IOS Press
Hand motion assessment and
rehabilitation system
Cheng-Huei Yanga,∗, Pau-Choo Chunga and Cheng-Hong Yangb
aDepartment of Electrical Engineering, National Cheng Kung University, Tainan, Taiwan, Republic of China
bDepartment of Electronic Engineering, National Kaohsiung Institute of Technology, Kaohsiung, Taiwan, Republic of China
Received 18 March 2000 Revised 8 April 2000
Abstract. Along with the rapid development of information technology, computers play an increasingly prominent and impor-tant role. One current trend is to use computers as instruments for physical rehabilitation. In this study, we introduce a new hand motion assessment and rehabilitation system. This system assesses a user’s grip strength and records the sudden changes in air pressure through a circuit and A/D adapter. A PC interface transforms and saves the data in a data record file. The data is then compiled and combined with a patient’s case history and keyed into a database as reference for clinical use. The system is highly efficient, cheap and convenient to use. Doctors can use it to monitor and analyze the progress of a rehabilitation program. Keywords: Rehabilitation, dynamometer, hand motion, assessment
1. Introduction
Life is full of pressures and stress that cause negligence and carelessness at work. This negligence and carelessness can cause bodily harm, for example, in car accidents, sports injuries, occupational injuries, and so on. Those injuries may be just minor, but some will lead to physical impairments. The afflicted will need physical rehabilitation and/or other instruments to help them to resume a normal life. Very commonly occurring injuries are briefly described below:
1. Sports injuries: Injuries are easily caused by over-exercising or not being well warmed up before strenuous exercise. Injuries of hand muscles and ligaments are often caused while playing bad-minton or volleyball, for instance.
2. Carpal tunnel syndrome: Carpal tunnel syndrome refers to a condition where nerves are pressed or squeezed near the carpal tunnel. Standard surgical procedure is to cut off horizontal ligaments, making physical rehabilitation even more important.
3. Shoulder pains: Shoulder pains are common among middle-aged and elder people. Shoulder pain in young patients is usually the result of sports injuries. Shoulder pains among middle aged and elder people are usually caused (for example) by symptoms of a general degeneration, such as degenerative spondylitis and degenerative joint disease. Various reasons can cause shoulder pains,
*
Corresponding author.
and the afflicted patients are often not able to move shoulder joints. This kind of condition is sometimes called “Fifties Shoulders”.
4. Finger injuries: Work or car related accidents often cause finger injuries.
It is necessary for people to retain full motion and functionality of their hands to maintain daily life operations. When hands are impaired or lose part of their functionality, life in general will become inconvenient and difficult. Patients may also have to overcome psychological obstacles and readjust themselves sociologically. Often, patients with hand injuries are at the peak of their productivity. For those people and society as a whole, the costs caused by those injuries are tremendous. Finding a way to rehabilitate and reinstate these people in their working environment is therefore an important issue.
Successful rehabilitation depends on an early diagnosis and on physical, psychological, and occupa-tional conditions. The purpose is to eliminate or reduce impaired functions caused by aging, disease, or injuries, or diagnose degeneration at an early time. Adjusted to individual needs and the practical situation, the combination of a rehabilitation program and a diagnosis system can help patients resume the abilities needed to live a normal life, work and learn. In the past, rehabilitation was only applied to physically impaired people. Now, due to rapid developments in medical engineering and electronic tech-nology, rehabilitation has been extended to patients with chronic diseases, injuries of the nervous system, blood vessel injuries, obesity, and tumor patients. The number of these patients gets progressively larger. More and more patients need rehabilitation after a clinical cure. The degree of injury to the nervous and muscle system can be assessed and evaluated through grip strength. After a correct assessment of the damage, we are able to develop appropriate training programs for the relevant muscles. In this study, we designed and manufactured a hand motion assessment and rehabilitation system that helps doctors and patients to understand and evaluate the degree of injuries.
2. System design
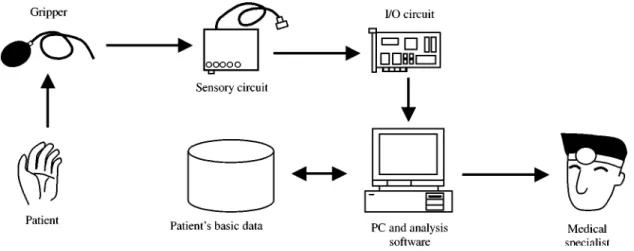
This system is an interface system combining computer hardware and software. Figure 1 shows the schematic system structure. The operational method is to let a patient grip a pneumatic squeeze dy-namometer slowly and then record the exerted strength through a sensory circuit. The sensory circuit
will convert the strength measurement into electronic pressure information and send it to an I/O inter-face. A graph will be displayed on the computer monitor and the patient will be able to view the current situation of his/her grip strength. Doctors are able to use grip strength tests as a basis for diagnosis. The system will also record and store the results of each visit, which will allow doctors to have a better un-derstanding of the rehabilitation progress of patients and set up an appropriate rehabilitation plan with which they can speed up a patients recovery.
