利用心導管植入手工縫製三瓣帶瓣膜支架移植物在一個肺動脈瓣膜閉鎖不全的動物模式
43
0
0
全文
(2) 中 文 摘 要 : [背景說明]: 利用聚四氟乙烯 (Polytetrafluoroethene,PTFE)手工來裁剪縫製肺動脈瓣膜,縫 製在目前衛福部核准在病患身上使用的支架人工血管(stent graft)上,並套入支架人工血管的套鞘,在全身麻醉下對小豬的股 靜脈來完成使用經皮心導管(percutaneous transcatheter)方式植 入新的肺動脈瓣膜,利用這種心導管植入肺動脈瓣膜法 (Transcatheter pulmonary valve replacement, TPVR)的動物實驗 在我們去年的科技部計畫(MOST 104-2314-B-006-090)證實這個概念 的可行性。因此我們希望能持續先前的計畫: (i)在體外實驗來檢驗 我們瓣膜支架的實用性;(ii)創造一個小豬肺動脈瓣膜閉鎖不全的 疾病動物模式,來證實瓣膜支架的可用性。 [材料與方法]:在本計畫中,我們利用4到6個月(體重約40公斤)的 小豬進行動物實驗,我們首先在全身麻醉下使用過大的氣球導管破 壞小豬的肺動脈瓣膜造成中度以上逆流,形成疾病動物模式,然後 經過1個月後,將我們的瓣膜支架套入支架人工血管的套鞘,在全身 麻醉下對小豬的股靜脈來完成使用經皮心導管方式植入新的肺動脈 瓣膜,並在植入後後利用x光、心臟超音波、電腦斷層、以及最後的 病理切片,來觀察探討疾病模式的豬隻本身在接受此肺動脈血管瓣 膜支架否有改善現象的治療成果的評估。我們也與航太所合作使用 模擬仿生平台(mock circulatory system)在體外利用不同的生理參 數,來測試我們的瓣膜支架的實用性評估。 [結果]:我們已將此支架人工血管植入在四隻肺動脈瓣膜閉鎖不全 的小豬。植入的支架人工血管在血管造影中顯示支架位置良好和正 常功能。心臟超音波與電腦斷層掃描(CT)在追蹤期間沒有發現瓣 膜支架脫位或變形,呈現正常的瓣膜和心臟功能的證據。在最後犧 牲解剖時,總體形態表現出良好的開口和閉合特性,病理切片與其 他連接組織並無發炎或血栓等不正常現象。在模擬仿生平台的離體 實驗中,與缺陷矽管導管相比,確定瓣膜支架的三葉瓣閥有效地將 平均肺動脈壓從10.2增加到14.4mmHg。另外瓣膜支架的回流分數值 為15.9〜18.1%,明顯優於有缺陷的閥導管(RF = 73.5〜85.7%)。 [討論與結論]:因為研究時間現制,在一年的研究計劃中,無法呈 現6個月以上的長期追蹤成果。但根據我們的結果,由於我們的M形 瓣膜支架移植邊界與開窗孔的特殊設計,在離體實驗和動物實驗中 都顯示出可接受的性能和結果。因此我們認為這種方法是容易的 ,可重複的和臨床可行的心導管瓣膜置換手術。我們預期進行動物 實驗的長期追蹤,證實安全性,然後將來能進一步確認我們的概念 來進行人體臨床試驗。 中 文 關 鍵 詞 : 先天性心臟病,肺動脈瓣膜置換,支架人工血管,經由心導管治療 ,動物模式,模擬仿生平台 英 文 摘 要 : [Background]: The handmade expanded polytetrafluoroethylene (ePTFE) trileaflet-valved conduit could potentially be used as a substitute pulmonary valve replacement material, especially in children (NSC 104-2314B-006-090). However, we need to study: (i) the function of the ePTFE trileaflet-valved conduits in an ex vivo experimental system and (ii) the short-term performance of.
(3) the conduit in a porcine pulmonary regurgitations model to verify their clinical applicability. [Materials and Methods]: We adapted the concept of the handmade tri-leaflet valve, made of 0.1-mm expanded polytetrafluoroethylene (ePTFE) coated with phosphorylcholine, with current stent graft to compose a novel TPVR deployment system. In vivo experiment, we used healthy piglets, 4 to 6 months old and weighing an average of 30-40 kg and then used the over-size balloon catheter to destroy the valve and to create the moderate to severe pulmonary regurgitations by echocardiography. After one month observation, transcatheter approach for our valve stent were done via femoral vein on piglet under general anesthesia. The competency of the ePTFE trileaflet-valved conduits was estimated through ex vivo (using a pulmonary mock circulation loop) and in vivo (in a porcine model with a damaged pulmonary valve) experiments. Explants were examined by gross morphology and histopathological examination. [Results]: In the in vivo experiment, the valved conduits were confirmed to be with good valve position maintenance, and the valve and leaflets showed no signs of thickening or peeling, after a short-term implantation period in 4 piglets. There were also no significant signs of inflammation reaction on histopathological examination. In the ex vivo experiment, the ePTFE trileaflet-valved conduits was determined to effectively increase mean pulmonary pressure from 10.2 to 14.4 mmHg, compared with defective silicon-valved conduits. Additionally, the regurgitation fraction value of ePTFE trileaflet-valved conduits was 15.9-18.1%, which was significantly better than the defective valve conduits (RF =73.5-85.7%). [Discussion and Conclusions]: The ePTFE trileaflet-valved conduits for pulmonary valve reconstruction showed acceptable performance and outcomes in the ex vivo and in vivo experiments. The ePTFE trileaflet-valved conduit may be clinically useful, although additional animal studies should be conducted to determine its long-term outcomes. 英 文 關 鍵 詞 : congenital heart disease, pulmonary valve replacement, stent graft, transcatheter replacement, animal model, mock circulatory system.
(4) 附件一. 科技部補助專題研究計畫成果報告 期末報告 利用心導管植入手工縫製三瓣帶瓣膜支架移植物在一個肺動脈瓣膜 閉鎖不全的動物模式 Transcatheter handmade trileaflet valved stent graft implantation in a pulmonary valve regurgitation animal model. 計畫類別:█ 個別型計畫 □ 整合型計畫 計畫編號:MOST 105-2314-B-006-023- 執行期間: 105 年 8月 1日至 106 年 7 月 31 日 計畫主持人:王玠能 共同主持人:甘宗旦、吳瑞得 計畫參與人員:林紹先 成果報告類型(依經費核定清單規定繳交):完整報告 本計畫除繳交成果報告外,另含下列出國報告,共 _1_ 份: □執行國際合作與移地研究心得報告 出席國際學術會議心得報告 期末報告處理方式: 1. 公開方式: 非列管計畫亦不具下列情形,立即公開查詢 □涉及專利或其他智慧財產權,□一年□二年後公開查詢 2.「本研究」是否已有嚴重損及公共利益之發現:否 □ 是 1.
(5) 3.「本報告」是否建議提供政府單位施政參考 否 □是, (請列舉提供之單位;本部不經審議,依勾選逕予轉送) 執行單位:成功大學附設醫院小兒科 中. 華. 民. 國. 106 年. 10 月. 2. 25 日.
