Risk of epilepsy in patients with systemic lupus erythematous –A retrospective
cohort study
Running title: Epilepsy and Systemic Lupus Erythematous
Jeng-Dau Tsai, MD, PhD1,2, Cheng-Li Lin, MSPH3,4, Cheng-Chieh Lin, MD, PhD5,6 Fung-Chang Sung, PhD, MPH3,4,7, Ko-Hung Lue, MD, PhD1,2
1Institute of Medicine and 2Department of Pediatrics, Chung Shan Medical University and Hospital, Taichung, Taiwan
3Institute of Clinical and Medical Science, China Medical University, Taichung 404, Taiwan
4Management Office for Health Data, China Medical University Hospital, Taichung 404, Taiwan
5Department of Family Medicine, China Medical University School of Medicine, Taichung 404, Taiwan
6Division of Family Medicine, China Medical University Hospital, Taichung 404, Taiwan
7Department of Health Care Administration, Asia University College of Health Science, Taichung, Taiwan
Drs Ko-Huang Lue and Fung-Chang Sung contributed equally to this work Address for reprints:
Ko-Huang Lue, MD, PhD, Department of Pediatrics, Chung Shan Medical University Hospital,
110 Jianguo North Road Section 1, Taichung 402, Taiwan e-mail: [email protected]
Telephone: (+886)-4-2473-9595 ext. 34112 Fax: (+886)-4-2471-0934
Fung-Chang Sung, PhD, MPH,
Institute of Clinical and Medical Science, China Medical University, 91 Hsueh-Shih Road,
Taichung 404, Taiwan
e-mail: [email protected]
Telephone: (+886)-4-2205-2121 ext 7520 Fax: (+886)-4-2233-9216
Word counts: 245 in Abstract, 2511 in Text, 3 Tables, 2 Figures and 35 references
Abstract
Background: Systemic lupus erythematosus (SLE) affects central and peripheral nervous systems, manifesting neuropsychiatric disorders vary from subtle signs to life-threatening complications. This study
compared the risk of epilepsy between general population and patients with SLE.
Methods: From the national insurance claims data of Taiwan, we identified 32301 patients with SLE newly diagnosed from 1997 to 2010, and 129204 randomly selected comparison people without SLE, frequency matched by gender, age and diagnosis date. The incidence of epilepsy was estimated for both cohorts by the end of
2010.
Results: The incidence of epilepsy was 2.86-fold higher in the SLE cohort than in the non-SLE cohort (9.10 vs. 3.18 per 10,000 person-years), with a Cox method estimated adjusted hazard ratio (aHR) of 2.33(95% confidence interval (CI) = 1.89, 2.88) for the SLE cohort. The incidence increased with age in the non-SLE cohort, while it decreased with the increase of age in the SLE cohort. Compared with the non-SLE cohort, the age-specific aHR of epilepsy for the SLE-cohort decreased from 8.05 (95% CI=4.30-15.0) for those aged ≤ 20 years to 0.90 (95% CI=0.57-1.42) for those aged 60 years and above (p for trend=0.01). Comorbidities that had significant association with epilepsy included infarction (aHR = 7.62), intracerebral hemorrhage (aHR = 5.75), aseptic meninigoencephalitis (aHR = 5.35) and psychiatric disorder
(aHR = 3.31).
Conclusion: Patients with SLE are at higher risk of epilepsy than general population, especially in younger SLE patients. Neurologic comorbidities and psychiatric disorder increase the epilepsy risk further.
Key words: Epilepsy, Incidence, Lupus, Health insurance data, Cohort Study
Introduction
Systemic lupus erythematous (SLE) is a well known inflammatory autoimmune disease, causing dysfunction and damage to systemic organ and nervous systems.1,2,3 Neuropsychiatric manifestations are common in SLE patients, involving active systemic diseases, and psychiatric and neurologic disorders, leading to other complications and increased mortality.4,5 The American College of Rheumatology (ACR) has defined 19 neuropsychiatric manifestations of systemic lupus
erythematous (NPSLE), including several neurological disorders.6 The ACR formulated a nomenclature system to define the 19 NPSLE, including central and peripheral neuropathy.7,8 The Systemic Lupus International Collaborating Clinics
criteria published in 2012 also include some of these SLE syndromes.9
Among these conditions, seizures are recognized as either a direct result of the primary complication or the secondary proinflammatory process of SLE.10,11 Cross sectional and follow-up studies have reported that 6.7 to 14.4% of patients with SLE are suffered from seizures.5,8,12. In a 7.8 years follow-up study, Appenzeller et al.
identified 60 (11.6%) epileptic seizures in 519 SLE patients, with 19 episodes appeared at the onset of SLE symptoms.8 An Italian 10-year multi-center, Gonovi et al. followed a cohort of 959 SLE patients and found 14.4% of epileptic cases13. These studies show that epilepsy is the unfavorable damage in addition to SLE for the
patients, occurring before or at the onset of SLE, or after the diagnosis of the disease.