2.1. Hardware circuit design
The design of the sensory circuit for the pneumatic squeeze dynamometer is shown below in Fig. 2. Step 1. The pressure value measured through exertion of grip strength is transformed into an amount of digital electronic pressure change.
Step 2. Connection to a PC through a designed interface. The function of the interface is to convert the value of above measured electronic pressure into digital information and to transfer this information to a computer.
2.2. Work theory
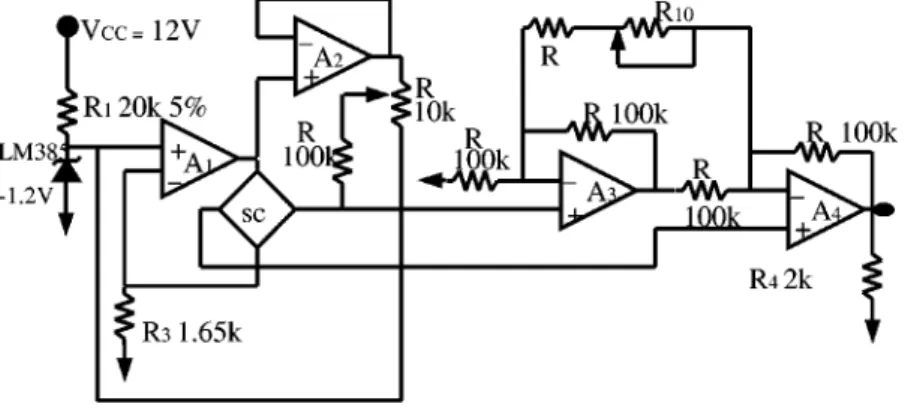
(1) Five elements, R1, LM385-1.2, A1, SCC, and R3compose the circuit drive for a fixed electrical
current (see Fig. 3).
Fig. 2. Analog convert and amplification circuit.
Iref = 590 µA > Iz (min)20 µA of reference current IC, LM385-1.2. Therefore, a stable 1.2 V DC
reference current can be supplied. And the value of the current IBbecomes:
IB = V (−)/R3 = V (+)/R3 = 1.2 V/1.65 k = 0.727 mA, which is in accordance with the regulation
for the SCC.
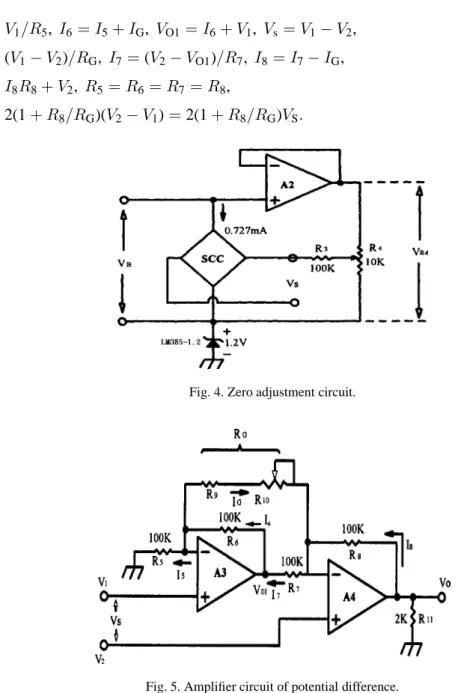
(2) Three elements A2, R3, and R4provide adjustment and compensation.
When pd = 0, Vo = 0 V. This means that the difference of pressure between two gases is zero. If
Vs6= 0, we can adjust R4and make Vs= 0 to achieve the purpose of correction (Fig. 4) [4].
(3) Two OPAmp, A3 and A4, as well as R5 and R11, compose a double OP difference amplifier of
high input-current resistance (see Fig. 5) [5].
I5= V1/R5, I6= I5+ IG, VO1= I6+ V1, Vs= V1− V2,
IG= (V1− V2)/RG, I7= (V2− VO1)/R7, I8= I7− IG,
VO= I8R8+ V2, R5= R6= R7= R8,
VO= 2(1 + R8/RG)(V2− V1) = 2(1 + R8/RG)VS.
Fig. 4. Zero adjustment circuit.
Because the V1and V2input is through “+” of A3 and A4, the amplifier has a high input resistance. The
equation for VOtells us that the amplifier composed of A3 and A4 is focused on the potential difference
of (V1− V2). Therefore, it can be properly used as a resistant bridge. The drive current of our system is
0.727 mA and the amount of the input current becomes: 90 mV(0.727 mA/1.5 mA) = 43.6 mV,
220 mV(0.727 mA/1.5 mA) = 106.6 mV.
