1
Cutaneous analgesia and systemic toxicity of carbetapentane
and caramiphen in rats
Ching-Hsia Hunga , Ph.D., Chin-Chen Chub, M.D., Ph.D., Yu-Chung Chenc, M.S., Kuo-Sheng Liud, Ph.D., Yu-Wen Chenb,e,*, Ph.D., Jhi-Joung Wangb, M.D., Ph.D.
a
Institute & Department of Physical Therapy, National Cheng Kung University, Tainan, Taiwan;
b
Department of Medical Research, Chi-Mei Medical Center, Tainan, Taiwan; c
Division of Physical Therapy, Department of Physical Medicine and Rehabilitation, Cheng Hsin General Hospital, Taipei, Taiwan;
d
Graduate Institute of Pharmaceutical Science, Chia Nan University of Pharmacy & Science, Tainan, Taiwan;
e
Department of Physical Therapy, China Medical University, Taichung, Taiwan
1. Ching-Hsia Hung, Ph.D. Title: Associate Professor
Affiliation: National Cheng Kung University Email: [email protected]
Role: This author helped design the study, conduct the study, and analyze the data
Conflicts: Ching-Hsia Hung reported no conflicts of interest
Attestation: Ching-Hsia Hung has seen the original study data, reviewed the analysis of the data, approved the final manuscript, and is the author responsible for archiving the study files
2. Chin-Chen Chu, M.D., Ph.D. Title: Assistant Professor
Affiliation: Chi-Mei Medical Center Email: [email protected]
Role: This author helped conduct the study and analyze the data Conflicts: Chin-Chen Chu reported no conflicts of interest
Attestation: Chin-Chen Chu has seen the study data, reviewed the analysis of the data, approved the final manuscript, and is the author responsible for
archiving the study files
3. Yu-Chung Chen, M.S. Title: P.T.
Affiliation: Cheng Hsin General Hospital Email: [email protected]
Role: This author helped design the study, conduct the study, and analyze the data
Conflicts: Yu-Chung Chen reported no conflicts of interest
Attestation: Yu-Chung Chen has seen the original study data, reviewed the analysis of the data, approved the final manuscript, and is the author responsible for archiving the study files
4. Kuo-Sheng Liu, Ph.D. Title: Assistant Professor
Affiliation: Chia Nan University of Pharmacy & Science Email: [email protected]
Role: This author helped conduct the study and analyze the data Conflicts: Kuo-Sheng Liu reported no conflicts of interest
Attestation: Kuo-Sheng Liu has seen the original study data, reviewed the analysis of the data, approved the final manuscript, and is the author responsible for archiving the study files
5. Yu-Wen Chen, Ph.D. Title: Associate Professor
Affiliation: China Medical University (current affiliation: Chi-Mei Medical Center)
Email: [email protected]
Role: This author helped design the study, conduct the study, analyze the data, and write the manuscript
Conflicts: Yu-Wen Chen reported no conflicts of interest
Attestation: Yu-Wen Chen has seen the original study data, reviewed the analysis of the data, approved the final manuscript, and is the author responsible for archiving the study files
6. Jhi Joung Wang, M.D., Ph.D. Title: Professor
Email: [email protected]
Role: This author helped conduct the study and analyze the data Conflicts: Jhi Joung Wang reported no conflicts of interest
Attestation: Jhi Joung Wang has seen the original study data, reviewed the analysis of the data, approved the final manuscript, and is the author responsible for archiving the study files
Institution: This work was done in National Cheng Kung University, Tainan, Taiwan.
Running Header (< 45 characters): Cutaneous analgesia and systemic toxicity of drugs
Funding: The financial support provided for this study by the National Science Council (NSC 99-2314-B-039-013-MY3; NSC 100-2314-B-039 -017-MY3) of Taiwan.
