഈੱǶӧᖏᔈҔǴҁጇࣴزᡉҢӄय़ЪԐයϟΕԾഈ
ੱѴٽޑՉࣁᆶբวୢᚒࢂԖѸाޑǶ
ᜢᗖӷ: ԾഈੱᜪဂምᛖǵѴٽਔයǵՉࣁǵբǵԐౢǵཱུեрғᡏख़
English Abstract
Background and Purposes: Studies have suggested that behavioral and motor developmental problems typically occur in the early childhood of people with autism spectrum disorder (ASD). However, few studies have used standardized developmental assessment instruments for evaluating early motor developmental disorders in toddlers with ASD. Furthermore, very-low-birth-weight preterm (VLBW-PT) toddlers were found to exhibit more autistic traits and a higher risk of ASD than full-term (FT) toddlers. However, developmental differences between FT toddlers with ASD
(FT-ASD) and VLBW-PT toddlers have rarely been evaluated. Therefore, the present study investigated the behavioral and motor development of Taiwanese toddlers with ASD and compared the development between FT-ASD, FT typically developing (FT-TD), and VLBW-PT toddlers. Methods: In total, 15 FT-ASD, 15 FT-TD, and 30 VLBW-PT toddlers aged 30 or 36 months were included in this study. All toddlers’
behavioral performances were examined using the Child Behavior Checklist for Ages 1.5–5 (CBCL/1.5–5) and the Repetitive Behavior Scale-Revised (RBS-R). Behavioral trajectory and interests were examined in a free play situation by using the automated behavioral tracking system. Toddlers’ motor functions were examined using the
Peabody Developmental Motor Scales, Second Edition (PDMS-2). The Mann–Whitney U test was conducted to examine the differences in each developmental indicator among the groups. For the behavioral or motor indicators for which both FT-ASD and
VLBW-PT toddlers differed significantly compared with FT-TD toddlers, a simple linear regression analysis was conducted to determine the effects of ASD versus VLBW and Preterm birth. Results: The results indicated that FT-ASD toddlers achieved
significantly higher CBCL/1.5–5 scores than FT-TD toddlers for four Diagnostic and Statistical Manual of Mental Disorders (DSM)-Oriented Scales; six Narrow-band
syndromes; and Internalizing, Externalizing, and Total Problems (all p’s < 0.05). By contrast, VLBW-PT toddlers and FT-TD toddlers had comparable scores for Affective and Pervasive Developmental Problems, Emotionally Reactive, Somatic Complaints, Withdrawn, Attention Problems and Internalizing Problems. Furthermore, the
behavioral tracking data revealed that FT-ASD toddlers spent significantly longer durations in peripheral areas, had less latency to approach the parent, and had higher absolute angular velocities of repetitive turning movements than FT-TD toddlers (all p’s
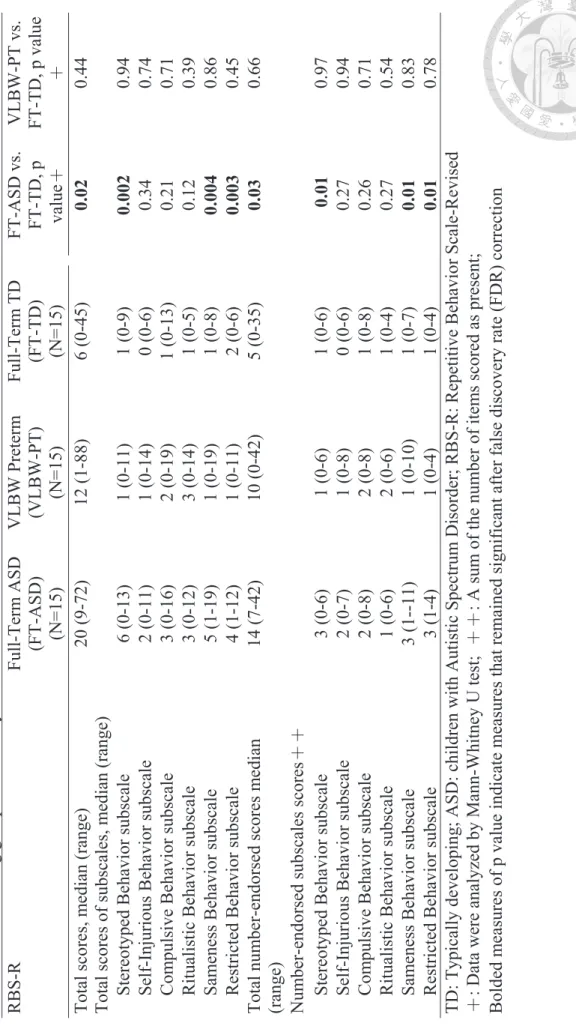
< 0.05), whereas VLBW-PT and FT-TD toddlers had comparable behavioral tracking results. Moreover, FT-ASD toddlers had higher total RBS-R scores and stereotyped, sameness, and restricted behavior subscales scores than FT-TD toddlers (all p’s < 0.05), whereas VLBW-PT and FT-TD toddlers had comparable RBS-R scales scores. In addition, the motor function assessment results revealed that FT-ASD toddlers achieved significantly lower motor scores and a higher proportion of poor classification in the Total, Gross, and Fine Motor Scales of the PDMS-2 than FT-TD toddlers (all p’s <
0.05), whereas VLBW-PT and FT-TD toddlers had comparable motor scores, except for locomotion scores, which were lower in VLBW-PT toddlers. The higher effects of ASD on several behavioral and motor indicators were associated with higher scores for the DSM-Oriented Scales (β = 1.8 – 2.5), Externalizing (β = 6.8), and Total Problems (β = 24.8); and lower locomotion scores (β = -1.7) compared with the effects of VLBW and Preterm birth (all p’s < 0.05). The present findings revealed that FT-ASD toddlers exhibited high degrees of various behavioral problems and poor motor functions at the ages of 30 and 36 months. Although VLBW and preterm birth may be associated with externalizing problems and poor locomotion skills, their effects on behavioral or motor performances were milder than those of ASD. The present findings suggest that
comprehensive interventions focused on multiple behavioral and motor developmental
domains are necessary for toddlers with ASD.
