Open Access
Research article
Rare clinical experiences for surgical treatment of melanoma with
osseous metastases in Taiwan
Kuo-Yuan Huang
1, Chrong-Reen Wang
2and Rong-Sen Yang*
3Address: 1Department of Orthopaedics and Institute of Clinical Medicine, College of Medicine, National Cheng Kung University Medical Center,
Tainan city, Taiwan, 2Section of Rheumatology and Immunology, Department of Internal Medicine, College of Medicine, National Cheng Kung
University Medical Center, Tainan city, Taiwan and 3Department of Orthopaedics, College of Medicine, National Taiwan University Medical
Center, Taipei city, Taiwan
Email: Kuo-Yuan Huang - [email protected]; Chrong-Reen Wang - [email protected]; Rong-Sen Yang* - [email protected] * Corresponding author
Abstract
Background: Malignant melanoma occurs infrequently in Taiwan. Once it has progressed into osseous metastases, the prognosis is poor. There are no reported clinical experiences of surgical management in this area.
Methods: To improve our understanding of the rare clinical experiences, we retrospectively investigated clinical characteristics, radiological findings, treatment modalities, survival outcomes and prognoses of 11 Taiwanese patients with osseous metastasis of melanoma treated surgically at two national medical centers, National Taiwan University Hospital and National Cheng Kung University Hospital from January 1983 to December 2006.
Results: Six patients suffered from acral-lentiginous melanoma. Nine patients sustained multiple osseous metastases and most lesions were osteolytic. Nine patients also had sustained metastases to other organs including liver, lungs, lymph nodes, brain and spleen. Second malignancies including lung cancer, thyroid papillary carcinoma, renal cell carcinoma and cervical cancer co-existed in four patients. The interval from the initial diagnosis of melanoma to the clinical detection of osseous metastases varied from 0–37.8 months (mean 9.75 months). Metastatic melanoma was invariably fatal; the mean survival time from bone metastases to death was 5.67 months.
Conclusion: Due to the high morbidity and poor survival of Taiwanese patients with osseous metastases of melanoma, surgical treatment should be directed towards pain relief and the prevention of skeletal debilitation in order to maintain their quality of life.
Background
After melanoma has grown radially and superficially in the epidermis and on mucosal surfaces, it can metastasize to any organ or tissue such as the lungs and bone, where melanoma metastases are common [1,2]. Melanoma most frequently occurs in fair-skinned Caucasian individ-uals older than 40 years who have numerous moles [3]. In
most countries, the incidence of melanoma has been increasing recently, with annual incidences reaching 3– 7% among fair-skinned populations [3,4]. In the United States, the incidence of melanoma has increased more than that of any other cancer [5]. An estimated 60,000 new cases of melanoma are diagnosed each year with more than 8,000 annual deaths in the United States;
Published: 25 July 2007
BMC Musculoskeletal Disorders 2007, 8:70 doi:10.1186/1471-2474-8-70
Received: 11 July 2007 Accepted: 25 July 2007 This article is available from: http://www.biomedcentral.com/1471-2474/8/70
© 2007 Huang et al; licensee BioMed Central Ltd.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
BMC Musculoskeletal Disorders 2007, 8:70 http://www.biomedcentral.com/1471-2474/8/70
Page 2 of 7 (page number not for citation purposes) about one in 75 persons will develop this cancer in their
lifetime [5,6]. After osseous metastases occur, the patient's survival is usually short-term [7,8]. In addition, bone metastases of melanoma predispose patients to patholog-ical fractures of axial and appendicular skeletons, bone marrow failure and neurological deficits. These complica-tions substantially increase their pain and result in a poor quality of life [6,7,9].
Despite its high mortality rate, melanoma is not well stud-ied in Asians, with only a limited number of reported cases [10]. Acral-lentiginous melanoma (ALM) is the most common subtype of melanoma in Asian populations including Taiwanese [11]. The diagnosis of this subtype is often delayed [11,12]. We conducted this retrospective chart review in two national medical centers in Taiwan to improve our understanding of the incidence, treatment and outcomes of osseous metastases of melanoma in Asia.
