Title: Reduction of surgery rate in endometriosis patients who take Chinese medicine: a population-based retrospective cohort study
Shan-Yu Su1,2, Chih-Hsin Muo3,4, Fung-Chang Sung3, and Donald E. Morisky5
1Department of Chinese Medicine, China Medical University Hospital, Taichung 40447, Taiwan
2School of Post-baccalaureate Chinese Medicine, College of Chinese Medicine, China Medical University, Taichung 40402, Taiwan
3Department of Public Health, China Medical University, Taichung, 40402, Taiwan
4Management Office for Health Data, China Medical University Hospital, Taichung 40402, Taiwan
5Department of Community Health Sciences, UCLA Fielding School of Public Health, Los Angeles, California 90095-1772, U.S.A.
Correspondence to: Shan-Yu Su. Department of Chinese Medicine, China Medical University Hospital. No. 2 Yuh-Der Road, Taichung, Taiwan 40447.
Tel: 886-4-22052121ext.1675; Fax: 886-4-22365141; E-mail address:
Abstract
Objectives: Female patients have frequently utilized Chinese medicine (CM) to treat symptoms that could possibly be related to endometriosis. The objective of this population-based retrospective cohort study was to evaluate the relationship between CM use and subsequent surgery among patients with endometriosis.
Design: A total of 8,283 CM users were identified among the 22,488 endometriosis patients found in the National Health Insurance reimbursement database between 2000 and 2010. A control group was identified and consisted of 8,283 matched nonusers with the same disease. A Cox proportional regression analysis was performed in order to assess risk factors for surgery for the CM users and nonusers.
Results: When compared to nonusers, CM users were significantly less likely to undergo surgery, with a hazard ratio of 0.47 (95% CI = 0.421, 0.534) after adjusting for age, occupation, childbirth status, hypermenorrhea, iron-deficient anemia, dysmenorrhea, and amount of conventional medications. Among patients who had undergone surgery, the follow-up time was longer for CM users than for CM nonusers (p < 0.001). Moreover, the most frequently used CM single and formula were Cyperus rotundus and Gui-zhi-fu-ling-wan, respectively.
Conclusions: These results suggest that whatever the underlying reason, CM provides an alternative option that reduces the incidence rate of surgery in endometriosis patients.
Keywords: endometriosis, Chinese medicine, surgery.
List of abbreviations used
CI, confidence interval; CM, Chinese medicine; ICD-9-CM, International Classification of Diseases, 9th Revision, Clinical Modification; HR, hazard ratio;
IR, incidence rate; IRR, incidence rate ratio; LHID, Longitudinal Health Insurance Database; NHI, National Health Insurance.
Background
Endometriosis is an estrogen-dependent inflammatory disorder defined by the presence of active endometrial tissue outside the uterine cavity. Asian women are reported to have a higher risk of endometriosis than other races,1 and the prevalence of endometriosis is estimated to be 2.7% in Taiwanese women.2 The most common sites for endometriosis to occur are the ovaries, cul-de-sac, posterior broad ligaments, uterosacral ligaments, the uterus, fallopian tubes, the sigmoid colon and the appendix.3 The implantation of endometrioid mucosa is associated with the main chronic features of the disease, including pelvic pain, severe dysmenorrhea, hypermenorrhea, dyspareunia and infertility, although it may also be asymptomatic.4
The management of endometriosis varies according to the individual, with a multidisciplinary approach, and with goals of pain relief and/or a successful pregnancy for infertile patients.5 For patients with a mild form of the disease, pharmacological therapies are advisable for controlling symptoms so as to avoid side effects and the costs of surgery until menopause,6 when endometriotic implant growth is suppressed as a result of reduced ovarian estrogen production.7 For patients whose symptoms have failed to resolve or have worsened under medical treatment, surgical management is advisable. Conservative surgery, including fulguration, excision, cauterization, and ablation, is recommended for women who have not completed childbearing, since it preserves the uterus and as much ovarian tissue as possible.6 On the other hand, definitive surgery, including hysterectomy, with or without the removal of fallopian tubes and
ovaries, is indicated when incapacitating symptoms persist even after conservative therapy, and when pregnancy is not desired.8 However, surgery is always associated with long lasting complications, including fistula formation, adhesion, and sexual dysfunctions, which can last well beyond menopause, sometimes resulting in a negative quality of life outcome.
Chinese medicine (CM) is the most popular complementary alternative medicine in Asian countries and the Taiwanese Government’s National Health Insurance (NHI) covers it. Based on the NHI database, CM is commonly used by females to treat reproductive system diseases, including menstruation disorders, abnormal bleeding, as well as non-infectious disorders of female genital organs,13-16 which can potentially be caused by endometriosis. However, no population-based evidence has been reported about the benefit of CM in women with endometriosis. Research regarding the effects of CM on subsequent endometriosis-related conventional treatment is also very limited.
