2015/February/18
Type of manuscript: Original article
Manuscript title: Splenectomy correlates with increased risk of pyogenic liver abscess: a nationwide cohort study in Taiwan
Running head: splenectomy and pyogenic liver abscess Authors' full names:
Shih-Wei Lai MD1,2, Hsueh-Chou Lai DM and MS 3,4, Cheng-Li Lin MS 1,5, Kuan-Fu Liao MD and MS 6,7
1College of Medicine, China Medical University and 2 Department of Family Medicine, China Medical University Hospital, Taichung, Taiwan
3College of Chinese Medicine, China Medical University and 4Division of Hepato- gastroenterology, Department of Internal Medicine, China Medical University Hospital, Taichung, Taiwan.
5Management Office for Health Data, China Medical University Hospital, Taichung, Taiwan
6Graduate Institute of Integrated Medicine, China Medical University and 7Department of Internal Medicine, Taichung Tzu Chi General Hospital, Taichung, Taiwan
(The first two authors equally contributed to this study)
Corresponding author: Kuan-Fu Liao, Department of Internal Medicine, Taichung Tzu Chi General Hospital, No.66, Sec. 1, Fongsing Road, Tanzi District, Taichung City, 427, Taiwan
Phone: 886-4-2205-2121; Fax: 886-4-2203-3986 E-mail: [email protected]
Word count: 247 in abstract, 2351 in text, 4 tables and 1 supplemental table, 1 figure and 22 references
ABSTRACT
Objectives. Little is known about the risk of pyogenic liver abscess in patients with splenectomy. We explore the relationship between splenectomy and pyogenic liver abscess in Taiwan. Methods. We conducted a nationwide cohort analysis using the hospitalization dataset of the Taiwan National Health Insurance Program. There were 17779 subjects aged 20-84 years who were newly diagnosed with splenectomy in 1998 to 2010 as the splenectomy group and 70855 randomly selected subjects without splenectomy as the non-splenectomy group. Both groups were matched by sex, age, other comorbidities and hospitalization year of receiving splenectomy. The incidence of pyogenic liver abscess at the end of 2011 was measured. The multivariable Cox
proportional hazard regression model was used to estimate the hazard ratio and 95%
confidence interval for pyogenic liver abscess associated with splenectomy and other comorbidities. Results. The overall incidence rate was 3.75-fold higher in the
splenectomy group than that in the non-splenectomy group (2.15 vs. 0.57 per 1000 person-years, 95% confidence interval 3.57, 3.94). After controlling for potential confounding factors, the adjusted hazard ratio of pyogenic liver abscess was 3.89 in subjects with splenectomy (95% confidence interval 3.20, 4.72), when compared with subjects without splenectomy. In further analysis, the HR markedly increased to 14.34 for those with splenectomy and comorbid with any one of comorbidities including alcoholism, biliary stone, chronic kidney disease, chronic liver diseases and diabetes mellitus (95% CI=10.61, 19.39). Conclusions. Patients with splenectomy are at an increased risk of developing pyogenic liver abscess, particularly comorbid with any comorbidity.
Keywords: alcoholism; diabetes mellitus; pyogenic liver abscess; splenectomy
INTRODUCTION
Human spleen mainly serves as an immune function against invading microorganisms.
Patients with splenectomy are more likely to suffer severe life-threatening infections, which have been recognized as overwhelming postsplenectomy infections with substantial morbidity and mortality. Recently, there is growing evidence that patients with splenectomy are associated with an increased risk of pulmonary tuberculosis and type II diabetes mellitus, but pyogenic liver abscess has not yet been mentioned.
Pyogenic liver abscess is an infective disease of the liver, which can be caused by numerous microorganisms. The overall mortality rate of pyogenic liver abscess ranged from 10 to 25%, depending on the population studied. A increasing amount of
literature reveals that numerous risk factors, such as biliary tract disease, cirrhosis, diabetics mellitus, male, cancer, as well as renal disease, are associated with pyogenic liver abscess, 8-12 but splenectomy has not yet been mentioned.
