Epidermal Growth Factor Receptor Genetic Polymorphisms Linked with
Rheumatoid Arthritis in Taiwan’s Han Chinese population.
Sui-Foon Lo,1,6 Lei Wan,2,7 Hsiu-Chen Lin,3 Chung-Ming Huang,4,8 Shih-Yin Chen,2,7 Su-Ching Liu2 and Fuu-Jen Tsai,2,5,7,9
1Department of Physical Medicine and Rehabilitation, 2Department of Medical Genetics; 4Division of Immunology and Rheumatology, Department of Internal Medicine; 5Department of Pediatrics; China Medical University Hospital. 3Department of Physical therapy; 6School of Chinese Medicine, 7Graduate Institute of Chinese Medical Science, 8 Graduate Institute of Integrated Medicine; China Medical University,Taichung,Taiwan. 9Department of Biotechnology, Asia University, Taichung, Taiwan.
Address correspondence to: Fuu-Jen Tsai,
Department of Medical Research, China Medical University Hospital, No 2, Yuh Der Road, Taichung, Taiwan
TEL: 886-4-22052121 ext 2041 Fax: 886-4-22033295
E-mail: [email protected]
Background: The involvement of the epidermal growth factor receptor (EGFR) in the
pathogenesis of cancer is well documented. In contrast, its role in rheumatoid arthritis (RA) development is not that well defined although previous studies suggested the possible link between autoimmune diseases and malignancy. Therefore, we aimed to examine if there is link between the EGFR genetic polymorphisms and RA.
Methods: Our study gauged effects of EGFR (rs11543848 and rs17337023) single
nucleotide polymorphisms (SNPs) on RA among Taiwan’s Han Chinese population. Polymorphism of EGFR gene was analyzed in 128 controls and 188 MGN patients. Genotyping for EGFR SNPs was performed by restriction fragment length polymorphism (RFLP) assay.
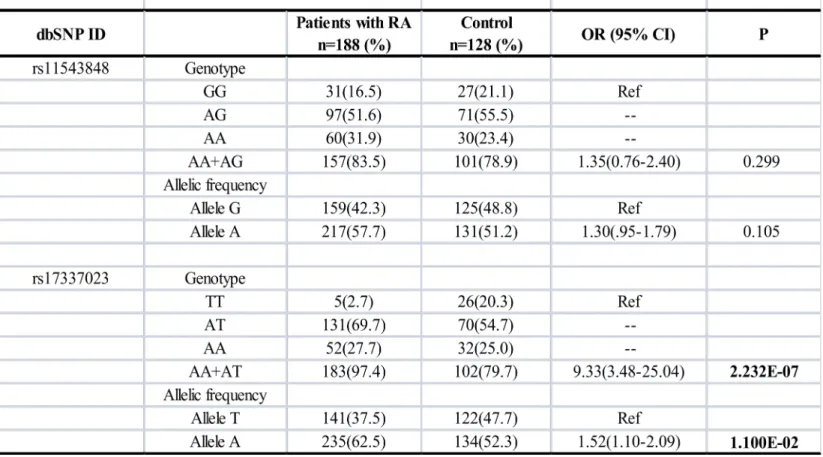
Results: Data confirmed statistically significant difference in genotype frequency
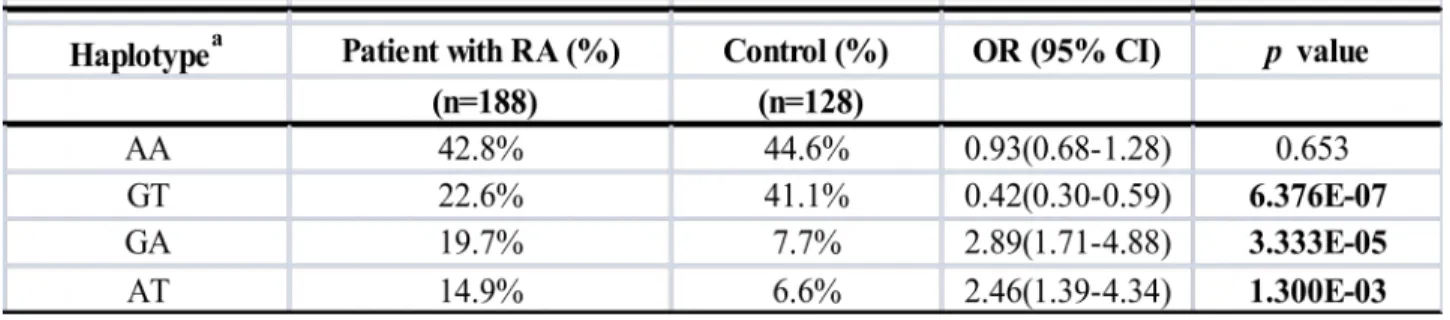
distributions at rs17337023 SNP between RA patients and controls (p=2.232E-07), plus A allele at rs17337023 SNP as a high risk factor in developing RA (odds ratio [OR] = 1.52; 95% confidence interval [CI] = 1.10-2.09). Also, from comparison of haplotype frequencies between case and control, RA patients with GA or AT haplotype appeared more “at-risk” for RA progression (p=3.333E-05 and 1.3E-03, respectively).
Conclusion: Data yield new information on EGFR polymorphisms (rs11543848 and
polymorphism revealed by this study merit further investigation.
Keywords: Rheumatoid Arthritis (RA); epidermal growth factor receptor (EGFR);
Single nucleotide polymorphisms (SNPs); Haplotypes.
Running Title:
EGFR polymorphisms and Rheumatoid Arthritis
Introduction:
