Accur ate Diagnosis of Helicobacter pylori infection by Stool Antigen Test and Six Other Cur r ently Available Tests in Children
Yen-Hsuan Ni, MD, PhD, Jaw-Town Lin*, MD, PhD, Shiu-Feng Huang#, MD, PhD,
Jyh-Chin Yang*, MD, and Mei-Hwei Chang, MD
Departments of Pediatrics, Internal Medicine*, and Pathology#
National Taiwan University Hospital,
College of Medicine, National Taiwan University,
Taipei, Taiwan
Corresponding author:
Mei-Hwei Chang, MD
Department of Pediatrics, National Taiwan University Hospital,
7, Chung-Shan South Road, Taipei, Taiwan 100
Tel: 886-2-23970800 ext 5131, 5509
Fax: 886-2-23938871
Email: [email protected]
Key words: Helicobacter pylori, urease, 13
C-urea breath test, stool antigen test,
ABSTRACT
Helicobacter pylori (H. pylori) infection has been associated with gastritis,
peptic ulcer, and gastric malignancy. Invasive and noninvasive tests have been
developed for the diagnosis of H. pylori infection. Since H. pylori infection is mostly
acquired in childhood and adolescence, accurate diagnosis of the infection in the
pediatric population is important. The noninvasive diagnostic methods are particularly
feasible in children. We conducted a study to compare the invasive tests: culture,
biopsy urease test (BUT), histology, and polymerase chain reaction (PCR) on gastric
biopsy specimens, with noninvasive tests: serology, 13
C-urea breath test (13
C-UBT),
and a new diagnostic modality: stool antigen test to diagnose H. pylori infection in
children. A total of 53 symptomatic children were enrolled into this study and all had
completed the seven diagnostic tests for H. pylori. Our results showed all the
diagnostic tests except serology were excellent methods of diagnosing H. pylori
infection in children. The diagnostic accuracy of the seven tests were as follows: stool
antigen test 96.2%; BUT 96.2%; histology 98.1%; PCR 94.3%; culture 98.1%; 13
C-UBT 100%; and serology 84.9%. Stool antigen test, being highly sensitive and
specific as shown in our data, will be potentially very helpful in diagnosing H. pylori
List of Abbreviations
H. pylori Helicobacter pylori
UBT Urea breath test
PCR Polymerase chain reaction
INTRODUCTION
Helicobacter pylori (H. pylori) infection has been linked to gastritis, 1-3
duodenal
ulcer, 4,5
gastric cancer,6
and mucosa-associated lymphoid tissue lymphoma. 7
It is now
generally agreed that most H. pylori infections are acquired during childhood or
adolescence, both in developing and developed countries.8
H. pylori infection causes
similar disease patterns in children as adults except for the rarity of malignancies. H.
pylori infection was found in 90% of children with duodenal ulcers and in 25% of
children with gastric ulcers.5, 9
Acquisition of H. pylori at an early stage might
increase the risk of developing gastric cancer.10
The association of H. pylori infection
to many clinical conditions in childhood increases the demand for an accurate
diagnosis of H. pylori in childhood.
Two categories of diagnostic methods for H. pylori infection are defined:
invasive tests to detect the microorganisms in biopsies sample of the gastric mucosa
obtained through endoscopy, and noninvasive tests which obviate the need for
endoscopy. These diagnostic tests have been applied to diagnose H. pylori infection in
adults as well as in children. Deep sedation or even general anesthesia is sometimes
required for endoscopy in children, while this procedure remains valuable in pediatric
patients with symptoms suggesting peptic ulcer. Noninvasive tests, such as urea
following-up H. pylori infection in children.11
Although several studies have simultaneously compared the diagnostic accuracy
among different methods in adult patients,12-14
none have been conducted among
pediatric patients. In this study, we have analyzed the diagnostic values of seven
different tests for H. pylori infection, including culture, histology, biopsy urease test
(BUT), polymerase chain reaction (PCR), 13
C-UBT, serology, and particularly, a
newly developed stool antigen test.15
This comparison may help to validate the
diagnostic accuracy of the newly developed noninvasive stool antigen test. For those
who are unable to cooperate to inhale and exhale on command, stool antigen test will
be a good alternative for diagnosing H. pylori infection.