Most studies observed only patients with SLE without none SLE subjects as a
reference group for the risk comparison. It is possible that SLE and the seizures occur because of a coincidental coexistence, common to a primary disease that causes the
epilepsy.14,15
The relative risk of epilepsy occurring after the SLE diagnosis is in fact not clear.
To the best of our knowledge, no cohort study has measured the risk of epilepsy for SLE patients comparing to general population. In this study, we would like to investigate the age-specific mean prevalence and incidence of epilepsy in SLE patients and general population by using health insurance database in Taiwan. We further performed a retrospective cohort study to evaluate the risk of epilepsy between patients with and without SLE.
Materials and Methods Data sources
The Department of Health in Taiwan incorporated 13 insurance programs into a universal National Health Insurance program in 1995. Since 1998, this program has provided the health care coverage to 99% of the entire 23.74 million people in Taiwan. With governmental authorization, the Taiwan National Health Research Institutes (NHRI) has been responsible to manage the insurance data. We obtained from NHRI longitudinal claims data sets for population insured in the period from 1997 to 2010. NHRI had scrambled patient identifications before the dataset was release to users for privacy protection. This study was exempted from full ethical
review.
Study subjects
All diagnoses of diseases in the claims data were coded using the International Classification of Disease, 9th Revision, Clinical Modification (ICD-9-CM). From the claims data, we identified 32301 patients with SLE (ICD-9-CM code 710.0) newly diagnosed as catastrophic illness patients in 1997-2010, without the history of epilepsy, as the SLE cohort. Diagnosis of SLE follows patients fulfilled the 1997 ACR classification criteria of SLE for at least four criteria. The date of SLE diagnosis was used as the index date. Patients with missing information on age or sex at the baseline were excluded. For each SLE case identified, 4 subjects without the history
of SLE and epilepsy were randomly selected into the non-SLE cohort, from the same insurance claims data set, frequency matched by age, sex, and the diagnosis month
and year of SLE.
Criteria and definition
The follow-up time was estimated for each subject from the index date until the diagnosis of epilepsy or until the subject was censored because of loss to follow-up, death, withdrawal from the insurance system, the end of 2010. The comorbidities with potential association with epilepsy were identified at the baseline from the in-patient claims data, including psychiatric disorder (ICD-9-CM codes 295-296, 300.0, 301, 307.40-307.49, and 309), aseptic meninigoencephalitis (ICD-9-CM codes 322.2, 322.9, 323.8-323.9), intracerebral hemorrhage (ICD-9-CM code 431), infarction (ICD-9-CM codes 433-434), headache (ICD-9-CM code 784.0), and peripheral
neuropathy (ICD-9-CM codes 337, 356.4, 356.8, 356.9, 357.4).
Statistical analysis
Data analysis first calculated the age-specific (<20, 20-29, 30-39, 40-49, 50-59, 60- 69, and 70 years and above) mean incidence and prevalence for both SLE patients and general population aged from 1997 to 2010. For the retrospective cohort study, we compared the distributions of sex, age (<20, 20-39, 40-59 and > 60 years) and comorbidities between the SLE and non-SLE cohorts, examined distributions using the Chi-square test for categorical variables and the t-test for continuous variables.
The sex-and age-specific incidence rates of epilepsy for both cohorts were calculated.
Follow-up time was used to estimate incidence density rate per 10000 person-years by demographic status and comorbidity. The SLE cohort to non-SLE cohort incidence rate ratio (IRR) with 95% confidence interval (CI) by each demographic status and comorbidity were calculated using Poisson regression analysis. Multivariable Cox proportion hazards regression model was used to assess the hazard ratio (HR) of epilepsy for the SLE cohort compared with the non-SLE cohort, with demographic characteristics and comorbid conditions included in the model. The Kaplan-Meier method was used to assess the age-specific cumulative proportional incidence of epilepsy for the 2 cohorts by age and the difference were tested with a log-rank test.
SAS (version 9.1 for windows; SAS institute, Cary, NC, U.S.A.) was used for all statistical analyses. All significant levels were set at 0.05.