Methods
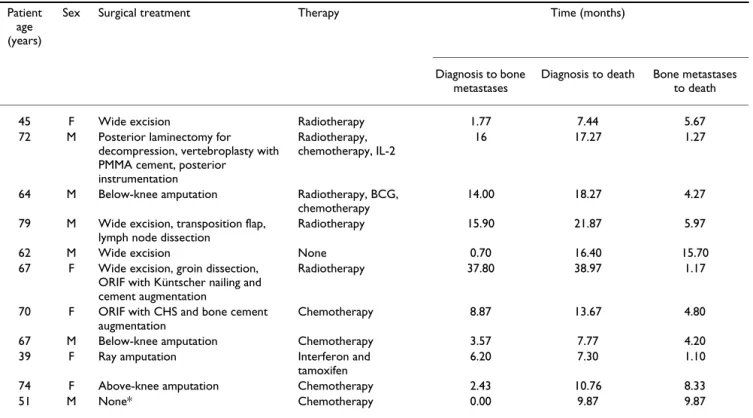
The hospital records of the National Taiwan University Hospital and the National Cheng Kung University Hospi-tal from January 1983 to December 2006 were surveyed to identify cases of malignant melanoma. We reviewed the charts, medical records, surgical notes, radiological images and pathology records of patients diagnosed with osseous metastases. A total of 11 patients underwent sur-gical intervention for osseous metastases. Sursur-gical indica-tions in our series included an intractable skin ulcer, mechanical instability due to pathologic fractures, neuro-logical deterioration due to neural compression by metas-tases, pain unresponsive to nonoperative measures such as radiation and the need for biopsy material for his-topathological verification of the diagnosis. The choice of surgical procedure depended on the patients' individual clinical situation, location of the tumor, medical comor-bidities and overall prognosis. Surgical treatments included wide excision (four patients), posterior laminec-tomy for decompression and posterior instrumentation (one patient), below-the-knee amputation (two patients), above-the-knee amputation (one patient), ray amputa-tion (one patient) and intralesional excision plus internal fixation with cement augmentation (two patients) (Tables 1 &2).
All patients had histopathological proof of bone tases. Table 1 lists the locations of their osseous metas-tases, and Table 2 shows the operations performed. Adjuvant therapies after surgical treatment varied depend-ing on the patient's age, the sites and number of metas-tases, disease progression, the patient's overall medical condition and the patient's intentions for further manage-ment. Table 2 lists the adjuvant therapies including chem-otherapy with or without tamoxifen (six patients), radiotherapy (five patients) and immunotherapy with
Bacillus Calmette-Guérin (BCG), interferon alpha or IL-2 (three patients).
We compiled data on the age and sex distribution of these patients, their primary lesions, clinical sizes, microscopic classification with depth of invasion (Clark level), bone metastases and complications, radiographic manifesta-tions, other metastases, synchronous tumors, usages of analgesic medications, interval from initial diagnosis to occurrence of osseous metastases, interval from diagnosis to death and survival after the occurrence of bone metas-tases.
Results
The 11 patients (six men and five women) ranged in age from 39–79 years (mean 61.8 years) at the time of diagno-sis of melanoma. Six patients had the ALM subtype. The metastases of the melanoma were correlated with the severity of the primary cutaneous lesions (Table 1). One patient who did not possess a primary cutaneous lesion had a melanoma of the navicular bone (Fig. 1), with an initial presentation of dull pain in the right midfoot that lasted six months. Most patients had pain and weakness in the involved regions. Osteolytic bone lesions were radi-ographically detected in 10 patients. Osteosclerosis of the thoracolumbar spine was also found (Table 1). Most lesions in the long bones were multiple, eccentric and oval, with clinically significant cortical erosion (Fig. 2). Two patients had permeated osteolytic lesions; such a pat-tern was characterized by numerous, tiny radiolucencies between the trabeculae of the residual bones. Periosteal reactions and dystrophic calcifications were found in one patient with multiple sites of bony destruction in the ileum and sacrum.