* Address correspondence and reprint requests to: Yu-Wen Chen, PhD, Department of Physical Therapy, China Medical University, No.91 Hsueh-Shih Road, Taichung 40402, Taiwan
Tel: 886-4-22053366 ext 7327
Fax: 886-4-22065051
ABSTRACT
Background: Although caramiphen produces spinal anesthesia, caramiphen and
carbetapentane have never been tested as infiltrative cutaneous analgesia. The aim of
this study was to compare cutaneous analgesia of caramiphen and carbetapentane with
bupivacaine and evaluated their central nervous system (CNS) and cardiovascular
(CV) toxicity.
Methods: After the blockade of cutaneous trunci muscle reflex with subcutaneous
drug injections in rats, we evaluated the local anesthetic effect of carbetapentane and
caramiphen on infiltrative cutaneous analgesia. Following continuous intravenous
infusion of equipotent doses of bupivacaine, carbetapentane, caramiphen, and saline,
we observed mean arterial blood pressure (MAP) and heart rate (HR) and monitored
the onset time of seizure, apnea, and impending death.
Results: Carbetapentane and caramiphen acted like bupivacaine and elicited
cutaneous analgesia in a dose-related fashion. On a 50% effective dose (ED50) basis,
the ranks of potencies were bupivacaine (1.78 [1.52 – 2.07]) > carbetapentane (2.53
[2.38 – 2.77]) > caramiphen (3.60 [3.41 – 3.99]) (P < 0.01). At equianalgesic doses
(ED25, ED50, ED75), the duration caused by carbetapentane or caramiphen was similar
to that caused by bupivacaine. Under equipotent doses, the infusion time of
was longer than that of bupivacaine (P < 0.05). The decline in MAP and HR was
slower with carbetapentane or caramiphen when compared with bupivacaine (P <
0.01 for the differences) at equipotent doses.
Conclusions: Carbetapentane and caramiphen were similar to bupivacaine at
producing durations of cutaneous analgesia but were less likely than bupivacaine to
induce CNS and CV toxicity.
Key words: Carbetapentane, Caramiphen, Bupivacaine, Infiltrative cutaneous
INTRODUCTION
Carbetapentane, a non-opioid antitussive agent, has been known to have
atropine-like and effectively suppresses acute cough due to common upper respiratory
infections.1 Another known non-opioid antitussive, caramiphen, was first introduced
into the therapy for diseases of the basal ganglia 2 and was available as an antitussive
agent in Europe since 1950.3 Recently, it has been shown that the antagonism of
N-Methyl-D-aspartate receptor activation and the facilitation of GABAA receptor
activation by caramiphen in the basolateral amygdale may play an important role in
the anticonvulsive and neuroprotective properties of caramiphen. 4 In addition,
caramiphen has been shown to have a local anesthetic effect on spinal anesthesia in
rats.5
The injections of local anesthetics are used for infiltration anesthesia of skin
incision sites for laparoscopic surgery 6 and to provide postoperative pain relief after
vaginal hysterectomy and inguinal hernia repair.7 However, the technique is limited
by the short duration of analgesia or anesthesia.8 For this reason, bupivacaine is
chosen for infiltration anesthesia because of its longer duration of effective analgesia.9
Recently, we showed that the long duration caused by caramiphen 5 was similar to
that caused by bupivacaine 10 on spinal anesthesia in rats. Furthermore,
chemical structures. However, cutaneous analgesia following subcutaneous injection
of carbetapentane and caramiphen has not been evaluated.
The local anesthetics, despite physical or chemical differences, all have central
nervous system (CNS) toxicity and cardiovascular (CV) toxicity.10-13 Although some
of them may have less toxicity to the CNS or CV system, however, the differences are
minor. This may be explained due to their similar chemical structures.11 Before
carbetapentane and caramiphen are applied in clinical practice, the toxicity of these
drugs should be tested. There are no studies evaluating the systemic toxicity of
carbetapentane and caramiphen; it is known that bupivacaine induces significant CV
toxicity.14,15 In this study, we compared cutaneous analgesia of carbetapentane and
caramiphen with that of bupivacaine. Furthermore, we also evaluated the systemic
MATERIALS AND METHODS
Animals
Male Sprague-Dawley rats weighting 240-290g were obtained from the National
Laboratory Animal Centre (Taipei, Taiwan), and then were housed in groups of three,
with food and water freely available until the time of the study. The room temperature
was controlled at 22℃ with approximately 50% humidity and a 12-h light/dark cycle (6:00 a.m. – 6:00 p.m.). The experimental procedures were approved by the
Institutional Animal Care and Use Committee of China Medical University, Taichung,
Taiwan and conformed to the recommendations and policies of the International
Association for the Study of Pain (IASP).
Drugs
Carbetapentane citrate salt and bupivacaine HCl were purchased from
Sigma-Aldrich Chemical Co. (St. Louis, MO, USA). Caramiphen edisylate was
purchased from Rarechemical Co. (R288810, USA). All drugs were freshly solved in
saline (0.9%NaCl) before the subcutaneous injections or intravenous infusion.
Experimental protocols
The protocol was divided into two parts. In Part I, the cutaneous analgesic effect
of different doses of bupivacaine (7.0, 4.0, 2.7, 2.0, 1.6, 1.3, 0.8 μmol · kg-1),
13.3, 8.0, 5.3, 2.7, 2.0, 1.3 μmol · kg-1) was performed (n = 8 rats for each dose of
each drug). According to the dose-response curves, bupivacaine at 8.0 μmol · kg-1,
carbetapentane at 11.4 μmol · kg-1, and caramiphen at 16.0 μmol · kg-1 also tested to
determine the equivalent potencies of these drugs; meanwhile, the full recovery time
(duration) of carbetapentane, caramiphen, and bupivacaine was evaluated at
equianalgesic doses (ED25, ED50, ED75) (n = 8 for each dose of each drug). In Part II,
time to cause toxicity (seizures, apnea, and cardiac arrest), mean arterial blood
pressure (MAP), and heart rate (HR) were evaluated after equipotent doses of the
drugs (bupivacaine, carbetapentane, and caramiphen) were infused into the rat (n = 8
rats for each dose of each drug). Saline group (n = 8 rats) was used as a control.
Part I - Infiltrative cutaneous analgesia
Subcutaneous injection and neurobehavioral examinations
A trained examiner who was blinded to the experimental groups was responsible
for handling of animals and behavioral examinations. Infiltrative cutaneous analgesia
was evaluated by the cutaneous trunci muscle reflex (CTMR), characterized by the
reflex movement of the skin over the back elicited by twitches of the lateral
thoracospinal muscle in response to local dorsal cutaneous stimulation after drug
injections.16 In brief, the hair on the rats' dorsal surface of the thoracolumbar region (6
then each drug solved in 0.6 ml saline was injected subcutaneously using a 30-gauge
needle into a naïve area of the shaved back of the un-anesthetized rats.17,18 The wheal
within 2 cm diameter was marked with ink within 1 min after subcutaneous injection.
The cut end of an 18-gauge needle (a fresh regular bevel needle) was affixed to a von
Frey filament (no. 15; Somedic Sales AB, Stockholm, Sweden) to produce a
standardized noxious punctate mechanical stimulus (191 g) without making tissue damage.
After observing a rat’s normal reaction to stimuli applied outside the wheal and
on the contralateral side, we applied 6 stimuli at 6 different points within each wheal,
with a frequency of 0.5 to 1 Hz, and scored the number to which the rat failed to react.
The magnitude of cutaneous analgesia was described as the percent of possible effect
(% PE). For example, the absence of any response after 6 stimuli was defined as
complete nociceptive block (100% PE), which was calculated as follows:
% PE = (number of stimuli that provoked no response/6) 100%
During the drug action, the maximum value of % PE was presented as percent of
maximal possible effect (% MPE). Each duration (full recovery time) of drug action
was defined as the time from drug injection (i.e., time=0) to full recovery of CTMR
(no analgesic effect or 0% MPE).19
After injecting subcutaneously the rats with 7 different doses of each drug (n = 8
for each dose of each drug), dose-response curves were constructed. Then the curves
were fitted by SAS NLIN Procedures (SAS Institute Inc., Carey, NC, version 9.1),
and the value of 50% effective dose (ED50), defined as the dose that caused 50%
cutaneous analgesia, was obtained.20,21 The ED25 and ED75 of drugs were obtained by
the same SAS NLIN Procedures that were used to derive the ED50.22 Then the
blockade duration caused by each drug was performed at equianalgesic doses (ED25,
ED50, ED75) (n = 8 rats for each dose of each drug). Furthermore, the area under
curves (AUCs) of sensory blockades of drugs was estimated using Kinetica version
2.0.1 (InnaPhase Corporation, Philadelphia, PA).
Part II - Cardiovascular and neurological effects
On Day 1, rats were anesthetized with pentobarbital sodium (i.p.) at the dose of
50 mg·kg-1 and the right femoral artery and vein were cannulated with polyethylene
catheters (PE-50), which were filled with heparin saline (35 U/mL). The free end of
the catheter was threaded through a 18-gauge needle and then tunneled
subcutaneously. The catheter was cut with 5 cm protruding from the skin at the
midline in the posterior cervical area and sealed by heating it with a match and
compressing it with a hemostat.17,23
lines to reach the animal and prevent the animal from chewing on the lines. The tube
in the right femoral vein was connected to an infusion pump (Harvard Model 22
Infusion Pump, Harvard Apparatus Inc., Holliston, MA) for delivery of the drugs. The
tube in femoral artery was connected to a transducer, and MAP and HR were recorded
using a polygraph (MP36, BIOPAC Systems Inc, Goleta, CA, USA).17,23 The
investigator (Dr. Chen) was blinded to the drugs under study. After intravenous
infusions of either 1) bupivacaine at 8.0 μmol · kg-1
· min-1, carbetapentane at 11.4
μmol · kg-1
· min-1, orcaramiphen at 16.0 μmol · kg-1 · min-1 or 2) normal saline at a
rate of 400 μL · kg-1 · min-1, the onset time of seizure, respiratory arrest, time to cause
impending death, MAP, and HR were evaluated.
The onset time of seizure was defined as the time when the first convulsion
occurred and respiratory arrest when apnea occurred for 15 seconds by observation of
chest movement. The time to impending death was defined as the time it took for the
HR decreased to 0 per minute.17,23
Statistical Analysis
Values are presented as meanSEM or ED50 values with 95% confidence interval (95% CI). The differences in baseline data, potencies (ED50s), %MPE, full
recovery time, AUCs, and the time to cause toxicity between medications were
Tukey's honestly significant difference (HSD) test. The differences in duration (Fig. 3)
among drugs were evaluated by two-way ANOVA followed by pairwise Tukey's HSD
test. Analysis of variance withrepeated measures followed by Duncan’s
multiple-rangetest was used for post hoc multiple comparisons of means onMAP and
HR. SPSS for Windows (version 17.0) was used for all statistical analyses. Statistical
RESULTS
Carbetapentane and caramiphen, as well as bupivacaine produced
dose-dependent cutaneous analgesia in rats (Figure 1). The ED50s of drugs are shown
in Table 1. On the ED50 basis, the relative potency of these three drugs was found to
be bupivacaine > carbetapentane > caramiphen (P<0.01; Table 1). At equipotent doses
of 8.0 μmol · kg-1
for bupivacaine, 11.4 μmol · kg-1 for carbetapentane, and 16.0
μmol · kg-1
for caramiphen, all the local anesthetic drugs caused 100% blockade with
durations of actions of 108±11, 124±11, and 115±12 min, respectively (Figure 2 and
Table 2). At these given doses (Table 2), there were no significant differences among
these three drugs for the %MPE, full recovery time, and AUCs. Saline elicited no
cutaneous analgesic effects. At equianalgesic doses (ED25, ED50, ED75), the block
duration caused by carbetapentane or caramiphen was similar to that caused by
bupivacaine, a long-acting local anesthetic (Fig. 3). All rats recovered completely
after each subcutaneous injection.
The baseline data of body weight, MAP, and HR showed no significant
differences among groups (Table 3). At equipotent doses, the times required to cause
seizure, respiratory arrest, and impending death were longer in the carbetapentane
(P<0.05) or caramiphen (P<0.05) group than in the bupivacaine group (Figure 4).
infusion period. The HR and MAP displayed a tendency to decrease before CV
collapse (Figure 5) in all drug groups. The declines in MAP and HR were slower in
the carbetapentane (P<0.01) or caramiphen (P<0.01) group when compared with the
bupivacaine group (Figure 5). The rapidity of decline of the MAP and HR occurred in
DISCUSSION
This study showed that carbetapentane and caramiphen displayed a
dose-dependent local anesthetic effect on infiltrative cutaneous analgesia. The
sensory/nociceptive block duration caused by carbetapentane or caramiphen was
equal to that caused by bupivacaine, a long-acting local anesthetic. At equipotent
doses, carbetapentane and caramiphen did not elicit systemic toxicity as quickly as
bupivacaine.
Both carbetapentane and caramiphen have been known to treat coughing and
related conditions clinically.1,4,24,25 Recently, we demonstrated that caramiphen has a
local anesthetic effect on spinal anesthesia.5 Infiltrative cutaneous anesthesia is an
acceptable choice for management of surgical anesthesia and postoperative pain,
because it is relatively free of side effects.15 In this study, we showed that
carbetapentane and caramiphen had a local anesthetic effect on infiltrative cutaneous
analgesia in a dose-related fashion. Although the pharmacological mechanisms of
carbetapentane and caramiphen are largely unclear, inhibiting Na+ currents may be
one of the principle mechanisms of carbetapentane and caramiphen to hold local
anesthetic effects, which is worth testing in the next study.
Our previous studies showed that the spinal blockades with caramiphen at 4.62
μmole/kg 5
anesthesia. In this recent experiment, bupivacaine has almost 1.4- and 2.0-fold greater
potencies than carbetapentane and caramiphen as infiltrative cutaneous analgesia,
respectively. There appears to be a uniformity of the comparative potencies of
caramiphen and bupivacaine with respect to cutaneous analgesia (Figure 1 and Table
1) and spinal anesthesia. Furthermore, the sensory block duration of carbetapentane or
caramiphen was similar to bupivacaine, a long-acting local anesthetic, on an
equianalgesic basis (ED25, ED50, ED75). These findings suggest that there may be a
great potential for the use of carbetapentane and caramiphen as local anesthetics in the
clinical setting, provided that the CNS and CV toxicity is investigated.
Accidental intravenous injection of local anesthetics may cause CNS and CV
system toxicity and even result in death.23,26 Through an animal model of local
anesthesia, we performed the local anesthetic effects of carbetapentane, caramiphen,
and bupivacaine as infiltrative cutaneous analgesia to determine the equipotent
analgesic doses of these drugs. At equipotent doses, we showed that infusion of
carbetapentane or caramiphen produced a delayed onset of CNS and CV toxicity
when compared with bupivacaine. However, the degrees of toxicities were the same
once toxicity occurred (Figure 4). Furthermore, we chose the animal model with the
spontaneously breathing rats, a clinical scenario when local anesthesia is practiced on
with carbetapentane and caramiphen compared with bupivacaine. Overall, these
results suggest that carbetapentane and caramiphen are less ―toxic‖ and may feature a
safer systemic toxicity profile than bupivacaine during continuous intravenous
infusion.
In summary, our experiments reported that carbetapentane and caramiphen
produced dose-dependent cutaneous analgesia and their block durations were similar
to bupivacaine. Intravenous equipotent analgesic doses of carbetapentane and
caramiphen are better tolerated to produce central nervous system and cardiovascular
system toxicity than bupivacaine. The clinical relevance of these effects warrants
ACKNOWLEDGEMENTS
The authors gratefully acknowledge the financial support provided for this study
by the National Science Council (NSC 99-2314-B-039-013-MY3; NSC
REFERENCES
1. Donmez OA, Asci B, Bozdogan A, Sungur S. Simultaneous determination of
potassium guaiacolsulfonate, guaifenesin, diphenhydramine HCl and
carbetapentane citrate in syrups by using HPLC-DAD coupled with partial
least squares multivariate calibration. Talanta. 2011;83:1601-1605.
2. Sciarra D, Carter S, Merritt HH. Caramiphen hydrochloride in the treatment of
diseases of the basal ganglions. J Am Med Assoc.1949;141:1226-1229.
3. Snyder GG. An evaluation of caramiphen ethane disulfonate as an antitussive
agent. Laryngoscope. 1953;63:1008-1013.
4. Figueiredo TH, Aroniadou-Anderjaska V, Qashu F, et al. Neuroprotective
efficacy of caramiphen against soman and mechanisms of action. Br J
Pharmacol. 2011.
5. Chen YW, Chu CC, Chen YC, Wang JJ, Hung CH. Isobolographic analysis of
caramiphen and lidocaine on spinal anesthesia in rats. Neurosci Lett.
2010;469:174-178.
6. Carbonell AM, Harold KL, Mahmutovic AJ, et al. Local injection for the
treatment of suture site pain after laparoscopic ventral hernia repair. The
American surgeon. 2003;69:688-691.
bupivacaine with epinephrine wound instillation for pain relief after pediatric
inguinal herniorrhaphy and hydrocelectomy. Regional anesthesia and pain
medicine. 2003;28:24-28.
8. Cameron AE, Cross FW. Pain and mobility after inguinal herniorrhaphy:
ineffectiveness of subcutaneous bupivacaine. Br J Surg. 1985;72:68-69.
9. Hannibal K, Galatius H, Hansen A, Obel E, Ejlersen E. Preoperative wound
infiltration with bupivacaine reduces early and late opioid requirement after
hysterectomy. Anesth Analg. 1996;83:376-381.
10. Hung CH, Wang JJ, Chen YC, Chu CC, Chen YW. Intrathecal oxybuprocaine
and proxymetacaine produced potent and long-lasting spinal anesthesia in rats.
Neurosci Lett. 2009;454:249-253.
11. Chen YW, Huang KL, Liu SY, et al. Intrathecal tri-cyclic antidepressants
produce spinal anesthesia. Pain. 2004;112:106-112.
12. Eledjam JJ, de la Coussaye JE, Bassoul B, Brugada J. [Mechanisms of the
cardiac toxicity of bupivacaine]. Ann Fr Anesth Reanim. 1988;7:204-210.
13. Mazoit JX, Lambert C, Berdeaux A, Gerard JL, Froideveaux R.
Pharmacokinetics of bupivacaine after short and prolonged infusions in
conscious dogs. Anesth Analg. 1988;67:961-966.
bupivacaine. Anesthesiology. 1979;51:285-287.
15. Khan MA, Gerner P, Kuo Wang G. Amitriptyline for prolonged cutaneous
analgesia in the rat. Anesthesiology. 2002;96:109-116.
16. Chen YW, Chu CC, Chen YC, Hung CH, Hsueh MI, Wang JJ. Clonidine as
adjuvant for oxybuprocaine, bupivacaine or dextrorphan has a significant
peripheral action in intensifying and prolonging analgesia in response to local
dorsal cutaneous noxious pinprick in rats. Neurosci Lett. 2011;496:186-190.
17. Hung CH, Liu KS, Shao DZ, Cheng KI, Chen YC, Chen YW. The systemic
toxicity of equipotent proxymetacaine, oxybuprocaine, and bupivacaine during
continuous intravenous infusion in rats. Anesth Analg. 2010;110:238-242.
18. Chen YW, Liu KS, Wang JJ, Chou W, Hung CH. Isobolographic analysis of
epinephrine with bupivacaine, dextromethorphan, 3-methoxymorphinan, or
dextrorphan on infiltrative anesthesia in rats: dose-response studies. Reg
Anesth Pain Med. 2008;33:115-121.
19. Chen YW, Chu CC, Chen YC, Wang JJ, Hung CH. The local anesthetic effect
of memantine on infiltrative cutaneous analgesia in the rat. Anesthesia and
analgesia. 2011;113:191-195.
20. Leung YM, Wu BT, Chen YC, Hung CH, Chen YW. Diphenidol inhibited
2010;58:1147-1152.