This population-based retrospective cohort study followed patients diagnosed with endometriosis from 1996 to 2010, using a national insurance reimbursement database. The association between CM use and the incidence of surgery in women with endometriosis was then evaluated. The results imply the benefits of CM for endometriosis patients from a public health perspective.
Methods Subjects
Endometriosis patients were identified according to the International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM) code 617 from 2000 to 2010 in the Longitudinal Health Insurance Database 2000 (LHID2000). The LHID2000 was set up by Taiwan’s National Health Research Institute and it contains chronological information about one million randomly selected individuals who were beneficiaries from 1996 to 2000.
Study designs
The date of the first diagnosis was used as the entry date, and the date of surgery was used as the outcome date. The types of endometriosis-related surgery include hysterectomy, oophorectomy, fulguration, excision, and the electric cauterization of endometriosis. Subjects who had undergone surgery before the entry date were excluded. CM users were defined as subjects who had received an orally administered CM treatment for more than two consecutive weeks. The CM nonuser group consisted of randomly selected patients who had not used CM, and this was matched with the CM user group according to age and to the duration between diagnosis and CM usage at a 1:1 ratio. The endpoint date was defined as the date of surgery, death, withdrawal from the insurance program, or December 31, 2010. The follow-up time was defined as the period from CM usage to the endpoint date.
Examined variables included socio-demographic factors (age, income level,
and occupation status), childbirth status, and endometriosis-related co- morbidities, including hypermenorrhea (ICD-9-CM 626.2), iron-deficiency anemia (ICD-9-CM 280), and dysmenorrhea (ICD-9-CM 625.3).
Statistical analysis
In terms of categorical and continuous variables, CM users and CM nonusers were compared using chi-square tests and t-tests, respectively, so as to assess any differences. A Cox proportional regression analysis was used to estimate the hazard ratio (HR) and its 95% confidence intervals (CIs) for undergoing surgery. The Kaplan-Meier method was used to plot the cumulative incidence, while the log-rank test was used to test the difference in cumulative rates between CM users and nonusers. The adjusted models were controlled for age, occupation, childbirth status, co-morbidities (hypermenorrhea, iron- deficiency anemia, and dysmenorrhea), and amount of conventional medications.
The incidence rate (IR) for surgery (per 1,000 person-years) was also calculated.
The relationship between the use of CM and uterine surgery was estimated by using the incidence rate ratio (IRR) and the corresponding 95% CI in a Poisson distribution model. All statistical analyses were performed using SAS software, version 9.1 (SAS Institute Inc., Carey, NC), and the significance level was set at a two-tailed p value of less than 0.05.
Results Study subjects
A total of 22,488 women diagnosed with endometriosis from 2000 to 2010 were extracted from the LHID2000 database. Among them, 8,283 patients were identified as CM users, and another 8,283 matched patients were identified as CM nonusers. The mean age of CM users and nonusers was 36.3 years. There was no difference in occupation status, co-morbidity of hypermenorrhea, or co- morbidity of iron-deficient anemia between CM users and nonusers (Table 1).
However, the income level of CM users was higher than that of CM nonusers. In addition, the proportion of patients who had not experienced childbirth, or who were co-morbid with dysmenorrhea was higher among CM users than it was among CM nonusers.
Risk factors for surgery among patients with endometriosis
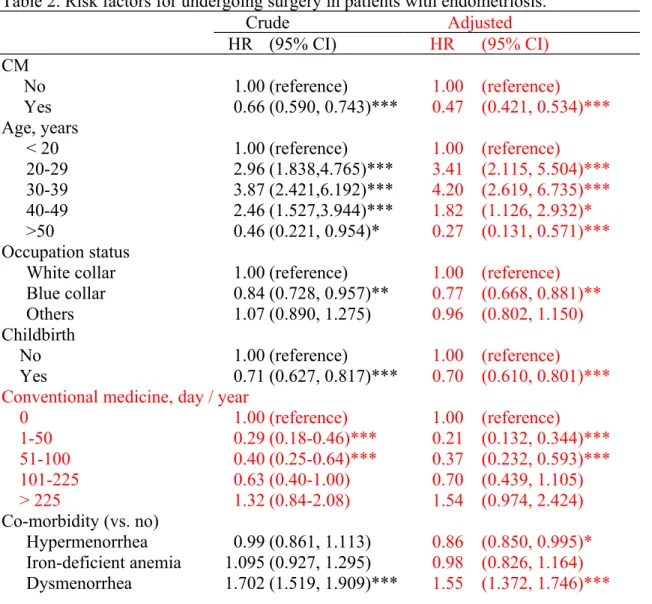
After a mean follow-up time of 3.5 years, 1,185 of our subjects had undergone surgery. CM users were significantly less likely to have undergone surgery than CM nonusers, after adjusting for socio-demographic factors (age and occupation), childbirth status, co-morbid covariates (hypermenorrhea, iron- deficiency anemia, and dysmenorrhea), and amount of conventional western medications with an adjusted HR of 0.47 (Table 2). The adjusted HR for surgery was higher among patients who were between 30 and 39 years of age, who were white-collar workers, who had no childbirth experience, who did not take conventional pharmaceutical treatment, and whose diseases were co-morbid with
dysmenorrhea.