(6) (A) 中文摘要 [背景說明]: 利用聚四氟乙烯(Polytetrafluoroethene,PTFE)手工來裁剪縫製肺 動脈瓣膜,縫製在目前衛福部核准在病患身上使用的支架人工血管(stent graft) 上,並套入支架人工血管的套鞘,在全身麻醉下對小猪的股靜脈來完成使用經皮 心導管(percutaneous transcatheter)方式植入新的肺動脈瓣膜,利用這種心導管植 入肺動脈瓣膜法(Transcatheter pulmonary valve replacement, TPVR)的動物實驗在 我們去年的科技部計畫(MOST 104-2314-B-006-090)證實這個概念的可行性。因 此我們希望能持續先前的計畫: (i)在體外實驗來檢驗我們瓣膜支架的實用性;(ii) 創造一個小猪肺動脈瓣膜閉鎖不全的疾病動物模式,來證實瓣膜支架的可用性。 [材料與方法]:在本計畫中,我們利用 4 到 6 個月(體重約 40 公斤)的小猪進行動 物實驗,我們首先在全身麻醉下使用過大的氣球導管破壞小猪的肺動脈瓣膜造成 中度以上逆流,形成疾病動物模式,然後經過 1 個月後,將我們的瓣膜支架套入 支架人工血管的套鞘,在全身麻醉下對小猪的股靜脈來完成使用經皮心導管方式 植入新的肺動脈瓣膜,並在植入後後利用 x 光、心臟超音波、電腦斷層、以及最 後的病理切片,來觀察探討疾病模式的猪隻本身在接受此肺動脈血管瓣膜支架否 有改善現象的治療成果的評估。我們也與航太所合作使用模擬仿生平台(mock circulatory system)在體外利用不同的生理參數,來測試我們的瓣膜支架的實用性 評估。 [結果]:我們已將此支架人工血管植入在四隻肺動脈瓣膜閉鎖不全的小猪。植入 的支架人工血管在血管造影中顯示支架位置良好和正常功能。心臟超音波與電腦 斷層掃描(CT)在追蹤期間沒有發現瓣膜支架脫位或變形,呈現正常的瓣膜和 心臟功能的證據。在最後犧牲解剖時,總體形態表現出良好的開口和閉合特性, 病理切片與其他連接組織並無發炎或血栓等不正常現象。在模擬仿生平台的離體 實驗中,與缺陷矽管導管相比,確定瓣膜支架的三葉瓣閥有效地將平均肺動脈壓 從10.2增加到14.4mmHg。另外瓣膜支架的回流分數值為15.9~18.1%,明顯優於 有缺陷的閥導管(RF = 73.5~85.7%)。 [討論與結論]:因為研究時間現制,在一年的研究計劃中,無法呈現 6 個月以上 的長期追蹤成果。但根據我們的結果,由於我們的 M 形瓣膜支架移植邊界與開 窗孔的特殊設計,在離體實驗和動物實驗中都顯示出可接受的性能和結果。因此 我們認為這種方法是容易的,可重複的和臨床可行的心導管瓣膜置換手術。我們 預期進行動物實驗的長期追蹤,證實安全性,然後將來能進一步確認我們的概念 來進行人體臨床試驗。 [關鍵詞]:先天性心臟病,肺動脈瓣膜置換,支架人工血管,經由心導管治療, 動物模式,模擬仿生平台. 3.
(7) (B) English A b s t r a c t [Background]: The handmade expanded polytetrafluoroethylene (ePTFE) trileaflet-valved conduit could potentially be used as a substitute pulmonary valve replacement material, especially in children (NSC 104-2314-B-006-090). However, we need to study: (i) the function of the ePTFE trileaflet-valved conduits in an ex vivo experimental system and (ii) the short-term performance of the conduit in a porcine pulmonary regurgitations model to verify their clinical applicability. [Materials and Methods]: We adapted the concept of the handmade tri-leaflet valve, made of 0.1-mm expanded polytetrafluoroethylene (ePTFE) coated with phosphorylcholine, with current stent graft to compose a novel TPVR deployment system. In vivo experiment, we used healthy piglets, 4 to 6 months old and weighing an average of 30-40 kg and then used the over-size balloon catheter to destroy the valve and to create the moderate to severe pulmonary regurgitations by echocardiography. After one month observation, transcatheter approach for our valve stent were done via femoral vein on piglet under general anesthesia. The competency of the ePTFE trileaflet-valved conduits was estimated through ex vivo (using a pulmonary mock circulation loop) and in vivo (in a porcine model with a damaged pulmonary valve) experiments. Explants were examined by gross morphology and histopathological examination. [Results]: In the in vivo experiment, the valved conduits were confirmed to be with good valve position maintenance, and the valve and leaflets showed no signs of thickening or peeling, after a short-term implantation period in 4 piglets. There were also no significant signs of inflammation reaction on histopathological examination. In the ex vivo experiment, the ePTFE trileaflet-valved conduits was determined to effectively increase mean pulmonary pressure from 10.2 to 14.4 mmHg, compared with defective silicon-valved conduits. Additionally, the regurgitation fraction value of ePTFE trileaflet-valved conduits was 15.9-18.1%, which was significantly better than the defective valve conduits (RF =73.5-85.7%). [Discussion and Conclusions]: The ePTFE trileaflet-valved conduits for pulmonary valve reconstruction showed acceptable performance and outcomes in the ex vivo and in vivo experiments. The ePTFE trileaflet-valved conduit may be clinically useful, although additional animal studies should be conducted to determine its long-term outcomes. [Key Words]: congenital heart disease, pulmonary valve replacement, stent graft, transcatheter replacement, animal model, mock circulatory system. 4.
(8) ( C ) 、研究計畫內容: (一)研究計畫之背景及目的。 Background and Purpose: Children with complex congenital heart disease involving the right ventricular outflow tract (RVOT) usually need surgical repair at an early age. These patients might need a secondary operation for their degenerative or poor functional pulmonary regurgitations. Traditionally, redo open surgery is necessary to relieve the RVOT dysfunction, which carries high risks and morbidity [1]. Surgical reconstruction of the right ventricular outflow tract, including valve implantation and pulmonary valve replacement or repair, is clinically efficacious. However, biologic valve deterioration often necessitates repeated cardiopulmonary bypass surgery. To circumvent the risks associated with multiple cardiopulmonary bypass surgeries, percutaneous valve replacement has been developed in recent years [2,3]. From the earliest transcatheter valve replacement experimental study performed by Andersen and colleagues in 1992 [2], to Bonhoeffer and colleagues’ pilot study of percutaneous pulmonary valve replacement in a right ventricle–to–pulmonary artery prosthetic conduit with valve dysfunction in 2000 [3], pulmonary valve replacement technology has steadily advanced [4-6]. Clinically, transcatheter pulmonary valve replacement (TPVR) appears to offer significant benefits over standard surgical procedures for patients with congenital heart diseases requiring additional surgical intervention [7-10]. Not only is the process efficacious and less traumatic, but the duration of hospital stay is shortened [7]. TPVR has also has the potential to improve symptoms, functional capacity, and biventricular hemodynamics [7-11]. In the view of anatomy, pulmonary conduits are tubular, low-pressure structures that in many ways are ideally suited to transcatheter pulmonary valve replacement (TPVR). These. 5.
(9) patients have frequently undergone multiple prior procedures; consequently, the threshold for reoperation is very high. Despite the fact that the use of percutaneous pulmonary valve transplantation has been readily adopted, various problems associated with stent implantation per se have been reported. These include stent fracture, valve dislocation, and restenosis [7, 12-15]. In addition, currently available stents are not suitable for use in all prospective patients due to anatomic variability which currently have various problems. First, most of the prospective patients for TPVR are young, the deterioration of bioprosthesis will lead to reoperation which means more agony for the young patients. Second, the sizes of currently available bioprosthetic valves are not suitable for use in all concerned patients due to anatomic variability [16]. Moreover, valved stent deployment during TPVR has been proved to be responsible for traumatic injury to bioprosthetic valve leaflets [17,18], which conceivably impact on the durability of bioprosthetic valves. However, the majority of prosthetic heart valves currently implanted are tissue valves that can be expected to degenerate with time and eventually fail. Repeat cardiac surgery to replace these valves is associated with significant morbidity and mortality. Transcatheter heart valve implantation within a failed bioprosthesis, a “valve-in-valve” procedure, may offer a less invasive alternative [19]. The ideal PV substitute would be readily available, easy to implant, nonimmunogeneic, durable, and would not require systemic anticoagulation. For use in children, growth potential would be an additional desirable feature. Currently, no such valve exists [20]. Polymeric prosthetic heart valve (PPHV) is a so-called’biomechanical valve’’ which is thought as a combination of the advantages of mechanical and bioprosthetic valves: long-term durability and no necessity for permanent anticoagulation [21], and as a promising alternative to bioprosthetic valves for TPVR [22]. Metzner et al [23] have demonstrated an excellent outcome of polyurethane valves with a self-expanding 6.
