C A S E R E P O R T Open Access
Recurrent tertiary hyperparathyroidism due to supernumerary parathyroid glands in a patient receiving long-term hemodialysis: a case report
Tsai-Sung Tai1, Yueh-Han Hsu1,2,3* , Jia Ming Chang4and Chien-Chin Chen5,6
Abstract
Background: Renal hyperparathyroidism is a common complication of chronic kidney disease (CKD) or end-stage renal disease (ESRD) characterized by elevated parathyroid hormone levels secondary to derangements in the homeostasis of calcium, phosphate, and vitamin D. Rapid correction of severe and prolonged hyperparathyroidism by surgical parathyroidectomy in long-term hemodialysis patients occasionally causes hungry bone syndrome. These patients then exhibit severe and long-lasting secondary or tertiary hyperparathyroidism with high bone turnover.
Case presentation: We report a case of recurrent tertiary hyperparathyroidism after total parathyroidectomy due to supernumerary parathyroid gland in a patient with long-term hemodialysis. Supplementation with intravenous calcium, oral calcium, and vitamin D immediately after patient surgery helps to prevent and treat hungry bone syndrome.
Conclusions: We should prompt a search for the supernumerary parathyroid glands in ESRD patients, who have recurrent or persistent hyperparathyroidism after total parathyroidectomy. ESRD patients are more likely to develop hungry bone syndrome after parathyroidectomy. Prevention and treatment of hungry bone syndrome may be required after ectopic parathyroidectomy in clinical practice.
Keywords: Hemodialysis, Supernumerary parathyroid glands, Parathyroidectomy, Tertiary hyperparathyroidism, Hungry bone syndrome, Case report
Background
Secondary and tertiary hyperparathyroidism occurs com- monly in patients with chronic kidney disease (CKD) or end-stage renal disease (ESRD). Previous estimates reported as many as 90% of patients with CKD devel- oped secondary or tertiary hyperparathyroidism by the time they started hemodialysis [1]. Tertiary hyperpara- thyroidism is a state of autonomously functioning para- thyroid tissue typically manifesting as hypercalcemia after either prolonged secondary hyperparathyroidism or successful renal transplantation [2]. Although most of
the parathyroid glands are located in eutopic locations, less common ectopic anatomic localization due to vari- able embryologic migration patterns of the parathyroid glands might occur. Patients with ectopic anatomic localization constitute an etiology of persistent or recur- rent hyperparathyroidism after total parathyroidectomy.
The incidence of supernumerary parathyroid glands is reported to be between 14.4 and 15% [3, 4]. The most common location of supernumerary parathyroid glands is within the thymus [5].
We report a case of recurrent tertiary hyperparathyr- oidism after total parathyroidectomy due to super- numerary parathyroid glands in a patient with long-term hemodialysis.
* Correspondence:cych07023@gmail.com
1Department of Internal Medicine, Ditmanson Medical Foundation Chia-Yi Christian Hospital, 539 Chung Hsiao Rd, Chiayi City 600, Taiwan
2Department of Medical Research, Ditmanson Medical Foundation Chia-Yi Christian Hospital, 539 Chung Hsiao Rd, Chiayi 600, Taiwan
Full list of author information is available at the end of the article
© The Author(s). 2019 Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
Tai et al. BMC Endocrine Disorders (2019) 19:16 https://doi.org/10.1186/s12902-019-0346-7
Case presentation
A 74-year-old Taiwanese man had ESRD secondary to essential hypertension and started hemodialysis therapy since 2002 until now. On 16 June 2005, parathyroid investigations showed the following values: serum intact parathyroid hormone (i-PTH) concentration of 757 pg/
ml (reference range 10–73), serum total calcium concen- tration of 11.2 mg/dl (reference range 8.4–10.2), and serum phosphate concentration of 6.5 mg/dl (reference range 2.7–4.5). As a result, the patient was diagnosed as having tertiary hyperparathyroidism. The ultrasound examination of parathyroid glands revealed the right inferior parathyroid gland 15.5 × 12.0 × 11.9 mm in size and the left inferior parathyroid glands 21.6 × 12.3 × 7.4 mm in size. The patient did not receive the examination of parathyroid scan with Tc-99 m MIBI.
