The Significant Association of CCND1 Genotypes with Gastric
Cancer in Taiwan
WU-HSIEN KUO1,2,3, CHUNG-YU HUANG4,5, CHUN-KAI FU2, CHENG-HSI LIAO6,
YUNG-HUNG HSIEH5, CHIN-MU HSU6, CHIA-WEN TSAI6,7, WEN-SHIN CHANG6,8
and DA-TIAN BAU6,7,8
1 Division of Gastroenterology, Department of Internal Medicine, Kaoshiung Armed Forces General Hospital, Kaoshiung, Taiwan. R.O.C;
2 Division of Gastroenterology, Department of Internal Medicine, Taichung Armed Forces General Hospital, Taichung, Taiwan, R.O.C;
3 Department of Medicine, National Defense Medical Center, Taipei, Taiwan, R.O.C;
4 Graduate Institute of Medical Sciences, National Defense Medical Center, Taipei, Taiwan, R.O.C;
5 Department of Pharmacy, Taichung Armed Forces General Hospital, Taichung, Taiwan, R.O.C;
6 Terry Fox Cancer Research Laboratory, China Medical University Hospital, Taichung, Taiwan, R.O.C;
7 Graduate Institute of Basic Medical Science, China Medical University, Taichung, Taiwan, R.O.C;
8 Graduate Institute of Clinical Medical Science, China Medical University, Taichung, Taiwan, R.O.C.
* The authors Wu-Hsien Kuo, Chung-Yu HuangandChun-Kai Fu contributed equally to this work
Correspondence to: Da-Tian Bau, Terry Fox Cancer Research Lab, China Medical University Hospital, 2 Yuh-Der Road, Taichung, 404 Taiwan, Tel: +886 422052121-Ext 7534, e-mail: [email protected] and [email protected]
Running title: Kuo et al: CCND1 in Gastric Cancer
Abstract. Background and Aim: Gastric cancer is one of the most
common malignant tumors all over the world. Due to the perplex initiation and intricate progression mechanisms, early detection and effective treatment of gastric cancer are both difficult to achieve. The genetic polymorphisms encoding critical protein cyclin D1 (CCND1) to regulate cell cycle transition from G1 phase to S phase may determine the susceptibility of individuals to gastric cancer. The study aimed at examining the contribution of CCND1 genotypes to gastric cancer risk in Taiwan. Materials: The genotypes of CCND1 A870G (rs9344) and G1722C (rs678653) were determined by polymerase chain reaction (PCR) and restriction fragment length polymorphism (RFLP) analysis among 358 gastric patients and 358 cancer-free controls, and the distribution of genotypic and allelic frequencies among the two groups were compared. Results: The results showed that there were significant differences between gastric cancer and control groups in the distribution of the genotypes (P=6.86x10-4) and allelic frequency (P=0.0016) in the CCND1 A870G genotype. In addition, individuals who carried the AG or GG genotype had 0.55- and 0.51-fold of odds ratios of developing gastric cancer compared to those who carried the AA genotype (95% confidence
intervals [CI]=0.39-0.76 and 0.32-0.81, respectively). There was no such association of CCND1 G1722C with gastric cancer. Furthermore, there was an obvious interaction of the CCND1 A870G genotype with personal smoking habit on gastric cancer risk (P=0.0005). Conclusion: These findings support the concept that the cell cycle regulation may play a role in gastric cancer initiation and development and the CCND1 A870G genotype maybe a useful biomarker for detection of early gastric cancer.
Key words: Cyclin D1, gastric cancer, genotype, polymorphism, Taiwan.
Gastric cancer is reported to be more common in male and in elder citizens aged 50 years or older (1). Even during these decades several beneficial developments, such as the increasing use of refrigerators, the lowering dependence on salts to preserve food, the elevating availability and intake of fresh fruits and vegetables and the effective control of chronic infection with H. pylori, decreased the incidence of gastric cancer, however, it remained as a critical cancer accounting for 8% of the total cancer incidence and 10% of the total cancer death worldwide (2).
