Falsely Low Hemoglobin A1c Values in Diabetic Patients Receiving Peginterferon-alpha and
Ribavirin for Chronic Hepatitis C
Yen-Kuang Tai
1, Chiu-Ling Huang
1, Chih-Ming Chien
1, Ching-Yang Tsai
2, and Hoi-Wan Lo
21
Division of Endocrinology and Metabolism, Department of Internal Medicine;
2
Division of Gastroenterology, Department of Internal Medicine, Yuan's General Hospital, Kaohsiung, Taiwan
Abstract
Hemoglobin A1c (A1C) values are usually lower during hemolysis because of the shortened red cell survival. Ribavirin (RBV) used in combination with peginterferon-alpha (peg-IFN) for chronic hepatitis C virus (HCV) infection causes reversible hemolytic anemia. This study was aimed to examine the effect of RBV treatment on A1C values in diabetic patients. A retrospective analysis identified 27 type 2 diabetic patients receiving peg-IFN and RBV for HCV. Each subject had at least three measures of hemoglobin (Hb), A1C, fasting plasma glucose, GPT and total bilirubin: before, during and after HCV therapy. During therapy, Hb levels decreased from 14.0 g/dL at baseline to a nadir of 10.2 g/dL (p < 0.001). A1C values decreased from a pre-treatment level of 7.1% to the lowest on-treatment level of 6.1% [mean paired difference: -1.0%; 95%
confidence interval (CI) -1.93 to -0.11; p = 0.023]. In contrast, matched fasting plasma glucose levels did not change significantly (mean paired difference: -4.4 mg/dL; 95% CI -26.9 to 18.2; p = 0.89). In addition, GPT decreased from a pre-treatment level of 129 U/L to an on-treatment level of 64 U/L (p < 0.001);
simultaneously measured total bilirubin increased from 0.82 mg/dL to 1.08 mg/dL (p = 0.016) supporting the occurrence of hemolysis. In conclusion, HCV therapy with peg-IFN plus RBV caused a significant fall in A1C values without a change to fasting plasma glucose levels in diabetic patients. The mean reductions of A1C values by 1.0% might be mostly caused by RBV-induced hemolysis. Falsely low A1C values may lead the clinicians to relax glycemic control inappropriately. Therefore, A1C should not be used to guide diabetes therapy during HCV treatment with RBV. (J Intern Med Taiwan 2011; 22: 431-437)
Key words: Hemoglobin A1c, Diabetes mellitus, Chronic hepatitis C, Ribavirin, Hemolytic anemia
Introduction
In patients with diabetes mellitus (DM), hemoglobin A1c (A1C) test is routinely used to estimate glycemic control over the previous 2-3
months. Recently, A1C is further recommended as one of diagnostic criteria of DM
1,2. However, there are clearly limitations in the measurement of A1C.
Interfering factor, such as hemolytic anemia, may cause unexpectedly low A1C value because of the
Reprint requests and correspondence:Dr. Yen-Kuang Tai
Address:Division of Endocrinology and Metabolism, Department of Internal Medicine, Yuan’s General Hospital, 162, Cheng-gong 1st Road, Kaohsiung 80211, Taiwan
shorter exposure of hemoglobin (Hb) to plasma glucose
3.
In addition to chronic hepatitis B virus infection, Taiwan is also a hyperendemic area of chronic hepatitis C virus (HCV) infection
4. According to a large-scale survey, the prevalence of HCV infection was 4.4% in Taiwan
5. There is growing evidence suggesting the mutual link between type 2 DM and HCV infection. The prevalence of DM had been reported in 18%
to 36% of patients with HCV infection, which was significantly higher than that in the general population
6-9. However, the impact of HCV therapy on the measurement of A1C has rarely been investigated. Oral ribavirin (RBV) plus peginterferon-alpha (peg-IFN) is the current standard therapy for chronic HCV infection.