PATIENTS AND METHODS
Patients. From July 1, 1998 to August 30, 1999, fifty-three consecutive symptomatic children who received endoscopic examination in Department of
Pediatrics, National Taiwan University Hospital, were enrolled into this study. There
were 31 females and 22 males with a median age of 12 years, ranging from 10 to 14
years. All patients had recurrent abdominal pain and epigastralgia for at least one
month. In addition, thirteen had hunger pain, five had family history of H.
pylori-associated duodenal ulcer, and two were evaluated for coexistent anemia. A booklet
procedures in this study was distributed to the patients and their parents. Informed
consents were obtained from all of their parents. Subjects who could not tolerate
endoscopy or who had been treated with antibiotics, H2-blockers, or proton pump
inhibitors in the recent six weeks were excluded from the study. If the subjects had
ever been documented to have H. pylori infection, they would also be excluded from
the study.
Endoscopy, biopsy, and biopsy urease test (BUT). All children received intramuscular injection of meperidine (2mg/kg, maximum 50 mg), and hyoscine
butylbromide (0.5 mg/kg) before endoscopic examination. None of them was deeply
sedated or underwent the endoscopic procedure under general anesthesia. Four
biopsied specimens were taken at the antrum, 1-3 cm from the pyloric canal, and
another three biopsied specimens were taken from the gastric corpus. These
specimens were processed for BUT, culture, histologic examinations, and PCR.
CLO test (Delta West, Bently, Australia) was adopted as BUT to detect the urease
activity in biopsied specimens. The chromogenic reaction was read after one hour and
24 hours after of incubation.
Histologic examinations. The specimens were snapped to phosphate-buffered formalin, subjected to paraffin-embedding, and stained with hematoxylin and eosin.
Polymerase chain reaction (PCR). The biopsied antrum tissues were minced and the DNA was extracted using the DNA extraction kit (Qiagen, Chatsworth, CA, USA).
Each biopsied specimen was finally adjusted to a DNA concentration of 0.1μg/μl.
The nucleotide sequences of primers (first and nested) are from H. pylori urease C
genome as previously described.17
If there was no product after the first run of PCR, 1 μl of first run PCR product was subjected to the nested PCR. A DNA fragment containing the sequences of urease C gene is cloned, expressed, and serially diluted.
This was used in the sensitivity assay as a positive control.
Bacterial culture. The procedures were described previously.18
Briefly, biopsied
specimens were immediately snapped into a brain-heart infusion broth. After grinding
and transformation, they were streaked in the blood agar plate and incubated at 35-37 ℃ under microaerophilic conditions (5% O2, 10%CO2, 85% N2) for 3-7 days. Organ-isms were identified as H. pylori on the basis of colony structure, results of Gram
stain, and the production of urease, oxidase, and catalase.
13
C-Urea breath test (13C-UBT). Infrared spectrophotometer (UBiT-IR200, Otsuka Electronics Co., Hirakata, Japan) was applied in this study.19,20
It had been validated
and correlated well with mass spectrometric analysis.21
The patient fasted overnight
before the test. The procedures were done following the manufacturer’s instruction.
ingestion of powder containing 100mg 13
C-urea in 100 cc drinking water. The two
bags were inserted into the inlets of infrared spectrophotometer and the increased
percentage of 13
CO2 urea could be shown in five minutes. The cut-off point was 4.5‰ .
Serology test. HEL-p II test kit (Amrad, Boronia, Victoria, Australia) for the determination of H. pylori IgG antibody was used in this study. This is an
enzyme-linked immunoadsorbent assay which has been validated in a previous adult
adenocarcinoma study.22
Because there was no data available to document the optimal
cut off point for H. pylori IgG antibody in children, we arbitrarily set it according to
the manufacturer’s instruction. All samples were tested in duplicate.