Clinically, the prognosis of gastric cancer is usual poor with a 5-year survival less than 20% for advanced disease (3) because most tumors are currently diagnosed at advanced stages of the disease. The detection of gastric cancer at earlier stages probably gives the best chance to improve prognosis and the determination of individuals with high cancer risk provides us a promising approach to achieve this goal.
The cyclin D1 (CCND1) gene located on human chromosome 1q31- 32 is expressed to regulate the transition through the restriction point in the G1 phase to S phase of the cell cycle. The mechanisms of CCND1 gene amplification, posttranscriptional or posttranslational modifications, rearrangements and polymorphisms can result in abnormal protein levels
and impaired CCND1 function, which may be closely related to carcinogenesis (4). In other types of cancer, such as cutaneous melanoma, esophageal squamous cell carcinoma, breast cancer and bladder cancer, highly expression of CCND1 was frequently found in the tumor cites (5- 8). Besides gene amplification, the transcriptional mRNA and translational protein levels of CCND1 may be controlled by CCND1 genetic polymorphism (9). For instance, the A870G single nucleotide polymorphism (SNP) (rs9344) was associated with an increased risk for cancer development or poor prognosis in squamous cell carcinoma of the head and neck (10, 11), pituitary adenoma (12), lung cancer (13) and urothelial carcinoma (14).
In the literature, the genotypes at CCND1 A870G (rs9344) were reported to be associated with gastric cancer in Japanese (15, 16), Korean (17) and Chinese populations (18). However, whether other SNP at CCND1 may contribute to gastric cancer or CCND1 may contribute to Taiwan gastric cancer susceptibility was never studied. Thus, the specific aim of this study was to determine the genotypic frequency of two SNPs of CCND1, A870G (rs9344) and G1722C (rs678653), in Taiwan gastric cancer population and the possibility to serve as potential biomarkers for
the detection of early gastric cancer.
Materials and Methods
Collection of investigated populations. Three hundred and fifty eight patients diagnosed by experienced surgeons with gastric cancer were included at the outpatient clinics of general surgery at China Medical University Hospital during 2001 to 2009. This study also comprised the same number of non-cancer healthy people selected by matching for age and gender as controls after initial random sampling from the Health Examination Cohort of the hospital. The exclusion criteria of the control group included previous malignancy, metastasized cancer from other or unknown origin and any familial or genetic diseases.
All subjects voluntarily participated, completed a self-administered questionnaire and provided their peripheral blood samples for DNA extraction and genotyping. The details of the characteristics of the patients and controls were summarized in Table I.
CCND1 genotyping conditions. Genomic DNA of each participant was extracted from peripheral blood leucocytes, aliquoted and processed according as previously described (10, 11, 13). The primers used for
CCND1 A870G (rs9344) were: forward 5’-GTG AAG TTC ATT TCC AAT CCG C-3’ and reverse 5’-GGG ACA TCA CCC TCA CTT AC-3’;
for CCND1 G1722C (rs678653): forward 5’-CTC TTG GTT ACA GTA GCG TAG C-3’ and reverse 5’-ATC GTA GGA GTG GGA CAG GT-3’.
The following cycling conditions were performed: one cycle at 94oC for 5 min; 35 cycles of 94oC for 30 s, 55oC for 30 s and 72oC for 30 s; with a final extension at 72oC for 10 min.
Restriction fragment length polymorphism (RFLP) conditions. As for the CCND1 rs9344, the resultant 167 bp PCR product was mixed with 2 U Nci I and incubated for 3 h at 37C. The G form PCR products could be further digested while the A form could not. In the results of gel electrophoresis, two fragments of 145 and 22 bps were presented for the genotype G form while one 167 bp fragment was presented for the genotype A form. As for the CCND1 rs678653, the resultant 159 bp PCR product was mixed with 2 U Hae III and incubated for 3 h at 37C. On digestion with Hae III, the PCR product arising from the G allele was cut into fragments of 111, 26 and 22 bp, whereas the C allele was cut into fragments of 137 and 22 bp. Then, 10 l of product was loaded into a 3%
agarose gel containing ethidium bromide for electrophoresis. The genotype analysis was performed by two researchers independently and blindly and the results were 100% concordant.