(10) stent in the pulmonary position of sheep in a period of 4 weeks. Currently, clinically used transcatheter pulmonary valve stents are designed for percutaneous therapy. With currently available stents, it is not possible to treat all concerned patients. So far, patients with small or distorted peripheral vessels and patients with wide or severely calcified and kinked RVOTs are not suitable for percutaneous therapy. New stent designs and hybrid approaches are desired to overcome these problems. Hence there is a definite need for continued development and refinement with regards to the application of this relatively recent technique. In Taiwan, most devices are not available for children. Therefore, Chang and Chang [24] reported their strategy in treating pulmonary regurgitation after surgery for tetralogy of Fallot using a handmade expanded polytetrafluoroethylene (ePTFE) trileaflet conduit for valve reconstruction in 2013. This concept inspired us to design a handmade valve stent graft for transcatheter pulmonary valve implantation. We therefore designed a cost-effective handmade trileaflet stent graft by suturing a semilunar tricusp-shaped ePTFE membrane to a commercial transcatheter stent graft. In our preliminary experience, this approach is easy, reproducible, and clinically practicable for transcatheter deployment in a 13 years old girl [25]. In our previous project (NSC 104-2314-B-006-090), we had designed a handmade trileaflet valve, made of 0.1-mm expanded polytetrafluoroethylene (ePTFE) coated with phosphorylcholine, with current commercial stent graft to compose a novel transcatheter pulmonary valve (PTPV) deployment system successfully deployment in the piglet model. However, the valved stent was implanted in the healthy piglet without pulmonary regurgitation (phase I trial). To systemically evaluate the effects of percutaneous valve stent insertion for real clinical situation, animal models with pulmonary regurgitation are needed (phase II trial)[26, 27]. In addition, Ex vivo tests are easier to design and perform than in vivo animal trials as parameters and boundary 7.
(11) conditions are less problematic to control in a bench setup. Accurate testing of new devices is essential prior to human use. In previous studies, valve tests were conducted in a mock circulatory system (MCS) designed to simulate the pulmonary circulation and near distal pulmonary artery [28, 29]. Therefore, the aims of this project investigated (i) the function of the ePTFE trileaflet-valved conduits in an ex vivo experimental system and (ii) the short-term performance of the conduit in a porcine model to verify their clinical applicability.. References: 1.. Ruzmetov M, Geiss DM, Fortuna RS. Outcomes of pericardial bovine xenografts for right ventricular outflow tract reconstruction in children and young adults. J Heart Valve Dis 2013;22:209-214.. 2.. Andersen HR, Knudsen LL, Hasenkam JM. Transluminal implantation of artificial heart valves. Description of a new expandable aortic valve and initial results with implantation by catheter technique in closed chest pigs. Eur Heart J 1992;13:704-708.. 3.. Bonhoeffer P, Boudjemline Y, Saliba Z, et al. Percutaneous replacement of pulmonary valve in a right-ventricle to pulmonary-artery prosthetic conduit with valve dysfunction. Lancet 2000;356:1403-1405.. 4.. Feinstein JA, Kim N, Reddy VM, Perry SB. Percutaneous pulmonary valve placement in a 10-month-old patient using a hand crafted stent-mounted porcine valve. Catheter Cardiovasc Interv 2006;67:644-649.. 5.. Garay F, Webb J, Hijazi ZM. Percutaneous replacement of pulmonary valve using the Edwards-Cribier percutaneous heart valve: first report in a human patient. Catheter Cardiovasc Interv 2006;67:659-662.. 6.. Coats L, Bonhoeffer P. New percutaneous treatments for valve disease. Heart 8.
(12) 2007;93:639-644. 7.. Ansari MM, Cardoso R, Garcia D, et al. Percutaneous pulmonary valve implantation: present status and evolving future. J Am Coll Cardiol 2015;66:2246-55.. 8.. Cheatham JP, Hellenbrand WE, Zahn EM, et al. Clinical and hemodynamic outcomes up to 7 years after transcatheter pulmonary valve replacement in the US Melody valve investigational device exemption trial. Circulation 2015;131:1960–1970.. 9.. Armstrong AK, Balzer DT, Cabalka AK, et al. One-year follow-up of the Melody transcatheter pulmonary valve multicenter post-approval study. J Am Coll Cardiol Intv 2014;7:1254–1262.. 10. Haas NA, Moysich A, Neudorf U, et al. Percutaneous implantation of the Edwards SAPIEN pulmonic valve: initial results in the first 22 patients. Clin Res Cardiol 2013;102:119–128. 11. Kenny D, Hijazi ZM, Kar S, et al. Percutaneous implantation of the Edwards SAPIEN transcatheter heart valve for conduit failure in the pulmonary position: early phase 1 results from an international multicenter clinical trial. J Am Coll Cardiol 2011;58:2248–2256. 12. Wagner R, Daehnert I, Lurz P. Percutaneous pulmonary and tricuspid valve implantations: an update. World J Cardiol 2015;7:167–177. 13. Schievano S, Petrini L, Migliavacca F, et al. Finite element analysis of stent deployment: understanding stent fracture in percutaneous pulmonary valve implantation. J Interv Cardiol 2007;20:546-554. 14. Kostolny M, Tsang V, Nordmeyer J, et al. Rescue surgery following percutaneous pulmonary valve implantation. Eur J Cardiothorac Surg 2008;33:607-612. 9.
(13) 15. Ruiz CE, Kliger C. Transcatheter pulmonary valve implants: the unchained Melody. J Am Coll Cardiol Intv 2014;7: 1263-1265. 16. Attmann T, Quaden R, Jahnke T, et al. Percutaneous pulmonary valve replacement: 3-month evaluation of self-expanding valved stents. Ann Thorac Surg 2006;82:708-713. 17. Zegdi R, Bruneval P, Blanchard D, Fabiani JN. Evidence of leaflet injury during percutaneous aortic valve deployment. Eur J Cardiothorac Surg 2011;40:257–259. 18. Kiefer P, Gruenwald F, Kempfert J, et al. Crimping May Affect the Durability of Transcatheter Valves: An Experimental Analysis. Ann Thorac Surg 2011;92:155–160. 19. Webb JG, Wood DA, Ye J, et al. Transcatheter valve-in-valve Implantation for failed bioprosthetic heart valves. Circulation 2010;121:1848-1857. 20. Mosca RS. Pulmonary valve replacement after repair of tetralogy of Fallot: Evolving strategies. J Thorac Cardiovasc Surg 2015;7:1-8. 21. Sachweh JS, Daebritz SH. Novel ‘‘biomechanical’’ polymeric valve prostheses with special design for aortic and mitral position: a future option for pediatric patients? ASAIO J 2006;52:575–580. 22. Claiborne TE, Slepian MJ, Hossainy S, Bluestein D. Polymeric trileaflet prosthetic heart valves: evolution and path to clinical reality. Expert Rev Med Devices 2012;9:577–594. 23. Metzner A, Iino K, Steinseifer U, et al. Percutaneous pulmonary polyurethane valved stent implantation. J Thorac Cardiovasc Surg 2010;139:748–752. 24. Chang TI, Chang CI. An efficient way to make a trileaflet conduit for pulmonary valve replacement. Ann Thorac Surg. 2013;96:e163-165. 25. TW Lin, JN Wang, CD Kan, YJ Yang. Handmade trileaflet valved stent graft for 10.