Key Words: ASD, Toddlers, Behavior, Motor, Preterm, VLBW
Chapter I. Introduction
1.1 Background
Autism spectrum disorder (ASD) is a neurodevelopmental disability characterized by deficits in social interaction and communication, and the presence of repetitive and restricted behaviors/ interests (RRBs) that can cause major problems in social
interaction and communication (American Psychiatric Association, 2013). Individuals with ASD were previously given a diagnosis of Autistic disorder, Pervasive
developmental disorder—not otherwise specified (PDD-NOS), or Asperger’s disorder according to the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR). In the fifth edition, all these diagnoses are now subsumed under the single label of ASD. The prevalence of ASD among 8-year-old children in the United States increased from 6.7 per 1,000 children in 2000 to 14.7 per 1,000 in 2012 (Autism and Developmental Disabilities Monitoring Network Surveillance Year 2000 Principal Investigators & Centers for Disease Control and Prevention, 2007; Autism Developmental Disabilities Monitoring Network Surveillance Year 2010 Principal Investigators, 2014). In Taiwan, the cumulative prevalence of ASD among 3- to
17-year-old children increased from 0.18 per 1000 children in 1996 to 2.87 per 1000 in 2005, and the prevalence rate increased rapidly to 2.21% in 2011 (Chien, Lin, Chou, &
Chou, 2011; Hwang, Weng, Cho, & Tsai, 2013; Lai, Tseng, & Guo, 2013). Parents have most frequently expressed concerns regarding the development of their children before the age of 3 years, but diagnoses of ASD occur at ages of approximately 4 – 6 years.
(De Giacomo & Fombonne, 1998; Hwang et al., 2013; Lai et al., 2013). Therefore, early intervention for children with ASD is necessary to address the symptoms of ASD and long-term outcomes.
RRBs are a core feature of ASD that include symptoms of stereotyped or repetitive motor movements, insistence on sameness, and inflexible adherence to routines.
Although RRBs are normally observed in typically developing (TD) toddlers (Morgan, Wetherby, & Barber, 2008), previous studies have indicated that children with ASD demonstrate significantly higher frequencies and longer durations of RRBs than do TD toddlers (Barber, Wetherby, & Chambers, 2012; Fulceri et al., 2016; Kim & Lord, 2010;
Richler, Bishop, Kleinke, & Lord, 2007). Furthermore, the symptoms of RRBs have been associated with more severe ASD symptoms and more impaired motor, language, cognitive, and social interaction functioning among children with ASD (Elison et al., 2014; Kim & Lord, 2010; Morgan et al., 2008; Richler, Huerta, Bishop, & Lord, 2010;
Watt, Wetherby, Barber, & Morgan, 2008). Therefore, assessment of RRBs in the early childhood is important to help identify early symptoms of ASD in young children.
Several clinically oriented measures are used for measuring RRBs in children with ASD. These methods include caregiver interviews, questionnaires, and observational methods. Caregiver interviews, such as the Autism Diagnostic Interview-Revised, include several repetitive behavior items for detecting features of RRBs. Questionnaire measures such as the Repetitive Behavior Scale-Revised (RBS-R) or the Repetitive Behavior Scale for Early Childhood (RBS-EC) are caregiver rating scales also capable of capturing a wider range of behavioral features. However, because interview or questionnaire measures are subjective, their accuracy may be hampered by recall bias.
In addition, semi-structured observational methods, such as the Repetitive and Stereotyped Movement Scales (RSMS) and the Autism Diagnostic Observational Schedule (ADOS), are designed for clinicians to examine the RRBs of children by interacting with children in standardized testing procedures. Although semi-structured observational methods are relatively objective and yield quantitative data, these
methods are more labor intensive and may be constrained by the RRBs observable during the assessment, such as a focus on stereotypical motor movements rather than on restricted rituals or routine behaviors. Cohen et al. (Cohen, Gardner, Karmel, & Kim, 2014) used an automatic behavioral tracking system to investigate behavioral trajectory of children with ASD in free play situations. Several time- and space-related variables relevant to behavior characteristics and interest were analyzed. The results revealed that children with ASD had a longer period of latency to approach parents and more time spent at the periphery than did atypically developing (ATD) children. Furthermore, the time spent at the periphery was positively and moderately correlated with the severity of ASD (r = 0.63). Thus, the automatic behavioral tracking system is a valid method for investigating the characteristics of RRBs in ASD.
Although social communication deficits and abnormal behavioral performance are important diagnostic criteria for ASD, the high co-occurrence of motor deficits
contributes to the clinical features of ASD. Abnormalities in motor-related brain regions and associations with motor impairments were identified in children with ASD. These findings indicated possible common neurological roots that are primarily involved in sensory–motor coordination problems and link to the core symptoms of ASD (Carr, Iacoboni, Dubeau, Mazziotta, & Lenzi, 2003; Courchesne et al., 2011; Courchesne et al., 2007; Oberman et al., 2005; Rizzolatti, 2005; Rizzolatti, Fogassi, & Gallese, 2001). In addition, previous studies have revealed that motor problems, including delayed gross and fine motor development, delayed postural development, and stereotyped
movements, can be observed in toddlers or preschoolers with ASD (Bhat, Galloway, &
Landa, 2012; Gernsbacher, Sauer, Geye, Schweigert, & Hill Goldsmith, 2008; Lloyd, MacDonald, & Lord, 2013; Nickel, Thatcher, Keller, Wozniak, & Iverson, 2013;
Ozonoff et al., 2014). Furthermore, early motor problems have been found to associate
with delayed and impaired social interaction and communication (Bhat et al., 2012) and maladaptive behaviors at older ages (MacDonald, Lord, & Ulrich, 2013). However, previous studies have used parental reports or home videos rather than standardized developmental assessment tools for assessing children’s motor function and were accordingly lacking detailed information regarding motor development in multiple motor dimensions. Moreover, no studies have yet assessed early motor development in Taiwanese children with ASD. A comprehensive evaluation of motor function in Taiwanese toddlers with ASD is warranted.
In addition to understanding the behavioral and motor development in young children with ASD, children born prematurely must be considered for long-term
development because they are more likely to show multiple developmental problems in early childhood and to sustain lifelong consequences. Preterm children are defined as live babies born before 37 weeks of pregnancy. Despite the increase in annual survival rates in preterm infants, a higher diagnostic rate of cerebral palsy, blindness, hearing impairments, intellectual disability, and multiple developmental disorders has been observed in preterm children than in full-term children (Barre, Morgan, Doyle, &
Anderson, 2011; Doyle, 2004; Linsell, Malouf, Morris, Kurinczuk, & Marlow, 2016;
Stoelhorst et al., 2003; Wong, Huertas-Ceballos, Cowan, & Modi, 2014). ASD is one of the neurodevelopmental disorders observed among preterm children, with an estimated prevalence of approximately 5 – 8% in the preterm cohort (Johnson et al., 2010;
Pinto-Martin et al., 2011). Furthermore, prematurity and very low birth weight (VLBW) are considered to be risk factors for ASD (Hwang et al., 2013; Kuzniewicz et al., 2014;
Lampi et al., 2012; Leavey, Zwaigenbaum, Heavner, & Burstyn, 2013; Limperopoulos et al., 2008). More autistic traits and ASD symptoms were detected in the VLBW preterm infants as compared with full-term infants in childhood (Williamson &
Jakobson, 2014a, 2014b; Wong et al., 2014). Previous studies have reported that, in early childhood, a greater number of autistic traits were detected in VLBW preterm infants than in full-term infants, and significantly higher percentages of children showed positive results in the screening of ASD before the age of 3 years (Gray, Edwards, O'Callaghan, & Gibbons, 2015; Guy et al., 2015; Limperopoulos et al., 2008).