On the basis of the above-mentioned literature review, we rationally hypothesize an association between splenectomy and pyogenic liver abscess due to the
immunocompromised condition caused by splenectomy, which can further potentially increase the risk of microorganism invasion to the liver. However, published literature from epidemiological studies on this issue is scarce. Given splenectomy associated with overwhelming postsplenectomy infections and pyogenic liver abscess carrying a potential fatality, exploring the risk of pyogenic liver abscess in patients with
splenectomy may have significant clinical and public health implications. We therefore conducted a nationwide cohort study using the hospitalization dataset of the Taiwan National Health Insurance Program to explore whether there is an association between splenectomy and pyogenic liver abscess.
METHODS Data Source
We conducted a nationwide cohort study using the National Health Insurance Research Database (NHIRD) released by the Taiwan National Health Research Institutes. In March 1995, the National Health Insurance Program was initiated in Taiwan to provide comprehensive medical care to the public. According to the annual
statistic report of National Health Insurance Program, the coverage rate was nearly 99% of the entire 23 million people living in Taiwan.13 A committee at the Bureau of National Health Insurance was responsible to randomly select claims and to check the accuracy of claims. The NHIRD encrypts patient’s personal information to protect privacy and provides researchers with anonymous identification numbers associated with relevant claim information, including patient’s sex, date of birth, medical services utilized, and prescriptions. We identified the investigated diseases based on the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9- CM) codes. This study was approved by the Institutional Review Board at China Medical University and Hospital in Taiwan (CMU-REC-101-012).
Sampled Participants
Using the inpatient claim dataset of the NHIRD, all hospitalized subjects aged 20-84 who received splenectomy (ICD-9-CM procedure code 41.5) between January 1, 1998 and December 31, 2010, were identified as the splenectomy group. The date for receiving splenectomy was defined as the index date. For each subject with splenectomy, 4 subjects without splenectomy were randomly selected from the NHIRD as the non-splenectomy group. Both groups were matched by sex, age (every 5-year span), other comorbidities and the hospitalization year of receiving splenectomy.
Subjects with history of pyogenic liver abscess, amebic liver abscess or liver transplantation before the index date were excluded from this study (Figure 1).
Outcome and Comorbidities
The main outcome was a new diagnosis of pyogenic liver abscess based on hospital discharge registries during the follow-up period. Each subject was monitored from the index date until being diagnosed with pyogenic liver abscess, or being censored because of loss to follow-up, death or withdrawal from insurance, or to the end of December 31, 2011.
Comorbidities potentially associated with pyogenic liver abscess were selected in the study as follows: alcoholism, biliary stone, chronic kidney disease, diabetes mellitus and chronic liver diseases including cirrhosis, alcoholic liver damage, hepatitis B, hepatitis C and other chronic hepatitis. All comorbidities were diagnosed with ICD-9- CM (Supplemental Table).
Statistical analysis
The differences between the sex, age and baseline comorbidities between the splenectomy group and the non-splenectomy group were compared by using the Chi-
square test for categorical variables and the t test for continuous variables. Follow-up time (in person-years) was used to estimate the incidence rate and incidence rate ratio (IRR) with 95% confidence interval (CI) of splenectomy group to non-splenectomy group using Poisson regression, by sex, age and follow-up period. The multivariable Cox proportional hazards regression model was used to estimate the hazard ratio (HR) with 95% CI of pyogenic liver abscess associated with splenectomy and other comorbidities after simultaneously controlling for variables found significantly in the univariable Cox proportional hazard regression model. To address the concern of constant proportionality, we examined the proportional hazard model assumption using a test of scaled Schoenfeld residuals. In the model evaluating the pyogenic liver abscess risk throughout overall follow-up period, results of the test revealed a significant relationship between Schoenfeld residuals for splenectomy and follow-up time, suggesting the proportionality assumption was violated (P < 0.001). In the subsequent analyses, we stratified the follow-up duration to deal with the violation of proportional hazard assumption. All statistical analyses were performed using SAS 9.3 (SAS Institute, Cary, North Carolina, USA). Two-tailed P < 0.05 was considered statistically significant.