Stool antigen test. A fresh stool sample about the size of a peanut was collected and stored at –20°C for analysis as described previously.23
H. pylori stool antigens were
detected by a commercial kit (HpSA Microwell EIA, Meridian Diagnostic Inc,
Cincinnati, OH, USA) using an enzyme-linked immunoadsorbent assay. This is an
qualitative test utilizing a polyclonal rabbit anti-H. pylori antibody adsorbed to
microwells. Diluted stool samples and a peroxidase-conjugated secondary polyclonal
antibody were added to the microwells and incubated for one hour at room
temperature. Reading of the results was based on spectrophotometric analysis.
Reading of the results was based on spectrophotometric analysis: OD450< 0.14 is
should be repeated.
Standards for determination of H. pylori infection. All the tests were read
independently without knowing the results of other tests. The final results of H. pylori
infection status was defined as “infected” when the culture was positive or
concordance of at least two of the three conventional tests (histology, BUT, 13
C-UBT).
Patients with negative results on all the above four tests (culture, histology, BUT, and 13
C-UBT) were defined as “non-infected”. Those who could not be categorized into
the above criteria were classified as “indeterminant” and excluded from the analysis.
RESULTS
Patients. A total of 53 children (31 females and 22 males) were enrolled into this study. Endoscopic diagnosis revealed active duodenal ulcer in three, duodenal ulcer
scar with fold convergence in two, antral nodularity in 19, hyperemic mucosa at
antrum and corpus in 19, and negative findings in the remaining 10 patients. The
diagnostic results for culture, histology, BUT, and 13
C-UBT are described in Table 1.
H. pylori status was diagnosed as “infected” in 27 cases, “non-infected” in the other
26 cases, and 0 in the “indeterminant” group.
Diagnostic accuracy of seven tests. The diagnostic accuracy of the seven tests were as follows: stool antigen test 96.2%; BUT 96.2%; histology 98.1%; PCR 94.3%;
culture 98.1%; 13
values for a positive or negative test, and diagnostic accuracy were calculated and are
shown in Table 2. For the stool antigen, there was no false positive and two cases
were false negative. None of stool samples were read as “equivocal” in this study.
Stool antigen test had a 92.6% sensitivity, 100% specificity, positive predictive value
of 100%, and negative predictive value of 92.9%. BUT results showed two false
negative cases and zero false positive. For the 25 cases BUT positive, 24 cases were
read reactive within one hour (range 5-30 minutes) and only one case was read
reactive 80 minutes after the biopsy. For the PCR, there was one false positive and
two false negative result. For IgG anti-H. pylori, there were five false positive cases
and three false negative cases.
DISCUSSION
To the best of our knowledge, this is the first report to simultaneously compare
seven different diagnostic modalities for H. pylori in the pediatric population. In this
study, we have demonstrated that current modalities to diagnose H. pylori infection in
adults are similarly accurate in children, except for IgG antibody to H. pylori. Both
invasive and noninvasive tests were satisfactory, with an accuracy rate about 95%.
Duodenal ulcer in children is highly associated with H. pylori infection.5
The risk
of developing gastric cancer is also relatively high if H. pylori infection is acquired at
a young age.10
infection is important. To achieve this, accurate diagnosis of H. pylori infection in
children is essential. At present, diagnosis of H. pylori infection in children still
largely depends on the endoscopic biopsy of the gastric tissues for culture and urease
test.24
These methods were regarded as the gold standard. However, the invasive
nature limits its wide use in children. Noninvasive diagnostic tests, including 13
C-UBT and serology, were recently developed and shown to be promising in
establishing the diagnosis of H. pylori infection in children.
Stool antigen test is a new noninvasive test and was reported to have a
comparable diagnostic value to any other diagnostic test in adults.23,25
However, there
have been no reports about the application of stool antigen test in children. Our data
proves that this test works well in children. It gave 100% specificity and 92.6%
sensitivity and the diagnostic accuracy is 96.2%. All the values were comparable to
other tests (Table 2). Its advantage over 13
C-UBT for children is no need to exhale air,
making it much easier for children who still cannot cooperate to inhale and exhale on
command. Further investigation of stool antigen test in infants are needed to validate
its use.
Non-dispersive infrared spectrometry was used to analyze 13
CO2 in this study.
Although it requires more exhaled gas to be collected than the conventional 13 CO2
sensitive and specific in adult patients.26
Rowland et al. reported that the sensitivity
and specificity of 13
C-UBT could be as high as 100%, and 97.6% if the subjects were
fasting.27
Our data also supported that 13
C-UBT is of good diagnostic accuracy in
school-aged children. It offers a feasible way for diagnosing H. pylori infection, and
monitoring the therapeutic effects in children who can successfully follow the
procedure of 13
C-UBT.
Most commercially available IgG antibody to H. pylori kits performed equally.28
They have some pitfalls for diagnosis and therapeutic monitoring in children.29,30
Probably due to the duration of infection and the difference in immunity and bacterial
load, the antibody levels in children differ from the adults.31
Moreover, spontaneous
clearance of H. pylori may occur in some children with persistent antibody, thus
resulting in false positive serological tests.32,33
The serological tests are not good to
detect previous infections since the titers decrease below the cut off value within
months after eradication of H. pylori infection. Our data also demonstrated this test is
of the least diagnostic value among the seven tests.
Noninvasive tests are not able to completely replace invasive tests such as
endoscopic examinations. The majority of pediatricians will prefer to eradicate H.
pylori infection according to the endoscopic and histologic examinations, rather than
severity of H. pylori infection still depends upon these invasive tests. Endoscopic
examination is especially indispensable since the current guidelines for eradication
therapy do not advocate treatment for all H. pylori-infected children.34
At present, we
suggest an endoscopic examination should be done before H. pylori eradication to
define the gastroduodenal pathology both endoscopically and histologically.
In conclusion, this study demonstrated the currently available invasive (culture,
BUT, PCR, histology) and noninvasive (UBT, and stool antigen test) diagnostic
methods for H. pylori infection are excellent in children. Serology is the least valuable
diagnostic method in children. Particularly, stool antigen test is potentially valuable in
diagnosing and following up H. pylori infection in children because of its accessibility
REFERENCES
1. Warren JR, Marshall BJ. Unidentified curved bacilli on gastric epithelium in active
chronic gastritis. Lancet 1983;i:1273-5.
2. Marshall BJ, Warren JR. Unidentified curved bacilli in the stomach of patients with
gastritis and peptic ulceration. Lancet 1984;i: 1311-4.
3. Tsai CJ, Chang MH, Tsai TC, Huang FC, Yang JC, Shun CT. Helicobacter pylori
infection and duodenal ulcer in children and adolencents. Acta Paediatr Sin
1996;37:415-9.
4. NIH consensus conference Helicobacter pylori in peptic ulcer disease. NIH
consensus development panel on Helicobacter pylori in peptic ulcer disease. JAMA
1994;272: 65-9.
5. Huang FC, Chang MH, Hsu HY, Lee PI, Shun CT. Long-term follow-up of
duodenal ulcer in children before and after eradication of Helicobacter pylori. J
Peidiatr Gastroenterol Nutr 1999;28:76-80.
6. Parsonnet J, Friedman GD, Vandersteen DP, Chang Y, Vogelman JH, Orentriech N,
et al. Helicobacter pylori infection and the risk of gastric carcinoma. N Engl J Med
1991;325:1127-31.
7. Delchier JC, Ebert M, Malfertheiner P. Helicobacter pylori in gastric lymphoma
8. Jones NL, Sherman PM. Helicobacter pylori infection in children. Curr Opin
Pediatr 1998;10:19-23.
9. MacArthur C, Saunders N, Feldman W. Helicobacter pylori, gastroduodenal
diseases and recurrent abdominal pain in children. JAMA 1995;273:729-34.
10. Blaser MJ, Chyou PH, Nomura A. Age at establishment of Helicobacter pylori
infection and gastric carcinoma, gastric ulcer and duodenal ulcer risk. Cancer Res
1995;55:562-5.
11. Vandenplas Y, Blecker U, Devreker T, Keppens E, Nijs J, Cadranel S.
Contribution of the 13C-urea breath test to the detection of Helicobacter pylori
gastritis in children. Pediatrics 1992;90:608-11.
12. CutlerAF, Havstad S, Ma CK, Blaser MJ, Perez-Perez GI, Schubert TT.
Accuracy of invasive and noninvasive tests to diagnose Helicobacter pylori
infection. Gastroenterology 1995;109:136-41.
13. Thijs JC, van Zwet AA, Thijs WJ, Oey HB, Karrenbeld A, Stellaard F, et al.
Diagnostic tests for Helicobacter pylori: A prospective evaluation of their accuracy,
without selecting a single test as the gold standard. Am J Gastroenterol
1996;91:2125-9.
14. Andersen LP, Pedersen KG, Thoreson AC, Jørgensen F, Rath J, Larsen NE, et al.
Scand J Gastroenterol 1998;33:24-30.
15. Makristathis A, Pasching E, Schtze K, Wimmer M, Rotter ML, Hirschl AM.
Detection of Helicobacter pylori in stool specimens by PCR and antigen enzyme
immunoassay. J Clin Microbiol 1998;36:2772-4.
16. Mendoza ML, Martin-Rabadan P, Carrion I, Morillas JD, Lopez-Alonso G,
Diaz-Rubio M. Helicobacter pylori infection: Rapid diagnosis with brush cytology. Acta
Cytol 1993;37:181-5.
17. Bamford KB, Lutton SA, O’Loughlin B, Coulter WA, Collins JS. Nested primers improve sensitivity in the detection of Helicobacter pylori by the polymerase chain
reaction. J Infect 1998;36:105-10.
18. Yang JC, Wang TH, Wang HJ, Kuo CH, Wang JT, Wang WC. Genetic analysis of the cytotoxin-associated gene and the vacuolating toxin gene in Helicobacter
pylori strains isolated from Taiwanese patients. Am J Gastroenterol
1997;92:1316-21.
19. Taniguchi Y, Kimura K, Sohara H, Shirasaki A, Kawada H, Satoh K, et al.
Simple 13
C-urea breath test with infra-red spectrophotometer. J Gastroenterol
1996;31(suppl 9): 37-40..
20. Ohara H, Suzuki T, Nakagawa T, Yoneshima M, Yamamoto M, Tsujino D, et al. 13
and for monitoring the effects of lansoprazole. J Clin Gastroenterol 1995;20 (supple
2): S115-7.
21. Ohara S, Kato M, Asaka M, Toyota T. The UBiT-100 13
CO2 infrared analyzer:
comparison between infrared spectrometric analysis and mass spectrometric
analysis. Helicobacter 1998;3:49-53.
22. Lin JT, Wang JT, Wu MS, Huang TS, How SW, Wang HP, et al. Serological,
histological, and polymerase chain reaction studies of Helicobacter pylori infection
in patients with gastric adenocarcinoma. J Formos Med Assoc 1994;93:15-9.
23. Chang MC, Wu MS, Wang HH, Wang HP, Lin JT. Helicobacter pylori stool
antigen (HpSA) test – A simple, accurate and noninvasive test for detection of
Helicobacter pylori infection. Hepato-Gastroenterology 1999;46:299-302.
24. Bourke B, Jones NL, Sherman PM. Helicobacter pylori infection and peptic
ulcer disease in children. Pediatr Infect Dis J 1996;15:1-13.
25. Vaira D, Malfertheiner P, Mégraud F, Axon ATR, Deltenre M, Hirschi AM, et al.
Diagnosis of Helicobacter pylori infection with a new non-invasive antigen-based
assay. Lancet 1999;354:30-33.
26. Koletzko S, Haissch M, Seeboth I, Braden B, Hengels K, Koletzko B.
Isotope-selective nondispersive infrared spectrometry for detection of Helicobacter pylori
infection with 13
27. Rowland M, Lambert I, Gormally S, Daly LE, Thomas JE, Hetherington C, et al.
Carbon 13-labeled urea breath test for the diagnosis of Helicobacter pylori
infection in children. J Pediatr 1997;131:815-20.
28. Glupczynski Y. Microbiological and serological diagnostic tests for Helicobacter
pylori: an overview. Br Med Bull 1998;54:175-86.
29. Khanna B, Cutler A, Israel NR, Perry M, Lastovica A, Fields P, et al. Use
Caution with serologic testing for Helicobacter pylori in children. J Infect Dis
1998;178:460-5.
30. Thomas JE, Dale A, Harding M, Coward A, Cole TJ, Weaver LT. Helicobacter
pylori colonization in early life. Pediatr Res 1999;45:218-23.
31. Casswall TH, Nilsson HO, Bergstrom M, Aleljung P, Wadstrom T, Dahlstrom
AK, et al. Evaluation of serology, 13
C-urea breath test and polymerase chain
reaction of stool samples to detect Helicobacter pylori in Bangladeshi chldren. J
Pediatr Gastroenterol Nutr 1999;28:31-6.
32. Perri F, Pastore M, Clemente R, Festa V, Quitadamo M, Niro G, et al.
Helicobacter pylori infection may undergo spontaneous eradication in children: A
2-year follow-up study. J Pediatr Gastroenterol Nutr 1998;27:181-3.
33. Kumagai T, Malaty HM, Graham DY, Hosogaya S, Misawa K, Furihata K, et al.
8-year birth cohort study. J Infect Dis 1998;178:717-21.
34. Sherman PM, Hunt RH. Why guidelines are required for the treatment of
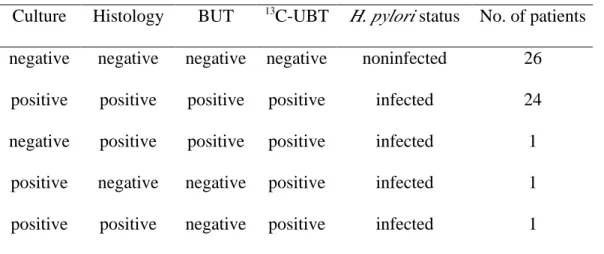
Table 1. Concordance of diagnosis of H. pylori infection in 43 children by four diagnostic tests as gold standard*
Culture Histology BUT 13C-UBT H. pylori status No. of patients negative negative negative negative noninfected 26
positive positive positive positive infected 24 negative positive positive positive infected 1
positive negative negative positive infected 1 positive positive negative positive infected 1
gold standard: either culture is positive or concordance positive with at least two of
the other three tests (Histology, BUT, and 13
C-UBT).
BUT: biopsy urease test 13
C-UBT: 13
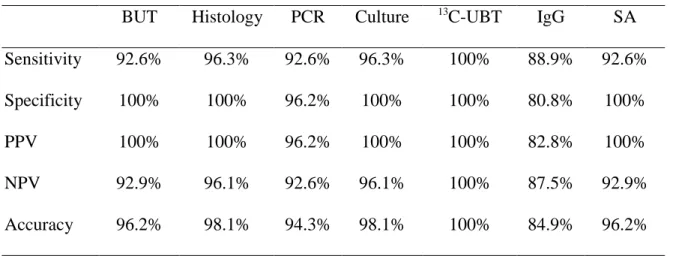
Table 2. Sensitivity, specificity, and diagnostic accuracy of seven diagnostic tests for H. pylori infection in children
BUT Histology PCR Culture 13C-UBT IgG SA Sensitivity 92.6% 96.3% 92.6% 96.3% 100% 88.9% 92.6% Specificity 100% 100% 96.2% 100% 100% 80.8% 100%
PPV 100% 100% 96.2% 100% 100% 82.8% 100%
NPV 92.9% 96.1% 92.6% 96.1% 100% 87.5% 92.9%
Accuracy 96.2% 98.1% 94.3% 98.1% 100% 84.9% 96.2%
PPV: positive predictive value, NPV: negative predictive value
BUT: biopsy urease test by CLO test
PCR: polymerase chain reaction 13
C-UBT: urea breath test by infrared spectrometer
IgG: serum IgG antibody to H. pylori