In addition to the high prevalence of autistic traits, behavioral problems are commonly observed in VLBW preterm children. Numerous studies have revealed that VLBW preterm children at preschool and school ages manifest adverse behavioral outcomes such as an excess of internalizing and externalizing problems (particularly, problems with attention), withdrawn behavior, poorer adaptive functioning, and lower levels of social and school competence (Gray et al., 2015; Hayes & Sharif, 2009;
Johnson, 2007; Johnson et al., 2010; Johnson & Marlow, 2011; Limperopoulos et al., 2008; Pritchard et al., 2016). In addition to behavioral problems, VLBW preterm children have a high co-occurrence of motor impairment in early childhood. Compared with their term peers, VLBW preterm children tend to exhibit a delayed attainment of motor skills, such as a delayed acquisition of crawling, sitting, and walking (van Haastert, de Vries, Helders, & Jongmans, 2006), muscle imbalance (Pin, Eldridge, &
Galea, 2010); and abnormal gait pattern (Cahill-Rowley & Rose, 2016; Pin et al., 2010), which causes impaired motor function at older ages. Therefore, early identification of motor and behavioral problems to predict later developmental disorders is helpful for early intervention among VLBW preterm children. Although many studies have focused on motor and behavioral developments among VLBW preterm children in the early childhood, no studies have compared the motor and behavioral developments of VLBW preterm children and full-term children with ASD in early childhood. By contrast, several studies have compared young children with ASD and ATD children with
different developmental problems (e.g., global developmental delay or language disorder etc.). Results have indicated that children with ASD revealed more impaired motor functions (Bolton, Golding, Emond, & Steer, 2012; Hellendoorn et al., 2015;
Karmel et al., 2010; Lam & Aman, 2007; Waelvelde, Oostra, Dewitte, Broeck, &
Jongmans, 2010; Zappella et al., 2015) and higher rates of behavioral problems than did ATD children (Elison et al., 2014; Kim & Lord, 2010; Morgan et al., 2008; Richler et al., 2007). Considering the necessity of the early identification of VLBW preterm children who are at risk of developing ASD for early intervention, examining the differences or similarities in motor and behavioral development between VLBW preterm children and full-term children with ASD is important.
1.2 Thesis purpose
The purposes of the study are 1) to examine the behavioral and motor performances in full-term toddlers with ASD (FT-ASD toddlers), VLBW preterm toddlers (VLBW-PT toddlers), and full-term TD toddlers (FT-TD toddlers) at ages of 30 and 36 months; 2) for the motor and behavioral indicators that both FT-ASD and VLBW-PT toddlers were different from the full-term TD toddlers (FT-TD toddlers), the effect of ASD was compared to that of preterm birth with VLBW on behavioral and motor problems.
1.3 Research questions and hypotheses Research question 1:
Do FT-ASD toddlers perform more behavioral problems or more RRBs than those in FT-TD toddlers at ages of 30 and 36 months?
Hypothesis 1:
FT-ASD toddlers obtain higher scores in the Pervasive Developmental Problem scales, Internalizing problems and Withdrawn syndrome defined by the CBCL/1.5-5 at ages of 30 and 36 months.
Research question 2:
Do FT-ASD toddlers obtain lower motor scores than do FT-TD toddlers at ages of 30 and 36 months? Do FT-ASD toddlers exhibit abnormal motor performance at ages of 30 and 36 months?
Hypothesis 2:
The FT-ASD toddlers obtain lower motor scores in the Total Motor, Gross Motor, Fine Motor Scales of the PDMS-2 than do FT-TD toddlers at ages of 30 and 36 months.
Furthermore, the number and percentages of toddlers classified as poor motor performance in the FT-ASD toddlers group are significantly higher than that in the FT-TD toddlers group.
Research question 3:
For the motor and behavioral indicators that both FT-ASD and VLBW-PT toddlers were different from the FT-TD toddlers, are there any differences between the effect of ASD and preterm birth with VLBW on the behavioral and motor problems at ages of 30 and 36 months?
Hypothesis 3:
The adverse effects of ASD on toddlers’ abnormal behavioral problems and poor motor functions are greater than the effects of preterm birth with VLBW at ages of 30 and 36 months.
Chapter II. Literature Review 2.1 Behavioral development and problems in children with ASD
ASD is a neurodevelopmental disability that cause major problems in social-communication and adaptive behavioral development. Deficits in
social-communication skills and the presence of RRBs are two core symptoms of ASD as defined by the DSM-5 (American Psychiatric Association, 2013). With regard to the symptoms of RRBs, Dr. Leo Kanner first conceptualized that the RRBs in person with Autism are a class of behaviors characterized by high frequency and repetition of
movement or speech in an invariant manner and insistence on sameness in activities and rituals (Kanner, 1968). According to the latest edition of diagnostic criteria of ASD in the DSM-5 (American Psychiatric Association, 2013), RRBs were characterized by four behavioral symptoms: 1) stereotyped or repetitive motor movements, use of objects, or speech; 2) insistence on sameness, inflexible adherence to routines, or ritualized patterns of verbal or nonverbal behavior; 3) hyper- or hypo-reactivity to sensory input or unusual interest in sensory aspects of the environment; and 4) highly restricted, fixated interests that are abnormal in intensity or focus. In addition to RRBs, children with ASD are at high risk for developing multiple behavioral problems, including aggressive behaviors (9 - 53%) (Kanne & Mazurek, 2011; Lecavalier, Leone, & Wiltz, 2006), inattention and hyperactivity (69 - 97%) (Mayes, Calhoun, Mayes, & Molitoris, 2012), mood disturbance (38 - 92%) (e.g. emotionally labile, problems with empathy, or over reactivity) (Mayes et al., 2012), sleep problems (50 - 80%) (Mazurek & Sohl, 2016; Richdale & Schreck, 2009; Souders et al., 2009), and withdrawn behaviors (70%) (Albores-Gallo, Betanzos-Cruz, Santos-Sánchez, Lemus-Espinosa, & Hilton, 2012;
Hartley, Sikora, & McCoy, 2008; Limberg, Gruber, & Noterdaeme, 2016). Therefore, early assessment of behavioral development and problems in children with ASD may be
helpful to identify early signs and symptoms of ASD.
2.1.1 Developmental change of RRBs in typical development and ASD
Although the RRBs are core feature in ASD, the appearance of RRBs is a necessary part of normal development in the early childhood. Evans et al. (Evans et al., 1997) have found that TD children begin to exhibit RRBs from 13 to 28 months of age.
The amount of RRBs reached a highest level between 2 - 4 years of age and then followed by a subsequent reduction after 5 years of age (Evans et al., 1997; Zohar &
Felz, 2001). However, children with ASD were found to demonstrate significantly higher frequencies and degrees of RRBs than did TD children across 2 to 5 years of age.