(14) pulmonary valve implantation. J Thorac Cardiovasc Surg 2014;148:1753-5. 26. Bai Y, Zong GJ, Jiang HB, Li WP, Wu H, Zhao XX, Qin YW. Percutaneous valve stent insertion to correct the pulmonary regurgitation: an animal feasibility study. Chin Med J 2010;123:3127-3131. 27. Agger P, Hyldebrandt JA, Nielsen EA, Hjortdal V, Smerup M. A novel porcine model for right ventricular dilatation by external suture plication of the pulmonary valve leaflets – practical and reproducible. Interact Cardiovasc Thorac Surg 2010;10:962-966. 28. Camp TA, Stewart KC, Figliola RS, McQuinn T. In vitro study of flow regulation for pulmonary insufficiency. J Biomech Eng 2007;129:284-288. 29. Vismara R, Laganà K, Migliavacca F, et al. Experimental setup to evaluate the performance of percutaneous pulmonary valved stent in different outflow tract morphologies. Artif Organs 2009;33:46–53. 30. Lancellotti P, Tribouilloy C, Hagendorff A, et al. Recommendations for the echocardiographic assessment of native valvular regurgitation: an executive summary from the European Association of Cardiovascular Imaging. Eur Heart J Cardiovasc Imaging. 2013;14:611-644. 31. Timms D, Hayne M, McNeil K, Galbraith A. A complete mock circulation loop for the evaluation of left, right, and biventricular assist devices. Artif Organs 2005;29:564–572. 32. ANSI/AAMI/ISO 5840. Cardiovascular Implants: Cardiac Valve Prostheses. AAMI; Arlington, VA: 2005. 33. Gohean J, Figliola R, Camp T, McQuinn T. Comparative in vitro Study of Bileaflet and Tilting Disk Valve Behavior in the Pulmonary Position. ASME J Biomech Eng 2006;128:631–635.. 11.
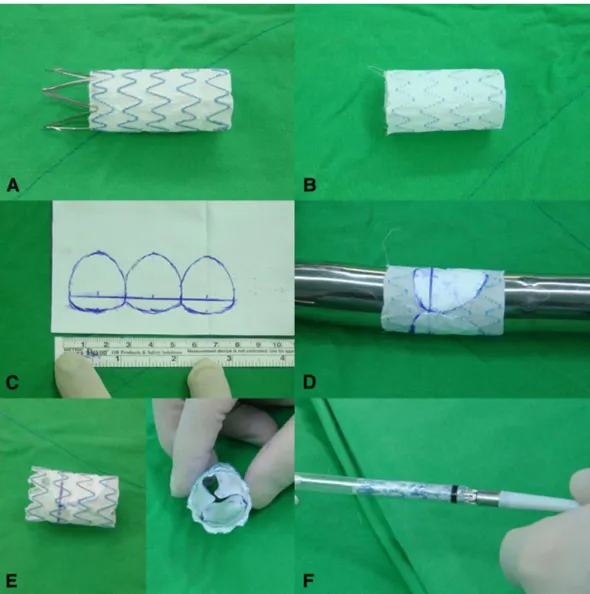
(15) (二)研究方法、進行步驟及執行進度。. Materials and Methods Valved Stent Construction and Ex Vivo Testing According to the general condition of patients’ main pulmonary artery size measured on computed tomography angiography, an Endurant II (Medtronic Inc, Galway, Ireland) aortic extension stent graft, 23 mm in diameter and 49 mm in length, was chosen. The stent graft was deployed ex vivo first for further manipulation (Figure 1, A). It was then flipped inside out, the anchor pins was cut off, and the stent graft was trimmed to achieve a final length of 3 cm (Figure 1, B). The most distal part of the polyester graft membrane was trimmed along the M-shaped stent. One thin ePTFE membrane (Gore-Tex Preclude pericardial membrane; WL Gore & Associates Inc, Flagstaff, Ariz) was trimmed into a semilunar tricusp shape on the basis of that introduced by Chang and Chang [21]. To allow better coaptation, we modified the shape by adding a curved structure to each leaflet in addition to the 3- to 5-mm connecting junctions, turning the membrane into a bi-semilunar tricusp shape [22] (Figure 1, C). The trileaflet piece was then sutured to the flipped stent graft with 6-0 polypropylene continuous suture, supported with a Hegar dilator inside (Figure 1, D). After completing the suture, we flipped the stent graft back into its original form. Three additional fenestration holes was created at the distal side of stent graft to prevent catastrophic pulmonary arterial obstruction caused by stent graft malposition. Fluid passing into the valved stent in the appropriate direction was filled the pouch-like valvar sinuses defined by each of the leaflets. In this way, the valve leaflets were coapted inside the segment of the vein, thereby forming an effective valve closure. Fluid flow in the opposite direction was not restricted. The accomplished 12.
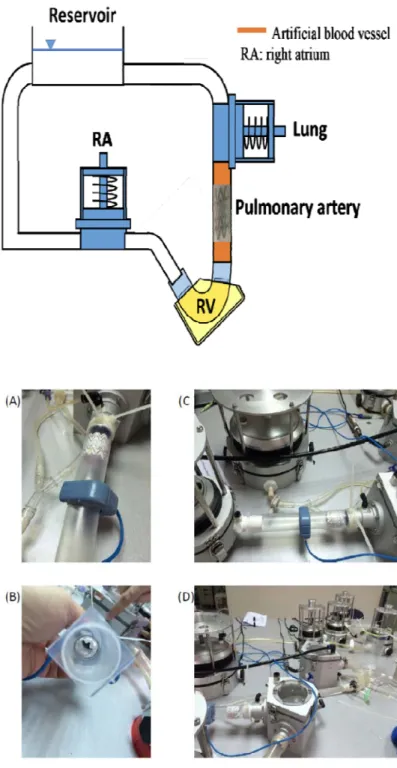
(16) valved stent graft was then reloaded into the delivery device (Figure 1, E and F).. Valve Competency Testing Using a Mock Circulation Loop The competency of our handmade ePTFE trileaflet-valved conduits was estimated by using a mock pulmonary circulation system at the National Cheng Kung University Heart Science and Medical Research Center. A mock circulation loop (MCL) is a mechanical representation of the human circulatory system. Typically, the lumped-parameter concept has been used for MCL designs, in which flow rate and pressure are considered important aspects while accurate wave phenomena are ignored. Pulmonary arteries were modeled and constructed using silicone rubber casts with simplified T-shape geometric and compliance properties that are similar to those seen in the pulmonary circulation system. In this study, pulmonary circulation was simulated with a hybrid one-dimensional and lumped-parameter MCL that can mimic pulse wave propagation phenomena, as shown in Figure 2. This MCL consisted of one artificial right ventricle and a main pulmonary artery with right and left pulmonary branches; returning blood flow was deposited into the right atrium. The artificial right ventricle was made of silicone rubber with a heart-like appearance, and stroke volume (SV) was installed in an aluminum chamber. Two silicone rubber tri-leaflets valves were installed in the inflow and outflow of the right ventricle respectively to direct the flow direction similar to the function of the normal tricuspid and pulmonary valves. Right ventricular function was simulated by using a digitally controlled hydraulic piston SuperPump (ViViTro Labs, Victor, British Columbia, Canada), which generated a pulsating flow to drive the chamber and send it into a compliant pulmonary artery. The artificial pulmonary artery was made of 2mm thick, inner diameter 25mm, silicone rubber with a T-shaped geometry. The volume compliance of 13.
(17) the T-shaped artery was about 0.2 mL/mmHg, and it was connected to the right and left lung compliance chambers. Two sets of compliance chambers and pinch valve resistors were designed and attached to the distal ends of the right and left pulmonary arteries to mimic the resistance and compliance characteristics of the distal vasculature. A reservoir compliance chamber was also connected to the left and right pulmonary branches with back flow to a right atrium compliance chamber. The measured segmental compliance and resistance values are presented in Table 1. The pulmonary valve was substituted with handmade ePTFE trileaflet-valved conduits or with defective trileaflet silicon valve to test valve competency.. In Vivo Tests in a Porcine Model Animal studies was approved by the hospital ethics committee. All animals received care in compliance with the Guide for the Care and Use of Laboratory Animals (www.nap.edu/catalog/5140.html). Four healthy piglets, aged 4–6 months with an average weight of 40 kg were used to evaluate the in vivo functions and morphological changes that occurred in the implanted valves. The piglets’ original pulmonary valves were destroyed by repeated CODA balloon (Cook Medical, Bloomington, IN) traction, which were pass through from the right femoral vein sheath, to create the pulmonary valve regurgitation model. One month later, the valved-stent conduits were implanted in the piglets’ pulmonary valve regions using a percutaneous delivery sheath method (Medtronic., Mininneapolis, MN) under C-arm, fluoroscopy-guided assistance; transthoracic echocardiography was then performed to confirm the success of the implant. Following surgery, chest radiography and transthoracic echocardiography were performed every 2 weeks. After 1 month, the piglets’ chest were scanned using CT and the ePTFE trileaflet-valved conduits were retrieved to evaluate the morphology and determine if thrombi were present. 14.
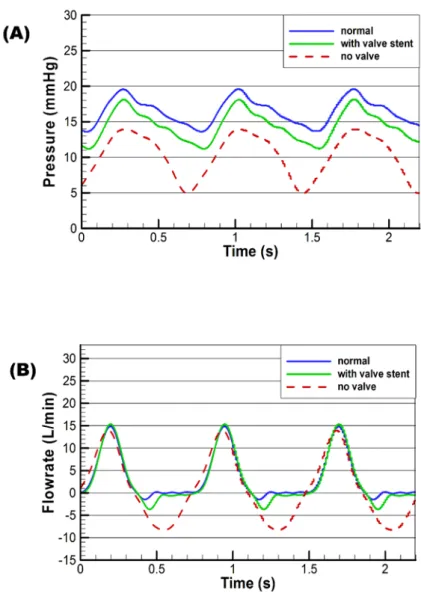
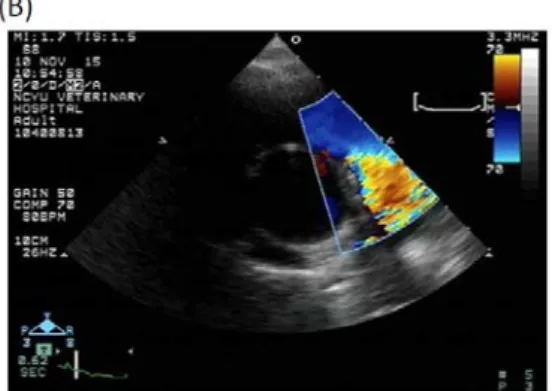
(18) (三)研究結果。 We adapted the concept of the handmade tri-leaflet valve, made of 0.1-mm expanded polytetrafluoroethylene (ePTFE) coated with phosphorylcholine, with current commercial stent graft to compose a novel TPVR deployment system (Fig. 1). Our valve tests conducted in a mock circulatory system (MCS) designed to simulate the circulation Under the assistant of Prof. Lu & Dr. Chan, we had set-up the MCS system (Fig. 2). Figure 3 depicts sample pressure and flowrate waveforms at the mock pulmonary artery. The right ventricle pumping SV and pumping rate were set at 40 mL and 80 bpm, respectively. The solid blue line, solid green line, and dashed red line represent the intact valve (silicone rubber tri-leaflet valve), handmade ePTFE trileaflet-valved conduits, and the defective silicon valve, respectively. Figure 3A revealed the ePTFE trileaflet-valved conduit increased the mean pulmonary pressure from 10.2 to 14.4 mmHg, compared with the defective silicon valve (although not as perfectly as can an intact valve). The flowrate results in Figure 3B also showed that the ePTFE trileaflet-valved conduit is able to effectively reduce regurgitation. The experimental results of the valve efficacy mock test at different heart rates and SVs are presented in Table 2; in particular, they indicate that the RF of the handmade ePTFE trileaflet-valved conduit was significantly improved compared with that of the defective trileaflet silicon valve (RF = 15.9%–18.1% vs 73.5%–85.7%, respectively). We had cooperated with veterinarians, Drs. Jui-Te Wu, and Zhi-Jia Zheng in the Veterinary Teaching Hospital, College of Veterinary Medicine, National Chiayi University, Chiayi, Taiwan to prepare and proceed this study. Finally, the implantation was done in 4 piglets. Angiography confirmed the destruction of pulmonary valve (Fig. 4: A-B), and the successful implantation of valve conduit (Fig. 4: C-D). Echocardiography (Fig. 5) and cardiac computed tomography (CT) (Fig. 6) during follow up revealed no evidence of ePTFE trileaflet-valved conduit 15.
(19) dislocation or deformation and normal valvular and cardiac functionality. Gross morphology demonstrated good opening and closure characteristics when sacrificed. ePTFE trileaflet-valved conduit adjacent area for pathologic examination also revealed no signs of inflammation reaction (Fig. 7).. (四)討論與結論。 Handmade ePTFE trileaflet-valved conduits showed acceptable performance for pulmonary valve reconstruction in both mock and animal experiments. The proposed optimal design algorithm was applied to design the handmade trileaflet-valved conduits with oversized diameter. Notably, the algorithm was easily implemented using a portable electronic device application. We suggest that these conduits may be suitable for clinical purposes, although their long-term in vivo behavior requires further evaluation.. 16.
(20) 17.
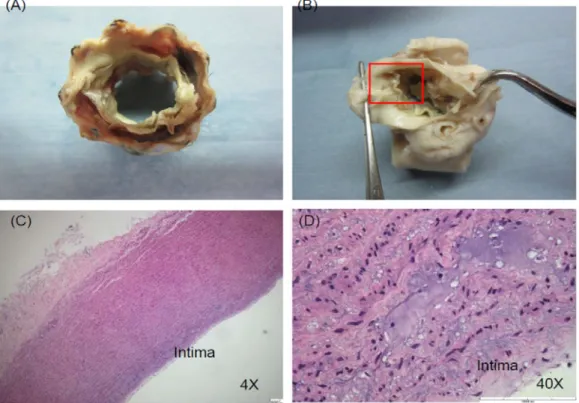
(21) Figure legends Fig. 1: The percutaneous transcatheter pulmonary valve deployment system. A, An Endurant II (Medtronic Inc, Galway, Ireland) aortic extension stent graft was deployed ex vivo. B, The stent graft was flipped inside out, with the anchor pins removed and total length trimmed to approximately 3 cm. C, Bi-semilunar tricusp design on an ePTFE membrane. D, A number 21 Hegar dilator was put inside the flipped stent graft during suturing of the trileaflet ePTFE membrane to the stent graft. E, The final appearance of the handmade trileaflet valved stent graft. F, The accomplished stent graft was reloaded into the delivery device. Fig. 2: Scheme and photo of the pulmonary circulation mock loop. A, Close view of the ePTFE trileaflet-valved conduit mounted in the MCS system. B, Cross-section view of the ePTFE trileaflet-valved conduit. C, The ePTFE trileaflet-valved conduit and the system. D, The whole MCS system. Fig. 3: Sample pressure and flow rate waveforms at the mock pulmonary artery. (A) Pulmonary artery pressure waveform. (B) Pulmonary artery flowrate waveform at HR=80 bpm and CO=3.2 L/min. Fig. 4: The procedure of transcatheter pulmonary valve deployment. A, Initial attempt to destroy the pulmonary valve using large sheath with balloon catheter. B, RVOT angiography to confirm the pulmonary regurgitation. C, The delivery sheath was placed in the RVOT and slowly deploy the ePTFE trileaflet-valved conduit. D, The ePTFE trileaflet-valved conduit was fully-open and in the good position. Fig. 5: Follow up echocardiography. A, 2-D echocardiography revealed stent in correct position. B, Color echocardiography revealed stent in the RVOT without obstruction. C, Doppler echocardiography revealed normal laminar flow through RVOT stent. Fig. 6: Follow up computed tomography (CT). A, CT revealed stent in the RVOT without obstruction. B, 3-dimentional CT revealed stent in the RVOT. Fig. 7: Gross & micro pathology. A, Macro view of cross section of ePTFE trileaflet-valved conduit in RVOT position. B, Valve conduit adjacent area for pathologic examination. C, Low-power (10x) field revealed no signs of inflammation reaction. D, High-power (40x) field revealed no signs of inflammation reaction. 18.
(22) Fig. 1: The percutaneous transcatheter pulmonary valve deployment system. 19.
(23) Fig. 2: Scheme and photo of the pulmonary circulation mock loop. 20.
(24) Fig. 3: Sample pressure and flowrate waveforms at the mock pulmonary artery. 21.
(25) Fig. 4: The procedure of transcatheter pulmonary valve destruction and valve stent deployment. 22.
(26) Fig. 5: Follow up echocardiography.. 23.
(27) Fig 6. Follow up computed tomography (CT).. 24.
(28) Fig. 7: Gross & micro pathology.. 25.
(29) 附件二. 國科會補助專題研究計畫成果報告自評表 請就研究內容與原計畫相符程度、達成預期目標情況、研究成果之學術或應用價值(簡要敘 述成果所代表之意義、價值、影響或進一步發展之可能性)、是否適合在學術期刊發表或申 請專利、主要發現或其他有關價值等,作一綜合評估。. 1. 請就研究內容與原計畫相符程度、達成預期目標情況作一綜合評估 ■ □. 達成目標 未達成目標(請說明,以 100 字為限) □ 實驗失敗 □ 因故實驗中斷 □ 其他原因. 說明:. 2. 研究成果在學術期刊發表或申請專利等情形: 論文:■已接受發表(The Journal of Thoracic and Cardiovascular Surgery, JTCVS) □未發表之文稿 □撰寫中 □無 專利:□已獲得 □申請中 ■無 技轉:□已技轉 □洽談中 ■無 其他:. 26.
(30) 3. 請依學術成就、技術創新、社會影響等方面,評估研究成果之學術或應用價值(簡要敘 述成果所代表之意義、價值、影響或進一步發展之可能性)(以 500 字為限) 先天性心臟病(法洛式四合症患者)因為先天性的肺動脈狹窄,導致雖經過矯正手術後仍 有產生重度肺動脈瓣膜逆流、以及心臟擴大衰竭,需要再次進行開心手術更換肺動脈及肺動 脈瓣膜的病患。因為這些先天性心臟病患者,大多數仍是兒童,體重與體型較小,無法使用 市面上商業化的人工瓣膜,因此傳統的開心手術來更換肺動脈及肺動脈瓣膜的兒童病患,都 是由外科醫師手工來裁剪縫製肺動脈及肺動脈瓣膜。手工縫製好的肺動脈其一定要再次開胸 且仍須大規模剝離肺動脈組織才能把血管及瓣膜置換上去,但對於再次或多次需經開胸手術 的患者而言,這過程相當困難且危險。因此我們預計使用永久植入主動脈支架血管取代一般 人工血管,並將肺動脈瓣膜縫製在支架血管上,希望能簡化手術過程,甚至也許以後能發展 經皮置換手術的可能性。雖然目前已有商業量產的類似支架瓣膜,但是非常昂貴而且尺寸的 選擇較少,因此我們期待這個客製化概念期望首先經由動物實驗來驗證,然後才能繼續人體 實驗;這也是本研究之目的即重要性。 我們利用聚四氟乙烯(Polytetrafluoroethene,PTFE)手工來裁剪縫製 M 形瓣膜支架移植 邊界與開窗孔的特殊設計肺動脈瓣膜,縫製在目前衛福部核准在病患身上使用的支架人工血 管(stent graft)上,並套入支架人工血管的套鞘,在全身麻醉下對小猪的股靜脈來完成使用經 皮心導管(percutaneous transcatheter)方式植入新的肺動脈瓣膜。利用這種心導管植入肺動脈 瓣膜法(Transcatheter pulmonary valve replacement, TPVR)。在我們去年的科技部計畫(MOST 104-2314-B-006-090)已證實這個概念的可行性。因此今年度我們持續先前的計畫: (i)在體外 實驗來檢驗我們瓣膜支架的實用性;(ii)創造一個小猪肺動脈瓣膜閉鎖不全的疾病動物模 式,來證實瓣膜支架的可用性。在這個計畫中,我們首先使用過大的氣球導管破壞小猪的肺 動脈瓣膜造成中度以上逆流,形成疾病動物模式,然後我們將此瓣膜支架植入在植入在肺動 脈瓣膜閉鎖不全的小猪。植入的瓣膜支架人工血管在顯示支架位置良好和正常功能。在模擬 仿生平台的離體實驗中,與缺陷矽管導管相比,確定瓣膜支架也明顯優於有缺陷的閥導管。 這種方法是容易的,可重複的和臨床可行的心導管瓣膜置換手術(TPVR)。而且透過動物 實驗的操作,也使團隊成員熟悉置放 TPVR 手術的步驟。這個計畫的結果除了已在今年度 的世界兒童心臟及心臟外科學大會(2017 WCPCCS)發表外,也完成論文投稿到頂尖的心臟外 科期刊(The Journal of Thoracic and Cardiovascular Surgery, JTCVS; 2016 Impact Factor: 4.446 Ranked 12/197 in Surgery)並已被接受刊登。我們將來預期進行動物實驗的長期追蹤,證實安 全性,然後將來能進一步確認我們的概念來進行人體臨床試驗。 27.
(31) 28.
(32) 附件五. 科技部補助專題研究計畫出席國際學術會議心得報告 日期: 106 年 10 月 15 日. 計畫編號. MOST(NSC). 105. 計畫名稱. 利用心導管植入手工縫製三瓣帶瓣膜支架移植物在一個肺動脈瓣膜閉. -. 2314. - B. -. 006. -. 063. -. 鎖不全的動物模式 出國人員 姓名. 王玠能. 會議時間. 106 年 7 月 16 日 至 106 年 7 月 21 日. 服務機構 及職稱 會議地點. 成功大學附設醫院小兒科 巴賽隆納、西班牙 (Barcelona, Spain). (中文) 第七屆世界兒童心臟及心臟外科學大會 會議名稱 (英文) 7th World Congress of Pediatric Cardiology & Cardiac Surgery, (WCPCCS) (中文) 肺動脈瓣膜重建中手工三葉心包膜瓣導管的體內和體外測試 發表題目. (英文) In vivo and in vitro testing for hand-made trileaflets pericardial patch valved-conduits in pulmonary valve reconstruction. 1.