Results
Figure 1 shows the mean age-specific average incidence and prevalence of epilepsy in general population and patients with SLE in the 14-year period. Both the incidence and prevalence in the general population were the lowest in the 20-30 years old (0.14 and 0.50 per 100, respectively) and then increased with age in U-shape trends to the highest in 70 years and older (3.5 and 7.0 per 100, respectively). On the other hand, the incidence and prevalence of epilepsy in SLE patients were the highest in the youngest group (1.29 and 1.94 per 100, respectively), which declined slightly and somewhat fell flat with the increase of age. The incidence of epilepsy was 4.5-fold higher in SLE patients than in the general population (1.29 vs. 0.29 per 100) for subjects aged <20 years. The incidence became 9.7-fold higher in the general population than in the SLE patients (3.50 vs. 0.36 per 100). A cross over in incidences between SLE patients and general population occurred in 30-39 years old. Similar trends also appeared for prevalence rates between SLE patients and general
population with the cross over occurred in 30-39 years old.
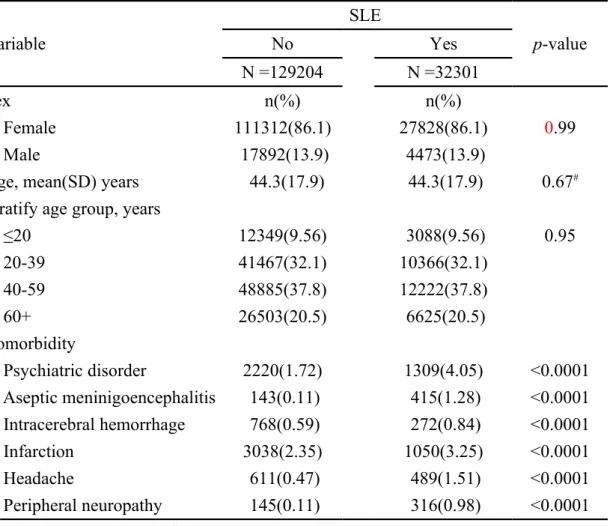
For the retrospective cohort study, we established a cohort of 32301 SLE patients and a non-SLE cohort with 129204 subjects. Age and sex distributions were similar in both the SLE and non-SLE cohorts with a mean age of 44.3 years and prone with women (86.1%) (Table 1). The SLE cohort were more prevalent than the non-SLE cohort with comorbidities of psychiatric disorder, aseptic meninigoencephalitis,
Intracerebral hemorrhage, infarction, headache, and peripheral neuropathy (p
<0.0001).
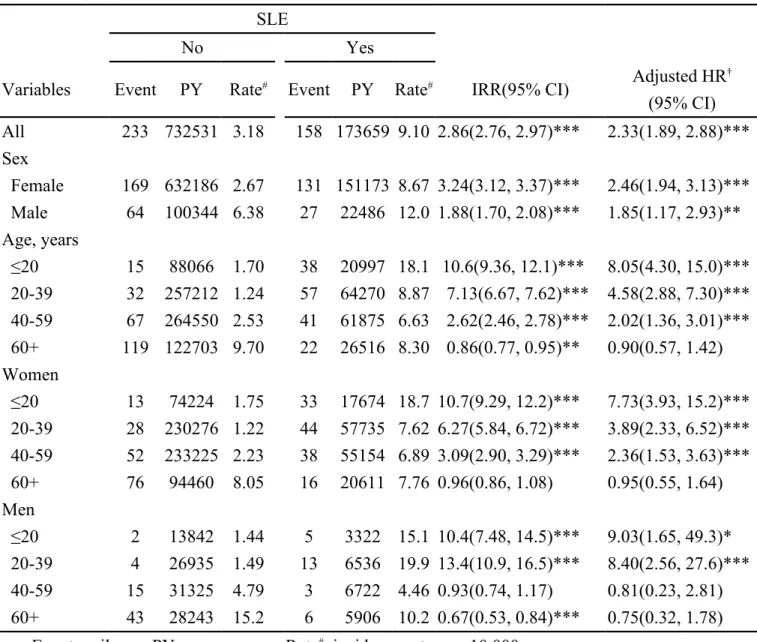
In the longitudinal cohort analysis, the overall incidence of epilepsy was 2.86-fold higher in the SLE cohort than in the non-SLE cohort (9.10 vs. 3.18 per 10,000 person- years) (Table 2), with a multivariable Cox model measured adjusted hazard ratio (aHR) of 2.33 (95% CI = 1.89-2.88). The SLE cohort to non-SLE cohort IRR of epilepsy was higher for women than men (IRR = 3.24, 95% CI = 3.12-3.37 vs. IRR = 1.88, 95% CI = 1.70-2.08). However, the adjusted hazard was significantly higher for
men when compared with women with an adjusted HR of 1.49 (95% CI = 1.18-1.90).
Table 3 shows that comorbidity increased the incidence of epilepsy. SLE patients with comorbidity of intracerebral hemorrhage had the highest incidence of epilepsy (97.8 per 10,000 person-years). However, SLE patients with infarction had the highest aHR of 7.62, 95% CI = 5.87-2.58), followed by comorbidity of intracerebral hemorrhage (aHR = 5.75, 95 % CI = 4.03-8.19), aseptic meninigoencephalitis (aHR = 5.35, 95% CI = 3.46-8.27) and psychiatric disorder (a HR = 3.31, 95% CI = 2.40-
4.58).