Difference in the incidence of surgery between CM users and CM nonusers
Kaplan-Meier analysis revealed a significantly higher cumulative incidence of surgery for CM nonusers than for CM users (p < 0.0001, Figure 1). The overall IR for surgery among CM users was 16.3 per 1,000 patients, which is significantly lower than that among CM nonusers (26.1 per 1,000 patients).
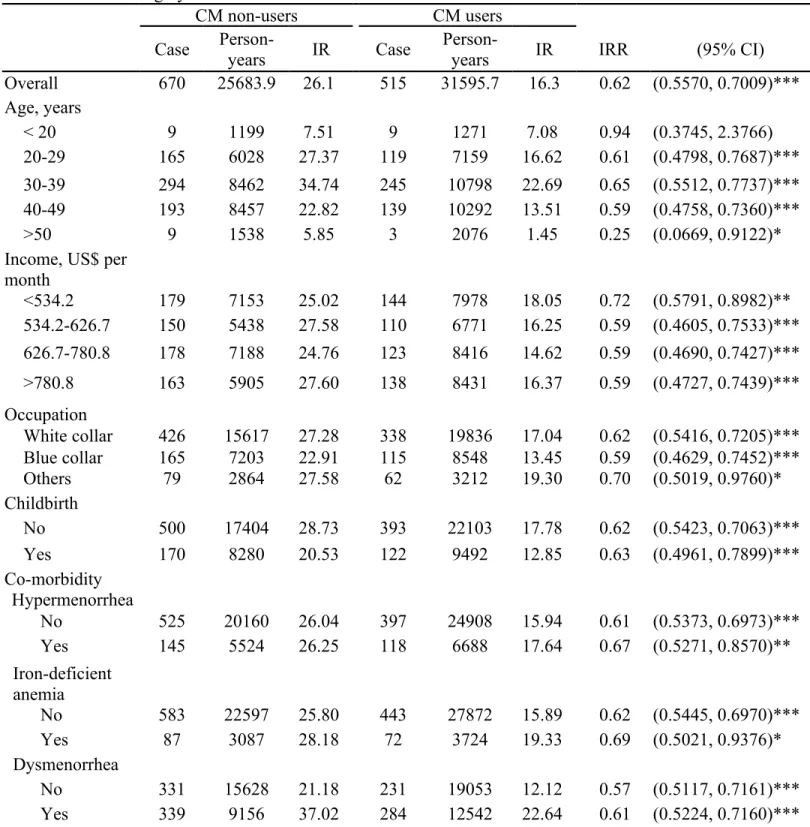
Poisson regression analysis revealed that the IRs for surgery were lower among CM users in all the demographic subgroups except for the subgroup under 20 years of age, in which only nine patients underwent surgery in each group. The IR was also lower for CM users than for CM nonusers, irrespective of the co- morbidities with hypermenorrhea, anemia, or dysmenorrhea, if any (Table 3).
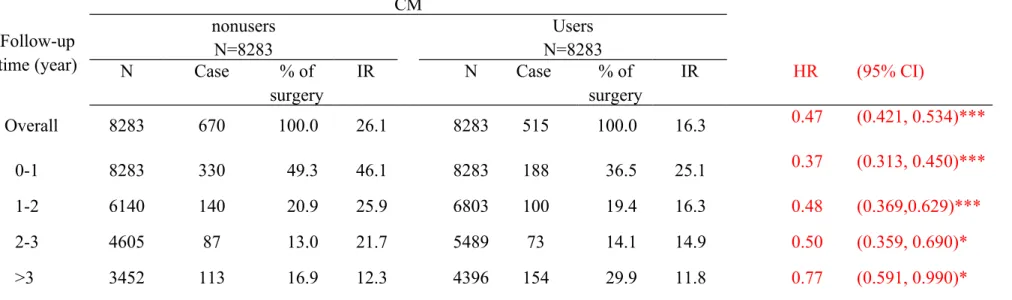
In order to compare the period of time before surgery between CM users and nonusers, the number of surgical procedures was calculated annually (Table 4). Most surgeries occurred during the first two years for both CM users and nonusers. Nevertheless, among patients who underwent surgery, the period between the index date and the date of surgery for CM users was longer (2.2 years) than that for CM nonusers (1.6 years) (p < 0.001). A significantly smaller proportion of surgeries occurred during the first year among CM users than occurred among CM nonusers (36.5% vs. 49.3%), but a larger proportion of surgeries occurred after the third year among CM users than among CM nonusers (29.9% vs. 16.9%). A comparison of the IRs between the two the groups shows that the IRs were smaller for CM users than for CM nonusers in
all the follow-up years, adjusted IR for surgery in CM users increased from 0.37 in the first year to 0.77 after the third year compared to nonusers.