Statistical analyses. The Pearson’s Chi-square test or Fisher’s exact test (when the expected number in any cell was less than five) was used to compare the distribution of the CCND1 genotypes between cases and controls. The associations between the CCND1 polymorphisms and gastric cancer risk were estimated by computing odds ratios (ORs) and their 95% confidence intervals (CIs) from unconditional logistic regression analysis with the adjustment for possible confounders. P <
0.05 was considered statistically significant and all statistical tests were two-sided.
Results
The characteristics of age, gender and personal cigarette smoking habits of all the investigated subjects together with the histological subtype and cancer stage of the gastric cancer patients are summarized in Table I. The data showed that there was no difference in the distribution of age
(P=0.5811), gender (P=0.2219) and personal cigarette smoking status (P=0.0912) among gastric cancer patients and non-cancer controls (Table I).
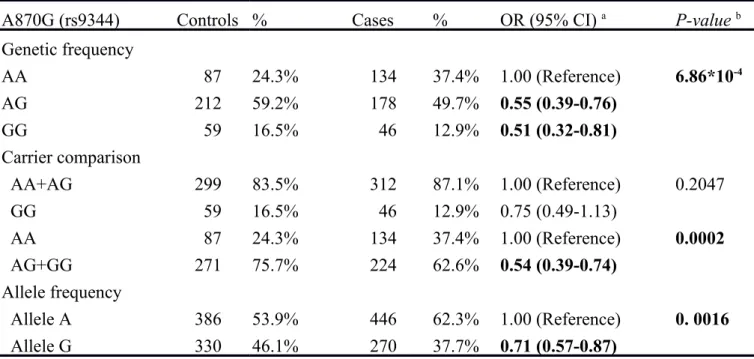
In Table II, the frequencies of the genotypes and alleles of the CCND1 A870G among the investigated gastric cancer patients and non- cancer healthy controls were presented and analyzed. The results showed that the genotypic frequencies of CCND1 A870G was differentially distributed between the control and cancer patient groups (P=6.86x10-4).
The odds ratios of the hetero- and homozygous variant AG and GG were 0.55 (95%CI=0.39-0.76) and 0.51 (95%CI=0.32-0.81), respectively, compared with the wild-type AA genotype. The comparison model of the AG+GG versus AA genotype (OR=0.54, 95%CI=0.39-0.74) also suggested that people of either AG or GG genotypes were of lower gastric cancer risk (Table II). As for the allelic frequency analysis, those who had the G allele were of lower gastric cancer risk (OR=0.71, 95%CI=0.57-0.87) than those who had the A allele at CCND1 A870G.
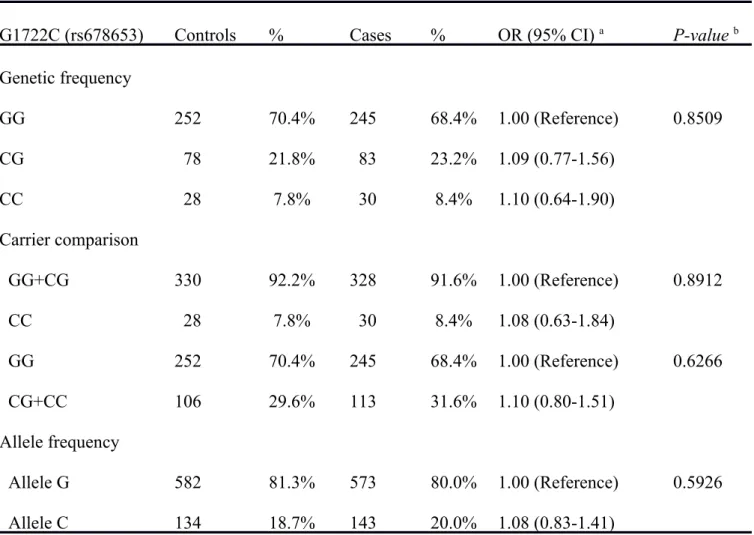
On the contrary, there was no difference in the distributions of either genotypic or allelic frequency between gastric cancer patient and control groups in relation to CNND1 G1722C (Table III). The conclusive
findings deduced from the data in Tables II and III is that CNND1 A870G, but not CNND1 G1722C, can be a potential biomarker for the detection of early gastric cancer. Also, the G allele at CNND1 A870G seems to be a protective genetic factor for gastric cancer progression among the Taiwanese population.