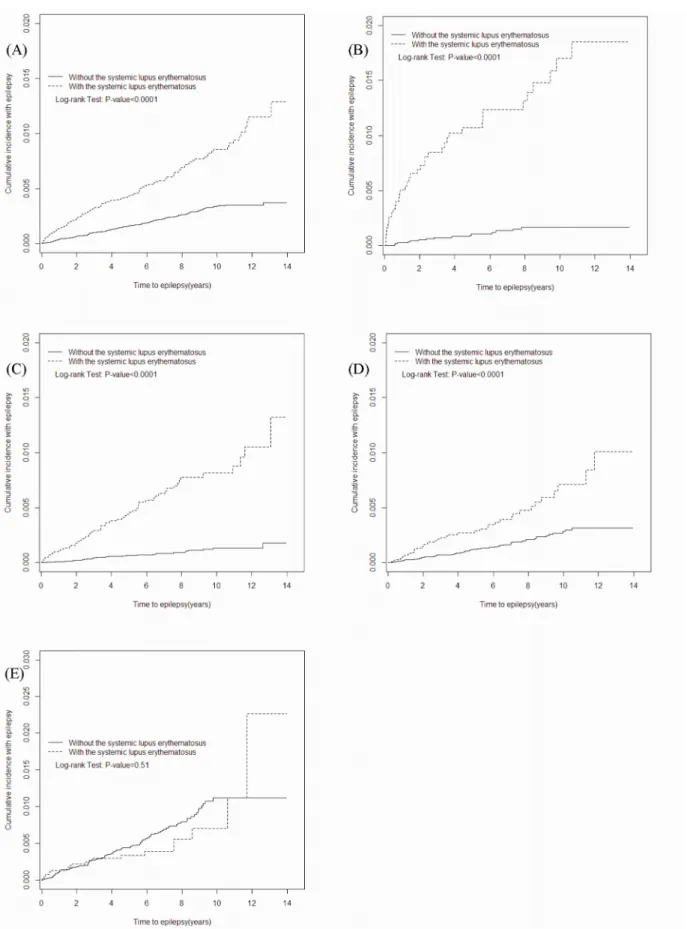
The mean follow-up periods were 5.38 years in the SLE cohort and 5.67 years in the non-SLE cohort. Figures 2A–2D shows the age-specific cumulative proportional incidence of epilepsy by the end of follow-up, compared between the 2 cohorts. The
SLE cohort had significantly higher epilepsy incidence than the non-SLE cohort measured for all subjects and for younger age groups (p <0.0001) except the elderly.
The difference was the greatest for the sub-cohort of <20 years of age, 1.55% greater for SLE subjects than for non-SLE subjects (1.75% vs. 0.20%, p <0.0001). One third of epilepsy cases in the young SLE patients occurred within two years post the diagnosis of SLE.
Discussions
The strength of the present study lies in using the population data, representing national population and allowing us estimate the age-specific occurrences of epilepsy in general population and patients with SLE. The rheumatologists and clinical physicians in Taiwan follow the 1997 ACR classification criteria for SLE and neuropsychiatric systemic lupus erythematosus enable the database standardized.16
The retrospective follow-up design compared the epilepsy incidences between patients with SLE and general population. Using the extended availability of claims
data with high validity enable us to eliminate potential coding biases.17
Patients with lupus may suffer from various neurological symptoms, which contribute to a number of complications and mortality.6,18,19 Among the 19 ACR defined neurolopsychiatric symptoms, from subtle signs of headache and mood disorders to severe life-threatening conditions of cerebrovascular accident, myelopathy and acute confusion, the risk of epilepsy needs adequate measure. The primary central nervous system involvement for SLE patients is a diagnosis challenge as manifestations can be focal, diffuse or a combination.8,15 As results, studies have focused the neurological manifestations in order to reduce complications and mortality. The diagnosis of NPSLE concurrent with SLE is one of the most difficult challenges for clinicians because of the diversity of complications.7
Results of the retrospective cohort analysis in this study demonstrate an overall incidence of epilepsy near 3-fold higher in the SLE cohort than in the non-SLE cohort, even though the severities of the disorders are not available from the claims database. Findings in this study confirm our hypothesis that, with a reference cohort, the epilepsy manifestation may occur at a high risk after SLE being diagnosed.20 Younger SLE patients are at the highest risk and females are more vulnerable than
males to the attack from SLE.