Details of the prescribed CM
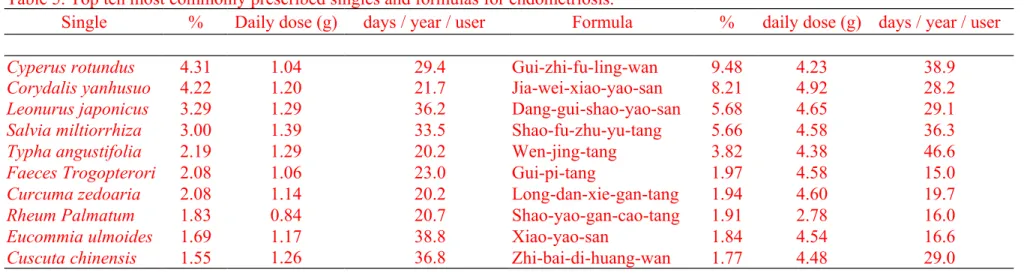
The top ten most frequently prescribed CM singles and formulas are listed in Table 5. The most frequently prescribed single was Cyperus rotundus, followed by Corydalis yanhusuo, Leonurus japonicas, Salvia miltiorrhiza, Typha angustifolia, Faeces Trogopterori, Curcuma zedoaria, Rheum Palmatum, Eucommia ulmoides, and Cuscuta chinensis. Cyperus rotundus dominated 4.22% of the total prescriptions, with a mean dose of 1.04 g per day and 29.4 days per year. The most frequently prescribed formula was Gui-zhi-fu-ling-wan, which dominated 9.48% of the total prescriptions, with a mean dose of 4.23 g per day and 38.9 days per year. The second to tenth frequently used CM formulas were Jia-wei-xiao-yao-san, Dang-gui-shao-yao-san, Shao-fu-zhu-yu- tang, Wen-jing-tang, Gui-pi-tang, Long-dan-xie-gan-tang, Shao-yao-gan-cao- tang, Xiao-yao-san, and Zhi-bai-di-huang-wan, in this order.
Discussion
Based on previous studies, which identified a high utilization of CM among women for treating symptoms related to endometriosis, the present study investigated the association between CM use and the subsequent surgery for patients with endometriosis. The data indicated that CM users were less likely to undergo surgery than CM nonusers. The incidence rate of surgery was much lower among CM users than CM nonusers, and the difference in the incidence rate between CM users and nonusers was seen in almost all socio-demographic subgroups. Moreover, a longer time period elapsed before surgery for CM users than for nonusers.
A comparison of socio-demographic factors between CM users and nonusers in the present study shows that CM users had higher income levels than CM nonusers among endometriosis patients. This coincides with another study that extracted subjects of the same disease from 1998 to 2008,2 and of two other female-specific diseases: uterine fibroid and breast cancer; this phenomenon, however, does not exist among males. This study also observed that subjects without childbirth experience were likely to use CM, in agreement with a previous report that found infertility to be a factor that drives patients to use CM.17 As for co-morbidities, endometriosis patients who were co-morbid with dysmenorrhea tended to use CM more often than patients co-morbid with hypermenorrhea or iron-deficient anemia. This implies that CM might have uneven effectiveness of CM on these three co-morbidities in endometriosis.
Analysis of the risk factors for surgery showed that CM use might be a
protective factor for surgery in endometriosis patients, with an HR of 0.47.
Socio-demographic risk factors for surgery included being between 20 and 49 years of age, being blue-collar, and having no childbirth experience. Fibroid patients also reported a correlation between CM usage and surgery, with an HR of 0.18,17 which was much lower than that found among endometriosis patients for this study. We propose that, although uterine fibroid and endometriosis have similar symptoms, co-morbidities and management, the efficacy of CM is greater in the treatment of fibroid than that of endometriosis. The socio- demographic trends for undergoing surgery among endometriosis patients were similar to that among fibroid patients, excepting for that fibroid patients with infertility had a lower surgery rate than those without infertility.17 This difference might be due to that the symptoms of endometriosis often disappearing or improving during pregnancy, sometimes even leading to a complete resolution of a mild form of the disease,20 but fibroid symptoms are aggravated after pregnancy since fibroids increase in size throughout gestation. 21 Poisson model indicates a significant decrease in the IR of surgery for CM users; moreover, Kaplan-Meier analysis also shows that the cumulative incidence of surgery in CM users was lower than in CM nonusers, suggesting the idea that CM use reduced the possibility of surgery for endometriosis patients.
The decrease in the incidence of surgery for CM users was not changed by socio-demographic factors, except for the subgroup of patients who were less than 20 years old, in which only 18 subjects underwent surgery. Similarly, the decrease in the incidence of surgery did not depend on childbirth experience, or
on co-morbidities with hypermenorrhea, iron-deficient anemia, or dysmenorrhea.