Among the previous studies, there were several studies focusing on measuring child’s repetitive and stereotyped movement with objects and body. Morgan et al. (Morgan et al., 2008) and Kim et al. (Kim & Lord, 2010) have examined repetitive and stereotyped movements in children with ASD and TD children aged 8 - 56 months. Research
clinicians interacted with the child in standardized procedures and recorded child’s body and upper limb movements by using the Repetitive Stereotyped Movement Scale
(RSMS). The results have shown that children with ASD performed significantly higher rates and larger inventories of repetitive and stereotyped movements with body and objects than did TD children (Cohen’s d = 0.61 - 1.40). Likewise, Barber et al. (Barber et al., 2012) have reported higher frequencies of repetitive and stereotyped movement (e.g., rubbing body, stiffening fingers, and spinning objects etc.) in children with ASD (mean age, 21.3 months) as compared with TD children (mean age, 14.6 months) using the RSMS. Besides, appearance of abnormal sensory reaction such as licking, fixating, and sucking fingers were found to occur more frequently in children with ASD than in TD children (Barber et al., 2012). Moreover, Kim et al. (Kim & Lord, 2010) have shown a greater severity level of RRBs in children with ASD as compared with TD
children. These findings suggest that abnormal repetitive and stereotyped movement in children with ASD as major behavioral problems that may interfere with their social interaction.
Except for repetitive and stereotyped movements, inflexible adherence to routines or rituals, restricted interest, or obsessive compulsive-like behaviors are important behavioral features of RRBs in children with ASD. Richler et al. (Richler et al., 2007) have assessed RRBs by interviewing caregivers of children with ASD, children with global developmental delay, and TD children at 2 years of age. The ASD children group showed higher prevalence in the following behaviors: unusual preoccupations (OR = 6.4), unusual sensory interests (OR = 15) , repetitive use of objects (OR = 12), hand/finger mannerisms (OR = 3.8), complex mannerisms (OR = 18), abnormal
response to sensory stimuli (OR = 4.1), difficulties with change (OR = 3.4), and unusual attachments (OR = 6.3) as compared with TD children group (all p’s < 0.05). Fulceri et al. (Fulceri et al., 2016) have examined RRBs in children with ASD and TD children aged 23 to 71 months. The results showed greater frequencies of stereotyped and ritualistic behaviors, restricted interest, compulsive and self-injured behaviors in the ASD children group as compared with TD children. These findings suggest that abnormal behavior and restricted interests are apparent in ASD.
It is noteworthy that higher frequency or more severe RRBs in children with ASD were correlated to more impaired motor, language, cognitive, and social interaction functioning. Elison et al. (Elison et al., 2014) have examined stereotyped motor
mannerisms and repetitive manipulation of objects among 12-month-old infants at high and low risk for developing ASD, and examined developmental outcomes at 24 months of age using the Mullen Scales of Early Learning (MSEL). The results revealed that children who were later diagnosed with ASD showed more repetitive and stereotyped
movements with body than those without ASD, and higher scores of repetitive and stereotyped movements were found to correlate to lower motor scores (r = -0.465, p = 0.01). Furthermore, Richler et al (Richler et al., 2010) have longitudinally examined RRBs and cognitive function in children with ASD at 2, 3, 5, and 9 years of age. The results revealed that higher scores in repetitive and stereotyped movements were correlated to lower nonverbal intelligence scores at each assessment age (r = -0.02). A similar finding was shown in Watt et al. (Watt et al., 2008) that negative and moderate correlations was found between the scores of repetitive and stereotyped movements with objects and the social, symbolic play, speech and non-verbal developmental composite scores [r = (-0.31) – (-0.38)] in children with ASD at 18 and 24 months of ages. Furthermore, higher scores of repetitive and stereotyped movements were predictive of lower non-verbal or verbal developmental quotients at 3 years of age.
These findings suggest that abnormal RRBs exhibited in the early childhood may associate with adverse developmental outcomes. Therefore, identification of RRBs at early ages is necessary to help understand early behavioral symptoms and long-term outcome in ASD.
2.1.2 Measurements of RRBs in young children with ASD.
The methods commonly used for measuring RRBs in young children include caregiver interview, questionnaires, and semi-structured observational methods that previous studies regarding the methods and psychometric properties were summarized in Table 1. For example, the Autism Diagnostic Interview-Revised (ADI-R) is a
structured interview conducted with the parents or caregivers for diagnostic purposes of ASD. The interview comprises items for evaluation of restricted and repetitive behavior.
The ADI-R has been shown to have excellent reliability for testing children aged 3 to 19 years [Inter-rater correlation coefficients (ICCs) = 0.82 - 0.96]. Furthermore, the
interview had acceptable discriminant validity that children with Autistic disorder obtained significantly higher ADI-R scores than that in children with PDD-NOS or
children with other developmental problems (Richler et al., 2007; Tsuchiya et al., 2013).
In addition to the interview method, questionnaire measures, such as the Repetitive Behavior Scale-Revised (RBS-R) is a caregiver rating scale that is capable of capturing a wide range of behavioral features in ASD. The RBS-R consists of six subscales (i.e., Stereotyped behavior, Self-injurious behavior, Compulsive behavior, Ritualistic behavior, Sameness behavior, and Restricted behavior subscales) that was reported to have good-to-excellent internal consistency (Cronbach’s alpha = 0.7 - 0.91) and moderate to high inter-rater reliability for all subscales (ICCs = 0.57 - 0.73) (Lam &
Aman, 2007). Fulceri et al (Fulceri et al., 2016) measured RRBs in children with ASD between 23 to 71 months of age by using the RBS-R. The results revealed that the RBS-R was able to discriminate children with ASD from TD children in the stereotyped behavior, ritualistic and sameness behavior, restricted interests behavior, and total scores. The overall findings revealed that both parental interview and questionnaire measure are good to obtain dimensional features of RRBs and to quantify the severity of behavioral symptoms. However, caregiver report may be subjective and the results may be affected by recall bias or errors.
Semi-structured observation method such as the RSMS or ADOS, are used for assessment of RRBs in standardized testing procedures. Clinician observe and record the frequency and duration of RRBs defined by the Scales. High inter-observer agreement (Kappa = 0.66 - 0.99), and high to excellent inter-rater reliability (ICCs = 0.74 - 0.93) of the RSMS (Barber et al., 2012; Watt et al., 2008), and moderate to high intra-rater reliability (ICCs = 0.6 - 0.75) of the ADOS (Luyster et al., 2009) have been reported. Furthermore, the RSMS had acceptable discriminant validity that children
with ASD demonstrated significantly higher frequency and duration of RRBs than did TD children (Barber et al., 2012; Kim & Lord, 2010; Watt et al., 2008). Although semi-structured observation methods may be more objective to yield quantitative data, they are more labor intensive and may be constrained by capturing a subset of possible RRBs operating during the assessment.