The osseous metastases were in the axial skeleton in eight patients, six of whom had spinal metastases. Two patients had osseous metastases to the cervical spine, four to the thoracic spine, six to the lumbar spine, two to the scapula, three to the ribs, four to the pelvis and three to the skull. Compression fractures with epidural compression occurred in three patients with spinal metastases. One patient received posterior laminectomy for decompres-sion and posterior instrumentation because of progressive muscle power weakness of right lower limb (Fig. 3). The other two patients received irradiation instead of laminec-tomy because of their poor medical condition. The appen-dicular skeletons were involved in six patients, with bone metastases to the femur in four patients, to the tibia in two and to the navicular bone in one. Four patients had path-ological fractures including one each in the subtro-chanteric region of the femur, the midshaft of the femur, the midshaft of the tibia, and the navicular bone. Two patients with femoral fractures were successfully treated with intralesional excision and internal fixation with
200 7, 8 :70 http ://www.bio m e dcent ral.com/147 1-247 Page (page nu mber not for cit a tion pur
(years) tumor (cm) classification (Clark level) complications tumor
45 F Scalp 1.5 × 1.0 Malignant melanoma V Frontoparietal skull, multiple cervico- thoracolumbar spine (compression fractures of thoracolumbar spine), bone
marrow infiltration
Multiple spinal metastases with bony destruction and
cord compression Liver, bone marrow None 72 M L anterior chest wall
1.5 × 1.5 Malignant melanoma IV 5th lumbar vertebra, R acetabulum L5 compression fracture
with bony destruction
Lung, Lymph nodes
None
64 M R sole 1.5 × 1.5 acral lentiginous melanoma
V L skull base, midcervical, mid thoracolumbar spine
Multiple bony destruction, permeative osteolytic skull
lesion
Lung None
79 M L sole 1.0 × 1.0 acral lentiginous melanoma
III R scapular, thoracolumbar spine (L2 compression fracture), L sacroiliac joint, pelvic rim and
bilateral femurs
Multiple bony destruction with periosteal reaction and
dystrophic calcifications
Lymph nodes Lung cancer
62 M L sole 2.3 × 2.1 acral lentiginous melanoma
IV L ninth rib, thoracolumbar spine Sclerotic lesions in thoracolumbar spine
Liver Thyroid papillary carcinoma, renal cell carcinoma
67 F R heel 3.5 × 1.0 acral lentiginous melanoma
V R femoral pathological fracture, R knee, L mid femur, R scapular, rib
Permeative osteolytic change Lymph node, lung, liver
None
70 F L lower leg 1.0 × 1.0 Malignant melanoma IV L femoral subtrochanteric fracture Osteolytic bony destruction Liver, spleen Renal cell carcinoma
67 M R foot 7.0 × 6.0 acral lentiginous melanoma
V R tibia, proximal femur Increased tracer uptake over R proximal femur
Lung, lymph nodes
None
39 F L subungual 1.1 × 0.9 acral lentiginous melanoma
V Skull, thoracolumbar spine, thoracic cage, pelvic rim
Osteolytic bony destruction Liver, lung, lymph nodes, brain
None
74 F L lower limb 1.0 × 0.8 Malignant melanoma V L midtibial pathological fracture, sacroiliac joint
Osteolytic bony destruction Lung Cervical cancer
51 M Unknown NA Malignant melanoma NA R navicular pathological fracture Comminuted fracture Liver, lung, lymph nodes
None
BMC Musculoskeletal Disorders 2007, 8:70 http://www.biomedcentral.com/1471-2474/8/70
Page 4 of 7 (page number not for citation purposes) pression hip screws and Küntscher nailing augmented
with cement fixation. The patient with the tibia fracture was treated with above-the-knee amputation because of multiple skin lesions and ulcers. The patient with the navicular fracture underwent conservative treatment with chemotherapy alone because of the coexistence of several distant metastases.