The pathophysiology mechanisms of neuronal damage from seizures and psychosis episodes for SLE patients have been associated with inflammatory cytokines, autoantibodies, and specific and non-specific immune complex.14,21 SLE patients are thus at an elevated risk of vasculopathic cytotoxic and autoantibody- mediated neuronal injury. The consequent microvasculopathy is a common in SLE patients with microscopic brain finding mainly relating to complement activation and antiphospholipid antibodies (APS).22 The exact cause of APS has not been well clarified, but activation of coagulation system is evident. As a result, the secondary APS causes blood to flow improperly and provokes blood clots in vessels leading to
subsequent disorders in central and peripheral nerve system.23,24 The serum anti- neuronal antibodies is prevalent in patients with SLE suffering from neurological manifestations subsequent encephalopathies and seizures.
This study also shows that SLE patients are therefore more likely to suffer stroke than general population without lupus. APS antibody may trigger the formation of blood clots and attack cell membranes inside blood vessels, traveling to the brain causing embolic strokes.25 Inflammation inside blood vessel walls forming vasculitis is particularly dangerous in the brain, leading to the stroke episode.26 Therapeutic strategies recommended for NPSLE manifestations are limited. Biologic agents targeting specific pathway has been proposed as a new tools for SLE treatment.
Among them, B-cell targeted therapeutic experiments are considered as at the forefront in the treatment of SLE. The open-label and randomized clinical trials have
shown the treatment efficacy for SLE and is potentially effective for NPSLE.29
It is important to note in the present study that the mean annual age-specific occurrences of epilepsy are different between SLE patients and non-SLE general population. The incidence and prevalence of epilepsy decrease with age slightly in patients with SLE, while the incidence and prevalence of the disease increase with age, sharply beginning at 40-50 years of age in those without SLE. The U-shape age- specific prevalence of epilepsy in general population is consistent with a previous study.28 A Finland study found a point active epilepsy prevalence of 0.39 per 100 for 6-15 years old children in general population,29 which is comparable to the prevalence of 0.51 per 100 in 6-12 years old children in Norway. 30 Both are lower than our
finding of 0.75 per 100 for children. An Italian study also found a U-shape prevalence of epilepsy by age much higher in children aged 5 to 14 years (5.05 per 1000), approximately 1.7-fold higher than the average prevalence of whole population.31 The age-specific analyses in our study are characterized by the cross over in incidence and prevalence between SLE patients and general population. In the retrospective cohort analysis, we found children with SLE are at the greatest risk of developing epilepsy, near one third of epilepsy cases appear within the first two years after diagnosis with
SLE.
It is likely that the etiology of epilepsy is different between general population and patients with SLE by age.32,33 In non-SLE subjects, the occurrence of epilepsy could be mainly due to other disorders that increase with age, starting 40 years of age.
Reproductive events, higher APS and other psychiatric and neurodevelopmental conditions may have stronger association with developing epilepsy events in general population.33-35 Our study found that the comorbidities increase the epilepsy risk dramatically, particularly those with cerebrovascular disorders and aseptic meninigoencephalitis. Intracerebral hemorrhage and infarction that increase with age may have greater contribution to the epilepsy risk in the older general population. The lower incidence and prevalence of epilepsy in older SLE patients could be due to higher mortality from SLE.
This study used a population data to conduct a natural study evaluating the epilepsy risk for SLE patients. However, certain limitations exist in this study. SLE is considered as a severe catastrophic illness in Taiwan, registered with the physician’s approval and evaluation by the National Bureau of Insurance. However, some patients were reluctant to apply for catastrophic care and they could be thus included in the non-SLE cohort. However, the size was likely minor. The information on clinical
conditions, laboratory data, images and severity of SLE may not be all available. We therefore were unable adapt these factors to evaluate the epilepsy risk. The other limitation is that information on SLE-related disease activity and damage was also
unavailable from insurance database. We are unable to make a clear distinction between acute symptomatic and unprovoked epilepsy in this nationwide population- based study. The residual confounding cannot completely be ruled out based on the
available data. ACR has defined 19 neuropsychiatric manifestations of SLE.
However, the numbers of epilepsy cases identified in this study remain not large enough to differentiate how other manifestations are associated with the occurrence of
epilepsy.
Despite the limitations, this study suggests the age-specific incidence and prevalence of epilepsy trend toward opposite directions between SLE patients and the general population, which may reflect etiological variation. The occurrence of
epilepsy is often unclear of the causes. SLE is a known cause and data in this study clearly shows the seizures tend to appear early in the course of SLE. The NPSLE may be subtle and variable, clinical physicians are aware of the need to carefully search the potential etiologies of undetermined neurological diseases. Epilepsy prevention cares
for young SLE patients deserve a greater attention.
