Title: Statins use and female lung cancer risk in Taiwan Running head: statins and lung cancer
Shih-Wei Lai, MD 1,2; Kuan-Fu Liao, MD and MS 3,4,5; Cheng-Li Lin, MS 6,7; Fung- Chang Sung, PhD, MPH 6,7; Ya-Hsin Cheng, DVM, MS, PhD8
1School of Medicine, 3Graduate Institute of Integrated Medicine, and 6Department of Public Health, China Medical University, Taichung, Taiwan
2Department of Family Medicine, and 7Management Office for Health Data, China Medical University Hospital, Taichung, Taiwan
4Department of Internal Medicine, Taichung Tzu Chi General Hospital, Taichung, Taiwan
5Department of Health Care Administration, Central Taiwan University of Science and Technology, Taichung, Taiwan
8Department of Physiology, School of Medicine, China Medical University, Taichung, Taiwan
(The first two authors contributed equally to this study.)
Corresponding author:
Ya-Hsin Cheng, DVM, MS, PhD
Department of Physiology, School of Medicine, China Medical University, No. 91, Shueh-Shih Road, Taichung, 404, Taiwan
Phone: 886-4-2205-3366, ext.2183 Fax: 886-4-2205-3764
Word counts: 37 in the abstract, 415 in the text, 2 tables, and 5 references
1
Abstract
In this present study, we found that use of rosuvastatin with cumulative using duration > 12 months could correlate with 2.8-fold increased risk of lung cancer in women. We did not have specific comments on these results. Further prospective clinical studies of statins use are needed to elucidate this issue.
Key words: statins; lung cancer
Introduction
In order to clarify the association between statins use and female lung cancer risk, we extended the study period and collected more female lung cancer cases by analyzing the Taiwan National Health Insurance database from 2000 to 2010.
Methods
There were 1117 female subjects with newly diagnosed lung cancer (based on ICD-9 codes162.X and A-code A101), who were aged 20 years or older at the date of
diagnosing lung cancer (mean age 66.5 years and standard deviation 13.4 years). In addition, 4468 control subjects without lung cancer were matched with age and index date (mean age 65.9 years and standard deviation 13.6 years). The insurance program details can be found in previously published studies . Six commercially available statins in Taiwan were analyzed, including simvastatin, fluvastatin, lovastatin, atorvastatin, pravastatin and rosuvastatin.
Results
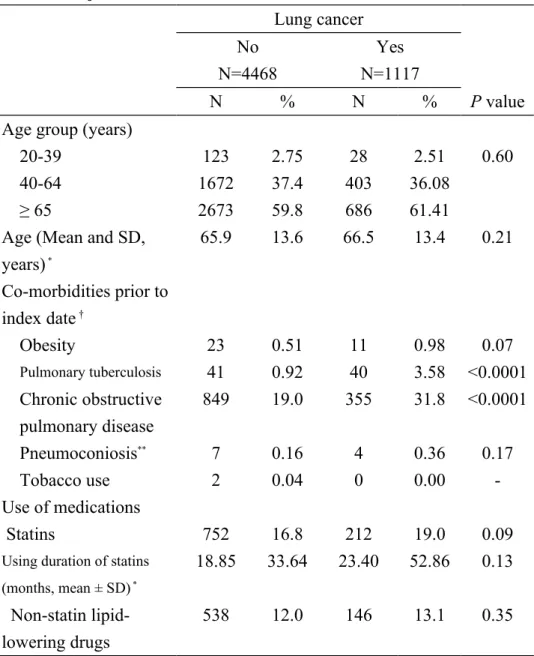
The lung cancer cases were more likely to have pulmonary tuberculosis (3.58% vs.
0.92%) and chronic obstructive pulmonary disease (31.8% vs. 19.0%)(P < 0.0001).
Moreover, there were 212 subjects with statins use among lung cancer cases (19.0%) and 752 subjects with statins use among control subjects (16.8%) (P = 0.09). There was no statistical difference in using duration of statins between lung cancer cases and control subjects (mean ± SD, months, 23.40 ± 52.86 vs.18.85 ± 33.64, P = 0.13) (Table 1).
After controlling for co-variables, multiple logistic regression analysis showed that no association was detected between statins use and lung cancer risk (odds ratio = 1.07, 95% CI = 0.90-1.27) (Table 2). In further analysis, only use of rosuvastatin with cumulative using duration > 12 months could correlate with increased risk of lung cancer (odds ratio = 2.79, 95% CI = 1.37-5.66), as compared with non-use of statins
3
(Table not shown).