All 11 patients had metastases other than osseous metas-tases from their melanomas. Four patients had a synchro-nous malignancy including one lung cancer, one thyroid papillary carcinoma, two renal cell carcinomas and one cervical cancer. The synchronous malignancy usually occurred first and then co-existed with the melanoma (Table 1). The use of analgesic medications was decreased after the operations, and most patients reported signifi-cant alleviation of pain after surgical intervention. Dra-matic pain relief was achieved in three patients with pathological fractures who received internal fixation. The interval from the diagnosis of melanoma to the detec-tion of osseous metastases varied from 0–37.8 months (mean 9.75 months) (Table 2). The prognosis of patients with melanoma and osseous metastases was generally poor. After osseous metastasis had been diagnosed, the mean survival was only 5.67 months (Table 2). We found no significant differences in prognosis between the axial
and appendicular osseous metastases (mean survival 5.44 and5.72 months, respectively). The average survival time of males (6.88 months) was longer than females (4.21 months). There was no obvious correlation between age and survival. The survival time of six patients with the ALM subtype averaged 5.40 months, which was only slightly shorter than that of the other five patients (5.99 months). Even in patients with a synchronous tumor, the prognosis did not deteriorate. There were no distinct dif-ferences in survival among patients receiving chemother-apy, radiotherapy and/or immunotherapy.
Discussion
Osseous metastases of malignant melanoma are rare among Asians [10,11]. Six of our patients had ALM, which has the predilection to occur on the palms, soles and sub-ungual nail beds. Such a distribution usually delays diag-nosis and patients accordingly have worsened prognoses. Indeed, presently we found that the survival time of ALM patients (5.4 months) was slightly shorter than that of other subtypes (5.99 months). Osseous metastases from malignant melanoma usually occur in patients with rela-tively advanced primary lesions and multiple bony lesions at the time of diagnosis [12-14], as shown in the histopathological findings of our series with a Clark level of III, IV or V. Until now, there has not been evidence to support the conclusion that the surgical treatment con-Table 2: Surgical treatments and outcomes
Patient age (years)
Sex Surgical treatment Therapy Time (months)
Diagnosis to bone metastases
Diagnosis to death Bone metastases to death
45 F Wide excision Radiotherapy 1.77 7.44 5.67
72 M Posterior laminectomy for decompression, vertebroplasty with PMMA cement, posterior
instrumentation
Radiotherapy, chemotherapy, IL-2
16 17.27 1.27
64 M Below-knee amputation Radiotherapy, BCG, chemotherapy
14.00 18.27 4.27
79 M Wide excision, transposition flap, lymph node dissection
Radiotherapy 15.90 21.87 5.97
62 M Wide excision None 0.70 16.40 15.70
67 F Wide excision, groin dissection, ORIF with Küntscher nailing and cement augmentation
Radiotherapy 37.80 38.97 1.17
70 F ORIF with CHS and bone cement augmentation
Chemotherapy 8.87 13.67 4.80
67 M Below-knee amputation Chemotherapy 3.57 7.77 4.20
39 F Ray amputation Interferon and tamoxifen
6.20 7.30 1.10
74 F Above-knee amputation Chemotherapy 2.43 10.76 8.33
51 M None* Chemotherapy 0.00 9.87 9.87
BCG, Bacillus Calmette-Guérin; ORIF, open reduction and internal fixation. *Diagnosed with fine-needle biopsy.
tributes to the survival of metastatic melanoma patients [1,8,15]. Therefore, management is directed towards the relief of symptoms and the maintenance of a good quality of life in patients with osseous metastases of melanoma. Primary melanoma of the bone has been rarely reported in the literature [16]. In isolated appendicular osseous metastases of melanoma, survival may be prolonged after aggressive surgical resection of the metastatic bony focus
[17]. Common sites for osseous metastases of melanoma include the vertebrae, skull, pelvis, thoracic cage and prox-imal parts of the femur [18-22]. Osseous metastases gen-erally occur in the axial skeleton; reflecting this, there were eight cases among the 11 patients presently studied. Spi-nal metastases may result in vertebral compression frac-tures, epidural or cord compression (Fig. 3) [6,7,9]. For patients with neurological deficits such as paraplegia or cauda equina syndrome, the neurological decompression to relieve symptoms and recover functions should be con-sidered as health permits. Moreover, simultaneous instru-mentation or vertebroplasty with polymethylmethacrylate (PMMA) cement can provide spinal stability to alleviate back pain in patients with pathological vertebral fractures. Intralesional excision or curettage of osseous metastatic melanoma lesions together with open reduction and internal fixation with PMMA cement augmentation might be an effective strat-egy for the surgical management of pathological fractures in the appendicular skeleton. Two patients in our series received such an intervention and obtained significant pain relief. Metastatic lesions within the long bones are usually multiple, osteolytic, eccentric and oval, and are associated with clinically significant cortical erosion [15]; this was evident in our cases (Fig. 2). Lesions usually appear first in the medullary cavity, and then spread to destroy the bone trabeculae, extend to the cortex and finally lead to pathological fractures (Fig. 2) [14,15]. However, such radiographic features in our patients were similar to those in other cancers.