Since personal smoking status is reported to be one of the environmental risk factors for gastric cancer in the literature, we were interested to investigate the interaction of the CNND1 A870G genotype and personal smoking status for gastric cancer risk. As shown in Table IV, the genotypic distributions of CCND1 A870G AA and AG+GG were significantly different between gastric cancer patient smokers and control smokers (P=0.0005) (Table IV). The AG+GG genotypic frequency was much lower (60.9%) among gastric cancer smokers than in healthy smokers (75.6%) and at lower gastric cancer risk (OR=0.50, 95%CI=0.34-0.74). There was no such differential distribution among the non-smokers (P>0.05) (Table IV).
Discussion
Previously, several potential genetic markers for the detection and prediction of early gastric cancer in Taiwan were proposed, including caveolin-1 G14713A, Ku70 T-991C, exonuclease I K589E and XRCC4 G-1394T (19-22). Most of them are SNPs on the DNA repair system genes, while little is known about the contribution of personal genotypes of the cell cycle regulation genes to gastric cancer risk. In the present study, we aimed at investigating the association of CCND1 genotypes and gastric cancer risk in Taiwan. We have selected and genotyped two most commonly investigated polymorphic sites, CCND1 A870G and G1722C, among the 358 gastric cancer cases and 358 age- and gender-matched controls. In Table II, it is shown that subjects carrying the AG and GG genotypes were of lower risk for gastric cancer compared with those carrying the AA genotype on CCND1 A870G (Table II). The combination of AG and GG versus the AA wild-type is also significantly of lower risk for gastric cancer. In addition, the results from the allelic frequency analysis suggest that the G allele is a protective genomic marker for gastric cancer in Taiwan (Table II). As for CCND1 A870G, there was no similar differentially genotypic or allelic distribution found
(Table III). Furthermore, we found that there was a synergistic genetic- lifestyle interaction for CCND1 A870G and personal smoking status (Table IV). However, whether the CCND1 A870G genotype has an interaction with other factors, such as H. pylori infection and/or fruit and vegetable intake, needs to be further investigated.
In the literature, the contribution of CCND1 A870G genotypes to gastric cancer risk has been investigated by several Asian groups with conflicting findings that are summarized in Table V. In 2007, Song and his colleagues, in a study with 253 gastric cancer patients together with 442 cancer-free controls, found that there was no association between CCND1 A870G genotypes and gastric cancer risk. They proposed that the male gastric cancer patients had a significantly higher proportion of the homozygous G/G genotype and that the CCND1 A870G genotype could have contributed to observed gastric cancer risk in men (17). In 2008, a study in Chinese population demonstrated that the risk of gastric cancer for subjects with CCND1 A870G GG or GA genotypes were 2.8- or 1.4- fold higher than those with AA genotype. Furthermore, in the stratification analyses, the risk of GG genotype was more evident in subjects equal to or older than 60 years of age and those positive for H.
pylori infection (18). The findings were valuable but discounted by the limited sample size (159 cases and 162 controls), especially those collected from stratified analysis, demanding validation with larger samples in the near future. Tahara and his colleagues’ continuous investigation added valuable information about the contribution of the CCND1 A870G genotype in relation to gastric cancer risk. First, they recruited people with precancerous conditions, including 111 gastric and 54 duodenal ulcers, as well as 359 non-ulcer subjects, and found that AA genotype carriers held a significant high risk of intestinal metaplasia, especially in older subjects of 61 years or older (23). However, after comparing the CCND1 A870G genotype of the 359 non-ulcer subjects with an equal amount of gastric cancer patients, no positive association was found (15). They further investigated the effects of the CCND1 A870G genotype on the methylation status of the promoter regions of tumor suppressor genes, providing the first evidence that the CCND1 A870G genotype might be involved in methylation-related gastric carcinogenesis, especially in the advanced stage (16). Even the Asian populations were of much more similar genetic background compared with the Western ones, the findings within the Asian countries are
remaining conflicting and inclusive. In addition to genetic background, several factors should be taken into consideration, including the different criteria in the inclusion and exclusion of subjects, study grouping, recording of patient age at diagnosis, genotyping methodologies and most of all the lifestyle background.