Rheumatoid arthritis (RA) is a chronic autoimmune inflammatory disease characterized by immune activation and hyperplasia of the synovium leading to progressive destruction of the affected joints. Activated synovial fibroblasts recruit inflammatory cells and cause granulomatous tissues (pannuses) formation and angiogenesis in the synovial membrane of the RA patients (1). These activated synoviocytes demonstrate the invasive behavior of metastatic malignant cells and show resistance to apoptosis (2,3). Similar to transformed cells, the rheumatoid fibroblasts have augmented tyrosine-phosphorylated proteins and manifest tumor-like behavior. Several cytokines that activate these fibroblasts mediate their action through tyrosine kinase growth factor receptors. Mechanisms of signal transduction via such tyrosine kinases are important in the development of rheumatoid lesions (4-6). Of the
receptor tyrosine kinases, the epidermal growth factor (EGF) /epidermal growth factor receptor (EGFR) families play a crucial role in the development, physiology, and cancer (7). Epidermal growth factor has been found as an important factor that stimulates the release of inflammatory mediators and enhances the growth of synovial cells (8). Among the members of the EGF family, amphiregulin and transforming growth factor–alpha (TGF-), which are the main ligands for EGFR, have been found to have increased expression in the synovial tissues of RA patients (9,10). In addition, EGFR has been found to be the predominantly expressed receptors in synovial fibroblasts (9). The EGFR is encoded by a gene located in the short arm of chromosome 7 (7p12.1-12.3) (11). The EGFR 2133A/T polymorphism (rs17337023) has been shown to have an association with malignant oral keratinocytes (12), systemic lupus erythematosus (SLE) (13), endometriosis, and leiomyomas (14) in previous studies. Another polymorphism, the EGFR 1808G/A polymorphism (rs11543848) was found to be associated with acute coronary syndrome (15), the prognosis of colorectal carcinoma (16), and advanced lung cancer (17). In view of the tumor-like behavior of synovial fibroblasts and chronic inflammatory process in rheumatoid arthritis, we hypothesized that the EGFR gene polymorphism may be associated with the risk of rheumatoid arthritis development. To verify our hypothesis, we compared the genotypic and allelic frequencies of the EGFR
polymorphisms (rs11543848 and rs17337023) between RA patients and normal control participants living in Taiwan. Furthermore, we compared the genotypes among RA patients with various clinical variables to find out if there is a relationship between EGFR polymorphisms and the clinical manifestation of RA.