RESULTS
Baseline information of the study population
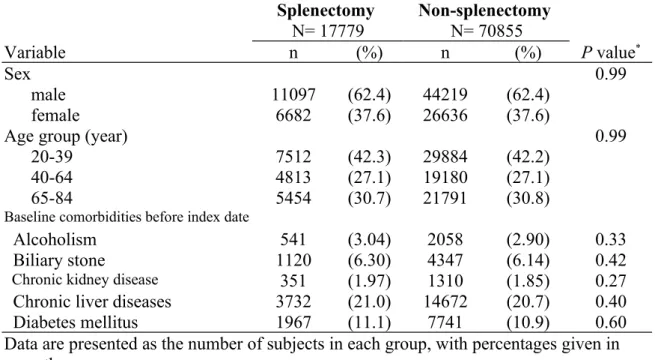
Table 1 reveals the baseline information of the study population. There were 17779 subjects with splenectomy and 70855 subjects without splenectomy during the study period, with similar distribution in sex and age. Male subjects accounted for 62.4% of the study population. The mean age of the splenectomy group was 53.6 ± 17.7 years (mean ± standard deviation) and that of the non-splenectomy group was 53.3 ± 17.8 years, with 42.3% of all subjects aged < 40 years. The mean follow-up period was 4.48
± 4.05 years (mean ± standard deviation) in the splenectomy group and 6.46 ± 3.87 years in the non-splenectomy group. There was no significant difference in the prevalence of comorbidities studied between the splenectomy group and the non- splenectomy group (P < 0.05 for all).
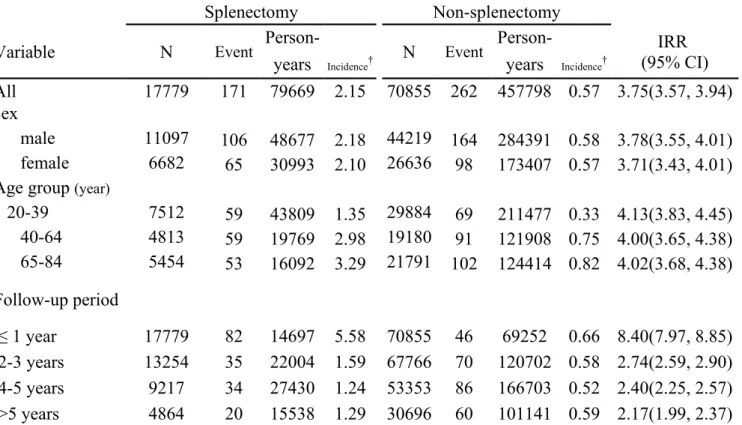
Incidence of pyogenic liver abscess stratified by sex, age and follow-up period Table 2 reveals the incidence rates of pyogenic liver abscess. At the end of the cohort study, the overall incidence rate was 3.75-fold higher in the splenectomy group than that in the non-splenectomy group (2.15 vs. 0.57 per 1000 person-years, 95% CI 3.57,
3.94). The incidence rates of pyogenic liver abscess, as stratified by sex, age and follow-up period, were all higher in the splenectomy group than those in the non- splenectomy group. The incidence rates of pyogenic liver abscess increased with age in both groups, with the highest in the splenectomy group aged 65-84 years. Stratified analysis by follow-up period revealed that the incidence rate of pyogenic liver abscess decreased with the follow-up time in the splenectomy group. The incidence rate ratio of pyogenic liver abscess was significantly higher in the first year of follow-up (incidence rate ratio 8.40, 95% CI 7.97, 8.85), and reduced with increasingly longer period to 2.40 for 5 years of follow-up. The risk remained for more than 5 years of follow-up. In the analysis on the entire follow-up period, the proportional hazard assumption was not met. These observations consistently suggested a time-varying association between splenectomy and pyogenic liver abscess particularly within the first year after splenectomy.
Hazard ratio of pyogenic liver abscess associated with splenectomy
Table 3 reveals the HR of pyogenic liver abscess associated with splenectomy and other comorbidities. Only those found significantly in the univariable analysis were further examined in the multivariable analysis. After controlling for age, alcoholism, biliary stone, chronic liver diseases, chronic kidney disease and diabetes mellitus, the multivariable Cox proportional hazards regression model revealed that the adjusted HR of pyogenic liver abscess was 3.89 for the splenectomy group (95 % CI 3.20, 4.72), when compared with the non-splenectomy group. Alcoholism (adjusted HR 1.77, 95 % CI 1.17, 2.67), biliary stone (adjusted HR 2.19, 95 % CI 1.69, 2.84), chronic kidney disease (adjusted HR 1.93, 95 % CI 1.18, 3.15), chronic liver diseases (adjusted HR 2.50, 95 % CI 2.02, 3.09) and diabetes mellitus (adjusted HR 1.74, 95 % CI 1.37, 2.22) were also associated with pyogenic liver abscess. Every one-year increase in age was associated with a 1.03-fold increased risk of developing pyogenic liver abscess (95% CI 1.02, 1.03).