To sum up, the current study reports that CCND1 A870G genotypes, synergistically interacted with personal cigarette smoking habit, may increase the personal risk to gastric carcinogenesis in Taiwan. The results provide evidence supporting that gastric carcinogenesis is a complex pathway that involves both inherited and environmental factors. The CG and GG genotypes of CCND1 A870G may be a protective marker in gastric oncology for early detection and prediction.
Acknowledgement
This study was supported by research grants from the Terry Fox Cancer Research Foundation and Taichung Armed Forces General Hospital (103A04, 103A24, and 103A25). The assistance from Tsai-Ping Ho in data collection and genotyping work from Hong-Xue Ji, Chieh-Lun Hsiao, Tzu-Chia Wang, Yun-Ru Syu, Lin-Lin Hou and Chia-En Miao
were highly appreciated by the authors.
References
1 Jemal A, Siegel R, Xu J and Ward E: Cancer statistics, 2010. CA Cancer J Clin 60: 277-300, 2010.
2 Jemal A, Bray F, Center MM, Ferlay J, Ward E and Forman D:
Global cancer statistics. CA Cancer J Clin 61: 69-90, 2011.
3. Nagini S: Carcinoma of the stomach: A review of epidemiology, pathogenesis, molecular genetics and chemoprevention. World J Gastrointest Oncol 4: 156-169, 2012.
4 Jayasurya R, Sathyan KM, Lakshminarayanan K, Abraham T, Nalinakumari KR, Abraham EK, Nair MK and Kannan S:
Phenotypic alterations in Rb pathway have more prognostic influence than p53 pathway proteins in oral carcinoma. Mod Pathol 18: 1056-1066, 2005.
5 Sauter ER, Yeo UC, von Stemm A, Zhu W, Litwin S, Tichansky DS, Pistritto G, Nesbit M, Pinkel D, Herlyn M and Bastian BC:
Cyclin D1 is a candidate oncogene in cutaneous melanoma. Cancer Res 62: 3200-3206, 2002.
6 Lung JC, Chu JS, Yu JC, Yue CT, Lo YL, Shen CY and Wu CW:
Aberrant expression of cell-cycle regulator cyclin D1 in breast
cancer is related to chromosomal genomic instability. Genes Chromosomes Cancer 34: 276-284, 2002.
7 Moonen L, Ong F, Gallee M, Verheij M, Horenblas S, Hart AA and Bartelink H: Apoptosis, proliferation and p53, cyclin D1, and retinoblastoma gene expression in relation to radiation response in transitional cell carcinoma of the bladder. Int J Radiat Oncol Biol Phys 49: 1305-1310, 2001.
8 Nagasawa S, Onda M, Sasajima K, Makino H, Yamashita K, Takubo K and Miyashita M: Cyclin D1 overexpression as a prognostic factor in patients with esophageal carcinoma. J Surg Oncol 78: 208-214, 2001.
9 Sawa H, Ohshima TA, Ukita H, Murakami H, Chiba Y, Kamada H, Hara M and Saito I: Alternatively spliced forms of cyclin D1 modulate entry into the cell cycle in an inverse manner. Oncogene 16: 1701-1712, 1998.
10 Shih LC, Tsai CW, Tsai MH, Tsou YA, Chang WS, Li FJ, Lee MH and Bau DT: Association of cyclin D1 genotypes with nasopharyngeal carcinoma risk. Anticancer Res 32: 1093-1098, 2012.