On 5 December 2007, endocrine surgeon performed parathyroidectomy to remove all four parathyroid glands and transplanted right superior parathyroid gland into the subcutaneous fat over the internal part of the right thigh. The pathology of the right and left inferior parathyroid glands showed oxyphil cells and chief cell hyperplasia of both parathyroid tissues. Pre-operative laboratory tests revealed serum i-PTH of 2148 pg/ml, serum total calcium of 11 mg/dl, and serum phosphate of 13.6 mg/dl. Post-operative laboratory tests showed serum i-PTH of 71 pg/ml, serum total calcium of 5.9 mg/dl, and serum phosphate of 8.0 mg/dl.
In December 2017, the patient was found to have elevated i-PTH concentration again to 1135.9 pg/ml, hypercalcemia (total calcium 11.0 mg/dl) and hyperpho- sphatemia (phosphate 8.4 mg/dl). Therefore, we performed
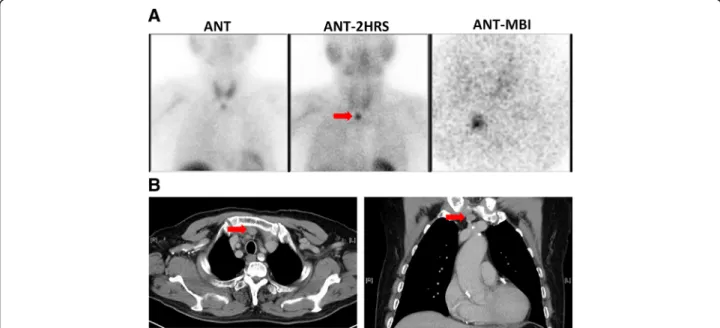
parathyroid scan with Tc-99 m MIBI and scanned with early and delayed imaging, which showed focal tracer up- take in retrosternal region (Fig.1A). There was no evidence of recurrent parathyroid gland in the neck or right thigh.
Besides, the patient did not have sterna related symptoms or physical findings. So, we suspected ectopic functioning parathyroid gland in the retrosternal region. Post contrast chest and mediastinal computed tomography (CT) scan showed a nodule around 1.3 cm in size in the retrosternal region (Fig.1B), which can be consistent with an ectopic parathyroid gland. Both investigations revealed evidence of an ectopic parathyroid gland in the retrosternal region.
On 27 February 2018, a thoracic surgeon performed a neck incision with partial sternotomy and resection of a 1.5 cm mediastinal nodule at the upper mediastinal above the left innominate vein and thymus. The ectopic parathyroid gland is located extra-thymic because we didn’t find any thymic tissue in the histological examin- ation of the resected specimen. Microscopic examination of the specimen showed a parathyroid gland composed of nodular hyperplasia of oxyphil cells and chief cells.
Immunohistochemically, the parathyroid gland was posi- tive for GATA-3, while negative for CD5 and synapto- physin (Fig.2). The pathologic findings were compatible with a diagnosis of an ectopic mediastinal parathyroid gland. We compared the laboratory tests between pre-operation and the second post-operative day: serum i-PTH level decreased from 1135.9 pg/ml to 272.7 pg/ml, serum phosphate level decreased from 7.9 mg/dl to 5.9 mg/dl, and serum total calcium level decreased from 11.0 mg/dl to ionized calcium 0.88 mmol/L (reference range 1.1–1.4). We continued by recording ionized
Fig. 1 a Parathyroid scan with Tc-99 m MIBI, (b) Post contrast chest and mediastinal CT scan. The arrow indicates the location of the ectopic parathyroid
Tai et al. BMC Endocrine Disorders (2019) 19:16 Page 2 of 4
calcium values as 0.81 mmol/L, 0.76 mmol/L, 0.73 mmol/L, 0.95 mmol/L, and 0.85 mmol/L for the past 5 post-operative days, respectively. We immediately ad- ministered intravenous calcium chloride 20 ml every 12 h, along with calcium acetate 667 mg four tablets three times a day and vitamin D 0.25 mcg daily from the second post-operative day.