Interaction effect on risk of pyogenic liver abscess between splenectomy and comorbidities
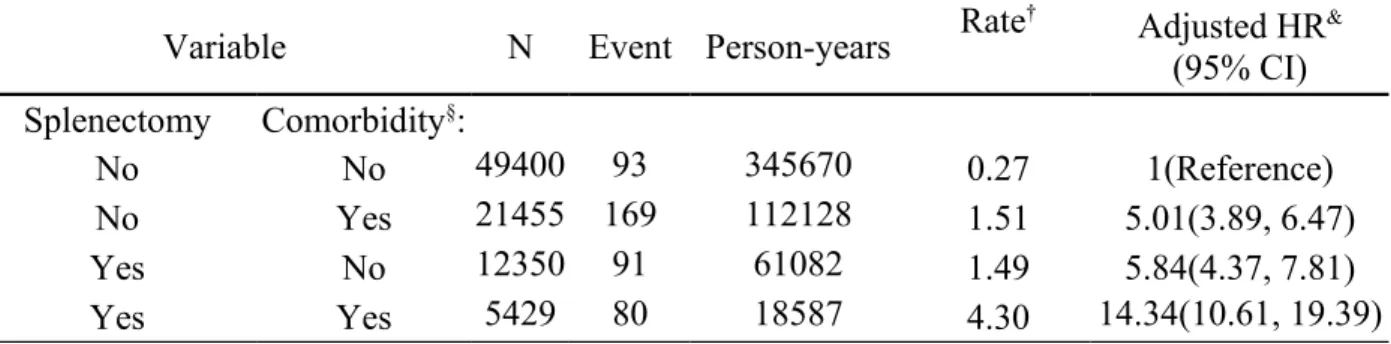
Table 4 reveals interaction effect on risk of pyogenic liver abscess between
splenectomy and other comorbidities including alcoholism, biliary stone, chronic kidney disease, chronic liver diseases and diabetes mellitus. As a reference of subjects without splenectomy and without comorbidity, the adjusted HR of pyogenic liver abscess was 5.84 for subjects with splenectomy alone and without comorbidity (95% CI 4.37, 7.81).
The HR was 5.01 for subjects with any comorbidity and without splenectomy (95% CI 3.89, 6.47). The HR markedly increased to 14.34 for those with splenectomy and comorbid with any comorbidity (95% CI 10.61, 19.39) (P value for interaction < 0.001).
DISCUSSION
In this nationwide cohort study, we found that the incidence rate of pyogenic liver abscess among patients with splenectomy seems to be slightly higher than that among patients with end-stage renal disease by Tsai et al’s study in Taiwan (21.5 vs. 18.2 per 10000 person-years),11 but significantly higher than that among patients with cirrhosis by Molle et al’s study in Denmark (215 vs. 23.3 per 100000 person-years).9 Whether this is due to the difference of patient-finding strategy or patients with splenectomy substantially have a higher risk of developing pyogenic liver abscess needs further research to clarify. In our study, after controlling for potential confounding factors, we also observed that patients with splenectomy were associated with increased risk of pyogenic liver abscess (adjusted HR 3.89). The HR seems to be higher than other comorbidities did. The HR was not confounded by comorbidities studied because there was no significant difference in the prevalence of comorbidities between the
splenectomy group and the non-splenectomy group. It means the increased risk of pyogenic liver abscess in patients with splenectomy cannot be totally attributable to the effect of comorbidities. In further analysis, even in absence of any comorbidity, patients with splenectomy still had a higher risk of pyogenic liver abscess (adjusted HR 5.84).
This indicates that not requiring presence of comorbidity, splenectomy may have a unique role on risk of pyogenic liver abscess. These findings are compatible with the literature that patients with splenectomy are not only more prone to suffer severe life- threatening infection due to the immunocompromised condition caused by splenectomy, but also at an increased risk of developing pyogenic liver abscess.
Extensive evidence has revealed that human spleen mainly serves as a protective role against invading microorganisms on the basis of bactericidal capacity of lymphoid cells and macrophages and the humoral immune response.14-17 Removal of the spleen, normal immune functions such as phagocytic activities and the humoral immune response may be significantly changed. Therefore, the impaired immune functions after splenectomy may potentially increase the risk of life-threatening infection and pyogenic liver abscess.