Because melanoma with osseous metastases is heteroge-neous in its biology, treatment plans must be highly indi-(a). Plain radiograph of a 74-year-old woman
Figure 2
(a). Plain radiograph of a 74-year-old woman. The radio-graph reveals a pathologic fracture at the diaphysis of the left tibia due to an osteolytic lesion in the medullary cavity. (b). T1-weighted magnetic resonance image showing several tibial lesions that are eccentric, oval and associated with clinically significant cortical erosion. (c). T1-weighted magnetic reso-nance image demonstrating a hypointense lesion with endo-steal scalloping of the tibia and cortical erosion.
Magnetic resonance image of lumbosacral spine showing a compression fracture of L5 of posterior bulging contour with enhancement and epidural soft tissue mass over the anterior epidural space with marked compression of the thecal sac Figure 3
Magnetic resonance image of lumbosacral spine showing a compression fracture of L5 of posterior bulging contour with enhancement and epidural soft tissue mass over the anterior epidural space with marked compression of the thecal sac. Pathologic fracture of the right naviculum in a 51-year-old
man with melanoma presented at the initial visit Figure 1
Pathologic fracture of the right naviculum in a 51-year-old man with melanoma presented at the initial visit.
BMC Musculoskeletal Disorders 2007, 8:70 http://www.biomedcentral.com/1471-2474/8/70
Page 6 of 7 (page number not for citation purposes) vidualized. Surgical management is generally followed by
adjuvant therapies such as chemotherapy, radiation ther-apy or immunotherther-apy. Single or combined chemother-apy does not improve survival in advanced-stage disease, as evident presently and reported previously [1,8,10]. External beam radiotherapy is effective in preventing local recurrence of malignant melanoma and can provide palli-ative treatment for metastatic melanoma [23]. In our cases, irradiation of the affected areas relieved pain con-siderably for several months without affecting the growth of tumor, similar to previous reports [10,15]. Significant proportions of melanoma cells express estrogen receptors, which leds to a supportive role for tamoxifen in the treat-ment of metastatic melanoma [8]. Given their immuno-logic effects, low-dose interleukin-2, granulocyte-monocyte colony stimulating factor and interferon alpha-2b produce durable remissions in patients with metastatic melanoma, and they have been used as postoperative adjuvant therapies [24]. Therefore, the goal of surgical treatment for osseous metastases of melanoma should be directed towards the palliation of symptoms, particularly if the anticipated relief of related symptoms exceeds the potential adverse effects of the therapy. Symptomatic metastases in weight-bearing bones require special con-sideration. For large lesions or cortical destruction, pro-phylactic stabilization and irradiation are preferred. Alternatively, the lesion may be treated with radiation alone and patients are monitored for evidence of patho-logic fractures. Unless the risk of surgery is high or the expected life span is short, pathologic fractures of weight-bearing bones should be stabilized to maximize the qual-ity of life and decrease hospital costs. Furthermore, surgi-cal resection can produce an immediate decrease in tumor burden at a reasonable expenditure [25].
Bisphosphonates such as pamidronate and zoledronic acid have been used for palliative therapy in patients with osteolytic lesions metastasized from multiple myeloma or metastatic breast cancer. The aim is to prevent or delay the onset of skeletal complications [26,27]. Moreover, bisphosphonates can reduce bone pain in patients with bony metastases [28]. Zoledronic acid has demonstrated efficacy in the treatment of bone metastases in patients with prostate cancer, lung cancer or other solid tumors [26]. The bisphosphonate pamidronate induces apoptosis in human melanoma cells in vitro [29]. In an in vivo ani-mal study, incadronate inhibited bone resorption by increasing numbers of apoptotic osteoclasts [30]. In addi-tion, incadronate can substantially suppress the growth of human melanoma cells, increase the numbers of apopto-sis of tumor cells and decrease the tumor-associated blood-vessel density [30]. Therefore, bisphosphonate therapy might be an alternative to surgery or an adjuvant treatment for osseous metastatic melanoma in the future.