According to the clinical history, the patient was diagnosed to have recurrent tertiary hyperparathyroid- ism before total parathyroidectomy and ectopic parathy- roidectomy. In addition, hungry bone syndrome was present after ectopic parathyroidectomy.
Discussion and conclusions
Supernumerary (more than four) parathyroid glands may be result from the separation of parathyroid anlage when the glands pull away from the pouch structures during the embryologic branchial complex phase [6].
These additional parathyroid glands are a common cause of recurrent or persistent hyperparathyroidism after parathyroidectomy. Residual small supernumerary glands with diffuse hyperplasia have the potential to be transformed to nodular hyperplasia during long-term hemodialysis [3]. In a retrospective study of 290 patients with renal hyperparathyroidism underwent reoperative parathyroidectomy, supernumerary parathyroid glands were identified in 87 patients (30%), corresponding to intrathymic in 70 cases and to extrathymic in 17 cases [7]. Supernumerary parathyroid glands are thus present in 30% of patients with renal hyperparathyroidism and are also responsible for 32% of persistent or recurrent hyperparathyroidism [7]. Thus, resecting the thymic tongue during the initial operation may reduce the need for reoperative parathyroidectomy to prevent recur- rences arising from anterior mediastinal glands [7, 8].
Beside, routine bilateral cervical thymectomy during the initial parathyroidectomy for renal hyperparathyroidism seems to be acceptable and can be recommended in patients on permanent hemodialysis not awaiting kidney transplantation [9,10].
Tertiary hyperparathyroidism represents an autonomous and advanced form of secondary hyperparathyroidism,
which is seen in ESRD patients receiving long-term dialysis and/or kidney transplant. Loss of response to serum calcium concentration leads to parathyroid glands with hyperplasia and autonomous activity, which then leads to elevated serum calcium, phosphate, and PTH levels. When PTH concentration rises, it causes certain complications in bone, vessels or tissues such as osteomalacia, osteoporosis, osteitis fibrosa cystica, vascular calcification, and soft tissue calcification. Operative correction of tertiary hyperparathyr- oidism is indicated if hypersecretion of PTH and severe or symptomatic hypercalcemia. Parathyroidectomy is consid- ered to be the only curative treatment for patients with tertiary hyperparathyroidism and all parathyroid glands should be examined [11]. In addition, medical treatment of tertiary hyperparathyroidism with Cinacalcet has been re- ported to be efficacious. A systemic review comparing the outcomes of surgical and medical treatment of tertiary hyperparathyroidism concluded that surgical treatment has higher cure rates than medical therapy [12]. One study reported that the diameter of the parathyroid gland is a main factor involved in resistance to Cinacalcet [13].
Parathyroidectomy for tertiary hyperparathyroidism is associated with lesser rates of renal allograft failure in cinacalcet management [14].
Patients with primary hyperparathyroidism who undergo parathyroidectomy demonstrate a rapid de- crease in serum calcium levels after successful removal of one or more hyperactive parathyroid gland(s). Hungry bone syndrome, been coined to the profound (serum calcium < 2.1 mmol/l) and prolonged (longer than 4th day post-operatively) hypocalcaemia, is a condition of hyperdynamic calcium reabsorption into bones following parathyroidectomy [15]. This syndrome manifests as prolonged and symptomatic hypocalcemia. Thus, high doses of calcium, high doses of active metabolites of vitamin D, and adequate correction of magnesium defi- ciency immediately after surgery helps to treat hypocal- cemia. Preoperative treatment with bisphosphonates has been suggested to reduce post-operative hypocalcemia [15]. Preoperative calcitriol therapy can reduce the use of postoperative administration of intravenous calcium by 56% and length of stay by 50% in parathyroidectomy
Fig. 2 a The histopathological examination showed lobules of hyperplastic parathyroid tissues composed primarily of chief cells with thin delicate vascularity, nuclear monomorphism, central round nuclei and granular cytoplasm (200X, H &E stain), (b) 400X, H &E stain. c Immunohistochemically, the parathyroid tissues are positive for GATA-3, while negative for TTF-1, CD5 and thyroglobulin
Tai et al. BMC Endocrine Disorders (2019) 19:16 Page 3 of 4
for renal-origin hyperparathyroidism patients [16]. In one study, severe postoperative hypocalcemia requiring intravenous calcium repletion occurred in 97% of ESRD patients with hyperparathyroidism but only 2% of those with primary hyperparathyroidism [17].
In conclusion, ectopic supernumerary parathyroid hyperplasia is an uncommon cause of recurrent tertiary hyperparathyroidism, we should prompt a search for the ectopic parathyroid glands in ESRD patients, who have recurrent or persistent hyperparathyroidism after total parathyroidectomy. ESRD patients are more likely to de- velop hungry bone syndrome after parathyroidectomy.
Prevention and treatment of hungry bone syndrome may be required after ectopic parathyroidectomy in clin- ical practice.
Abbreviations
CKD:chronic kidney disease; CT: computed tomography; ESRD: end-stage renal disease; i-PTH: intact parathyroid hormone
Acknowledgements Not applicable.
Funding None.
Availability of data and materials
The datasets analyzed during the current study are available from the corresponding author on reasonable request.
Authors’ contributions
TST, JMC and CCC diagnosed the patient, provided follow-up, and acquired clinical data. TST and YHH conducted investigations, reviewed literature, drafted the manuscript, and reviewed the manuscript for final publication. All of the authors read and approved the final manuscript.
Ethics approval and consent to participate
Informed consent was obtained from this patient for publication of this case history and associated images were provided.
Consent for publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Competing interests
The authors declare that they have no relevant financial interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Author details
1Department of Internal Medicine, Ditmanson Medical Foundation Chia-Yi Christian Hospital, 539 Chung Hsiao Rd, Chiayi City 600, Taiwan.2Department of Medical Research, Ditmanson Medical Foundation Chia-Yi Christian Hospital, 539 Chung Hsiao Rd, Chiayi 600, Taiwan.3Department of Nursing, Min-Hwei Junior College of Health Care Management, 1116, Sec. 2, Zhongshan E. Rd, Liuying Dist, Tainan City 736, Taiwan.4Division of Thoracic Surgery, Department of Surgery, Ditmanson Medical Foundation Chia-Yi Christian Hospital, 539 Chung Hsiao Rd, Chiayi 600, Taiwan.5Department of Pathology, Ditmanson Medical Foundation Chia-Yi Christian Hospital, 539 Chung Hsiao Rd, Chiayi 600, Taiwan.6Department of Cosmetic Science, Chia Nan University of Pharmacy and Science, 60, Sec. 1, Erren Rd, Rende Dist, Tainan 717, Taiwan.
Received: 29 October 2018 Accepted: 17 January 2019
References
1. Memmos DE, Williams GB, Eastwood JB, Gordon EM, Cochrane CL, Gower PE, et al. The role of parathyroidectomy in the management of hyperparathyroidism in patients on maintenance haemodialysis and after renal transplantation. Nephron. 1982;30(2):143–8.
2. Shindo M, Lee JA, Lubitz CC, McCoy KL, Orloff LA, Tufano RP, et al.
The changing landscape of primary, secondary, and tertiary
hyperparathyroidism: highlights from the American College of Surgeons panel,“what’s new for the surgeon caring for patients with
hyperparathyroidism”. J Am Coll Surg. 2016;222(6):1240–50.