These results imply that the reduction of surgery rate by CM was strong and could be applied to all socio-demographic subgroups.
When comparing yearly IRs, the surgery IRs for CM users were lower than those for CM nonusers, but the adjusted IR for surgery increased from 0.37 in the first year to 0.77 after third year, implying that the protection provided by CM was weakened in patients who had a long diagnosis-to-surgery duration. The decrease in apparent protection from surgery of CM was speculated to be due to that there were more asymptomatic and mildly symptomatic patients in subgroups with long follow-up time. These patients would not have reached the stage of surgery irrespective of whether they used CM or not. Moreover, there was a longer follow-up time for CM users who underwent surgery compared to CM nonusers. Almost half of the surgeries for CM nonusers happened within the first year, but only 36% of surgeries for CM users happened within the first year.
This result suggests that CM use delays surgery among endometriosis patients.
As endometriosis is suppressed as a result of reduced estrogen production, the delay of surgery by CM might help perimenopausal patients to avoid surgery.
By analyzing the breakdown of CM, this study found that the most frequently used CM formula was Gui-zhi-fu-ling-wan, followed by Jia-wei-xiao- yao-san, and Dang-gui-shao-yao-san. Gui-Zhi-Fu-Ling-Wan was also demonstrated in a previous to be the most common prescribed formula among endometriosis patients between 1998 to 2008.2 All of the above formulas are administered commonly in the treatment of dysmenorrhea and
hypermenorrhea.22 Jia-wei-xiao-yao-san and Dang-gui-shao-yao-san are the top two formulas to treat primary dysmenorrhea23. In regards to CM singles, the most frequently used two CM singles were Cyperus rotundus and Corydalis yanhusuo, those are the top two most frequently used singles to treat dysmenorrhea in Taiwan.23 Nevertheless, only a limited number of rigorous clinical trials regarding to the efficacy of CM on endometriosis have been performed.24 One of these trials reported a reduction in the dysmenorrhea pain score when using a CM formulation called Nei-Yi-Wan,25 and another trial reported Nei-Yi-Wan users as having a similar symptomatic relief rate as gestrinone users.26 The pain relief by CM is also accompanied by an increase in patients’ quality of life.27 In addition, the CM formulation granules called Quyu Jiedu, reduce levels of tumor necrosis factor-α and interleukin-6,28 both of which have been shown to be up-regulated during the menstrual phase in endometriosis patients.29 Therefore, the delayed surgery and low incidence of surgery among CM users implies that CM might be effective for the treatment of endometriosis or its co-morbidities, rendering that the disease failed to meet the criteria needed for surgery. However, more rigorous clinical trials are still needed to clarify the mechanism.
As with any other retrospective study, the main limitation of this study was that the methodology could only find a correlative relationship between CM usage and surgery, but not a causal relationship between the two variables. The difference between CM users and nonusers could reflect patients’ preference to delay surgery and use CM as an alternative. Therefore, more randomized
controlled trials are needed in the future in order to examine the effectiveness of CM on endometriosis. Secondly, since the NHI database was originally created for the purpose of administrative and insurance claims, and not for rigorous academic research, there may be a bias in register information,
Conclusions
In summary, using a population-based database, this study found that, in patients with endometriosis, the incidence rate and risk of surgery were both lower among CM users than among CM nonusers. Moreover, surgery occurred earlier for CM nonusers than for CM users. Whatever the underlying reason, CM appears to provide an alternative treatment option that does reduce the incidence of surgery and that could have important health economic implications.
Acknowledgements
The authors thank the National Health Research Institute in Taiwan for providing the insurance claims data. This study was supported in part by grants from Taiwan Department of Health Clinical Trial and Research Center of Excellence (DOH102-TD-B-111-004) and the Cancer Research Center of Excellence (DOH 102-TD-C-111-005), the National Science Council (NSC 100- 2621-M-039-001) and China Medical University Hospital (grant number 1MS1).
References
1. Sangi-Haghpeykar H, Poindexter AN, 3rd. Epidemiology of endometriosis among parous women. Obstet Gynecol. 1995;85:983-92.
2. Fang RC, Tsai YT, Lai JN, Yeh CH, Wu CT. The traditional chinese medicine prescription pattern of endometriosis patients in taiwan: a population-based study. Evid Based Complement Alternat Med. 2012;2012:Article ID:591391, 9 pages.
3. Gustofson RL, Kim N, Liu S, Stratton P. Endometriosis and the appendix: a case series and comprehensive review of the literature. Fertil Steril.
2006;86:298-303.
4. Sinaii N, Plumb K, Cotton L, Lambert A, Kennedy S, Zondervan K, et al.
Differences in characteristics among 1,000 women with endometriosis based on extent of disease. Fertil Steril. 2008;89:538-45.
5. Rocha AL, Reis FM, Petraglia F. New trends for the medical treatment of endometriosis. Expert Opin Investig Drugs. 2012;21:905-19.
6. Gelbaya TA, Nardo LG. Evidence-based management of endometrioma.
Reprod Biomed Online. 2011;23:15-24.
7. Fagervold B, Jenssen M, Hummelshoj L, Moen MH. Life after a diagnosis with endometriosis - a 15 years follow-up study. Acta Obstet Gynecol Scand.
2009;88:914-9.
8. Brown J, Farquhar C. Endometriosis: an overview of Cochrane Reviews.
Cochrane Database Syst Rev. 2014;3:Article ID:CD009590, 44 pages.
9. Clayton RD. Hysterectomy. Best Practice & Research Clinical Obstetrics &
Gynaecology. 2006;20:73-87.
10. Chalermchockchareonkit A, Tekasakul P, Chaisilwattana P, Sirimai K, Wahab N. Laparoscopic hysterectomy versus abdominal hysterectomy for severe pelvic endometriosis. Int J Gynaecol Obstet. 2012;116:109-11.
11. Hsieh SC, Lai JN, Lee CF, Hu FC, Tseng WL, Wang JD. The prescribing of Chinese herbal products in Taiwan: a cross-sectional analysis of the national health insurance reimbursement database. Pharmacoepidemiol Drug Saf.
2008;17:609-19.
12. Chen FP, Kung YY, Chen TJ, Hwang SJ. Demographics and patterns of acupuncture use in the Chinese population: the Taiwan experience. J Altern Complement Med. 2006;12:379-87.
13. Chang LC, Huang N, Chou YJ, Lee CH, Kao FY, Huang YT. Utilization patterns of Chinese medicine and Western medicine under the National Health Insurance Program in Taiwan, a population-based study from 1997 to 2003.
BMC Health Serv Res. 2008;8:170.
14. Tu CC, Li CS, Liu CM, Liu CC. Comparative use of biomedicine and Chinese medicine in Taiwan: using the NHI Research Database. J Altern Complement Med. 2011;17:339-46.
15. Shih CC, Liao CC, Su YC, Tsai CC, Lin JG. Gender Differences in Traditional Chinese Medicine Use among Adults in Taiwan. PLoS One.
2012;7:e32540.
16. Wolsko PM, Eisenberg DM, Davis RB, Ettner SL, Phillips RS. Insurance coverage, medical conditions, and visits to alternative medicine providers:
results of a national survey. Arch Intern Med. 2002;162:281-7.
17. Su SY, Muo CH, Morisky DE. Use of chinese medicine and subsequent surgery in women with uterine fibroid: a retrospective cohort study. Evid Based Complement Alternat Med. 2012;2012:Article ID:617918, 9 pages.
18. Lin YH, Chiu JH. Use of Chinese medicine by women with breast cancer: a nationwide cross-sectional study in Taiwan. Complement Ther Med.
2011;19:137-43.
19. Kuan YC, Yen DJ, Yiu CH, Lin YY, Kwan SY, Chen C, et al. Treatment- seeking behavior of people with epilepsy in Taiwan: a preliminary study.
Epilepsy Behav. 2011;22:308-12.
20. Schenken RS, Williams RF, Hodgen GD. Effect of pregnancy on surgically induced endometriosis in cynomolgus monkeys. Am J Obstet Gynecol.
1987;157:1392-6.
21. Neiger R, Sonek JD, Croom CS, Ventolini G. Pregnancy-related changes in the size of uterine leiomyomas. J Reprod Med. 2006;51:671-4.
22. Maciocia C. Obstetrics and gynecology in Chinese medicine. second ed.
Edinburgh, UK: Churchill Livingstone; 2011.
23. Chen HY, Lin YH, Su IH, Chen YC, Yang SH, Chen JL. Investigation on Chinese herbal medicine for primary dysmenorrhea: implication from a nationwide prescription database in Taiwan. Complement Ther Med.
2014;22:116-25.
24. Flower A, Liu JP, Lewith G, Little P, Li Q. Chinese herbal medicine for endometriosis. Cochrane Database Syst Rev. 2012;5:Article ID:CD006568, 51 pages.
25. Wu SZ, Chen XL, Huang YC, Liu CD. Observation on effect of combined therapy of Neiyi pill and Neiyi enema on endometriosis. Chinese Journal of Integrated Traditional and Western Medicine. 2006;26:557-9.
26. Wu SZ, Chen XL, Chen WZ, Li SY. Clinical analysis of the treatment of endometriosis using Nei Yi pills and Nei Yi enema. Journal of Liaoning University of TCM. 2006;8:5-6.
27. Flower A, Lewith GT, Little P. A feasibility study exploring the role of Chinese herbal medicine in the treatment of endometriosis. J Altern Complement Med. 2011;17:691-9.