When the pressure equals 30 Psid (pounds per square inch difference), the ideal potential should be VO= 5 V, so the amplification calculates as:
5 V/43.6 mV = 115> AV > 5 V/106.6 mV = 46, then
466 2(1 = R8/RG)6 115,
then
R8/56.5 = 100 k/56.5 = 1.77 k6 RG6 R8/22 = 100 k/22 = 4.55 k.
Thus, we can select the fixed-current resistor. R9 = 1.5 k, R10 = 5 k which is a 10 times more
precision variable resistant replacement for RG. We will thus obtain a correct input value through the
adjustment of R10.
(4) Steps for adjustment and correction
1. Because SCC30D detects the difference of pressure values, we let the pressure of the two gases become equal at the entrance. Thus, P1− P2 = 0. This adjustment is called zero adjustment and
compensation. Vout= 0 V.
2. When P1− P2= 30 Psid (the maximum amount of pressure difference), we adjust the gain control
of R10and the input will become 5.00 V. Sensibility of the circuit (S) will become S = 5.00 V/30
Psid = 166.67 mV/Psid.
3. Steps 1 and 2 are repeated until a sufficient accuracy is reached. (1) Circuit analysis of A/D converter (analog to digital converter):
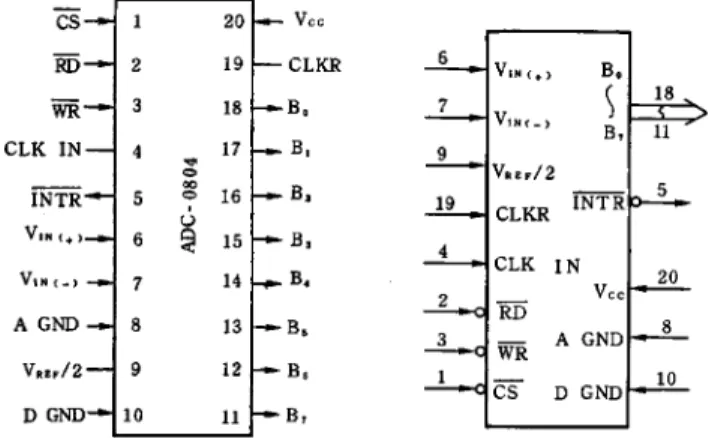
The A/D converting circuit uses 8 digital ASC0804 IC to transfer analogue/digital information [6] and convert electronic pressure into digital information. Then the information is sent to the PC. ADC is a continuous approximation of an A/D converter. The adapter and internal structure are shown in Fig. 6.
The relations of electronic pressure of ADC: ADC order = 28= 256.
Electronic pressure of hand pneumatic squeeze dynamometer = 5 V, and each level of electronic pressure = 5 V/256 = 0.0196 V.
Fig. 6. Adapters and internal structure of ADC.
(3) IC chips can be used on the edges of PPI 8255 IC of a general computer interface. We use a 40 pins DIP input/output IC with three ports, A, B, and C (PA0-PA7, PB0-PB7, and PC0-PC7). We can use software to plan the function of the PPI 8255. The software planning includes three work modes and each port is independently allowed to control the eight-bit control register and represent the meaning of each digital. An address register is then used to define the I/O address of the interface in order for the PC to control the interface circuit and save the data properly [7].
2.3. Software function design
The system has six functions: introduction of the system, personal information, evaluation of grip strength, numerical presentation of evaluation data (figures and tables), result analysis, and system set up. A database system is used for the management of patients’ personal information and the results of each clinic visit. The software tool used is Visual C++ 6.0 [8]. The database is designed through ADO (Activate Data Object) [9] to access multiple computer database files and enhance its functions and usage.
Each function is briefly described below:
1. System introduction: Briefly introduces the functions of this system and allows users to become familiar with the system in the short time.
2. Personal information: Records users’ information (such as name, gender, ID number, occupation and so on) and the results of a training session. Through this information, a doctor will be able to evaluate the progress of patients. Four functions are included [10]. (1) Adding new files to record results of rehabilitation and information of patients; (2) File compilation is used to amend recorded results of rehabilitation and information; (3) Delete file is used to erase incorrect information and reduce unused files; (4) Print file prints the current information (see Fig. 7).
3. Evaluation of grip strength: Uses curves to graphically represent the grip strength of users. The system allows users to set up renewable ratios and executing times. It also will show the maximum, average, and current values (shown as Fig. 8).
4. Figures and tables: Uses varied figures and tables to illustrate the results (such as dot figure, columns, and region figure). New figures can be compared to previous sessions (Fig. 9).