3. Numano M, Tominaga Y, Uchida K, Orihara A, Tanaka Y, Takagi H.
Surgical significance of supernumerary parathyroid glands in renal hyperparathyroidism. World J Surg. 1998;22(10):1098–102.
4. Carter WB, Carter DL, Cohn HE. Cause and current management of reoperative hyperparathyroidism. Am Surg. 1993;59(2):120–4.
5. Edis AJ, Levitt MD. Supernumerary parathyroid glands: implications for the surgical treatment of secondary hyperparathyroidism. World J Surg.
1987;11:398.
6. Norris EH. The parathyroid glands and the lateral thyroid in man: their morphogenesis, histogenesis, topographic anatomy and prenatal growth.
Carnegie Instn Wash Publ Contrib Embryol. 1937;26:247–94.
7. Pattou FN, Pellissier LC, Noël C, Wambergue F, Huglo DG, Proye CA.
Supernumerary parathyroid glands: frequency and surgical significance in treatment or renal hyperparathyroidism. World J Surg. 2000;24(11):1330–4.
8. Okada M, Tominaga Y, Yamamoto T, Hiramitsu T, Narumi S, Watarai Y.
Location frequency of missed parathyroid glands after parathyroidectomy in patients with persistent or recurrent secondary hyperparathyroidism.
World J Surg. 2016;40(3):595–9.
9. Schneider R, Waldmann J, Ramaswamy A, Fernández ED, Bartsch DK, Schlosser K. Frequency of ectopic and supernumerary intrathymic parathyroid glands in patients with renal hyperparathyroidism: analysis of 461 patients undergoing initial parathyroidectomy with bilateral cervical thymectomy. World J Surg. 2011;35(6):1260–5.
10. Schneider R, Bartsch DK, Schlosser K. Relevance of bilateral cervical thymectomy in patients with renal hyperparathyroidism: analysis of 161 patients undergoing reoperative parathyroidectomy. World J Surg. 2013;
37(9):2155–61.
11. Nichol PF, Starling JR, Mack E, Klovning JJ, Becker BN, Chen H. Long-term follow-up of patients with tertiary hyperparathyroidism treated by resection of a single or double adenoma. Ann Surg. 2002;235(5):673–8.
12. Dulfer RR, Franssen GJH, Hesselink DA, Hoorn EJ, van Eijck CHJ, van Ginhoven TM. Systematic review of surgical and medical treatment for tertiary hyperparathyroidism. Br J Surg. 2017;104(7):804–13.
13. Okada M, Tominaga Y, Izumi K, Nobata H, Yamamoto T, Hiramitsu T, et al.
Tertiary hyperparathyroidism resistant to cinacalcet treatment. Ther Apher Dial.
2011;15(Suppl 1):33–7.
14. Finnerty BM, Chan TW, Jones G, Khader T, Moore M, Gray KD, et al.
Parathyroidectomy versus Cinacalcet in the Management of Tertiary Hyperparathyroidism: surgery improves renal transplant allograft survival.
Surgery. 2019;165(1):129–34.
15. Witteveen JE, van Thiel S, Romijn JA, Hamdy NA. Hungry bone syndrome:
still a challenge in the post-operative management of primary
hyperparathyroidism: a systematic review of the literature. Eur J Endocrinol.
2013;168(3):R45–53.
16. Alsafran S, Sherman SK, Dahdaleh FS, Ruhle B, Mercier F, Kaplan EL, et al.
Preoperative calcitriol reduces postoperative intravenous calcium requirements and length of stay in parathyroidectomy for renal-origin hyperparathyroidism. Surgery. 2019;165:151–7.
17. Mittendorf EA, Merlino JI, McHenry CR. Post-parathyroidectomy hypocalcemia: incidence, risk factors, and management. Am Surg. 2004;
70(2):114–9.
Tai et al. BMC Endocrine Disorders (2019) 19:16 Page 4 of 4