Materials and Methods: Patient selection
The study subjects included 192 RA patients and 192 healthy subjects, recruited from China Medical University Hospital in Taiwan. Patients with RA according to the revised America College of Rheumatology criteria(18) were enrolled. Nephelometry detected rheumatoid factor (RF), values 30 IU/ml defined as positive. Presence or≧ history of extra-articular manifestations in patients RA was recorded (19). The healthy controls from the general population were selected by health examination. All blood samples were collected by venipuncture for genomic DNA isolation, with informed consent obtained from participants and approved by the local Ethics Committee.
Polymerase chain reaction
Polymerase chain reaction (PCR) was used to identify the EGFR polymorphisms including rs11543848 and rs17337023. Polymerase chain reaction was carried out in a total volume of 50 μL, containing genomic DNA 50ng, 2–6 pmol of each primer, 1X Taq polymerase buffer (1.5mM MgCl2) and 0.5 units of AmpliTaq DNA polymerase (Perkin
Elmer; Foster City,CA,USA). In the study of the EGFR rs17337023 SNP, the primers used were upstream ATATATGCCAAAGAAGTAG-3' and downstream 5'-TGATCAGGACAGAGGACAG-3'. For the EGFR 1808 G/A polymorphism (rs11543848), the primers used were upstream 5'-TGCTGTGACCCACTCTGTCT-3' and downstream 5’-CCAGAAGGTTGCACTT- GTCC-3'. Polymerase chain reaction amplification was performed in a programmable PCR thermal cycler (GeneAmp PCR System 2400, Perkin Elmer). The PCR cycling conditions for EGFR rs17337023 SNP examination were as follows: one cycle at 95°C for 5 min ,35 cycles at 95 °C for 30 seconds, 56 °C for 30 seconds, 72 °C for 45 seconds. One final cycle of extension at 72°C for 7 min, then holding at 25°C. The EGFR rs17337023 SNP was analyzedby PCR amplification followed by restriction enzyme analysis with BsrI. Two fragments of 136 bp and 64 bp were present if the product was excised (TT homozygote). The uncut band showed up as a 200 bp length on the gel. The reaction was then incubated for overnight at 65°C, and then 10μl of the products were loaded into a 3% agarose gel containing ethidium bromide for electrophoresis. The EGFR rs17337023 SNP was categorized as excisable (TT homozygote), non-excisable (AA homozygote), and (AT heterozygote). The PCR cycling conditions for EGFR rs11543848 SNP examination were as follows: one cycle at 95°C for 5 min ,35 cycles at 95 °C for 30 seconds,59 °C for 30 seconds, 72 °C for 45 seconds. One final cycle of extension at 72°C for 7 min, then holding at 25°C.
The EGFR rs11543848 SNP was analyzedby PCR amplification followed by restriction enzyme analysis with BstNI. Three fragments of 67 bp ,50bp and 38 bp were present if the product was excised(GG homozygote). The uncut band showed up as two fragments of 117bp and 38 bp length on the gel. The reaction was then incubated for overnight at 60°C, and then 10μl of the products were loaded into a 3% agarose gel containing ethidium bromide for electrophoresis. The EGFR rs11543848 SNP was categorized as excisable (GG homozygote), non-excisable (AA homozygote), and (AG heterozygote).
Statistical analysis
The genotypic and allelic frequencies of EGFR SNPs (rs17337023 and rs11543848) for the RA patients and controls were compared using the chi-square test. Among the RA patients, genotype groups with different clinical variables were also compared using chi-square test. When one cell had an expected count of <1 or >20% of the cells had an expected count of <5, Fisher’s exact test was used. Results were considered statistically significant when p values less than 0.05.The odds ratios (OR) were calculated from the genotypic frequency and allelic frequency with a 95% confidence interval (95% CI) for the EGFR SNPs (rs17337023 and rs11543848). The statistical analysis was performed by using the SPSS version 11.