(33) 一、 參加會議經過 世界兒童心臟及心臟外科學大會(World Congress of Pediatric Cardiology & Cardiac Surgery, 以下簡稱 WCPCCS)是每四年一次集合全世界一些相關兒童心臟學及兒童心 臟外科學的醫學會共同來舉辦的醫學會議。其主要的目的在聚集有研究心血管科學 的專家,共同來分享並發表最新而且尖端的兒童心臟醫學研究。因此世界各地的相 關學者,都把該學會視為一個重要的舞台來發表他(她)們的最近研究。這是第七屆 的 WCPCCS,原本選定土耳其舉辦,但因為恐怖攻擊因素,改選定在本年度(2017) 的 7 月 16 日到 7 月 21 日在西班牙的巴賽隆納城市(Barcelona, Spain)的加泰隆尼亞大 會堂(the Palau de Congressos de Catalunya)來舉辦。因此對我們有相關研究的人而 言,這是一個不該錯過的與其他專家交流的機會,因此當我們的研究報告被接受之 後就開始準備此次的行程。 我在 7 月 13 日(星期四)晚上由台南出發,到達桃園機場後,因為沒有直航班機, 我因此搭乘由中華航空的航班(CI61)飛往德國、法蘭克福後,再轉乘德國漢莎航空 班機(LH1130)於 7 月 14 日(星期五)抵達巴賽隆納後,到達會場附近的飯店。由於時 差的關係稍作休息並拜訪會場附近的巴賽隆納大學校園(University of Barcelona)以 及這個特別的城市,於 7 月 16 日到 7 月 21 日參與大會開會,而後於 7 月 22 日搭乘 德國漢莎航空的航班(LH1139)飛往法蘭克福轉乘中華航空的班機(CI62)於 7 月 23 日 到達桃園機場後,搭乘高鐵回到台南。. 2.
(34) 二、 與會心得 會議的第一天(7 月 16 日)是大會所舉辦的會前研討會(pre-conferences)。會中邀請 許多知名的學者針對以下的主題 Fetal Cardiology、Neurodevelopment Symposium、 Innovation & Technology、International Quality Improvement Collaborative (IQIC) Learning Session at 7th WCPCCS、5th Nomenclature Summit at at 7th WCPCCS、Pediatric Sports Cardiology 來探討。其中我對 Fetal Cardiology 的演講很感興趣,其中 Fetal Imaging 來自德國的 Renate Oberhoffer 教授所發表的 Clues to fetal cardiac disease during screening 啟發我幾個訣竅,讓我學到如何早期偵測胎兒心臟病。會前研討會有另一個 Pediatric Sports Cardiology 的部分也很有趣,因為強調兒童運動健康應該是未來台灣要 努力的方向,而小兒心臟科醫師的確可以伴演重要角色。會前研討會到下午 4 點結束 後緊接著是大會開幕典禮,由來自土耳其的知名學者 Dr.Sertac Cicek 擔任主席發表歡 迎詞後舉行歡迎茶會,來自世界各地的學者共聚一堂進行交流。 會議的第二天(7 月 17 日)就是大會正式開始,有多達十多個會場包含(Surgery、 Cath、 Imaging、 ICU、 ACHD 、EP 、Anesthesia、Transplant & Heart failure、 Rheumatic 、Ambulatory & Genetics、 ICHLS、 PAH 、Coronary 、Perfusion、 Humanitarian、 Nursing、 Case Abstract、 Research Abstract)這些幾乎涵蓋所有不同領 域。因為我對 Cath (Interventional Cardiology)比較有興趣,一直待在這個會場觀看 Live Case Demo 以及演講。另來自德國的知名學者 Dr. Felix Berger (Germany) 發表 Perspectives on over 15 Years of Transcatheter Pulmonary Valve Replacement: Impact of the Learning Curve on Clinical Outcomes 以及來自卡達的知名學者 Dr. Ziyad M. Hijazi (Qatar) 發表 Clinical Outcomes With Self-Expanding Pulmonary Valve Systems 的演講, 3.
(35) 非常精彩引發熱烈討論。因為我的研究主題也是相關,因此收穫不少。接下來下午就 是因為在我的海報報告處(Poster session : Interventional Cardiology, No 1778)接受大會 安排的 Moderators 的詢問以及 Brief presentation,並與其他國家的學者進行交流,Dr. Balekundri Vijayalakshmi 對於我的研究提出一些驗證方法見解,受益良多。 會議的第三天(7 月 18 日) 早上由來自美國的知名學者 Dr. Carole Warnes 發表 Adult Congenital Heart Disease: The Courage to be Imperfect 的大會演講(Jane Somerville Jonorary Lecture),這是我認為最棒的一場演講,講述她們團隊如何建立起照顧成人期 先天性心臟病換的經驗對於正要起步的我們有很大的幫忙。接下來我留在 Cath (Interventional Cardiology)這個會場觀看 Live Case Demo 以及演講。另來自美國的學者 Dr. Michel Illbawi 以及來自美國的 Dr. Zahid Amin 針對 Transcatheter closure in younger patients has more potential for negative consequences than surgical closure 的正反雙方辯 論的演講,非常精彩引發熱烈討論。 會議的第四天(7 月 19 日) 我跑到 ICU (Intensive Care Unit)這個會場聍聽重症病患 的照顧經驗,幾位大師的演講,非常精彩讓我受益良多。下午一些演講,因為跟我的 相關主題比較遠因此沒有太多心得。中間抽空也觀摩其他學者的海報報告,並與其他 國家的學者進行交流,收穫很多。 會議的第五天(7 月 20 日) 我參加 Tetralogy of Fallot and Behond 這個主題演講,幾 位大師的演講非常精彩,主席 Drs. Dan Penny & Gil Wernovsky 經驗豐富,針對演講內 容提出重要的評論,讓我學到許多。 會議的第六天(7 月 21 日)主要都是大師回顧演講(Landmark Lectures),來自卡達的 知名學者 Dr. Ziyad M. Hijazi (Qatar) 發表 Pediatric Interventioanl Cardiology: The past, 4.
(36) present and future 的演講,這是我認為最重要的一場演講,對於我們有很大的啟發。. 大會會場. 5.
(37) 三、發表論文全文或摘要 In vivo and in vitro testing for hand-made trileaflets pericardial patch valved-conduits in pulmonary valve reconstruction Jieh-Neng Wang, Chung-Dann Kan1, Wei-Ling Chen2, Jui-Te Wu3, Min-Ling Hsieh, Jing-Ming Wu Departments of Pediatrics and Surgery1, National Cheng Kung University Hospital, College of Medicine, National Cheng Kung University, Tainan, Taiwan Department of Engineering and Maintenance2, Kaohsiung Veterans General Hospital, Kaohsiung, Taiwan Veterinary Teaching Hospital3, College of Veterinary Medicine, National Chiayi University, Chiayi, Taiwan Background. The hand-made trileaflets pericardial patch valved-conduits might be used as the pulmonary valve replacement substitute materials. The aim of this study was to investigate the valve function of the hand-made trileaflets pericardial patch valved-conduits by mock system (in vitro) and their short-term conditions in piglet animal model (in vivo) to justify the applicability of clinical purpose. Methods. The competency of the hand-made trileaflets pericardial patch valved-conduits were tested on the pulmonary circulation mock system. The valved-conduit assembled into a delivery system to deploy into the pig animal destroyed pulmonary valve model via femoral vein under general anesthesia. In vivo functional and morphology analysis were tested during a 4-week period. Results. On mock circultatory system, the hand-made trileaflets pericardial patch valved-conduit, although not as perfect as the silicon trileaflets valve, can effectively rise the mean pulmonary pressure from 10.2 to 14.4 mmHg with compared to the defected silicon valve one. The regurgitation fraction (RF) value of hand-made trileaflets pericardial patch valved-conduit group is 15.9- 18.1% significantly improved compare with the defected valve group (RF=73.5-85.7%). The in-vivo pulmonary condition experiments showed their good valve position conditions and the valve and leaflets characteristics and function. The histological analysis of the valved-conduits adjacent pulmonary area also revealed no significant signs of inflammation reaction. Conclusion. The hand-made trileaflets pericardial patch valved-conduits for pulmonary valve reconstruction on both mock and animal experiments showed with acceptable performance and outcome. It might implicate that this hand-made trileaflets pericardial patch valved-conduits can be used in further clinical purpose. However, the long-term animal results still need time to justify. Key word: transcatheter pulmonary valve replacement, hand-made valved-conduits, mock, animal model. 6.