A prior study used automated behavioral tracking devices to detect social interaction and social preference in mice by measuring the percentage of time they spent with an unfamiliar mouse (Moy et al., 2004). In the present, automated
behavioral tracking devices have also been shown to be a promising alternative tool to detect behavioral trajectory and stereotypic behaviors in children with ASD. Cohen et al. (Cohen et al., 2014) has used automated video tracking device and videotaped analysis software to capture a real-time data regarding child’s location and behavior trajectory in a free play situation. In the setting of the study, the toys were placed on the floor and table top, and parents were told to sit on the chair on the corner and minimize interactions between them and their children. The child was tracked for 5 minutes in free play situations. Time spent that child’s ROI toward parent or periphery and relative angular velocities of turning movement were calculated. The results revealed that children with ASD showed more interest toward periphery region by touching the walls or watching themselves in our one-way mirror for sensory seeking and were more likely to perform left-sided of repetitive turning movements than those in ATD children. Besides, positive correlations were found between the time that child spent in the periphery and severities of RRBs measured by the ADOS (r = 0.36-0.69).
These findings suggest the automated video tracking system is able to provide valid data of measuring child’s interest toward specific region and repetitive movements in an objective way, which could help to capture real-time behavioral trajectories of
children for measuring the variety of RRBs in children with ASD.
Although Cohen et al. (Cohen et al., 2014) found behavioral characteristics in children with ASD, the analysis of behavioral trajectory and interest might be
restricted in parent region and periphery region. The interest toward the toy region and the frequencies or velocities of turning movements have not yet been measured.
Furthermore, little is known about the RRBs and behavioral interest among young children with ASD. The investigation of more characteristics regarding behavioral trajectories using the automated behavioral tracking system in toddlers with ASD is warranted.
2.2. Motor development and deficits in young children with ASD
Despite the core symptoms of ASD are deficits in social interaction and
communication and the presence of RRBs, high co-occurrence of motor deficits were found to contribute to clinical features of ASD (Esposito, Venuti, Maestro, & Muratori, 2009; Hilton et al., 2007; Provost, Lopez, & Heimerl, 2007). The prevalence of motor deficits in person with ASD varied from 50% to 80% (Green et al., 2002; Hilton et al., 2007; Ming, Brimacombe, & Wagner, 2007). Bhat et al. (Bhat et al., 2012) have summarized several motor deficits of ASD from early to middle childhood. The motor function was more impaired in young children with ASD comparing to young TD children, such as delayed motor milestones, delayed posture achievement, and stereotyped motor movements. Among the school-aged children, the deficits of imitation and praxis are common and contribute poor performance in postural control and balance, imitation of gestural/ facial expression, and in complex movement sequences, suggesting generalized dyspraxia (Bhat et al., 2012). Therefore, early
assessment of motor development is important for early intervention of motor deficits in children with ASD.
2.2.1 Motor deficits and the association with ASD in early childhood
Several previous studies revealed that the abnormalities of cerebellum (Esposito et al., 2009; Hilton et al., 2007; Provost et al., 2007), subcortical white matter (Courchesne et al., 2011), basal ganglion (Qiu, Adler, Crocetti, Miller, & Mostofsky, 2010) and mirror neuron system (Oberman et al., 2005) may play the roles in motor impairments of ASD. These associations suggest possible common neurological roots that are thought to be primarily involved in motor problems and link to core autistic symptoms.
Furthermore, previous studies revealed correlations between motor performance and social-communication dysfunction in young children with ASD. Bhat et al. (Bhat et al., 2012) have reported that the gross motor scores at 3 months was predictive of low communication scores at 18 months of age in a group of children who were later diagnosed as ASD. Sipes et al. (Sipes, Matson, & Horovitz, 2011) have reported an association between the motor skill and socialization of 17- to 35-month-old children with ASD. The results indicated that those with higher level of gross motor skills exhibiting less impairments in socialization. Furthermore, MacDonald et al.
(MacDonald, Lord, & Ulrich, 2014) has measured motor function and
social-communication skill in 14- to 33-month-old children with ASD. The results showed that lower gross and fine motor scores were associated with lower
social-communication scores. These findings suggest that children with ASD exhibiting more impaired gross or fine motor function may also have more impaired social
communication skill.
2.2.2 Assessment of motor development in young children with ASD
Motor impairment can be observed in children with ASD in early childhood.
Various measurements were used in previous studies for assessing motor function in young children with ASD, including home videotaped observation, parental report, and
developmental assessment instruments (as shown in Table 2). A prior study by Nickel et al. (Nickel et al., 2013) have investigated posture development (supine, prone, sitting, kneeling, all-four, standing, and squat) by video-recording at home in children at high and low risk of ASD. The study found that posture repertoires were significantly more delayed in children who were later diagnosed with ASD than in those without ASD at 6, 9, and 12 months of age. Gernsbacher et al. (Gernsbacher et al., 2008) have assessed oral- and manual-motor skills of children with ASD and TD children at 6, 12, 18, 24, and 36 months of age by parental interview. The results showed that children with ASD demonstrated significantly lower scores of both oral- and manual-motor composite scores than did TD children (Gernsbacher et al., 2008). Besides, a prior study
longitudinally examined child’s fine motor skills at 6, 12, 18, 24, and 36 months of ages using a standardized motor assessment instrument in three groups of children, including children with ASD, TD children with low-risk or high-risk of developmental problems (Ozonoff et al., 2014). The results showed that fine motor scores in children with ASD were comparable to TD children groups at 6 months, but followed by a sharp decrease in scores that significantly lower than the TD children from ages 12 to 36 months.
The above-mentioned findings suggest that delayed motor development can be early detected in young children with ASD. However, there were very limited studies using the standardized motor assessment instruments for assessing motor development in children with ASD before 3 years of age. Besides, the existing studies only
demonstrated total motor scores instead of reporting subscale scores that may further help to understand multiple motor functions in young children with ASD.
2.3 Behavioral and motor development in very-low-birth weight (VLBW) preterm children
Except for young children with ASD, preterm children are a high risk group of
suffering multiple developmental problems in early childhood. Preterm children are defined as babies born alive before 37 weeks of pregnancy. The incidence of preterm birth worldwide has estimated ranges from 5% to 15% (Tielsch, 2015), whereas the incidence in Taiwan is relatively stable from 8.5% to 9.4ʘ from 2006 to 2015 (Health Promotion Administration, 2016). The sub-categories of preterm birth are based on gestational age (i.e., extremely preterm [< 28 weeks], very preterm [28 - 31 weeks], and moderate to late preterm [32 - 36 weeks]) and birth weight (i.e., extremely low birth weight [ELBW, birth weight < 1000 g], very low birth weight [VLBW, birth weight <
1500 g], and low birth weight [LBW, birth weight < 2500 g]) (Baron & Rey-Casserly, 2010). Literatures have highlighted that the risk of neurodevelopmental impairments is particularly evident in VLBW (Baron & Rey-Casserly, 2010; Bartlett & Piper, 1993;
Biasini et al., 2012; Hack et al., 1995) and ELBW preterm children (Hack et al., 2000;
Marlow, 2004; O'Callaghan et al., 1995; Rugolo, 2005; Tommiska et al., 2003).