Some important caveats in this present study deserve discussion. First, the underlying
causes for splenectomy in this present study were not recorded due to the inherent limitation of this insurance database. For example, hematological malignant diseases may need splenectomy in some patients. Cancer is also associated with pyogenic liver abscess. In fact, we observed that cancer was the most common diagnosis accompanied with splenectomy at the time of discharge in this present study. In further analysis, as a reference of patients without splenectomy, the adjusted HR of pyogenic liver abscess was 5.42 for patients with splenectomy and with cancer (95% CI 4.14, 7.10, data not shown in Table). Therefore, whether the risk of pyogenic liver abscess can be
attributable to splenectomy alone or only is confounded by the underlying causes for splenectomy is a critical point in this present study. It needs further research to clarify.
Second, due to the same limitation, the exact causes of pyogenic liver abscess in this present study were not recorded. According to our data, alcoholism, biliary stone, chronic kidney disease, chronic liver diseases and diabetes mellitus may be other factors related to pyogenic liver abscess. Third, the adjusted HR of pyogenic liver abscess was 5.84 for patients with splenectomy alone and the adjusted HR markedly increased to 14.34 for patients with splenectomy and comorbid with any one of comorbidities including alcoholism, biliary stone, chronic kidney disease, chronic liver diseases and diabetes mellitus. Fourth, the highest risk of pyogenic liver abscess was noted within the first year after splenectomy. Although the risk gradually decreased over time, the risk remained for more than 5 years after splenectomy. These findings are compatible with previous studies showing that the majority of severe infections occur within the first 3 years after splenectomy, and even the risk declining over time, the risk might last for more than 5 years after splenectomy.18-20 We think that the impaired immune functions might be more significant within the first year after splenectomy, which more likely precipitates to development of pyogenic liver abscess and other severe infections.
Therefore, when patients presenting with typical features including fever, right upper abdominal pain and body weight loss, 12 clinicians should highly suspect the probability of pyogenic liver abscess among those within the first year after splenectomy,
particularly comorbid with any one of comorbidities included. Fifth, the strength of this study is to use the hospitalization dataset with large sample size and great statistical power. The diagnosis codes of comorbidities included have been validated in previous studies. Last, the topic is novel and the results are fascinating. The study design, statistical methods, and limitations are well described in details. The results suggest some clinical importance and will give us some improvement in more understanding
pyogenic liver abscess. Our results were relatively convincing because the splenectomy group and the non-splenectomy group had similar distributions of comorbidities studied.
The confounding effects of comorbidities on risk of pyogenic liver abscess could be excluded.
In conclusion, patients with splenectomy are at an increased risk of developing pyogenic liver abscess, particularly comorbid with any one of comorbidities including alcoholism, biliary stone, chronic kidney disease, chronic liver diseases and diabetes mellitus.
Acknowledgement
This study is supported in part by Taiwan Ministry of Health and Welfare Clinical Trial and Research Center of Excellence (MOHW104-TDU-B-212-113002), China Medical University Hospital, Academia Sinica Taiwan Biobank, Stroke Biosignature Project (BM104010092), NRPB Stroke Clinical Trial Consortium (MOST 103-2325-B-039 -006), Tseng-Lien Lin Foundation in Taichung in Taiwan, Taiwan Brain Disease Foundation in Taipei in Taiwan, and Katsuzo and Kiyo Aoshima Memorial Funds in Japan. These funding agencies did not influence the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Specific author contributions
Shih-Wei Lai substantially contributed to the conception of this article. He planned and conducted this article. He initiated the draft of the article and critically revised the article.
Hsueh-Chou Lai planned and conducted this article. He critically revised the article.
Cheng-Li Lin conducted the data analysis and critically revised the article.
Kuan-Fu Liao planned and conducted this article. He participated in the data interpretation and critically revised the article.
Conflict of Interest Statement
The authors disclose no conflicts of interest.
REFERENCES
1. Spencer RP, Pearson HA. The spleen as a hematological organ. Seminars in Nuclear Medicine. 1975;5:95-102.
2. Trigg ME. Immune function of the spleen. Southern Medical Journal.
1979;72:593-9.
3. Di Cataldo A, Puleo S, Li Destri G, Racalbuto A, Trombatore G, Latteri F, et al.
Splenic trauma and overwhelming postsplenectomy infection. Br J Surg.
1987;74:343-5. (in eng).
4. Lynch AM, Kapila R. Overwhelming postsplenectomy infection. Infect Dis Clin North Am. 1996;10:693-707. (in eng).
5. Lai SW, Wang IK, Lin CL, Chen HJ, Liao KF. Splenectomy correlates with increased risk of pulmonary tuberculosis: a case-control study in Taiwan. Clin Microbiol Infect. 2014;20:764-7. (in eng).
6. Wu SC, Fu CY, Muo CH, Chang YJ. Splenectomy in trauma patients is
associated with an increased risk of postoperative type II diabetes: a nationwide population-based study. Am J Surg. 2014. (in Eng).
7. Karatassas A, Williams JA. Review of pyogenic liver abscess at the Royal Adelaide Hospital 1980-1987. Aust N Z J Surg. 1990;60:893-7. (in eng).
8. Kaplan GG, Gregson DB, Laupland KB. Population-based study of the epidemiology of and the risk factors for pyogenic liver abscess. Clin Gastroenterol Hepatol. 2004;2:1032-8. (in eng).
9. Molle I, Thulstrup AM, Vilstrup H, Sorensen HT. Increased risk and case fatality rate of pyogenic liver abscess in patients with liver cirrhosis: a nationwide study in Denmark. Gut. 2001;48:260-3. (in eng).
10. Tsai FC, Huang YT, Chang LY, Wang JT. Pyogenic liver abscess as endemic disease, Taiwan. Emerg Infect Dis. 2008;14:1592-600. (in eng).
11. Tsai LW, Chao PW, Ou SM, Chen YT, Shih CJ, Li SY, et al. Pyogenic liver abscess in end-stage renal disease patients: A nationwide longitudinal study.
Hemodial Int. 2014. (in Eng).
12. Krige JE, Beckingham IJ. ABC of diseases of liver, pancreas, and biliary system. BMJ. 2001;322:537-40. (in eng).
13. Database NHIR. Taiwan. http://nhird.nhri.org.tw/en/Background.html. [cited in 2014 October].
14. Eibl M. Immunological consequences of splenectomy. Prog Pediatr Surg.
1985;18:139-45. (in eng).
15. Van Rooijen N. The humoral immune response in the spleen. Res Immunol.
1991;142:328-30. (in eng).
16. Altamura M, Caradonna L, Amati L, Pellegrino NM, Urgesi G, Miniello S.
Splenectomy and sepsis: the role of the spleen in the immune-mediated bacterial clearance. Immunopharmacol Immunotoxicol. 2001;23:153-61. (in eng).
17. Jirillo E, Mastronardi ML, Altamura M, Munno I, Miniello S, Urgesi G, et al.
The immunocompromised host: immune alterations in splenectomized patients and clinical implications. Curr Pharm Des. 2003;9:1918-23. (in eng).
18. Bisharat N, Omari H, Lavi I, Raz R. Risk of infection and death among post- splenectomy patients. J Infect. 2001;43:182-6. (in eng).
19. Kyaw MH, Holmes EM, Toolis F, Wayne B, Chalmers J, Jones IG, et al.
Evaluation of severe infection and survival after splenectomy. Am J Med.
2006;119:276 e1-7. (in eng).
20. Dendle C, Sundararajan V, Spelman T, Jolley D, Woolley I. Splenectomy
sequelae: an analysis of infectious outcomes among adults in Victoria. Med J Aust. 2012;196:582-6. (in eng).
21. Lai SW, Muo CH, Liao KF, Sung FC, Chen PC. Risk of acute pancreatitis in type 2 diabetes and risk reduction on anti-diabetic drugs: a population-based cohort study in Taiwan. Am J Gastroenterol. 2011;106:1697-704. (in eng).
22. Lai HC, Lin CC, Cheng KS, Kao JT, Chou JW, Peng CY, et al. Increased incidence of gastrointestinal cancers among patients with pyogenic liver abscess:
a population-based cohort study. Gastroenterology. 2014;146:129-37 e1. (in eng).
Table 1. Baseline information between splenectomy group and non-splenectomy group
Splenectomy
N= 17779 Non-splenectomy N= 70855
Variable n (%) n (%) P value*
Sex 0.99
male 11097 (62.4) 44219 (62.4)
female 6682 (37.6) 26636 (37.6)
Age group (year) 0.99
20-39 7512 (42.3) 29884 (42.2)
40-64 4813 (27.1) 19180 (27.1)
65-84 5454 (30.7) 21791 (30.8)
Baseline comorbidities before index date
Alcoholism 541 (3.04) 2058 (2.90) 0.33
Biliary stone 1120 (6.30) 4347 (6.14) 0.42
Chronic kidney disease 351 (1.97) 1310 (1.85) 0.27
Chronic liver diseases 3732 (21.0) 14672 (20.7) 0.40
Diabetes mellitus 1967 (11.1) 7741 (10.9) 0.60
Data are presented as the number of subjects in each group, with percentages given in parentheses.
*Chi-square test comparing subjects with and without splenectomy
Table 2. Incidence density of pyogenic liver abscess stratified by sex, age and follow-up period between splenectomy group and non-splenectomy group
Splenectomy Non-splenectomy
Variable N Event Person-
N Event Person- IRR
(95% CI) years Incidence† years Incidence†
All 17779 171 79669 2.15 70855 262 457798 0.57 3.75(3.57, 3.94)
Sex
male 11097 106 48677 2.18 44219 164 284391 0.58 3.78(3.55, 4.01)
female 6682 65 30993 2.10 26636 98 173407 0.57 3.71(3.43, 4.01)
Age group (year)
20-39 7512 59 43809 1.35 29884 69 211477 0.33 4.13(3.83, 4.45)
40-64 4813 59 19769 2.98 19180 91 121908 0.75 4.00(3.65, 4.38)
65-84 5454 53 16092 3.29 21791 102 124414 0.82 4.02(3.68, 4.38)
Follow-up period
≤ 1 year 17779 82 14697 5.58 70855 46 69252 0.66 8.40(7.97, 8.85) 2-3 years 13254 35 22004 1.59 67766 70 120702 0.58 2.74(2.59, 2.90) 4-5 years 9217 34 27430 1.24 53353 86 166703 0.52 2.40(2.25, 2.57) >5 years 4864 20 15538 1.29 30696 60 101141 0.59 2.17(1.99, 2.37) IRR (incidence rate ratio): splenectomy vs. non-splenectomy (95% CI)
†Incidence: per 1000 person-years
Table 3. Adjusted hazard ratio and 95% confidence interval of pyogenic liver abscess associated with splenectomy and other comorbidities
Variable Crude Adjusted†
HR (95%CI) HR (95%CI)
Age (per one year) 1.02 (1.02, 1.03) 1.03 (1.02, 1.03) Baseline comorbidities before
index date (yes vs. no)
Splenectomy 3.60 (2.97, 4.37) 3.89 (3.20, 4.72)
Alcoholism 2.68 (1.82, 3.96) 1.77 (1.17, 2.67)
Biliary stone 3.80 (2.96, 4.87) 2.19 (1.69, 2.84)
Chronic kidney disease 3.14 (1.93, 5.10) 1.93 (1.18, 3.15) Chronic liver diseases 3.35 (2.86,4.06) 2.50 (2.02, 3.09) Diabetes mellitus 3.00 (2.38, 3.77) 1.74 (1.37, 2.22)
†Adjusting for age, alcoholism, biliary stone, chronic kidney disease, chronic liver diseases and diabetes mellitus
Table 4. Interaction effect on pyogenic liver abscess between splenectomy and other comorbidities
Variable N Event Person-years Rate† Adjusted HR&
(95% CI) Splenectomy Comorbidity§:
No No 49400 93 345670 0.27 1(Reference)
No Yes 21455 169 112128 1.51 5.01(3.89, 6.47)
Yes No 12350 91 61082 1.49 5.84(4.37, 7.81)
Yes Yes 5429 80 18587 4.30 14.34(10.61, 19.39)
† Incidence rate: per 1000 person-years
&Adjusting for age
Comorbidity§: patients with any one of comorbidities including alcoholism, biliary stone, chronic kidney disease, chronic liver diseases and diabetes mellitus were classified as the comorbidity group
The interaction between splenectomy and comorbidities was significant.
(P value for interaction < 0.001)
Figure 1. Flow chart depicting the selection process of study participants