28. Lian F, Li XL, Sun ZG, Zhang JW, Liu YH, Ma FM. Effect of Quyu Jiedu granule on microenvironment of ova in patients with endometriosis. Chin J Integr Med. 2009;15:42-6.
29. Burney RO, Giudice LC. Pathogenesis and pathophysiology of endometriosis. Fertil Steril. 2012;98:511-9.
Figure legend
Figure 1. Kaplan-Meier analysis for cumulative incidence of surgery for endometriosis between CM users and CM nonusers.
Table 1. Socio-demographic factors and co-morbidities of Chinese medicine (CM) users and nonusers in patients with endometriosis.
CM nonusers
N=8283
users N=8283
Total N=16566
n % n % n % P-value
Age, years 0.6945
< 20 361 4.3 356 4.3 717 4.3
20-29 1929 23.3 1913 23.1 3842 23.2
30-39 2811 33.9 2843 34.3 5654 34.1
40-49 2685 32.4 2635 31.8 5320 32.1
>50 497 6.0 536 6.5 1033 6.2
Mean ± SD 36.3 ± 9.6 36.3 ± 9.6 36.3 ± 9.6 0.9578
Income, US$ per month < 0.0001
<534.2 2443 29.5 2249 27.2 4692 28.3
534.2-626.7 1799 21.7 1846 22.3 3645 22.0
626.7-780.8 2169 26.2 2082 25.1 3645 25.7
>780.8 1872 22.6 2106 25.4 3978 24.0
Mean ± SD 651 ± 438 681 ± 439 666 ± 438 < 0.0001
Occupation status 0.0960
White collar 5106 61.6 5228 63.1 10334 62.4
Blue collar 2230 26.9 2177 26.3 4407 26.6
Others 947 11.4 878 10.6 1825 11.0
Childbirth < 0.0001
No 5893 71.15 6225 75.15 12118 73.15
Yes 2390 28.85 2058 24.85 4448 26.85
Conventional medicine (days / year) < 0.0001
0 463 5.59 449 5.42 912 5.51
1-50 2921 35.27 1057 12.76 3978 24.01
51-100 1667 20.13 1967 23.75 3634 21.94
101-225 1477 17.83 2613 31.55 4090 24.69
> 225 1755 21.19 2197 26.52 3952 23.86
Mean ± SD 2.14 ± 1.26 2.61 ± 1.16 2.37 ± 1.23 < 0.0001 Co-morbidity
Hypermenorrhea 2014 24.3 2045 24.7 4059 24.5 0.5755
Iron-deficient anemia 1110 13.28 1110 13.4 2210 13.3 0.8193 Dysmenorrhea 3371 40.7 3700 44.7 7071 42.7 < 0.0001 Chi-square test and t-test.
Table 2. Risk factors for undergoing surgery in patients with endometriosis.
Crude Adjusted
HR (95% CI) HR (95% CI)
CM
No 1.00 (reference) 1.00 (reference)
Yes 0.66 (0.590, 0.743)*** 0.47 (0.421, 0.534)***
Age, years
< 20 1.00 (reference) 1.00 (reference)
20-29 2.96 (1.838,4.765)*** 3.41 (2.115, 5.504)***
30-39 3.87 (2.421,6.192)*** 4.20 (2.619, 6.735)***
40-49 2.46 (1.527,3.944)*** 1.82 (1.126, 2.932)*
>50 0.46 (0.221, 0.954)* 0.27 (0.131, 0.571)***
Occupation status
White collar 1.00 (reference) 1.00 (reference)
Blue collar 0.84 (0.728, 0.957)** 0.77 (0.668, 0.881)**
Others 1.07 (0.890, 1.275) 0.96 (0.802, 1.150)
Childbirth
No 1.00 (reference) 1.00 (reference)
Yes 0.71 (0.627, 0.817)*** 0.70 (0.610, 0.801)***
Conventional medicine, day / year
0 1.00 (reference) 1.00 (reference)
1-50 0.29 (0.18-0.46)*** 0.21 (0.132, 0.344)***
51-100 0.40 (0.25-0.64)*** 0.37 (0.232, 0.593)***
101-225 0.63 (0.40-1.00) 0.70 (0.439, 1.105)
> 225 1.32 (0.84-2.08) 1.54 (0.974, 2.424)
Co-morbidity (vs. no)
Hypermenorrhea 0.99 (0.861, 1.113) 0.86 (0.850, 0.995)*
Iron-deficient anemia 1.095 (0.927, 1.295) 0.98 (0.826, 1.164) Dysmenorrhea 1.702 (1.519, 1.909)*** 1.55 (1.372, 1.746)***
Cox proportional hazard model adjusted for age, occupation, childbirth status, hypermenorrhea, iron-deficient anemia, dysmenorrhea and western medicine.
* p < 0.05, ** p < 0.01, and *** p < 0.001.