Ribavirin alone has been shown to induce a dose-dependent, reversible hemolytic anemia
10,11. This anemia would be more pronounced with combination of IFN and RBV, because the myelosuppressive effect of IFN inhibits the bone marrow to compensate for RBV-induced hemolysis
12. In addition, the reimbursement criteria for HCV therapy has been loosened since November 2009 in Taiwan. There are more patients eligible for free treatment of HCV. In selected cases, the treatment duration can be extended up to 48 weeks. Diabetic patients on peg-IFN plus RBV therapy would be more commonly encountered in our daily clinical practice. It is unknown as to what extent RBV-induced hemolysis affects the A1C values in Taiwanese patients with diabetes. Hence, we try to conduct this study and investigate the reality of A1C values in diabetic patients under the treatment for HCV.
Materials and Methods
We retrospectively reviewed the medical records of 256 subjects receiving peg-IFN and RBV for HCV between January 2007 and February
2010. This study was approved by the Institutional Review Board of Yuan's General Hospital. A diagnosis of diabetes was confirmed based on the American Diabetes Association (ADA) criteria
1. Subjects were included in this analysis if HCV therapy lasted for a minimum of 12 weeks and included oral RBV given in combination with peg-IFN. In addition, subjects should have at least three measures of A1C, fasting plasma glucose, Hb, GPT and total bilirubin: before, during and after HCV therapy.
The A1C values were chosen at the following time points: the most recent one prior to HCV therapy (pre-treatment), at least 12 weeks after initiating therapy (on-treatment), and a minimum of 12 weeks after the end of therapy (post-treatment).
When more than one A1C value was identified between week 12 and the end of treatment, the lowest one was selected for analysis. To assess the matched mean glucose level to each A1C value, the fasting plasma glucose levels measured within 12 weeks before the pre-treatment and post-treatment A1C tests were collected; the fasting plasma glucose levels measured between 2 weeks before and after the on-treatment A1C test were obtained.
In addition, Hb, GPT and total bilirubin values were collected at the same time interval. Similarly, the lowest Hb value during HCV treatment was selected for analysis. Simultaneously measured GPT and total bilirubin were chosen on the same day with Hb measurement. Demographic data, baseline weight, anti-diabetic regimens, dose of peg-IFN and RBV, and duration of HCV therapy were also recorded.
Fasting plasma glucose, serum GPT and
total bilirubin were measured using an automatic
biochemistry analyzer (Beckman Coulter AU
2700; Mishima, Japan). Complete blood cell count
was measured using Beckman Coulter LH 750
(Miami, FL, U.S.A). A1C value was determined
by ion-exchange high-performance liquid
chromatography (HPLC) using HLC-723 G8 (Tosoh
corp., Tokyo, Japan).
Changes in A1C, fasting plasma glucose, Hb, GPT and total bilirubin levels were analysed using repeated-measures analysis of variance (ANOVA).
A comparison of these variables between two time points was tested for significance using paired t-test with Bonferroni adjustment for multiple testing.
A correlation between changes in A1C and Hb levels or baseline characteristics were measured using Pearson correlation test. All analyses were performed using SPSS for Windows (SPSS Inc., Version 14.0, Chicago, IL, USA).
Results
A total of 27 subjects with type 2 diabetes were included for this analysis. The baseline characteristics and therapeutic regimen for HCV are displayed in Table 1.
Following HCV therapy, the on-treatment Hb nadir occurred at a median of 16 weeks; the lowest on-treatment A1C values were obtained at a median of 19 weeks. As shown in Table 2, anemia defined as Hb < 10 g/dL occurred in one third of subjects;
low A1C value defined as less than 5% was noted in
Table 1. Baseline characteristics and therapeutic regimen for HCV
Variables N = 27
Age, years (mean ± SD) 56.6 ± 9.3
Sex, male [n (%)] 14 (51.9)
Weight, kg
*[median (range)] 70 (44-99)
Diabetes treatment [n (%)]
Diet 5 (18.5)
OAD 21 (77.8)
Insulin 1 (3.7)
Dose of peginterferon [n (%)]
2a (180 mcg/wk) 8 (29.6)
2b (80 mcg/wk) 19 (70.4)
Daily ribavirin dose, mg/d
*[median (range)] 800 (800-1200)
Daily weight-based ribavirin dose, mg/kg/d
*[median (range)] 14 (9.4-22.7)
Duration of HCV treatment, weeks
*[median (range)] 24 (14-48)
HCV, hepatitis C virus; SD, standard deviation; OAD, oral antidiabetic drug.