Compared with term counterparts, VLBW preterm children are more likely to manifest developmental problems and sustain lifelong consequences (Johnson et al., 2009). From the previous reports, VLBW or ELBW preterm children have been found to show neuro-motor abnormalities (20% - 30%) (O'Callaghan et al., 1995; Rugolo, 2005;
Tommiska et al., 2003), visual function abnormalities (27.7%) and hearing impairment (15.3%) (van der Pal-de Bruin, van der Pal, Verloove-Vanhorick, & Walther, 2015).
Several developmental disabilities, such as cognitive problems (15 - 30%) (Hack et al., 2000; Marlow, 2004; O'Callaghan et al., 1995; Pugliese et al., 2013), motor deficits (10 - 40%) (Stoelhorst et al., 2003), language or social-communication impairments (7 - 42%) (Barre, Morgan, Doyle, & Anderson, 2011; Sansavini et al., 2010; Tommiska et al., 2003; Woodward et al., 2009), and behavioral problems (10 - 20%) (Farooqi, Hagglof, Sedin, Gothefors, & Serenius, 2007), have been frequently occurred in VLBW
preterm children.
Among developmental problems, behavioral problems are commonly observed in both VLBW and ELBW preterm children in middle childhood. At school ages,
internalizing behaviors (i.e., anxiety/depression, withdrawn, and somatic problems), attention, thought, and social problems have been developed in VLBW preterm children (Farooqi et al., 2007). Previous studies revealed that VLBW preterm children aged 6 - 16 years exhibited higher behavioral problems scores in inattention/ hyperactivities, depression/anxiety, withdrawal from social contacts than those in term-peers (Conrad, Richman, Lindgren, & Nopoulos, 2010; Whitfield, Grunau, & Holsti, 1997). At preschool ages, several studies reported an increased likelihood of total behavioral difficulties (OR = 1.9 - 2.4), hyperactivity (OR = 1.7 - 2.1), peer problems (OR = 1.5 - 1.8), and emotional problems (OR = 1.4 - 2.7) in very preterm children (gestational age:
22 – 32 weeks) at 3 and 5 years of age compared to term children (Delobel-Ayoub et al., 2009; Delobel-Ayoub et al., 2006). Furthermore, two previous studies (Reijneveld et al., 2006) had showed 7-13% of VLBW preterm children and 11-15 % of ELBW preterm children obtaining clinical range of scores in internalizing, externalizing and total behavioral problems with the mean age of 50 ± 2.6 months (Brown, Burns, Watter, Gibbons, & Gray, 2015; Reijneveld et al., 2006). Besides, the percentages of
aforementioned problems and four syndromes scores (i.e., somatic complaints, thought problems, attention problems, delinquent behavior) were significantly higher than that in term-peers. Moreover, Conrad et al. (Conrad et al., 2010) have reported an inverse relationship between birth weight and behavior outcomes (β = - 0.001, p < 0.002), which suggest that the lower birth weight of children, the more behavior and emotional problems. Besides, Wong et al (Wong et al., 2014) have found that VLBW preterm children aged 18.5 to 35.6 months performed more repetitive behaviors in lining,
spinning object, echolalia, and more difficulties in adaptation to change in routines than did term children.
In addition to abnormal behavioral developments, co-occurrence of motor deficits (22 - 32%) have been found as important developmental problems in VLBW preterm children (Hsu et al., 2013; Hus, Potharst, Visser, Kok, & Leemhuis, 2014). A
meta-analysis conducted in a prior study has indicated that motor problems in balance function, ball skills, and manual dexterity persistently occurred at school-aged VLBW preterm children (de Kieviet, Piek, Aarnoudse-Moens, & Oosterlaan, 2009). Compared to term counterparts, VLBW and ELBW preterm infants tend to exhibit delayed
acquisition of crawling, sitting, walking in early ages (Cahill-Rowley & Rose, 2016;
Ferrari et al., 2002; Pin et al., 2010; van Haastert et al., 2006). Therefore, it is important to examine the behavioral and motor development in VLBW preterm children to help early identify those who may later develop any developmental disorders.
2.3.1 VLBW preterm toddlers and the risk of developing ASD
Several previous studies indicated that VLBW preterm children may show autistic traits and symptoms at the young ages. More RRBs and social-communication
difficulties have been found in VLBW preterm children as compared to general
population (Wong et al., 2014). Among various neurodevelopmental disorders, ASD is one of comorbidities in VLBW preterm children (Johnson & Marlow, 2011). Previous studies have reported that VLBW preterm infants or preterm infant born with very low gestational age are increased risk of developing ASD (Hwang et al., 2013; Kuzniewicz et al., 2014; Lampi et al., 2012; Leavey et al., 2013; Limperopoulos et al., 2008).
Furthermore, higher prevalence of ASD have been found in preterm children than in full-term children. Recent estimates for ASD in a LBW preterm cohort is about 5%
(Pinto-Martin et al., 2011) and 8% in ELBW preterm cohort (Johnson et al., 2010). In a
study by Hwang et al. (Hwang et al., 2013), Autism was more prevalent in Taiwanese preterm children that the prevalence rates were 3.7 times higher in early preterm population and 2.2 times higher in late preterm population comparing to the prevalence rates in full-term population. Since preterm children might be at risk of developing ASD, a comparison of early development between preterm children and children with ASD could help inform early signs or autistic traits in preterm children that may be beneficial for early identification and diagnosis of ASD.
Previous studies reported that behavioral problems occurred in the early childhood might be early signs of ASD. The study conducted by Gray et al. (Gray et al., 2015) have found that 2-year-old very preterm children (birth weight: 1072 ± 326 g) with positive screening results of ASD obtained significantly higher externalizing and internalizing behaviors scores than that of those with negative screening. The other study conducted by Pritchard et al. (Pritchard et al., 2016) has assessed adaptive
behavior in 169 VLBW preterm children and screening of ASD at 2 and 4 years of age.
Children with positive screening result of ASD showed significantly higher rates of maladaptive behaviors than that of children with negative screening results
(ASD-positive vs. ASD-negative children = 68% vs. 13%, OR= 13.6). Furthermore, Johnson et al. (Johnson et al., 2010) have assessed behavioral problems in 219 extremely preterm children (gestational age Љ 26 weeks) at 2.5 and 6 years old, respectively. The results showed that higher behavioral problems scores were associated with a later diagnosis of ASD at 11 years of age. Therefore, behavioral assessment of VLBW preterm children in early childhood is important that more maladaptive behaviors and behavioral problems might increase risk for developing ASD.