5. Result analysis: Analyzes information according to the patient ID number, diagnosis code, and evaluation date. Then lists statistic numbers for maximum grip strength, ranking, and average grip
Fig. 7. Window showing personal user information.
Fig. 9. Graphic presentation of test results.
strength. It also provides a preview and printing function to print out analyzed information in com-parison.
6. System set up: Set up connects I/O addresses and selects names of connected databases. Other characteristics of this system are the following:
1. Portable small-sized air compressor insures mobility of the system. 2. Window’s software design, easy operations, and user friendly interfaces.
3. Complete rehabilitation plans can be implemented based on the information gained through the evaluation.
3. Results and discussion
In order to help doctors and patients to understand and evaluate the degree of injuries, a good hand mo-tion assessment and rehabilitamo-tion system is needed. Currently, these instruments include the NK Hand Assessment System [1], the JAMAR Digital Hand Dynamometer [2] and the Bseline strain-type Hand Dynamometer [3]. Among them, only the JAMAR Digital Hand Dynamometer is a digital product, the others are analog products. Currently rehabilitation instruments in use at small and medium-sized hos-pitals rely on more traditional methods for the evaluation of stretch strength. Rubber bands and flexible springs are used to measure the strength of fingers. It is difficult to diagnose and determine the degree of injuries and rehabilitation accurately with those instruments. Their use is also troublesome and causes inconveniences to patients and doctors. General rehabilitation systems will only measure maximum grip strength and will not record all the information that can be obtained from the grip-release process. Thus, it is impossible to analyze the overall procedure.
The new system we introduced in this study takes advantage of air pressure differences to acquire a measure for a patient’s grip strength. When a patient grips slowly, a sensor will produce a stream of information. The system will convert the analog information into digital information and send it to a computer through a PC I/O interface while simultaneously displaying figures on a monitor. Users will be able to view a graphic representation of their grip strength and compare it with maximum and average values. The system uses interval times to track the difference in grip strength. The interval time can be adjusted according to the need of different users. Many curves and figures are available to show the various results and progress made in each rehabilitation. All rehabilitation information can be saved in a database of the system for further reference.
The system design consists of two parts: hardware and software. The hardware consists of reassembled circuit parts packaged for the purpose of miniaturizing the system and ensures its convenient operation. Air pressure sensors and digital output of data distinguishes this product from other traditional spring and analog products. Our purpose was to improve the accuracy of measurements for our customers. We cur-rently cooperate with the Rehabilitation Department of the Kaohsuing Chang Gung Memorial Hospital, which uses our system in clinical trials. After a few months, users are able to see a marked improvement of grip strength. The results can also be used as a basis for evaluating the whole rehabilitation progress.
4. Conclusion
Owing to the high cost and inefficiency of current hand motion assessment and rehabilitation systems, we designed and manufactured a more ideally suited one. This system takes advantage of air pressure sensors and the results are more accurate and reliable than those measured through springs and strong rubber bands. The method of operation is to ask patients to squeeze a pneumatic squeeze dynamometer with a sensory circuit measuring the pressure difference. These pressure differences will then be con-verted into digital information and sent to an I/O interface. The information will finally be displayed on a monitor and saved in a database for further reference. This system can be used to evaluate the grip strength of patients, to give instant information to doctors and patients, and to allow them to better un-derstand the degree of injury. The system emphasizes low cost, high efficiency, and convenience. Using this system, doctors are able to evaluate the result, progress, and efficiency of the rehabilitation program. In the future, this system can be installed at home and be compatible with PCs. By transmitting data through a network, patients will be able to send self-assessed data to a doctor’s computer, thereby cutting time and cost of the rehabilitation by avoiding in-house assessments at a medical facility; this will reduce the social costs of rehabilitation significantly.
References
[1] NK Hand Assessment System, NK Biotechnical Corporation, 1997. [2] JAMAR Digital Hand Dynamometer, JAMAR, 1998.
[3] Baseline Strain-Type Hand Dynamometer, Fabrication Enterprises Inc. [4] T.E. Kissel, Industrial Electronics, Prentice-Hall, 1997.
[5] F.R. Dungan, OP-Amps & Linear Integrated Circuits for Technicians, Delmar Publishers. [6] E. Karalis, Digital Design Principles & Computer ARC, Prentice-Hall, 1997.
[7] R.E. Thomas, The Analysis & Design of Linear Circuits, Prentice-Hall, 1994. [8] J. Richter, Advanced Windows, 3rd edn, Microsoft Press, 1998.
[9] MICROSOFT, MS OLE DB 2.0 Programmer’s Reference and Data Access SDK, Microsoft Press, 1998. [10] MICROSOFT, Microsoft Visual Studio 6.0 Core Reference Set, Microsoft Press, 1998.