ACKNOWLEDGMENTS
This study was supported by Taiwan Department of Health (grant number DOH102-TD-B-111-004 and DOH102-TD-C-111-005), National Sciences Council
(Grant Numbers NSC 100-2621-M-039-001) and CMUH (Grant Number 1MS1).
DISCLOSURE
None of the authors has any conflict of interest to disclose.
References:
1. D'Cruz DP, Khamashta MA, Hughes GR. Systemic lupus erythematosus. Lancet.
2007; 369:587-96.
2. Rahman A, Isenberg DA. Review Article: Systemic Lupus Erythematosus. N Engl
J Med 2008; 358 (9): 929–939.
3. Popescu A, Kao AH. Neuropsychiatric systemic lupus erythematosus. Curr
Neuropharmacol. 2011; 9:449-57.
4. Benedict RH, Shucard JL, Zivadinov R, Shucard DW. Neuropsychological impairment in systemic lupus erythematosus: a comparison with multiple
sclerosis. Neuropsychol Rev. 2008; 18:149-66.
5. Andrade RM, Alarcón GS, González LA, Fernández M, Apte M, Vilá LM, McGwin G Jr, Reveille JD; LUMINA Study Group. Seizures in patients with systemic lupus erythematosus: data from LUMINA, a multiethnic cohort
(LUMINA LIV). Ann Rheum Dis. 2008; 67:829-34.
6. ACR Ad Hoc Committee on Neuropsychiatric Lupus Nomenclature. The American College of Rheumatology nomenclature and case definitions for
neuropsychiatric lupus syndromes. Arthritis Rheum. 1999, 42:599-608.
7. Rahman A, Isenberg DA. Review Article: Systemic Lupus Erythematosus. N Engl J Med 2008; 358 (9): 929–939.
8. Appenzeller S, Costallat LTL, Cendes F. Neurolupus. Arch Neurol 2006;63:458
63:1808-12.
9. Petri M, Orbai AM, Alarcón GS, et al. Derivation and validation of the Systemic Lupus International Collaborating Clinics classification criteria for systemic lupus
erythematosus. Arthritis Rheum. 2012; 64:2677-86.
10. Hochberg MC. Updating the American College of Rheumatology revised criteria for the classification of systemic lupus erythematosus. Arthritis Rheum. 1997;
40:1725.
11. Hanly JG, Urowitz MB, Su L, et al. Seizure disorders in systemic lupus
erythematosus results from an international, prospective, inception cohort study.
Ann Rheum Dis. 2012; 71:1502-9.
12. Honczarenho K, Budziznowska A, Ostanek L. Neurologic syndroms in systemic lupus erythematosus and thir association with antiphospholipid. Neurol Neurochir
Pol 2008;42: 513–7.
13.Govoni M, Bombardieri S, Bortoluzzi A, Caniatti L, Casu C, Conti F, De Vita S, Doria A, Farina I, Ferraccioli G, Gremese E, Mansutti E, Mosca M, Padovan M, Piga M,Tincani A , Tola MR, Tomietto P, Taglietti M, Trotta F, Valesini G, Zen
M, Mathieu A, on behalf of the Italian Society of Rheumatology. Factors and comorbidities associated with first neuropsychiatric event in systemic lupus erythematosus: does a risk profile exist? A large multicentre retrospective cross- sectional study on 959 Italian patients. Rheumatol 2012;51:157-168
14. Shorvon SD. The etiologic classification of epilepsy. Epilepsia. 2011; 52:1052-7.
15. West SG. Lupus and the central nervous system. Curr Opin Rheumatol. 1996;
8:408-14.
16.Yu HH, Lee JH, Wang LC, Yang YH, Chiang BL. Neuropsychiatric
manifestations in pediatric systemic lupus erythematosus: a 20-year study. Lupus.
2006; 15: 651-7.
17. Fang K, Shia BC, Ma S. Health insurance coverage, medical expenditure and
coping strategy: evidence from Taiwan. BMC Health Serv Res. 2012; 12:442.
18. Souza DC, Santo AH, Sato EI. Mortality profile related to systemic lupus erythematosus: a multiple cause-of-death analysis. J Rheumatol. 2012; 39:496-
503.
19. Bernatsky S, Boivin JF, Joseph L, Manzi S, Ginzler E, Gladman DD, Urowitz M, et al. Mortality in systemic lupus erythematosus. Arthritis Rheum. 2006; 54:2550-
7.
20. Rai D, Kerr MP, McManus S, Jordanova V, Lewis G, Brugha TS. Epilepsy and psychiatric comorbidity: a nationally representative population-based study.
Epilepsia. 2012; 53:1095-103.
21. Vincent A, Crino PB. Systemic and neurologic autoimmune disorders associated with seizures or epilepsy. Epilepsia. 2011; 52 Suppl 3:12-7.