In addition to associations between behavioral problems and ASD, several studies have shown that VLBW or EBLW preterm children displayed more delayed milestones,
more impaired gross and fine motor function than that of TD children in early childhood (Cahill-Rowley & Rose, 2016; de Kieviet et al., 2009; Ferrari et al., 2002; Pin et al., 2010; van Haastert et al., 2006). Furthermore, motor problems might be the early sign for ASD in VLBW preterm children. A prior study conducted by Gray et al. (Gray et al., 2015) have assessed motor function in very preterm children (birth weight: 1072 ± 326 g) at 2 years of age and all of children were screened for ASD. The results showed that very preterm children with lower motor scores were more likely to have a positive screen of ASD. The findings suggest that VLBW preterm children with more impaired motor development might increase the risk of developing ASD.
2.3.2 Behavioral and motor development between young children with ASD and ATD children
Although many studies have focused on motor and behavioral developments among preterm children in the early childhood, no studies have compared the motor and behavior developments of preterm children and those of ASD in early childhood. By contrast, several studies have compared young children with ASD and ATD children with different developmental problems. The findings of previous studies for
comparisons of behavioral development in children with ASD and ATD children were shown in Appendix C. Elison et al. (Elison et al., 2014) revealed that children with ASD at 12 months of age obtained significantly higher composite score of repetitive and stereotyped movement with body than that of children with high risk of developing ASD, whereas no significant difference between the scores of repetitive and stereotyped movements with object between the two groups. Furthermore, Morgan et al. (Morgan et al., 2008) have found children with ASD obtained significantly higher scores of
repetitive and stereotyped movement with body and objects than that of children with developmental delay at 18 and 24 months of age. Moreover, Watt et al. (Watt et al.,
2008) showed higher duration of repetitive and stereotyped movements with objects, body, and abnormal sensory behaviors in 18- to 24-months-old children with ASD than that of children with developmental delay.
In addition to repetitive and stereotyped movement, Richler et al. (Richler et al., 2007) have assessed more dimensions of RRBs in children with ASD (n = 165), children with global developmental delay (n = 49) at 2 years of age. The children with ASD showed higher prevalence in the following behaviors: unusual preoccupations (OR
= 4.04); unusual sensory interests (OR = 4.12); repetitive use of objects (OR = 5.04);
hand and finger mannerisms (OR = 4.69); complex mannerisms (OR = 7.29); abnormal/
idiosyncratic response to sensory stimuli (OR = 2.92); difficulties with change (OR = 2.53); unusual attachments (OR = 2.69); and compulsions and rituals (OR = 3.67) as compared with children with global developmental delay. Besides, the percentages of showing any form of RRBs were significantly higher in 8- to 56-month-old children with ASD than in ATD children (Kim & Lord, 2010). All of the findings suggest that abnormal pattern of RRBs frequently occurred in children with ASD than in ATD children. Although several previous studies have compared the motor and behavioral development in young children with ASD with ATD children, none has investigated developmental differences between VLBW preterm children and children with ASD.
Considering the necessity of early identification of autistic traits in VLBW preterm children who are at risk of developing ASD, examining the differences and similarities in motor and behavioral development between VLBW preterm children and children with ASD is warranted.
In addition to behavioral development, previous studies indicated that children with ASD demonstrated more impaired motor function than that of ATD children. The articles for comparisons of motor development in children with ASD and ATD were
shown in Table 4. Provost et al. (Provost et al., 2007) have examined gross and fine motor development among three groups of children aged 21 to 41 months, including children with ASD, ATD children with developmental delay, and children with motor delay. The results showed that the motor scores in children with ASD were comparable to children with motor delay, whereas children with ASD obtained significantly lower motor scores than that of children with developmental delay. The other study conducted by Waelvelde et al. (Waelvelde et al., 2010) have assessed motor development in 4- to 6-year-old children with ASD and ATD children without motor problems using the Movement Assessment Battery for Children (M-ABC). The results revealed that children with ASD demonstrated a significantly lower MABC percentile scores than that of ATD children (ASD vs. ATD = 3.1 ± 3.8 vs. 7.1 ± 4.4, p = 0.02). Furthermore, two studies conducted by Maston et al. (Matson, Mahan, Fodstad, Hess, & Neal, 2010;
Matson, Mahan, Kozlowski, & Shoemaker, 2010) have examined motor developments among 17- to 36-month-old children with Autistic disorder, children with PDD-NOS and ATD children (had a diagnosis of developmental delay, intellectual disability or language disorders etc.). The results showed that the onsets of crawling in the AD group were significantly later than that of PDD-NOS and ATD groups, whereas the onsets of crawling in children with PDD-NOS was comparable to that of ATD children group.
Furthermore, lower gross (effect size = 0.21) and fine motor scores (effect size = 0.31) were found in children with AD than in ATD children, whereas children with PDD-NOS had comparable gross motor scores but lower fine motor score than those of ATD children (Matson, Mahan, Fodstad, et al., 2010).
However, Lane et al. (Lane, Harpster, & Heathcock, 2012) retrospectively collected the motor data in children with ASD (n = 8) and ATD children (n = 22;
including children with global developmental delay, language delay, hypotonia, apraxia
of speech, or hearing loss). The results revealed that children with ASD tend to show lower motor composite scores than did ATD children but the result was not statistically significant that may be due to a small sample size. In conclusion, children with ASD may be characterized as motor delay in early childhood, and may have more impaired motor development than that of ATD children.
Chapter III. Method 3.1 Participants
Three groups of toddlers aged 24 – 36 months were recruited in this study, including 15 FT-ASD toddlers, 15 FT-TD toddlers, and 30 VLBW-PT toddlers. The FT-ASD toddlers were enrolled from the outpatient clinic of Pediatric Rehabilitation at the National Taiwan University Hospital (NTUH) and the outpatient clinic of Psychiatry at the NTUH Hsin-Chu Branch. The inclusion criteria for the children with ASD were: 1) having a clinical diagnosis of ASD at enrollment; 2) full-term gestation with gestational age Њ 37 weeks and birth weight > 2500 g; 3) absence of congenital anomalies, chromosome abnormalities, major sensory or neurological impairments/ disorders (e.g., microcephalus, macrocephalus, seizure, epilepsy, cerebral palsy, uncorrected visual or hearing loss, or severe brain damage) were excluded from this study.
The VLBW-PT toddlers were recruited from a birth cohort research project which is a randomized control trail of an early intervention program for Taiwanese VLBW preterm infants. The VLBW preterm infants were randomly assigned in the intervention or control groups that the infants in the former received a family-centered intervention program and the latter received a usual care program from birth to one year of age. Only the first child of twins or triplets were introduced in the intervention project. For those siblings who did not attend any research projects, we invited them to participate the present study. The inclusion criteria for the preterm children including: 1) gestational age < 37 weeks and birth weight < 1500 g; 2) absence of severe perinatal or neonatal diseases (e.g., seizures, hydrocephalus, ventriculoperitoneal shunt, meningitis, periventricular leukomalacia, grade III-IV intraventricular hemorrhage; stage IV-V retinopathy of prematurity and grade II necrotizing enterocolitis).