11 Tsai MH, Tsai CW, Tsou YA, Hua CH, Hsu CF and Bau DT:
Significant association of cyclin D1 single nucleotide polymorphisms with oral cancer in Taiwan. Anticancer Res 31:
227-231, 2011.
12 Simpson DJ, Fryer AA, Grossman AB, Wass JA, Pfeifer M, Kros JM, Clayton RN and Farrell WE: Cyclin D1 (CCND1) genotype is associated with tumour grade in sporadic pituitary adenomas.
Carcinogenesis 22: 1801-1807, 2001.
13 Hsia TC, Liu CJ, Lin CH, Chang WS, Chu CC, Hang LW, Lee HZ, Lo WC and Bau DT: Interaction of CCND1 genotype and smoking habit in Taiwan lung cancer patients. Anticancer Res 31: 3601- 3605, 2011.
14 Lin HH, Ke HL, Hsiao KH, Tsai CW, Wu WJ, Bau DT and Chang LL: Potential role of CCND1 G870A genotype as a predictor for urothelial carcinoma susceptibility and muscle-invasiveness in Taiwan. Chin J Physiol 54: 196-202, 2011.
15 Tahara T, Arisawa T, Shibata T, Yamashita H and Hirata I:
Association between cyclin D1 (CCND1) polymorphism and gastric cancer risk in Japanese population. Hepatogastroenterology
56: 1232-1235, 2009.
16 Tahara T, Shibata T, Nakamura M, Yamashita H, Yoshioka D, Okubo M, Yonemura J, Maeda Y, Maruyama N, Kamano T, Kamiya Y, Fujita H, Nakagawa Y, Nagasaka M, Iwata M, Hirata I and Arisawa T: Association between cyclin D1 polymorphism with CpG island promoter methylation status of tumor suppressor genes in gastric cancer. Dig Dis Sci 55: 3449-3457, 2010.
17 Song JH, Kim CJ, Cho YG, Park YK, Nam SW, Yoo NJ, Lee JY and Park WS: Association of cyclin D1 G870A polymorphism with susceptibility to gastric cancers in Korean male patients.
Neoplasma 54: 235-239, 2007.
18 Jia A, Gong J, Li Y, Hao Z, Chang X, Dai F and Yu B: GG genotype of cyclin D1 G870A polymorphism is associated with non-cardiac gastric cancer in a high-risk region of China. Scand J Gastroenterol 43: 1353-1359, 2008.
19 Lin CH, Lin CC, Tsai CW, Chang WS, Yang CW and Bau DT:
Association of Caveolin-1 Genotypes with Gastric Cancer in Taiwan. Anticancer Res 34: 2263-2267, 2014.
20 Yang MD, Wang HC, Chang WS, Tsai CW and Bau DT: Genetic
polymorphisms of DNA double strand break gene Ku70 and gastric cancer in Taiwan. BMC Cancer 11: 174, 2011.
21 Bau DT, Wang HC, Liu CS, Chang CL, Chiang SY, Wang RF, Tsai CW, Lo YL, Hsiung CA, Lin CC and Huang CY: Single- nucleotide polymorphism of the Exo1 gene: association with gastric cancer susceptibility and interaction with smoking in Taiwan. Chin J Physiol 52: 411-418, 2009.
22 Chiu CF, Wang CH, Wang CL, Lin CC, Hsu NY, Weng JR and Bau DT: A novel single nucleotide polymorphism in XRCC4 gene is associated with gastric cancer susceptibility in Taiwan. Ann Surg Oncol 15: 514-518, 2008.
23 Tahara T, Shibata T, Yamashita H, Hirata I and Arisawa T: Effect of cyclin D1 (CCND1) polymorphism on gastric premalignant condition. Clin Chem Lab Med 46: 1696-1701, 2008.
Table I. Distributions of characteristics of gastric cancer patients and healthy controls.