Table 3. Relative surgery incidence for CM users and nonusers
CM non-users CM users
Case Person-
years IR Case Person-
years IR IRR (95% CI)
Overall 670 25683.9 26.1 515 31595.7 16.3 0.62 (0.5570, 0.7009)***
Age, years
< 20 9 1199 7.51 9 1271 7.08 0.94 (0.3745, 2.3766)
20-29 165 6028 27.37 119 7159 16.62 0.61 (0.4798, 0.7687)***
30-39 294 8462 34.74 245 10798 22.69 0.65 (0.5512, 0.7737)***
40-49 193 8457 22.82 139 10292 13.51 0.59 (0.4758, 0.7360)***
>50 9 1538 5.85 3 2076 1.45 0.25 (0.0669, 0.9122)*
Income, US$ per month
<534.2 179 7153 25.02 144 7978 18.05 0.72 (0.5791, 0.8982)**
534.2-626.7 150 5438 27.58 110 6771 16.25 0.59 (0.4605, 0.7533)***
626.7-780.8 178 7188 24.76 123 8416 14.62 0.59 (0.4690, 0.7427)***
>780.8 163 5905 27.60 138 8431 16.37 0.59 (0.4727, 0.7439)***
Occupation
White collar 426 15617 27.28 338 19836 17.04 0.62 (0.5416, 0.7205)***
Blue collar 165 7203 22.91 115 8548 13.45 0.59 (0.4629, 0.7452)***
Others 79 2864 27.58 62 3212 19.30 0.70 (0.5019, 0.9760)*
Childbirth
No 500 17404 28.73 393 22103 17.78 0.62 (0.5423, 0.7063)***
Yes 170 8280 20.53 122 9492 12.85 0.63 (0.4961, 0.7899)***
Co-morbidity Hypermenorrhea
No 525 20160 26.04 397 24908 15.94 0.61 (0.5373, 0.6973)***
Yes 145 5524 26.25 118 6688 17.64 0.67 (0.5271, 0.8570)**
Iron-deficient anemia
No 583 22597 25.80 443 27872 15.89 0.62 (0.5445, 0.6970)***
Yes 87 3087 28.18 72 3724 19.33 0.69 (0.5021, 0.9376)*
Dysmenorrhea
No 331 15628 21.18 231 19053 12.12 0.57 (0.5117, 0.7161)***
Yes 339 9156 37.02 284 12542 22.64 0.61 (0.5224, 0.7160)***
IRR, incidence rate ratio, compared to CM non-users in Poisson distribution mode.
*p < 0.05, ** p < 0.01, and *** p < 0.001.
Table 4. Yearly hazard ratio of surgery for CM users and nonusers CM
Follow-up time (year)
nonusers N=8283
Users N=8283
N Case % of
surgery
IR N Case % of
surgery
IR HR (95% CI)
Overall 8283 670 100.0 26.1 8283 515 100.0 16.3 0.47 (0.421, 0.534)***
0-1 8283 330 49.3 46.1 8283 188 36.5 25.1 0.37 (0.313, 0.450)***
1-2 6140 140 20.9 25.9 6803 100 19.4 16.3 0.48 (0.369,0.629)***
2-3 4605 87 13.0 21.7 5489 73 14.1 14.9 0.50 (0.359, 0.690)*
>3 3452 113 16.9 12.3 4396 154 29.9 11.8 0.77 (0.591, 0.990)*
Cox proportional hazard model adjusted for age, occupation, delivery, hypermenorrhea, iron-deficient anemia, dysmenorrhea and western medicine.
*p < 0.05 and ***p < 0.001.
Table 5. Top ten most commonly prescribed singles and formulas for endometriosis.
Single % Daily dose (g) days / year / user Formula % daily dose (g) days / year / user
Cyperus rotundus 4.31 1.04 29.4 Gui-zhi-fu-ling-wan 9.48 4.23 38.9
Corydalis yanhusuo 4.22 1.20 21.7 Jia-wei-xiao-yao-san 8.21 4.92 28.2
Leonurus japonicus 3.29 1.29 36.2 Dang-gui-shao-yao-san 5.68 4.65 29.1
Salvia miltiorrhiza 3.00 1.39 33.5 Shao-fu-zhu-yu-tang 5.66 4.58 36.3
Typha angustifolia 2.19 1.29 20.2 Wen-jing-tang 3.82 4.38 46.6
Faeces Trogopterori 2.08 1.06 23.0 Gui-pi-tang 1.97 4.58 15.0
Curcuma zedoaria 2.08 1.14 20.2 Long-dan-xie-gan-tang 1.94 4.60 19.7
Rheum Palmatum 1.83 0.84 20.7 Shao-yao-gan-cao-tang 1.91 2.78 16.0
Eucommia ulmoides 1.69 1.17 38.8 Xiao-yao-san 1.84 4.54 16.6
Cuscuta chinensis 1.55 1.26 36.8 Zhi-bai-di-huang-wan 1.77 4.48 29.0