The FT-TD toddlers were recruited by distribution of flyer via church,
kindergartens, and the websites of Early Intervention Service Reporting and Referral Center. The inclusion criteria for the FT-TD toddlers including: 1) full-term gestation with gestational age Њ 37 weeks and birth weight > 2500 g; 2) without any clinical diagnosis or history of developmental disabilities. Moreover, there were 2 selection criteria for parents including: 1) parental age Њ 20 years at child birth; and 2) parents have a minimum 9 years of education year that can read Chinese.
Considering the sample size in the present study, the projected sample size is calculated as 11 per group based on child motor function as previously reported for the children with ASD and ATD children (motor standard score: 7.6 ± 1.2 vs. 9.0 ± 6.9, p = 0.01) at 30 months of age by Provost et al. (Provost et al., 2007). Accounting for 10% of the attrition rate in attending developmental assessments at 30 or 36 months of age, at least 15 toddlers each group was appropriate while the statistical power is set to be 80%
and α level set at 0.05. The Mann-Whitney U test was used to analyze the difference among groups on behavioral and motor development. The study has been approved by the Ethnics Committee of the NTUH. Informed consent was obtained from parents before participation in this study.
3.2 Experimental procedures
After obtaining agreements from parents, birth and demographic data will be extracted from a basic demographic form (Appendix F) written by parents or will be abstracted from child’s medical record. The birth data include child’s birth weight and gestational age; and demographic data include child’s age, sex, parental ages at child birth, parental education and occupation, and total hours of receiving developmental intervention per week. Parental education and occupation was transformed to the SES index using the formula reported by Chang et al. (Chang, Lee, Tseng, & Wang, 2011)
The SES index are classified into high (SES index: 11 - 29), moderate (SES index: 30 – 40) and low level (SES index: 41 - 55).
The participating toddlers received one time of developmental assessments at 30 or 36 months of age depending on child’s age at enrollment. All participants were assessed the cognitive level using the Mullen Scales of Early Learning (MSEL) and were
examined whether any differences of cognitive function among 3 groups of children.
Child’s motor functions were measured by the PDMS-II that consists of 5 subscales including Stationary, Locomotion, Object Manipulation, Grasping, and Visual-Motor Integration. Child’s behavioral functions were reported by parents’ observation for child’s behavioral problems using the Chinese version of CBCL/1.5–5 and RBS-R (Appendix G). Furthermore, child’s behaviors in free play situations were tracked automatically via an automated behavioral tracking system. Several time- and space-related variables relevant to the behavior trajectory were measured. All the assessments were completed in 1 or 2 times of laboratory visit.
3.3 Measurements Assessment of cognition
Mullen Scales of Early Learning (MSEL) The MSEL is a comprehensive
norm-referenced developmental test for children aged from 0 to 68 months (Mullen, 1995). The instrument contains 5 subscales: Visual Reception, Expressive Language, Receptive Language, Fine Motor and Gross Motor scales. The former 4 subscales are combined to yield an Early Learning Composite (ELC) composite score with a mean of 100 and standard deviation of 15as representing overall cognitive function. The scores for each testing item ranged from 0 - 2 to 0 - 5. The raw score of each subscale can be converted to standard T scores, percentile, and developmental-equivalent ages for comparison with the data in a normative samples of 1,849 children residing in 46 areas
of US aged 2 days - 69 months. Good internal consistency (Cronbach’s α = 0.75-0.80), 1- to 2-week test-retest (ICCs = 0.71 - 0.96), and inter-rater reliabilities (ICCs = 0.91 - 0.99), and moderate to high correlations with the Bayley Mental Development Index (r
= 0.53 – 0.59) and the Peabody Fine Motor Scale (r = 0.65 – 0.82) in assessment of young children with ASD have been reported (Mullen, 1995). In addition, previous studies showed the MSEL had acceptable discriminative validity that children with ASD performed lower standard scores of 5 subscales than that of TD children (Akshoomoff, 2006; Burns, King, & Spencer, 2013; Hellendoorn et al., 2015) and children with other developmental delay/ disorders (Hellendoorn et al., 2015).
Assessment of motor function
Peabody Developmental Motor Scales, Second Edition (PDMS-2) It is a
norm-referenced assessment composed of 6 subscales, including Reflexes (for children birth through 11 months), Stationary (ability to sustain control of body within its center of gravity), Locomotion (ability to move from one place to another), Object
Manipulation (ability to manipulate balls, for children 12 months and older), Grasping (ability to use hands), and Visual-Motor Integration (ability to use visual perceptual skills to perform complex eye–hand coordination tasks) for evaluating multiple
dimensions of motor functions in children through the ages of 0 to 5 years (Agarwal &
Lim, 2003). The scores for each item are from 0 - 2 (0: the child cannot or will not attempt the item or the attempt does not indicate that the skill is emerging; 1: the child’s performance indicates a clear resemblance to the item mastery criteria but does not fully meet the criteria; and 2: the child performs the item according to the criteria specified for mastery). The raw score of 6 subscales can be converted to
developmental-equivalent ages, standard scores, and percentiles based on normative samples of 2,003 children aged 0 - 71 months residing in 46 areas of US and Canada.
The standard scores of 6 subscales are summed up as the total composite standard scores and are converted to Total Motor Quotient (TMQ). The summed standard scores in Stationary, Locomotion, and Object Manipulation standard scores can be converted to the Gross Motor Composite Quotient (GMQ) and the rests are for the Fine Motor
Composite Quotient (FMQ). Excellent internal consistency (Cronbach’s α = 0.90 - 0.98) and 1-week test-retest reliability (ICCs = 0.73 - 0.99) (Agarwal & Lim, 2003; Tavasoli, Azimi, & Montazari, 2014), as well as good convergent validity with the Psychomotor Development Index of Bayley Scales of Infant Development, second edition (r = 0.91 - 0.93) (Tavasoli et al., 2014).
Assessment of behavioral function
Child Behavior Checklist for Ages 1.5-5 (CBCL/1.5–5) It is a parental report of child
behavioral, emotional and social functioning at ages 1.5 – 5 years, consists of 100 items, in which 99 items assess specific behavior problems and one item is blank for parents to note child behavior problems not listed in the questionnaire (Achenbach, 2000). Each item is scored on a 3-point scale (0 as ‘‘not true of the child,’’ 1 as ‘‘somewhat or sometimes true,’’ and 2 as ‘‘very true or often true’’). The sum of the 100 items is counted as the Total Problems score, whereas 67 of them were scored specifically to Empirically-Based scales including seven Narrow-Band syndromes, such as,
Emotionally Reactive (9 items), Anxious/Depressed (8 items), Somatic Complaints (11 items), Withdrawn (8 items), Sleep Problems (7 items), Attention Problems (5 items), and Aggressive Behavior (19 items). In addition, two Broad-Band scales are derived, with the former 4 syndromes constituting the Internalizing Problems and the latter 2 syndromes constituting the Externalizing Problems. Besides, 45 of them were scored specifically to 5 DSM-Oriented Scales, including Affective Problems (10 items), Anxiety Problems (10 items), Pervasive Developmental Problems (13 items), Attention