The prognosis of patients with melanoma is related to the extent and the stage of the tumor. Early detection and management of melanoma are the key factors to improve overall survival. The prognosis is poor after melanoma progresses and undergoes osseous metastasis [2,31]. Osseous metastases of melanoma may predispose indi-viduals to pathologic fractures in the axial or appendicular bones or to bone marrow failure and may substantially influence the quality of life and survival expectancy of patients. For Asian patients with melanoma, the mean survival after the diagnosis of osseous metastases was 5.67 months in our series, which was longer than 4.7 months reported in Caucasian populations [2,7,31].
Conclusion
In conclusion, osseous metastases of melanoma are rare in Taiwan and the prognoses of patients are as poor as with Caucasians. Surgical intervention is effective in pro-viding pain relief, especially for those with pathological fracture and those receiving internal fixation. Due to the high morbidity and poor survival, surgical treatment should be directed towards pain relief and the prevention of skeletal debilitation in order to maintain a patient's quality of life.
Competing interests
The author(s) declare that they have no competing inter-ests.
Authors' contributions
KYH conceived the study, participated in its design, col-lected the data, and drafting of the manuscript.
CRW did the data analysis, and revised the manuscript. RSY assisted in the creation and design of the study, col-lected the data, advised and assisted drafting of the man-uscript.
All authors read and approved the final manuscript.
References
1. Atkins MB: The treatment of metastatic melanoma with chemotherapy and biologics. Curr Opin Oncol 1997, 9:205-213. 2. Barth A, Wanek LA, Morton DL: Prognostic factors in 1,521
melanoma patients with distant metastases. J Am Coll Surg 1995, 181:193-201.
3. Brochez L, Naeyaert JM: Understanding the trends in melanoma incidence and mortality: where do we stand? Eur
J Dermatol 2000, 10:71-75.
4. Hall HI, Miller DR, Rogers JD, Bewerse B: Update on the inci-dence and mortality from melanoma in the United States. J
Am Acad Dermatol 1999, 40:35-42.
5. Jemal A, Siegel R, Samuels A, Ward E, Murray T, Xu J, Thun MJ: Can-cer statistics, 2007. CA CanCan-cer J Clin 2007, 57:43-66.
6. Chatelain D, de Pinieux G, Guillemette J, Forest M: Bone metasta-sis of a clear cell tumor. Ann Pathol 1999, 19:139-140.
7. Motzkin NE, Rock MG, Wold LE, Beabout JW: Malignant melanoma metastatic to bone. Orthopedics 1992, 15:657-659.
Publish with BioMed Central and every scientist can read your work free of charge "BioMed Central will be the most significant development for disseminating the results of biomedical researc h in our lifetime."
Sir Paul Nurse, Cancer Research UK
Your research papers will be:
available free of charge to the entire biomedical community peer reviewed and published immediately upon acceptance cited in PubMed and archived on PubMed Central yours — you keep the copyright
Submit your manuscript here:
http://www.biomedcentral.com/info/publishing_adv.asp
BioMedcentral
8. O'Day SJ, Kim CJ, Reintgen DS: Metastatic melanoma: chemo-therapy to biochemochemo-therapy. Cancer Control 2002, 9:31-38. 9. Kato N, Kimura K, Sugawara H, Aoyagi S, Kondo K, Yamashiro K:
Pedunculated melanoma with pulmonary and bony metas-tases. J Dermatol 2000, 27:769-773.
10. Lange JR, Sharfman WH, Alani RM, Balch CM: melanoma. In Clinical Oncology 3rd edition. Churchill Livingstone; 2004:1561-1583. 11. Chen YJ, Wu CY, Chen JT, Shen JL, Chen CC, Wang HC:
Clinco-pathologic analysis of malignant melanoma in Taiwan. J Am
Acad Dermatol 1999, 41:945-9.
12. O'Connell ME, Powell BW, O'Connell JM, Harmer CL: Spontane-ous regression of multiple bone metastases in malignant melanoma. Br J Radiol 1989, 62:1095-1100.