22. Sciascia S, Murru V, Sanna G, Roccatello D, Khamashta MA, Bertolaccini ML.
Clinical accuracy for diagnosis of antiphospholipid syndrome in systemic lupus erythematosus: evaluation of 23 possible combinations of antiphospholipid
antibody specificities. J Thromb Haemost. 2012; 10:2512-8.
23.Borowoy AM, Pope JE, Silverman E, et al. Neuropsychiatric lupus: the
prevalence and autoantibody associations depend on the definition: results from
the 1000 faces of lupus cohort. Semin Arthritis Rheum. 2012; 42:179-85.
24.Rand JH. Antiphospholipid antibody syndrome: new insights on thrombogenic mechanisms. Am J Med Sci. 1998; 316:142-51.
25. Belmont HM, Abramson SB, Lie JT. Pathology and pathogenesis of vascular injury in systemic lupus erythematosus. Interactions of inflammatory cells and
activated endothelium. Arthritis Rheum. 1996; 39:9-22.
26. Kampylafka EI, Alexopoulos H, Kosmidis ML,et al. Incidence and prevalence of major central nervous system involvement in systemic lupus erythematosus: a 3-
year prospective study of 370 patients. PLoS One. 2013; 8:e55843.
27. Chen CC, Chen LS, Yen MF, Chen HH, Liou HH. Geographic variation in the age- and gender-specific prevalence and incidence of epilepsy: analysis of
Taiwanese National Health Insurance-based data. Epilepsia. 2012; 53:283-90.
28. Eriksson KJ, Koivikko MJ. Prevalence, classification, and severity of epilepsy and epileptic syndromes in children. Epilepsia. 1997; 38:1275-82.
29.Murdaca G1, Colombo BM, Puppo F. Emerging biological drugs: a new
therapeutic approach for Systemic Lupus Erythematosus. An update upon efficacy
and adverse events. Autoimmun Rev. 2011; 11:56-60.
30. Waaler PE, Blom BH, Skeidsvoll H, Mykletun A. Prevalence, classification, and
severity of epilepsy in children in western Norway. Epilepsia. 2000; 41:802-10.
31. Gallitto G, Serra S, La Spina P, Postorino P, Laganà A, Tripodi F, Gangemi S, et al. Prevalence and characteristics of epilepsy in the Aeolian islands. Epilepsia.
2005; 46:1828-35.
32. González-Duarte A, Cantú-Brito CG, Ruano-Calderón L, García-Ramos G.
Clinical description of seizures in patients with systemic lupus erythematosus. Eur
Neurol. 2008; 59:320-323.
33. Adelöw C, Andersson T, Ahlbom A, Tomson T. Unprovoked seizures in multiple sclerosis and systemic lupus erythematosus: a population-based case-control
study. Epilepsy Res. 2012; 101:284-7.
34. Nicoletti A, Reggio A, Bartoloni A, Failla G, Sofia V, Bartalesi F, Roselli M, et al. Prevalence of epilepsy in rural Bolivia: a door-to-door survey. Neurology.
1999; 10; 53:2064-9.
35. Shoenfeld Y, Lev S, Blatt I, Blank M, Font J, von Landenberg P, Lev N,et al.
Features associated with epilepsy in the antiphospholipid syndrome. J Rheumatol.
2004; 31:1344-8.