Results:
Genotype distributions were in Hardy-Weinberg equilibrium. We observed A allele as the major one at rs11543848 polymorphism, both in RA patients (57.7%; 217/376) and controls (51.2%; 131/256), A allele as the major one at rs17337023 polymorphism in patients (62.5%; 235/376) and controls (52.3%; 134/256). Comparison of allele and genotype distribution yielded significant differences for the rs17337023 SNP in RA patients and controls (p=1.1E-02 and 2.232E-07, respectively). Data indicated individuals with A allele or A carrier (AA + AT) genotype at rs17337023 SNP at higher risk for RA.
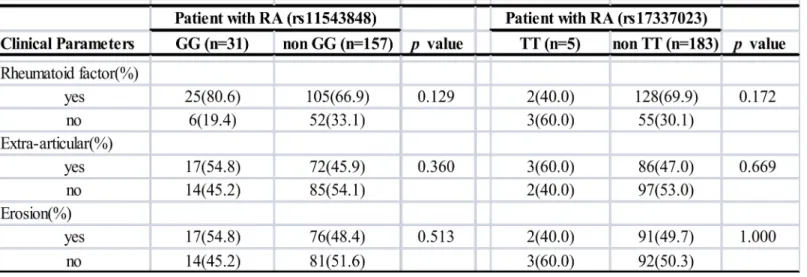
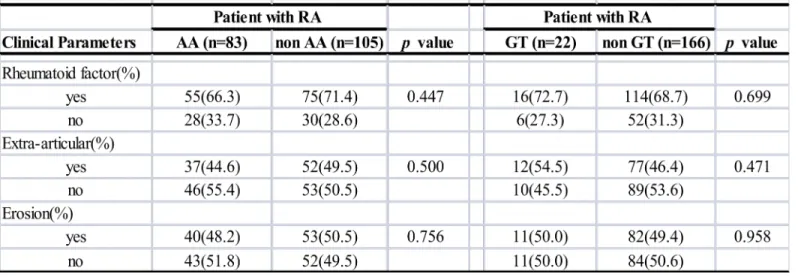
Haplotype frequencies were estimated via rs11543848 and rs17337023 SNPs. Four haplotypes EGFR emerged in the study population: AA is the most common both in RA patients (42.8%) and healthy controls (44.6%). When we compared the overall distribution of haplotype frequencies between RA patients and health controls, significant differences were observed in Table 2. Our data showed that individuals with GT haplotype appeared to be a significant “protective” haplotype compared with other haplotypes (OR: 0.42, 95% CI: 0.3-0.59; p=6.376E-07). Also, individuals with GA or AT haplotype appeared to be a significant “at-risk” haplotype for RA development (p = 3.333E-05 and 1.3E-03, respectively). In addition, comparisons of the clinical features of RA patients with the different genotypes and haplotypes were shown in Table 3 and 4. However, there were no significant differences results in
rheumatoid factor accompaniment, incidence of extra-articular and bone erosion occurrence.