*
Variables are not normally distributed and are displayed at median (minimum- maximum) values.
Table 2. Changes in Hb and A1C after HCV therapy (N = 27)
Variables n (%)
Maximum Hb decline ≧ 3 g/dL 20 (74.1)
On-Rx Hb nadir < 10 g/dL 9 (33.3)
Maximum A1C decline ≧ 2 % 5 (18.5)
On-Rx A1C nadir < 5% 4 (14.8)
Pre-Rx A1C < 6.5% 10 (37.0)
On-Rx A1C nadir < 6.5% 18 (66.7)
Hb, hemoglobin; A1C, hemoglobin A1c; HCV, hepatitis C virus; Rx, treatment.
four subjects.
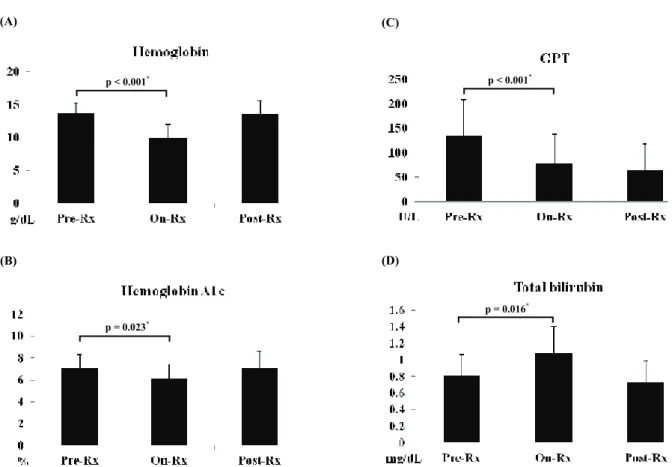
During peg-IFN plus RBV therapy, mean Hb levels decreased from 14.0 g/dL at baseline to a nadir of 10.2 g/dL [95% confidence interval (CI) -5.06 to -2.56; p < 0.001] (Fig.1A). A1C values decreased from a pre-treatment level of 7.1%
to the lowest on-treatment level of 6.1% with a mean difference of -1.0% (95% CI -1.93 to -0.11;
p = 0.023) (Fig. 1B). In contrast, matched fasting plasma glucose levels did not change significantly following HCV therapy with a mean difference of -4.4 mg/dL (95% CI -26.9 to 18.2; p = 0.89) (Figure 2). In addition, GPT decreased from a mean pre-treatment level of 129 U/L to an on-treatment level of 64 U/L (p < 0.001); mean total bilirubin increased from 0.82 mg/dL to 1.08 mg/dL (p = 0.016) (Fig.1C and 1D).
Following HCV therapy, the change in A1C values was not correlated either to the decline in Hb levels (r = 0.249, p = 0.210) or other baseline variables, such as pretreatment A1C (r = 0.304, p = 0.123) and Hb levels (r = -0.084, p = 0.679), weight (r
= -0.044, p = 0.851), daily RBV dose (r = -0.124, p = 0.537), and duration of therapy (r = 0.106, p = 0.599).
Fig 1. Hemoglobin (A), hemoglobin A1c (B), GPT (C) and total bilirubin (D) before, during, and after hepatitis C therapy.
Rx, treatment. p < 0.001 in panel A, C and D; p = 0.007 in panel B with repeated-measures ANOVA. Comparisons by paired t-test (*) with Bonferroni adjustment for multiple testing.
18 (A)
p < 0.001*
Fig 2. Fasting plasma glucose before, during, and after hepatitis C therapy. Rx, treatment. p = 0.866 with repeated-measures ANOVA. A comparison by paired t-test (*) with Bonferroni adjustment for multiple testing.
22 p = 0.89*
19 (B)
p = 0.023*
20 (C)
p < 0.001*
21 (D)
p = 0.016*
19 (B)
p = 0.023*
19 (B)
p = 0.023*