(38) 論文海報原稿. 7.
(39) 四、 建議 1. 這次大會有一個我們較為忽視的主題 Pediatric Sports Cardiology,因為強調兒童運 動健康,鼓勵未來主人翁喜歡運動促進健康,應該是未來台灣要努力的方向,而 小兒心臟科醫師的確可以伴演重要角色。 2.. 感謝科技部的補助,讓我有機會出國開會與其他國家的學者進行交流,收穫很多。 但是因為本年度的計畫預算必須用於本年度,但是有些大型學會的投稿必須在半 年前就截止,但是研究的成果不太容易在年度初就馬上有成果。因此建議出國開 會的補助應該可以再更有彈性較好。. 五、攜回資料名稱及內容 因為歐洲強調環保,許多檔案都在雲端電子化,利用個人登錄的帳號來進行登錄 觀看,同時涉及版權,只能個人使用,不能附上報告引用。因此只攜回自己手抄的 資料本及隨身碟。. 六、其他 無. 8.
(40) 105年度專題研究計畫成果彙整表 計畫主持人:王玠能. 計畫編號:105-2314-B-006-063-. 計畫名稱:利用心導管植入手工縫製三瓣帶瓣膜支架移植物在一個肺動脈瓣膜閉鎖不全的動物模式 成果項目. 學術性論文. 質化 (說明:各成果項目請附佐證資料或細 單位 項說明,如期刊名稱、年份、卷期、起 訖頁數、證號...等) . 量化. 期刊論文. 0. 研討會論文. 0. 專書. 0 本. 專書論文. 0 章. 技術報告. 0 篇. 其他. 0 篇. 專利權 國 內. 發明專利. 申請中. 0. 已獲得. 0. 新型/設計專利. 篇. 0. 商標權 智慧財產權 營業秘密 及成果 積體電路電路布局權. 0. 著作權. 0. 品種權. 0. 其他. 0. 件數. 0 件. 收入. 0 千元. 技術移轉. 國 外. 研討會論文 專書. 0 本. 專書論文. 0 章. 技術報告. 0 篇. 其他. 0 篇. 專利權 智慧財產權 及成果. 0. The Journal of Thoracic and Cardiovascular Surgery 1 (accepted)(2017), doi: 篇 10.1016/j.jtcvs.2017.09.049. 7th World Congress of Pediatric 1 Cardiology & Cardiac Surgery, (WCPCCS). 期刊論文. 學術性論文. 0 件. 發明專利. 申請中. 0. 已獲得. 0. 新型/設計專利 商標權. 0 件 0. 營業秘密. 0.
(41) 技術移轉. 本國籍 參 與 計 畫 人 力 非本國籍. 積體電路電路布局權. 0. 著作權. 0. 品種權. 0. 其他. 0. 件數. 0 件. 收入. 0 千元. 大專生. 0. 碩士生. 0. 博士生. 0. 博士後研究員. 0. 專任助理. 1. 大專生. 0. 碩士生. 0. 博士生. 0. 博士後研究員. 0. 專任助理. 0. 其他成果 (無法以量化表達之成果如辦理學術活動 、獲得獎項、重要國際合作、研究成果國 際影響力及其他協助產業技術發展之具體 效益事項等,請以文字敘述填列。) . 人次. 助理林紹先.
(42) 科技部補助專題研究計畫成果自評表 請就研究內容與原計畫相符程度、達成預期目標情況、研究成果之學術或應用價 值(簡要敘述成果所代表之意義、價值、影響或進一步發展之可能性)、是否適 合在學術期刊發表或申請專利、主要發現(簡要敘述成果是否具有政策應用參考 價值及具影響公共利益之重大發現)或其他有關價值等,作一綜合評估。 1. 請就研究內容與原計畫相符程度、達成預期目標情況作一綜合評估 ■達成目標 □未達成目標(請說明,以100字為限) □實驗失敗 □因故實驗中斷 □其他原因 說明: 2. 研究成果在學術期刊發表或申請專利等情形(請於其他欄註明專利及技轉之證 號、合約、申請及洽談等詳細資訊) 論文:■已發表 □未發表之文稿 □撰寫中 □無 專利:□已獲得 □申請中 ■無 技轉:□已技轉 □洽談中 ■無 其他:(以200字為限) 3. 請依學術成就、技術創新、社會影響等方面,評估研究成果之學術或應用價值 (簡要敘述成果所代表之意義、價值、影響或進一步發展之可能性,以500字 為限) 我們利用聚四氟乙烯(Polytetrafluoroethene,PTFE)手工來裁剪縫製M形瓣 膜支架移植邊界與開窗孔的特殊設計肺動脈瓣膜,縫製在目前衛福部核准在病 患身上使用的支架人工血管(stent graft)上,並套入支架人工血管的套鞘 ,在全身麻醉下對小豬的股靜脈來完成使用經皮心導管(percutaneous transcatheter)方式植入新的肺動脈瓣膜。利用這種心導管植入肺動脈瓣膜法 (Transcatheter pulmonary valve replacement, TPVR)。這種方法是容易的 ,可重複的,和臨床可行的心導管瓣膜置換手術(TPVR)。而且透過動物實驗的 操作,也使團隊成員熟悉置放TPVR手術的步驟。這個計畫的結果除了已在今年 度的世界兒童心臟及心臟外科學大會(2017 WCPCCS)發表外,也完成論文投稿 到頂尖的心臟外科期刊(The Journal of Thoracic and Cardiovascular Surgery, JTCVS; 2016 Impact Factor: 4.446 Ranked 12/197 in Surgery)並已被接受刊登。.
(43) 4. 主要發現 本研究具有政策應用參考價值:■否 □是,建議提供機關 (勾選「是」者,請列舉建議可提供施政參考之業務主管機關) 本研究具影響公共利益之重大發現:□否 □是 說明:(以150字為限).
(44)
數據

+4

相關文件
Vulpes bengalensis (India) 孟加拉狐 (印度) Vulpes vulpes griffithi (India) 紅狐 (印度) Vulpes vulpes montana (India) 紅狐 (印度) Vulpes vulpes pusilla (India) 紅狐
Atretium schistosum (India) 綠滇西蛇 (印度) Cerberus rynchops (India) 波加丹蛇 (印度) Xenochrophis piscator (India) 草花蛇 (印度) Xenochrophis schnurrenbergeri
Vulpes bengalensis (India) 孟加拉狐 (印度) Vulpes vulpes griffithi (India) 紅狐 (印度) Vulpes vulpes montana (India) 紅狐 (印度) Vulpes vulpes pusilla (India) 紅狐
A factorization method for reconstructing an impenetrable obstacle in a homogeneous medium (Helmholtz equation) using the spectral data of the far-field operator was developed
Yesterday he was absent from school because he had a coldD. Yesterday the weather was
For 5 to be the precise limit of f(x) as x approaches 3, we must not only be able to bring the difference between f(x) and 5 below each of these three numbers; we must be able
[This function is named after the electrical engineer Oliver Heaviside (1850–1925) and can be used to describe an electric current that is switched on at time t = 0.] Its graph
A model of shape and motion model was learned from training sequences of hand motion against a plain background, tracked by Kalman filter (using signed.. The Condensation