Discussion:
Epidermal growth factor receptor (EGFR) is a trans-membrane receptor with a molecular weight of approximately 170 kDa encoded by the c-erbB1 proto-oncogene (20-22). It belongs to a family of four closely related receptor tyrosine kinases which has been recognized as a convergence and switch point for diverse signal transduction pathways involved in cellular communication (23,24). The biological responses to the EGFR signal transductions are pleiotrophic including mitogenesis, protein secretion, enhanced cell motility, proliferation, invasion, cell adhesion, and angiogenesis (21,25). Many studies have shown enough evidence supporting the role of EGFR activation and signaling in the pathogenesis of malignancies. Meanwhile, numerous reports have suggested a link between rheumatic diseases, autoimmune phenomena, and cancer (26). Increased risk of certain cancers, particularly hematologic cancers, has been found in RA and SLE patients compared with the general population, (26-28). Autoantibodies to EGFR in systemic lupus erythematosis, systemic sclerosis, and autoimmune mice also have been found (29), further suggesting the possible link between autoimmune disease and tumor immunology in relation to EGFR. Therefore, it is possible that EGFR gene
polymorphism is associated with the risk of RA development. Our results in the study of the EGFR rs17337023 SNP support this hypothesis (Table1). When compared with the controls, RA patients were found to have significantly higher frequencies of the A allele. These results suggested that individuals with A allele or A carrier (AA + AT) genotype at rs17337023 SNP at higher risk for RA. Although the study of rs11543848 SNP showed no such risk association (Table 1), the risk association of the rs17337023 SNP in autoimmune diseases was further supported by previous studies of our group in identifying the association of rs17337023 SNP with SLE (13). However, we found that the EGFR polymorphisms have no association with clinical severity in RA given that no significant difference was noted in comparing the genotype groups according to different clinical variables, which is similar to our previous findings in SLE (13). Although the exact pathogenic mechanism relating these polymorphisms to these chronic inflammatory diseases still remain unknown, the extremely complex signaling network could be regulated at essentially every step, especially considering that the EGFR signal transduction system is not a direct linear pathway from the cell surface to the nucleus. In addition, the rs17337023 SNP could be in linkage disequilibrium with other polymorphisms, leading to disease development in RA and SLE patients. Therefore, further studies are required to explore if rs17337023 SNP is an independent risk factor or an indirect marker of different genetic factors in RA development. In
conclusion, our present study is the first to identify that the EGFR 2133T/A polymorphism is associated with the risk of RA development irrespective of the latter’s clinical severity.
References:
1. Firestein G. Etiology and pathogenesis of rheumatoid arthritis. In: Harris ED, Budd RC, Firestein GS, et al editors. Kelley’s textbook of rheumatology, 7th edition. Philadelphia: Elsevier/Saunders company; 2005:996-1042.
2. Asahara H, Hasumuna T, Kobata T, Yagita H, Okumura K, Inoue H, Gay S, Sumida T, Nishioka K. Expression of Fas antigen and Fas ligand in the rheumatoid synovial tissue.Clin Immuno Immunopathol 1996;81:27-34.
3. Baier A, Meineckel I, Gay S, Pap T. Apoptosis in rheumatoid arthritis. Curr Opin Rheumatol 2003;15:274-9
4. Williams WV, VonFeldt JM, Ramanujam T, Weiner DB. Tyrosine kinase signal transduction in rheumatoid synovitis. Semin Arthritis Rheum 1992;21:317–29. 5. Migita K, Eguchi K, Tsukada T, Kawabe Y, Aoyagi T, Nagataki S. The role of
protein kinase in human synovial fibroblast growth. Biochem Biophys Res Commun 1995;210:1066–75.
6. Takeuchi T, Abe T. Tyrosine phosphorylated proteins in synovial cells of rheumatoid arthritis. Intl Rev Immunol 1998;17:365–81.
7. Wieduwilt MJ, Moasser MM. The epidermal growth factor receptor family: Biology driving targeted therapeutics. Cell Mol Life Sci 2008 May;65:1566-84.
8.Goddard DH, Grossman SL, Newton R. Polypeptide growth factors augment interleukin 1-induced release of prostaglandin E2 by rheumatoid arthritis synovial cells in vitro. Cytokine 1990; 2: 294–9.
9. Yamane S, Ishida S, Hanamoto Y, et al. Proinflammatory role of amphiregulin,an epidermal growth factor family member whose expression is augmented in rheumatoid arthritis patients. J Inflamm (Lond). 2008;27:5:5.
10. Hallbeck AL, Walz TM, Briheim K, Wasteson A. TGF- and ErB2 production in synovial joint tissue: increased expression in arthritic joints. Scand J Rheumatol 2005;34:204-11
11. Haley J, Whittle N, Bennet P, et al. The human EGF receptor gene: structure of the 110 kb locus and identification of sequences regulating its transcription. Oncogene Res 1987; 1:375-96.