Table 1 Demographic characteristics and comorbidities compared between cohorts with and without systemic lupus erythematosus
Variable
SLE
p-value
No Yes
N =129204 N =32301
Sex n(%) n(%)
Female 111312(86.1) 27828(86.1) 0.99
Male 17892(13.9) 4473(13.9)
Age, mean(SD) years 44.3(17.9) 44.3(17.9) 0.67#
Stratify age group, years
≤20 12349(9.56) 3088(9.56) 0.95
20-39 41467(32.1) 10366(32.1)
40-59 48885(37.8) 12222(37.8)
60+ 26503(20.5) 6625(20.5)
Comorbidity
Psychiatric disorder 2220(1.72) 1309(4.05) <0.0001 Aseptic meninigoencephalitis 143(0.11) 415(1.28) <0.0001 Intracerebral hemorrhage 768(0.59) 272(0.84) <0.0001
Infarction 3038(2.35) 1050(3.25) <0.0001
Headache 611(0.47) 489(1.51) <0.0001
Peripheral neuropathy 145(0.11) 316(0.98) <0.0001 Chi-square test except #Two-sample t-test
Figure 1 Mean age-specific incidence and prevalence of epilepsy identified in general population and patients with systemic lupus erythematosus from 1997 to 2010 in Taiwan
Table 2 Sex and age specific incidence of epilepsy and SLE cohort to non-SLE cohort incidence rate ratio and adjusted hazard ratio
SLE
No Yes
Variables Event PY Rate# Event PY Rate# IRR(95% CI) Adjusted HR† (95% CI) All 233 732531 3.18 158 173659 9.10 2.86(2.76, 2.97)*** 2.33(1.89, 2.88)***
Sex
Female 169 632186 2.67 131 151173 8.67 3.24(3.12, 3.37)*** 2.46(1.94, 3.13)***
Male 64 100344 6.38 27 22486 12.0 1.88(1.70, 2.08)*** 1.85(1.17, 2.93)**
Age, years
≤20 15 88066 1.70 38 20997 18.1 10.6(9.36, 12.1)*** 8.05(4.30, 15.0)***
20-39 32 257212 1.24 57 64270 8.87 7.13(6.67, 7.62)*** 4.58(2.88, 7.30)***
40-59 67 264550 2.53 41 61875 6.63 2.62(2.46, 2.78)*** 2.02(1.36, 3.01)***
60+ 119 122703 9.70 22 26516 8.30 0.86(0.77, 0.95)** 0.90(0.57, 1.42)
Women
≤20 13 74224 1.75 33 17674 18.7 10.7(9.29, 12.2)*** 7.73(3.93, 15.2)***
20-39 28 230276 1.22 44 57735 7.62 6.27(5.84, 6.72)*** 3.89(2.33, 6.52)***
40-59 52 233225 2.23 38 55154 6.89 3.09(2.90, 3.29)*** 2.36(1.53, 3.63)***
60+ 76 94460 8.05 16 20611 7.76 0.96(0.86, 1.08) 0.95(0.55, 1.64)
Men
≤20 2 13842 1.44 5 3322 15.1 10.4(7.48, 14.5)*** 9.03(1.65, 49.3)*
20-39 4 26935 1.49 13 6536 19.9 13.4(10.9, 16.5)*** 8.40(2.56, 27.6)***
40-59 15 31325 4.79 3 6722 4.46 0.93(0.74, 1.17) 0.81(0.23, 2.81) 60+ 43 28243 15.2 6 5906 10.2 0.67(0.53, 0.84)*** 0.75(0.32, 1.78)
Event: epilepsy, PY, person-years; Rate#, incidence rate, per 10,000 person-years;
IRR, incidence rate ratio; Adjusted HR†: multivariable analysis including age, sex, and comorbidities
*p<0.05, **p<0.01, ***p<0.001
Table 3 Incidence rates of epilepsy by comorbidity and SLE cohort to non-SLE cohort incidence rate ratio and adjusted hazard ratio
SLE
No Yes
Variables Event PY Rate# Event PY Rate# IRR*(95% CI) Adjusted HR
(95% CI) Psychiatric disorder
No 205 719949 2.85 138 166012 8.31 2.92(2.81, 3.03)*** 1(Reference) Yes 28 12582 22.3 20 7647 26.2 1.18(0.95, 1.45) 3.31(2.40, 4.58)***
Aseptic
meinigoencephalitis
No 226 731815 3.09 138 171203 8.06 2.61(2.51, 2.71)*** 1(Reference)
Yes 7 716 97.8 20 2456 81.4 0.83(0.49, 1.41) 5.35(3.46, 8.27)***
Intracerebral hemorrhage
No 207 728426 2.84 145 172330 8.41 2.96(2.85, 3.07)*** 1(Reference) Yes 26 4105 63.3 13 1329 97.8 1.54(1.07, 2.23)* 5.75(4.03, 8.19)***
Infarction
No 153 716325 2.14 126 167978 7.50 3.51(3.38, 3.65)*** 1(Reference) Yes 80 16205 49.4 32 5681 56.3 1.14(0.93, 1.39) 7.62(5.87, 9.88)***
Headache
No 224 729272 3.07 154 170747 9.02 2.94(2.83, 3.05)*** 1(Reference)
Yes 9 3258 27.6 4 2912 13.7 0.50(0.32, 0.77)** 1.42(0.78, 2.58)
Peripheral neuropathy
No 231 731714 3.16 152 172004 8.84 2.80(2.70, 2.90)*** 1(Reference)
Yes 2 817 24.5 6 1655 36.3 1.48(0.75, 2.92) 1.20(0.57, 2.56)
PY, person-years; Rate#, incidence rate, per 10,000 person-years; IRR*, incidence rate ratio; Adjusted HR†: multivariable analysis including age, sex, and comorbidities
*p<0.05, **p<0.01, ***p<0.001
Figure 2 Kaplan-Meier method estimated cummulative incidence of epilepsy in SLE cohort and non-SLE cohort by age: (A) Overall, (B) <20 years old, (C) 20-39 years, (D) 40-59 years, (E) 60+years