Discussion
To date, controversy exists about the association between statins use and lung cancer risk. A case-control study by Khurana and colleagues in US showed that statins use fore more than 6 months could correlate with risk reduction of lung cancer
(odds ratio = 0.45, 95% CI = 0.42 to 0.48) , which was contrary to Cheng and colleagues’ findings in Taiwan (odds ratio = 0.82 , 95% CI = 0.58-1.15) . In this present study, we found that use of rosuvastatin with cumulative using duration > 12 months could correlate with 2.8-fold increased risk of lung cancer in women. We did not have specific comments on these results. In our view, because of inconclusive clinical data, further prospective clinical studies of statins use are needed to clearly elucidate this issue.
Funding: This study was supported in part by grants from Taiwan Department of Health Clinical Trial and Research Center of Excellence (DOH 101-TD-B-111-004), the Cancer Research Center of Excellence (DOH 101-TD-C-111-005), the National Science Council (NSC 100-2621-M-039-001), and China Medical University Hospital (1MS1). The funding agencies did not influence the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Conflict of Interest Statement: The authors disclose no conflicts of interest.
5
REFERENCES
1. Lai SW, Liao KF, Liao CC, Muo CH, Liu CS, Sung FC. Polypharmacy correlates with increased risk for hip fracture in the elderly: a population- based study. Medicine (Baltimore) 2010;89: 295-299.
2. Lai SW, Muo CH, Liao KF, Sung FC, Chen PC. Risk of acute pancreatitis in type 2 diabetes and risk reduction on anti-diabetic drugs: a population-based cohort study in taiwan. Am J Gastroenterol 2011;106: 1697-1704.
3. Lai SW, Lin CH, Liao KF, Su LT, Sung FC, Lin CC. Association between polypharmacy and dementia in older people: a population-based case-control study in Taiwan. Geriatr Gerontol Int 2012;12: 491-498.
4. Khurana V, Bejjanki HR, Caldito G, Owens MW. Statins reduce the risk of lung cancer in humans: a large case-control study of US veterans. Chest 2007;131: 1282-1288.
5. Cheng MH, Chiu HF, Ho SC, Yang CY. Statin use and the risk of female lung cancer: a population-based case-control study. Lung Cancer 2012;75: 275-279.
Table 1. Baseline characteristics between lung cancer cases and control subjects in women
Lung cancer No
N=4468
Yes N=1117
N % N % P value
Age group (years)
20-39 123 2.75 28 2.51 0.60
40-64 1672 37.4 403 36.08
≥ 65 2673 59.8 686 61.41
Age (Mean and SD, years) *
65.9 13.6 66.5 13.4 0.21
Co-morbidities prior to index date †
Obesity 23 0.51 11 0.98 0.07
Pulmonary tuberculosis 41 0.92 40 3.58 <0.0001
Chronic obstructive pulmonary disease
849 19.0 355 31.8 <0.0001
Pneumoconiosis** 7 0.16 4 0.36 0.17
Tobacco use 2 0.04 0 0.00 -
Use of medications
Statins 752 16.8 212 19.0 0.09
Using duration of statins (months, mean ± SD) *
18.85 33.64 23.40 52.86 0.13
Non-statin lipid- lowering drugs
538 12.0 146 13.1 0.35
Chi-square, ** Fisher’s exact test, and * t test comparing women with and without lung cancer
†The co-morbidities potentially associated with lung cancer were diagnosed as follows:
obesity (ICD-9 codes 278.00 and 278.01, and A-code A183), pulmonary tuberculosis (ICD-9 codes 010.X, 011.X, 012.X and 018.X), chronic obstructive pulmonary disease (ICD-9 codes 491.X, 492.X, 493.X and 496.X), pneumoconiosis (ICD-9 codes 500,502,503, 504 and 505), and tobacco use (ICD-9 codes 305.1).
7
Table 2. Odds ratios and 95% confidence intervals of lung cancer associated with statins use and covariates in women
Crude Adjusted †
Variable OR (95%CI) OR (95%CI)
Age (per one year) 1.00 (0.998, 1.01) - -
Co-morbidities prior to index date (yes vs. no)
Obesity 1.92 (0.93, 3.96) - -
Pulmonary tuberculosis 4.01 (2.58, 6.23) 3.22 (2.06, 5.05) Chronic obstructive pulmonary disease 1.99 (1.72, 2.30) 1.92 (1.65, 2.24)
Pneumoconiosis 2.29 (0.67, 7.84) - -
Medications (use vs. non-use)
Statins 1.16 (0.98, 1.37) 1.07 (0.90, 1.27)
Non-statin lipid-lowering drugs 1.10 (0.90, 1.34) - -
† Adjusted for pulmonary tuberculosis and chronic obstructive pulmonary disease