12. Shintani S, Matsuo K, Crohin CC, et al. Intragenic mutation analysis of the human epidermal growth factor receptor (EGFR) gene in malignant human oral
keratinocytes. Cancer Res 1999;59: 4142–7.
13.Huang CM, Tsai CH, Chen CL, Chang CP, Lai CC, Tsai FJ. Epidermal growth factor receptor (EGFR) gene Bsr I polymorphism is associated with systemic lupus erythematosus. Lupus 2004;13:773-6.
14.Hsieh YY, Chang CC, Tsai FJ, Lin CC, Tsai CH. T homozygote and allele of epidermal growth factor receptor 2073 gene polymorphism are associated with higher susceptibility to endometriosis and leiomyomas. Fertil Steril. 2005;83:796-9. 15.Gao LB, Zhou B, Zhang L et al. R497K polymorphism in epidermal growth factor
receptor gene is associated with the risk of acute coronary syndrome BMC Med Genet. 2008;9:74
16. Wang WS, Chen PM, Chiou TJ, et al. Epidermal growth factor receptor R497K polymorphism is a favorable prognostic factor for patients with colorectal carcinoma.Clin Cancer Res 2007;13:3597-604.
17.Sasaki H, Okuda K, Shimizu S, et al. EGFR R497K polymorphism is a favorable prognostic factor for advanced lung cancer.J Cancer Res Clin Oncol 2009 135:313-8. 18.Arnett FC, Edworthy SM, Bloch DA, et al. The American Rheumatism
Association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis Rheum 1988;31:315-24.
19.Yen JH, Chen JR, Tsai WJ, Tsai JJ, Liu HW. HLA-DRB1 genotyping in patients with rheumatoid arthritis in Taiwan. J Rheumatol 1995;22:1450-4.
20. Ullrich A, Coussens L, Hayflick JS, et al. Human pidermal growth factor receptor cDNA sequence and aberrant expression of the amplified gene in A431 epidermoid carcinoma cells. Nature 1984 ;309:418-25.
22.Yarden Y. The EGFR family and its ligands in human cancer. signalling mechanisms and therapeutic opportunities. Eur J Cancer.2001; 37 Suppl 4:S3-8. 23. Hackel PO, Zwick E, Prenzel N, Ullrich A. Epidermal growth factor receptors:
critical mediators of multiple receptor pathways. Curr Opin Cell Biol. 1999; 11:184-9.
24. Moghal N, Sternberg PW. Multiple positive and negative regulators of signaling by the EGF-receptor.Curr Opin Cell Biol. 1999 Apr;11(2):190-6.
25. Lafky JM, Wilken JA, Baron AT, Maihle NJ. Clinical implications of the ErbB/epidermal growth factor (EGF) receptor family and its ligands in ovarian cancer. Biochim Biophys Acta 2008;1785:232-65.
26.Chakravarty EF, Genovese MC. Musculoskeletal syndromes in malignancy. In Harris ED, Budd RC, Firestein GS, et al editors. Kelley's textbook of rheumatology, 7th ed. Philadelphia: Elsevier/Saunders company;2005:1754-72. 27. Smitten AL, Simon TA, Hochberg MC, Suissa S. A meta-analysis of the incidence
of malignancy in adult patients with rheumatoid arthritis. Arthritis Res Ther. 2008;10:R45.
28. Bernatsky S, Boivin JF, Joseph L, et al. An international cohort study of cancer in systemic lupus erythematosus. Arthritis Rheum 2005;52:1481-90
29.Planque S, Zhou YX, Nishiyama Y, et al. Auto antibodies to the epidermal growth factor receptor in systemic sclerosis,lupus, and autoimmune mice. FASEB J. 2003 ;17:136-43.
Table 1. Genotypic and allelic frequencies of EGFR genetic polymorphisms in the patients with RA and controls.
Table 2. Distribution of EGFR haplotype frequencies in the patients with RA and controls.
CI, confidence interval; OR, odds ratio.