Characteristics Controls (n = 358) Cancer patients (n = 358) P-value a
n % n %
Mean Age (SD) 62.1 (9.5) 63.8 (11.4) 0.5811
Gender 0.2219
Male 242 67.6% 25
8
72.1%
Female 116 32.4% 10
0
27.9%
Histologic subtype
Intestinal type 20
1
56.2%
Diffuse type 15
7
43.8%
Stage
Early stage 17
3
48.3%
Advanced stage 18
5
51.7%
Personal smoking status
Cigarette smokers 234 65.4% 25
6
71.5% 0.0912
Non-smokers 124 34.6% 10
2
28.5%
aP-value based on two-sided Chi-square test without Yate’s correction.
Table II. Distribution of CCND1 A870G genetic and allelic frequencies among gastric cancer patients and controls.
A870G (rs9344) Controls % Cases % OR (95% CI) a P-value b
Genetic frequency
AA 87 24.3% 134 37.4% 1.00 (Reference) 6.86*10-4
AG 212 59.2% 178 49.7% 0.55 (0.39-0.76)
GG 59 16.5% 46 12.9% 0.51 (0.32-0.81)
Carrier comparison
AA+AG 299 83.5% 312 87.1% 1.00 (Reference) 0.2047
GG 59 16.5% 46 12.9% 0.75 (0.49-1.13)
AA 87 24.3% 134 37.4% 1.00 (Reference) 0.0002
AG+GG 271 75.7% 224 62.6% 0.54 (0.39-0.74)
Allele frequency
Allele A 386 53.9% 446 62.3% 1.00 (Reference) 0. 0016
Allele G 330 46.1% 270 37.7% 0.71 (0.57-0.87)
a OR, odds ratio; CI, confidence interval; b Based on Chi-square test, those bolded were statistically significant.
Table III. Distribution of CCND1 G1722C (rs678653) genetic and allelic frequencies among gastric cancer patients and controls.
G1722C (rs678653) Controls % Cases % OR (95% CI) a P-value b Genetic frequency
GG 252 70.4% 245 68.4% 1.00 (Reference) 0.8509
CG 78 21.8% 83 23.2% 1.09 (0.77-1.56)
CC 28 7.8% 30 8.4% 1.10 (0.64-1.90)
Carrier comparison
GG+CG 330 92.2% 328 91.6% 1.00 (Reference) 0.8912
CC 28 7.8% 30 8.4% 1.08 (0.63-1.84)
GG 252 70.4% 245 68.4% 1.00 (Reference) 0.6266
CG+CC 106 29.6% 113 31.6% 1.10 (0.80-1.51)
Allele frequency
Allele G 582 81.3% 573 80.0% 1.00 (Reference) 0.5926
Allele C 134 18.7% 143 20.0% 1.08 (0.83-1.41)
a OR, odds ratio; CI, confidence interval; b Based on Chi-square test.
Genotypes Non-smokers P-value OR (95% CI) a Smokers P-value OR (95% CI) a
Controls (%) Cases (%) Controls (%) Cases (%)
AA 30 (26.3) 34 (33.3) 0.1401 1.000 (Reference) 57 (24.4) 100 (39.1) 0.0005* 1.000 (Reference)
AG+GG 94 (73.7) 68 (66.7) 0.64 (0.36-1.14) 177 (75.6) 156 (60.9) 0.50 (0.34-0.74)*
Total 124 (100) 102 (100) 234 (100) 256 (100)
a OR, Odds ratio; CI: confidence interval; ORs were estimated with multivariate logistic regression analysis.
*Statistically identified as significant.
First author Year Population Controls (n) Cases (n) Association
Kuo WH* 2014 Taiwanese 358 358 gastric cancer cases Allele A associated with higher risk, especially in smokers
Tahara T 2010 Japanese 139 gastric cancer cases G allele carriers had higher hypermethylation status at tumor suppressor genes, especially those at advanced stage
Tahara T 2009 Japanese 359 392 gastric cancer cases No association
Tahara T 2008 Japanese 359 165 premalignant cases Allele A associated with higher risk, especially in older people
Jia A 2008 Chinese 162 159 gastric cancer cases Allele G associated with higher risk, especially in older people
Song JH 2007 Korean 442 253 gastric cancer cases No association
* The article is the present study