13. Potepan P, Spagnoli I, Danesini GM, Laffranchi A, Gadda D, Masch-eroni L, Guzzon A: The radiodiagnosis of bone metastases from melanoma. Radiol Med 1994, 87(6):741-746.
14. Salwen WA, Krementz ET, Campeau RJ: Bone and liver imaging in regionally advanced melanoma. J Surg Oncol 1989, 42:225-228.
15. Brountzos EN, Panagiotou IE, Bafaloukos D, Kelekis DA: Bone metastases from malignant melanoma: a retrospective review and analysis of 28 cases. Radiol Oncol 2001, 35:209-214. 16. Yokoyama R, Mukai K, Hirota T, Beppu Y, Fukuma H: Primary
malignant melanoma (clear cell sarcoma) of bone: report of a case arising in the ulna. Cancer 1996, 77:2471-2475.
17. DeBoer DK, Schwartz HS, Thelman S, Reynolds VH: Heterogene-ous survival rates for isolated skeletal metastases from melanoma. Clin Orthop 1996, 323:277-283.
18. Downey MS, Lamm BM: Metastatic malignant melanoma to the foot and ankle: a review of the literature and case report. J
Foot Ankle Surg 2000, 39:392-401.
19. Jaeger HJ, Kruegener GH, Donovan AG: Patellar metastasis from a malignant melanoma. Int Orthop 1992, 16:282-284.
20. Laredo J, Morris DJ, Thurer RL: Metastatic melanoma to the manubrium sternum. Eur J Cardiothorac Surg 1998, 14:629-630. 21. Tamburri SA, Boberg JS: Skeletally metastatic malignant
melanoma of the foot. J Foot Ankle Surg 1994, 33:368-372. 22. Tandogan RN, Aydogan U, Demirhan B, Arican A, Yuceturk A:
Intra-articular metastatic melanoma of the right knee. Arthroscopy 1999, 15:98-102.
23. Seegenschmiedt MH, Keilholz L, Altendorf-Hofmann A, Urban A, Schell H, Hohenberger W, Sauer R: Palliative radiotherapy for recurrent and metastatic malignant melanoma: prognostic factors for tumor response and long-term outcome: a 20-year experience. Int J Radiat Oncol Biol Phys 1999, 44:607-18. 24. de Gast GC, Batchelor D, Kersten MJ, Vyth-Dreese FA, Sein J, van de
Kasteele WF, Nooijen WJ, Nieweg OE, de Waal MA, Boogerd W: Temozolomide followed by combined immunotherapy with GM-CSF, low-dose IL2 and IFN alpha in patients with meta-static melanoma. Br J Cancer 2003, 88:175-180.
25. Young SE, Martinez SR, Essner R: The role of surgery in treat-ment of stage IV melanoma. J Surg Oncol 2006, 94:344-51. 26. Berenson JR: Recommendations for zoledronic acid
treat-ment of patients with bone metastases. Oncologist 2005, 10:52-62.
27. Lipton A, Theriault RL, Hortobagyi GN, Simeone J, Knight RD, Mel-lars K, Reitsma DJ, Heffernan M, Seaman JJ: Pamidronate prevents skeletal complications and is effective palliative treatment in women with breast carcinoma and osteolytic bone metas-tases: long term follow-up of two randomized, placebo-con-trolled trials. Cancer 2000, 88:1082-90.
28. Wong R, Wiffen PJ: Bisphosphonates for the relief of pain sec-ondary to bone metastases. Cochrane Database Syst Rev 2002:CD002068.
29. Riebeling C, Forsea AM, Raisova M, Orfanos CE, Geilen CC: The bisphosphonate pamidronate induces apoptosis in human melanoma cells in vitro. Br J Cancer 2002, 87:366-71.
30. Kitagawa Y, Hiraga T, Yura Y, Yoneda T: Suppression by incadro-nate of invasion and growth of A-375 human melanoma in mandible in nude mice. Oncol Rep 2005, 13:211-6.
31. Reintgen DS, Cox C, Slingluff CJ, Seigler HF: Recurrent malignant melanoma: the identification of prognostic factors to predict survival. Ann Plast Surg 1992, 28:45-49.
Pre-publication history
The pre-publication history for this paper can be accessed here: