Manuscript Number:
Title: Spinal anesthesia with diphenhydramine and pheniramine in rats Article Type: Research Paper
Section/Category: Neuropharmacology and analgesia
Keywords: diphenhydramine; pheniramine; lidocaine; spinal anesthesia Corresponding Author: Associate Professor Yu-Wen Chen, Ph.D.
Corresponding Author's Institution: China Medical University First Author: Ching-Hsia Hung, Ph.D.
Order of Authors: Ching-Hsia Hung, Ph.D.; Chin-Chen Chu, M.D., Ph.D.; Yu-Chung Chen, M.S.; Yu-Wen Chen, Ph.D.; Zong-Ying Li, B.S.; Jhi-Joung Wang, M.D., Ph.D.
Abstract: The aim of this study was to evaluate the effects of pheniramine and diphenhydramine, two histamine H1 receptor antagonists, on spinal anesthesia and their comparison with lidocaine, a commonly used local anesthetic. After rats were injected intrathecally with diphenhydramine and pheniramine, the dose—response curves were obtained. The potency and duration of
diphenhydramine and pheniramine on spinal anesthesia were compared with lidocaine. We showed that diphenhydramine and pheniramine produced dose-dependent spinal blockades in motor function, proprioception, and nociception. On a 50% effective dose (ED50) basis, the rank of potency of drugs was diphenhydramine = pheniramine > lidocaine (p < 0.05 for the differences). In equianesthetic doses (ED25, ED50, and ED75), the block duration caused by diphenhydramine was longer than that caused by pheniramine or lidocaine (p < 0.01 for the differences). Diphenhydramine, but not pheniramine or lidocaine, elicited longer duration of sensory block than that of motor block at the same dose of 1.75 μmol. These preclinical data reported that diphenhydramine with a more sensory-selective action over motor blockade demonstrated more potent and longer-lasting spinal blockades, compared with pheniramine or lidocaine.
1
Spinal anesthesia with diphenhydramine and pheniramine in rats
Ching-Hsia Hunga, Chin-Chen Chub, Yu-Chung Chenc, Yu-Wen Chenb,d,*, Zong-Ying Lid, Jhi-Joung Wangb
a Institute & Department of Physical Therapy, National Cheng Kung University, Tainan, Taiwan
b Department of Medical Research, Chi-Mei Medical Center, Tainan, Taiwan
c Division of Physical Therapy, Department of Physical Medicine and Rehabilitation, Cheng Hsin General Hospital, Taipei, Taiwan
d Department of Physical Therapy, China Medical University, Taichung, Taiwan
Conflicts of interest: There is no conflict of interests for all authors.
* Address correspondence and reprint requests to: Yu-Wen Chen, PhD, Department of Physical Therapy, China Medical University, No.91 Hsueh-Shih Road, Taichung 40402, Taiwan
Tel: 886-4-22053366 ext 7327 Fax: 886-4-22065051
E-mail: [email protected]
ABSTRACT
The aim of this study was to evaluate the effects of pheniramine and diphenhydramine, two histamine H1 receptor antagonists, on spinal anesthesia and their comparison with lidocaine, a commonly used local anesthetic. After rats were injected intrathecally with diphenhydramine and pheniramine, the dose—response curves were obtained.
The potency and duration of diphenhydramine and pheniramine on spinal anesthesia were compared with lidocaine. We showed that diphenhydramine and pheniramine produced dose-dependent spinal blockades in motor function, proprioception, and nociception. On a 50% effective dose (ED50) basis, the rank of potency of drugs was diphenhydramine = pheniramine > lidocaine (p < 0.05 for the differences). In
equianesthetic doses (ED25, ED50, and ED75), the block duration caused by
diphenhydramine was longer than that caused by pheniramine or lidocaine (p < 0.01 for the differences). Diphenhydramine, but not pheniramine or lidocaine, elicited
longer duration of sensory block than that of motor block at the same dose of 1.75 μmol. These preclinical data reported that diphenhydramine with a more
sensory-selective action over motor blockade demonstrated more potent and longer-lasting spinal blockades, compared with pheniramine or lidocaine.
Key Words: diphenhydramine; pheniramine; lidocaine; spinal anesthesia
1. Introduction
Diphenhydramine and pheniramine, two histamine H1 receptor antagonists, are widely used antihistaminics (Estelle and Simons, 1999; Pullman et al., 1975; Sharma and Hamelin, 2003) and have antipruritic effects (Pavlidakey et al., 2009).
Diphenhydramine is a first generation antihistamine mainly used to treat allergies and may act as an antiemetic, sedative and hypnotic (Pavlidakey et al., 2009; Shepherd, 2011). Diphenhydramine also has the local anesthetic properties (Steffen et al., 1956),
and has been used successfully as a local cutaneous anesthetic when allergies to other local anesthetic agents exist (Pollack and Swindle, 1989). From that time onwards, there is a growing body of evidence that diphenhydramine had topical ocular and dermal local anesthetic properties (Green et al., 1994; Pavlidakey et al., 2009;
Suffridge et al., 2009).
Diphenhydramine has been shown to have the characteristic of the blockade of Na+ currents (Kim et al., 2000; Kuo et al., 2000), which is one of the major
mechanisms of local anesthesia, produces spinal anesthesia, peripheral nerve block, and infiltrative cutaneous analgesia (McLure and Rubin, 2005). However, to the best of our knowledge, no study of diphenhydramine or pheniramine on spinal anesthesia has been reported to date. Spinal anesthesia is a relatively simple technique, which brings competent surgical conditions by the injection of a small amount of local
anesthetic with easy landmarks, giving a wide popularity to this practice (Vandermeersch et al., 1991). The aim of this study was to evaluate the spinal anesthesia following intrathecal injections of diphenhydramine and pheniramine by testing motor function, proprioception, and nociception on rats. Lidocaine, a known local anesthetic, was used as control.
2. Materials and methods
2.1. Animals
The experiment was approved by the Institutional Animal Care and Use
Committee of China Medical University, Taiwan on 11 January 2010 and conformed to the recommendations and policies of the International Association for the Study of Pain (IASP). Two hundred and sixteen male Sprague-Dawley rats weighting
300-350g were obtained from the National Laboratory Animal Centre in Taiwan, and then housed in a climate controlled room maintained at 21℃ with approximately 50%
relative humidity. Lighting was on a 12-h light/dark cycle (light on at 6:00 AM), with food and water available ad libitum up to time of the experiment.
2.2. Drugs
Diphenhydramine HCl, pheniramine maleate, and lidocaine HCl monohydrate were purchased from Sigma-Aldrich Chemical Co. (St. Louis, MO, USA). All drugs in stock were freshly prepared in 5% dextrose as solution before intrathecal injections.
After injections, the low pH of these plain solutions (range, 6.0–6.5) is likely to be buffered quickly by the cerebral spinal fluid (pH 7.4).
2.3. Experimental protocols
Three specific experiments were carried out. In experiment 1, the effects of diphenhydramine (0.30, 0.60, 0.90, 1.50, 1.75 µmol), pheniramine (0.40, 0.75, 0.90,
1.50, 1.90 µmol), lidocaine (0.50, 0.75, 1.00, 1.50, 2.50 µmol), and vehicle (5%
dextrose) on spinal block were evaluated (n=8 rats for each dose of each drug). In experiment 2, the spinal block effect of diphenhydramine or pheniramine was
compared with that of lidocaine at the same dose of 1.75 μmol (n=8 rats for each dose of each drug). In experiment 3, on an equipotent basis (ED25, ED50 and ED75), the duration of lidocaine on spinal anesthesia was compared with that of
diphenhydramine or pheniramine (n=8 rats for each dose of each drug).
2.4. Spinal anesthesia by intrathecal injections of drugs
All animals were injected intrathecally one time in this study. Lumbar puncture was done on conscious rats. Before the intrathecal injections, local anesthesia was given. Following an optimal flexion of the rat lumbar spine under prone position, each 50-µl of 0.5% lidocaine was injected into the right- and left- side of paraspinal space (0.5 cm in depth) which was 0.5 cm away from the mid-point of the longitudinal line of L4–5 intervertebral space (Chen et al., 2010b; Leung et al., 2010). Two minutes later, a 27-gauge needle attached to a 50-µl syringe (Hamilton, Reno, Nevada) was inserted into the mid-line of the L4–5 intervertebral space until a tail-flick indicated entrance into the intrathecal space. Fifty microliters of drug were injected and the rat was observed for the development of spinal blockade, indicated by paralysis of both hind limbs. Rats, which demonstrated unilateral blockade, were excluded from the
study and sacrificed by using an over dose of isoflurane.
2.5. Neurobehavioral evaluation
After intrathecal injection of drug, three neurobehavioral evaluations, which consisted of evaluations of motor, proprioception, and nociception, were conducted (Chen et al., 2007; Chen et al., 2010a). For consistency, a trained examiner who was blinded to the treatment groups was responsible for handling of all animals and behavioral examinations. Rats were evaluated before medication and at 1, 5, and 10 min afterwards, then again at 10-min interval until 1 h and at 15 min interval until 2 h.
The magnitude of spinal blockade in motor function, proprioception, and nociception was described as the percentage of possible effect (% PE). The maximum blockade in a time course of spinal anesthesia of drugs was described as the percent of maximal possible effect (% MPE).
In brief, nociception was evaluated by the withdrawal reflex elicited by pinching a skin fold over each rat's back at 1 cm from the proximal part of the tail, the lateral metatarsus of bilateral hind limbs, and the dorsal part of the mid-tail. At each testing time, only one pinch was given to each of the four testing sites, and the time interval between stimulations at different sites was around 2 s. The nociceptive blockade was graded as 4 (normal or 0% MPE), 3 (25% MPE), 2 (50% MPE), 1 (75% MPE), and 0 (absent or 100% MPE) (Chen et al., 2004; Hung et al., 2009).
Proprioception evaluation was based on the resting posture and postural reactions (‘tactile placing’ and ‘hopping’). This test was performed by lifting the front half of
the animal off the ground and lifting one hind limb at a time off the ground so that the animal was standing on just one limb. Then, the animal was moved laterally, which normally evoked a prompt hopping response with the weight-bearing limb in the direction of movement to prevent the animal from falling. A predominantly proprioceptive block causes a delayed hopping followed by greater lateral hops to prevent the animal from falling. The functional deficit was graded as 3 (normal or 0%
MPE), 2 (slightly impaired), 1 (severely impaired), and 0 (completely impaired or 100% MPE) (Chen et al., 2004; Hung et al., 2009).
Motor function was evaluated by measuring 'the extensor postural thrust' of the right hind limb of each rat. The extensor thrust was measured as the gram force, which resisted contacting the platform by the rat heel applied to a digital platform balance (Mettler Toledo, PB 1502-S, Switzerland). The reduction in this force, representing reduced extensor muscle tone, was considered as a deficit of motor function and expressed as a percentage of the control force. The preinjection control value was considered as 0% motor block or 0% maximal possible effect (% MPE). A force less than 20 g (also referred to as the weight of the 'flaccid limb') was
interpreted as the absence of extensor postural thrust or a 100% motor block or 100%
MPE (Leung et al., 2010; Thalhammer et al., 1995).
2.6. Effective doses (EDs)
After intrathecally injecting the rats with four different doses of each drug (n = 8 for each dose of each drug), the dose—response curve was constructed. The curve was then fitted using a SAS Nonlinear (NLIN) Procedures (SAS Institute Inc., Carey, NC), and the value of 50% effective dose (ED50), defined as the dose that caused 50%
spinal anesthesia, were obtained (Chen et al., 2011a; Minkin and Kundhal, 1999). The ED25 or ED75 of drug was obtained by the same curve-fitting (SAS NLIN Procedures) which was used to derive the ED50 (Chen et al., 2011b; Minkin and Kundhal, 1999).
The full recovery time, defined as the interval from injection to full recovery, caused by each drug (n = 8 rats for each dose of each drug) was evaluated on an equipotent basis (ED25, ED50 and ED75). In this study, we also evaluated the %MPE, complete blockade time, time to full recovery, area under curves (AUCs) of motor,
proprioception and nociception for diphenhydramine, pheniramine, and lidocaine at the same dose of 1.75 μmol. The AUC of spinal blockade of drug was obtained by using Kinetica v 2.0.1 (MicroPharm International, USA).
2.7. Statistical analysis
Data are presented as means ± S.E.M. or ED50 values with 95% confidence interval (95% CI). Values were evaluated by either 1-way (experiments 1 and 2) or
2-way (experiment 3) analysis of variance (ANOVA) followed by pairwise Tukey's honest significance difference (HSD) test. A statistical software, SPSS for Windows (version 17.0, SPSS, Inc, Chicago, IL, USA), was used, and a P value less than 0.05 was considered statistically significant.
3. Results
3.1. The spinal blockade of diphenhydramine and pheniramine
Diphenhydramine and pheniramine, as well as lidocaine, displayed
dose-dependent effects on spinal anesthesia in rats (Fig. 1). Intrathecal injection of 5%
dextrose (vehicle) produced no spinal anesthetic effects (data not shown). The ED50s of drugs are shown in Table 1. On the ED50 basis, the ranks of potencies in motor function, proprioception, and nociception were diphenhydramine = pheniramine >
lidocaine (P < 0.05; Table 1). Furthermore, the sensory/nociceptive blockade (ED50) was more potent than the motor blockade for diphenhydramine, but not lidocaine or pheniramine (P < 0.05; Table 1).
3.2. The spinal blockade of diphenhydramine, pheniramine, and lidocaine at the
dose of 1.75 μmol
At a given dose of 1.75 μmol, diphenhydramine showed 100, 100, and 100% of
blockades (% MPE) in motor function, proprioception, and nociception with duration of action of about 41, 56, and 88 min, respectively (Fig. 2). Pheniramine at 1.75 μmol demonstrated 94, 92, and 94% of blockades in motor function, proprioception, and nociception with duration of action of about 25, 28, and 35 min, respectively. At the same given dose, lidocaine displayed 74, 75, and 81% of blockades in motor function, proprioception, and nociception with duration of action of about 19, 19, and 23 min,
respectively (Fig. 2 and Table 2). Of note, diphenhydramine at 1.75 μmol elicited
complete spinal blockade (100% MPE) of motor function, proprioception, and nociception (Fig. 2 and Table 2).
3.3. The complete block time, full recovery time, and AUCs of diphenhydramine, pheniramine, and lidocaine on spinal anesthesia
The complete block time, time to full recovery, and AUCs of spinal anesthesia of diphenhydramine are significantly greater than those of pheniramine or lidocaine in Figure 2 and Table 2. In addition, diphenhydramine also elicited longer duration of
sensory blockade than that of motor blockade (Table 2). On an equipotent basis (ED25, ED50, and ED75), all drugs tested produced similar duration in motor blockades, but the blockades of proprioception and nociception caused by diphenhydramine were longer than those caused by pheniramine or lidocaine (Fig. 3).
4. Discussion
We reported that diphenhydramine and pheniramine produced dose-dependent spinal anesthesia in rats. Diphenhydramine was more potent at producing spinal blockades than pheniramine or lidocaine. At equianesthetic doses, diphenhydramine displayed the longest duration of action of sensory/nociceptive block among these three drugs.
In this study, diphenhydramine and pheniramine blocked motor, sensory, and proprioceptive functions, suggesting the spinal (local) anesthetic characteristics of diphenhydramine and pheniramine. It has been known that local anesthetics produce neural blockade by inhibiting the sodium currents in the nervous tissues through the voltage-gated sodium channels (McLure and Rubin, 2005). Because diphenhydramine blocked sodium channels (Kim et al., 2000; Kuo et al., 2000), it produced dermal local anesthesia (Green et al., 1994), topical anesthesia (Suffridge et al., 2009), and spinal anesthesia. Although the pharmacology of pheniramine is largely unknown, our study showed that pheniramine produced a dose-dependent spinal anesthetic effect.
We showed that diphenhydramine, pheniramine, and lidocaine produced dose-dependent spinal anesthesia. Diphenhydramine produced almost 1.1- and 1.4-folds higher potency than did pheniramine or lidocaine on spinal anesthesia, respectively. Our results are in agreement with that previous injection of lesser
diphenhydramine (20mg) dose with venous occlusion can be considered as an alternative to larger lidocaine (40mg) dose in decreasing the prevalence of pain caused by injection of propofol into forearm veins (Apiliogullari et al., 2007).
Antihistamines are easily available medications. On an equal mole basis (1.75 μmol), spinal block duration of diphenhydramine was longer than that of pheniramine
or lidocaine (Fig. 2 and Table 2). Among these three drugs, diphenhydramine elicited predominantly nociceptive-specific blockades. In addition, diphenhydramine
produced a longer duration of sensory blockade than the motor blockade (Fig. 2 and Fig. 3). Furthermore, we found that the nociceptive blockade (ED50) was more potent than the motor blockade (ED50) for diphenhydramine, but not pheniramine or
lidocaine. The sensory/nociceptive blockade in diphenhydramine was almost 1.2-folds higher potency (ED50) than the motor blockade. Clinically, local anesthetics have mostly been used to assist with complete blockage of pain and not to augment potency.
Surgery by injecting long-acting local anesthetics is frequently practiced (Job et al., 1979). There are few cases where ultrashort spinal anesthesia is needed, and for
these they use 2-chloroprocaine, lidocaine or mepivacaine clinically. For this reason, we evaluated diphenhydramine, pheniramine, and lidocaine at equianesthetic doses (ED25, ED50, and ED75). Our results demonstrated that the duration of spinal blockade
caused by diphenhydramine was longer than that caused by pheniramine or lidocaine on an equipotent basis (Fig. 3). Treatment with local anesthetics (e.g.
diphenhydramine) for surgery or postoperative pain control may be worth studied in the future.
Our study has some limitations. We did not evaluate whether
diphenhydramine and pheniramine had neurotoxicity, however, it is noteworthy that in neurobehavioral studies we detected no apparent side effects after drug injection.
Although we used diphenhydramine at 1.75 µmol (1.0%) to elicit complete spinal block, Suffridge et al. have proved that all 5% diphenhydramine-treated eyes showed no toxic effects on the corneal epithelium on New Zealand rabbits (Suffridge et al., 2009). Histologic studies must be performed in the future before the possible use of
diphenhydramine and pheniramine as spinal analgesic in humans.
In conclusion, the preclinical data reported that diphenhydramine and pheniramine elicited local anesthetic effects on spinal anesthesia in rats.
Diphenhydramine with a more sensory-selective action over motor blockade is more potent and longer spinal block duration than pheniramine or lidocaine. The neural block potential by diphenhydramine and pheniramine is worth studying in the further.
Acknowledgements
The authors gratefully acknowledge the financial support provided for this study by the National Science Council of Taiwan (NSC 99-2815-C-039-038-B; NSC 99-2314-B-039-013-MY3).
References
Apiliogullari, S., Keles, B., Apiliogullari, B., Balasar, M., Yilmaz, H., Duman, A., 2007. Comparison of diphenhydramine and lidocaine for prevention of pain after injection of propofol: a double-blind, placebo-controlled, randomized study. Eur J Anaesthesiol 24, 235-238.
Chen, Y.W., Chen, Y.C., Lin, C.N., Chu, C.C., Lin, M.T., Wang, J.J., Kao, C.H., 2007.
The spinal anaesthetic effect of dextromethorphan, dextrorphan, and 3-methoxymorphinan. Eur J Pharmacol 569, 188-193.
Chen, Y.W., Chu, C.C., Chen, Y.C., Hung, C.H., Hsueh, M.I., Wang, J.J., 2011a.
Clonidine as adjuvant for oxybuprocaine, bupivacaine or dextrorphan has a significant peripheral action in intensifying and prolonging analgesia in response to local dorsal cutaneous noxious pinprick in rats. Neurosci Lett 496, 186-190.
Chen, Y.W., Chu, C.C., Chen, Y.C., Wang, J.J., Hung, C.H., 2010a. The
dose-dependent study of verapamil and diltiazem on spinal anesthesia in the rat.
Neurosci Lett 482, 76-80.
Chen, Y.W., Chu, C.C., Chen, Y.C., Wang, J.J., Hung, C.H., 2010b. Isobolographic analysis of caramiphen and lidocaine on spinal anesthesia in rats. Neurosci Lett 469, 174-178.
Chen, Y.W., Chu, C.C., Chen, Y.C., Wang, J.J., Hung, C.H., 2011b. The local anesthetic effect of memantine on infiltrative cutaneous analgesia in the rat.
Anesthesia and analgesia 113, 191-195.
Chen, Y.W., Huang, K.L., Liu, S.Y., Tzeng, J.I., Chu, K.S., Lin, M.T., Wang, J.J., 2004.
Intrathecal tri-cyclic antidepressants produce spinal anesthesia. Pain 112, 106-112.
Estelle, F., Simons, R., 1999. H1-receptor antagonists: safety issues. Ann Allergy Asthma Immunol 83, 481-488.
Green, S.M., Rothrock, S.G., Gorchynski, J., 1994. Validation of diphenhydramine as a dermal local anesthetic. Ann Emerg Med 23, 1284-1289.
Hung, C.H., Wang, J.J., Chen, Y.C., Chu, C.C., Chen, Y.W., 2009. Intrathecal oxybuprocaine and proxymetacaine produced potent and long-lasting spinal anesthesia in rats. Neurosci Lett 454, 249-253.
Job, C.A., Fernandez, M.A., Dorph, D.J., Betcher, A.M., 1979. Inguinal hernia repair.
Comparison of local, epidural, and general anesthesia. N Y State J Med 79, 1730-1733.
Kim, Y.S., Shin, Y.K., Lee, C., Song, J., 2000. Block of sodium currents in rat dorsal root ganglion neurons by diphenhydramine. Brain Res 881, 190-198.
Kuo, C.C., Huang, R.C., Lou, B.S., 2000. Inhibition of Na(+) current by
diphenhydramine and other diphenyl compounds: molecular determinants of selective binding to the inactivated channels. Mol Pharmacol 57, 135-143.
Leung, Y.M., Wu, B.T., Chen, Y.C., Hung, C.H., Chen, Y.W., 2010. Diphenidol inhibited sodium currents and produced spinal anesthesia. Neuropharmacology 58, 1147-1152.
McLure, H.A., Rubin, A.P., 2005. Review of local anaesthetic agents. Minerva Anestesiol 71, 59-74.
Minkin, S., Kundhal, K., 1999. Likelihood-based experimental design for estimation of ED50. Biometrics 55, 1030-1037.
Pavlidakey, P.G., Brodell, E.E., Helms, S.E., 2009. Diphenhydramine as an alternative local anesthetic agent. J Clin Aesthet Dermatol 2, 37-40.
Pollack, C.V., Jr., Swindle, G.M., 1989. Use of diphenhydramine for local anesthesia in "caine"-sensitive patients. J Emerg Med 7, 611-614.
Pullman, B., Courriere, P., Berthod, H., 1975. Quantum mechanical study on the conformational properties of antihistaminic drugs. Mol Pharmacol 11, 268-279.
Sharma, A., Hamelin, B.A., 2003. Classic histamine H1 receptor antagonists: a critical review of their metabolic and pharmacokinetic fate from a bird's eye view. Curr Drug Metab 4, 105-129.
Shepherd, G., 2011. Diphenhydramine dose response. Clin Toxicol (Phila) 49, 57.
Steffen, C.G., Zimmerman, M., Mihan, R., 1956. Diphenhydramine hydrochloride as a local anesthetic agent. AMA Arch Derm 74, 76-79.
Suffridge, P.J., Wiggins, M.N., Landes, R.D., Harper, R.A., 2009. Diphenhydramine as a topical ocular anesthetic. Can J Ophthalmol 44, 181-184.
Thalhammer, J.G., Vladimirova, M., Bershadsky, B., Strichartz, G.R., 1995.
Neurologic evaluation of the rat during sciatic nerve block with lidocaine.
Anesthesiology 82, 1013-1025.
Vandermeersch, E., Kick, O., Mollmann, M., de Gouw, N., Van Aken, H., 1991.
[CSE--the combination of spinal and epidural anesthesia]. Reg Anaesth 14, 108-112.
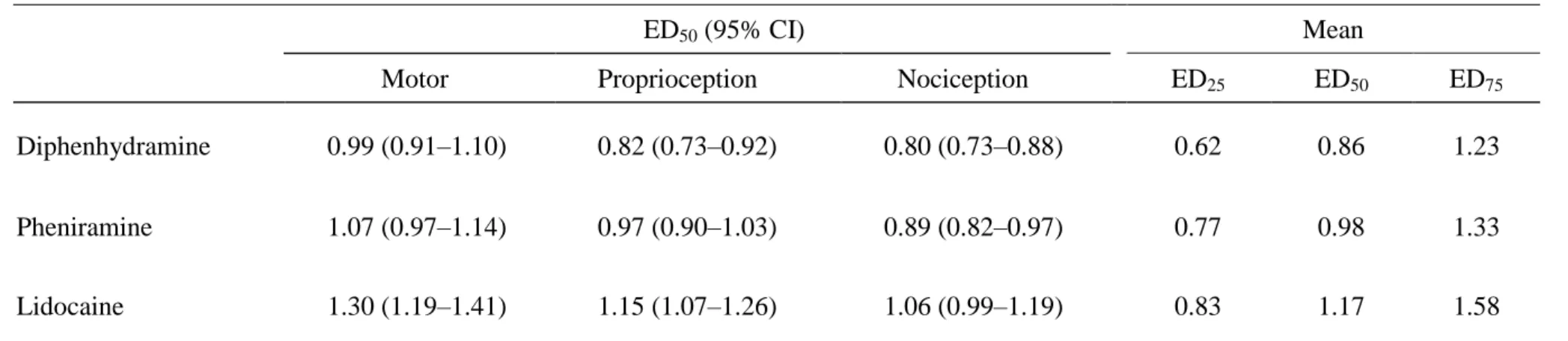
Table 1. The 50% effective doses (ED50s) of drugs on spinal anesthesia in rats
ED50 (95% CI) Mean
Motor Proprioception Nociception ED25 ED50 ED75
Diphenhydramine 0.99 (0.91–1.10) 0.82 (0.73–0.92) 0.80 (0.73–0.88) 0.62 0.86 1.23
Pheniramine 1.07 (0.97–1.14) 0.97 (0.90–1.03) 0.89 (0.82–0.97) 0.77 0.98 1.33
Lidocaine 1.30 (1.19–1.41) 1.15 (1.07–1.26) 1.06 (0.99–1.19) 0.83 1.17 1.58
ED50s of drugs (μmol) were obtained from Figure 1. CI = confidence interval. The potencies of drugs (ED50s) were diphenhydramine = pheniramine > lidocaine (P<0.05, for each comparison) by using 1-way ANOVA followed by pairwise Tukey’s HSD test.
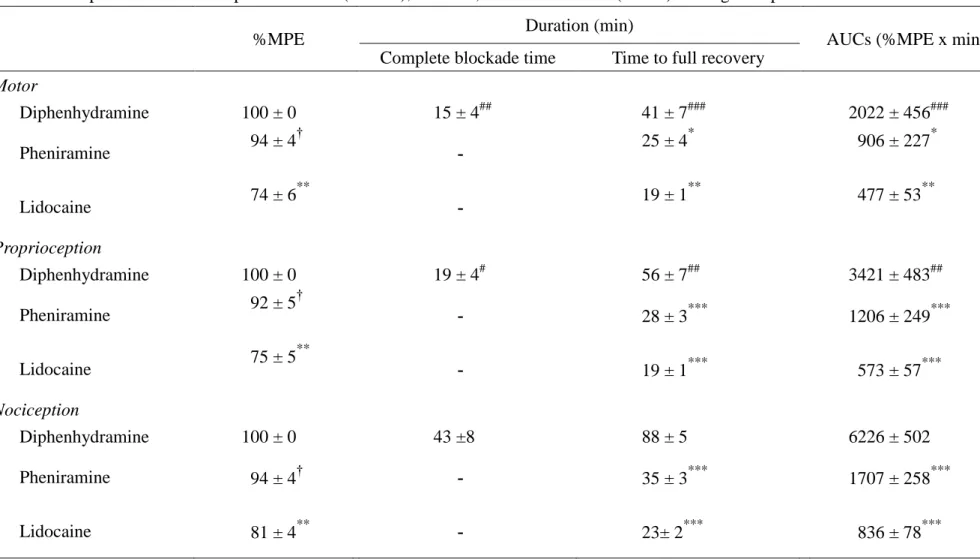
Table 2. The percent of maximal possible effect (%MPE), duration, area under curves (AUCs) of drugs on spinal anesthesia in rats
%MPE Duration (min)
AUCs (%MPE x min) Complete blockade time Time to full recovery
Motor
Diphenhydramine 100 ± 0 15 ± 4## 41 ± 7### 2022 ± 456###
Pheniramine 94 ± 4†
- 25 ± 4* 906 ± 227*
Lidocaine 74 ± 6**
- 19 ± 1** 477 ± 53**
Proprioception
Diphenhydramine 100 ± 0 19 ± 4# 56 ± 7## 3421 ± 483##
Pheniramine 92 ± 5†
- 28 ± 3*** 1206 ± 249***
Lidocaine 75 ± 5**
- 19 ± 1*** 573 ± 57***
Nociception
Diphenhydramine 100 ± 0 43 ±8 88 ± 5 6226 ± 502
Pheniramine 94 ± 4† - 35 ± 3*** 1707 ± 258***
Lidocaine 81 ± 4** - 23± 2*** 836 ± 78***
Spinal anesthesia (means S.E.M.) with drugs at the same dose of 1.75 μmol (n = 8 in each group). Of note, all of the rats in the
diphenhydramine group demonstrated complete blockade (100%MPE) of any function tested. Symbols (*,**,***) indicate P < 0.05, P < 0.01, P < 0.001 when diphenhydramine compared with pheniramine or lidocaine; The symbol (†) indicates P < 0.05 when pheniramine compared with lidocaine; Symbols (#,##,###) indicate P < 0.05, P < 0.01, P < 0.001 when nociception compared with motor or proprioception.
0.1 1
%MPE (maximal possible effect)
0 20 40 60 80 100
Diphenhydramine Pheniramine Lidocaine
0.1 1
%MPE (maximal possible effect)
0 20 40 60 80 100
Dose (mol)
0.1 1
%MPE (maximal possible effect)
0 20 40 60 80 100
Proprioception Motor
Nociception
Fig. 1.
0 15 30 45 60 75 90 105
%PE (possible effect)
0 20 40 60 80 100
Diphenhydramine Pheniramine Lidocaine
0 15 30 45 60 75 90 105
%PE (possible effect)
0 20 40 60 80 100
Motor
Proprioception
Time (min)
0 15 30 45 60 75 90 105
%PE (possible effect)
0 20 40 60 80 100
Nociception
Fig. 2.
25 50 75
Full Recovery Time (min)
0 8 16 24 32 40
Diphenhydramine (D) Pheniramine (P) Lidocaine (L)
ED ( effective dose )
25 50 75
Full Recovery Time (min)
0 8 16 24 32 40
25 50 75
Full Recovery Time (min)
0 8 16 24 32 40
Motor
Proprioception
Nociception
D > P = L D = P = L
D > P = L
Fig. 3.
Figure Legends
Fig. 1. The dose—response curves of diphenhydramine, pheniramine, and lidocaine
on spinal blockades of motor, proprioception, and nociception (% MPE) in rats (n = 8 at each testing point). Data are means ± S.E.M. %MPE = percent of maximal possible effect.
Fig. 2. Time courses of diphenhydramine, pheniramine, and lidocaine on spinal
anesthesia at the same dose of 1.75 μmol in rats. Values are expressed as means S.E.M. Each testing point of the time course study contained eight rats.
Fig. 3. Full recovery time (duration) of action of diphenhydramine, pheniramine, and
lidocaine on spinal anesthesia at doses of ED25, ED50, and ED75 (n = 8 at each testing point). Values are expressed as means S.E.M.