21. Chen YW, Chu CC, Chen YC, Wang JJ, Hung CH. The dose-dependent study
of verapamil and diltiazem on spinal anesthesia in the rat. Neurosci Lett.
2010;482:76-80.
22. Chen YW, Chen YC, Lin CN, et al. The spinal anaesthetic effect of
dextromethorphan, dextrorphan, and 3-methoxymorphinan. Eur J Pharmacol.
2007;569:188-193.
23. Chen YW, Wang JJ, Liu TY, Chen YC, Hung CH. Systemic dextromethorphan
and dextrorphan are less toxic in rats than bupivacaine at equianesthetic doses.
Can J Anaesth. 2011;58:55-61.
24. Thomas J, Heurich AE, Shepherd DA, Sanzari NP. A system for the clinical
assessment of the antitussive activity of caramiphen. Curr Ther Res Clin Exp.
1974;16:1082-1090.
25. Van Hoorde AJ. Clinical experience with carbetapentane. Int Rec Med Gen
Pract Clin. 1956;169:513-516.
26. Srinivasa V, Gerner P, Haderer A, Abdi S, Jarolim P, Wang GK. The relative
toxicity of amitriptyline, bupivacaine, and levobupivacaine administered as
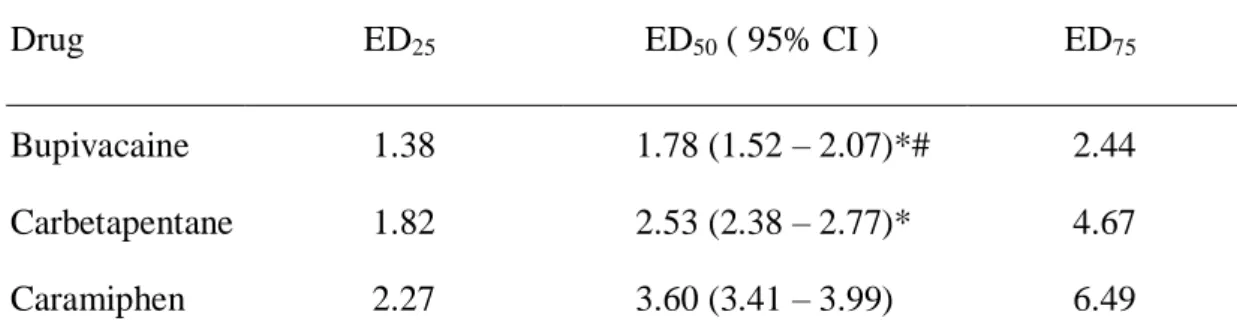
Table 1. The 50% effective dose (ED50), ED25, and ED75 of drugs on infiltrative cutaneous analgesia in rats
Drug ED25 ED50 ( 95% CI ) ED75
Bupivacaine 1.38 1.78 (1.52 – 2.07)*# 2.44
Carbetapentane 1.82 2.53 (2.38 – 2.77)* 4.67
Caramiphen 2.27 3.60 (3.41 – 3.99) 6.49
EDs of drugs (μmol/kg) were obtained from Fig. 1. CI = confidence interval. Symbols (*,#) indicate P<0.01 when compared with caramiphen and carbetapentane,
respectively, by using one-way ANOVA and pairwise Tukey’s HSD test for paired comparisons.
Table 2. The percent of maximal possible effect (%MPE), full recovery time, and area under curves (AUCs) of bupivacaine at 8.0 μmol · kg-1, carbetapentane 11.4 at μmol · kg-1 and caramiphen at 16.0 μmol · kg-1 as infiltrative cutaneous analgesia in rats
%MPE Full recovery time (min) AUCs (%min)
Bupivacaine 100 ± 0 108 ± 11 7036 ± 762
Carbetapentane 100 ± 0 124± 11 7552±415
Caramiphen 100 ± 0 115 ± 12 6668 ± 806
The %MPE, duration of drug action, AUCs (mean±SEM) between bupivacaine, carbetapentane, and caramiphen were not significantly different.
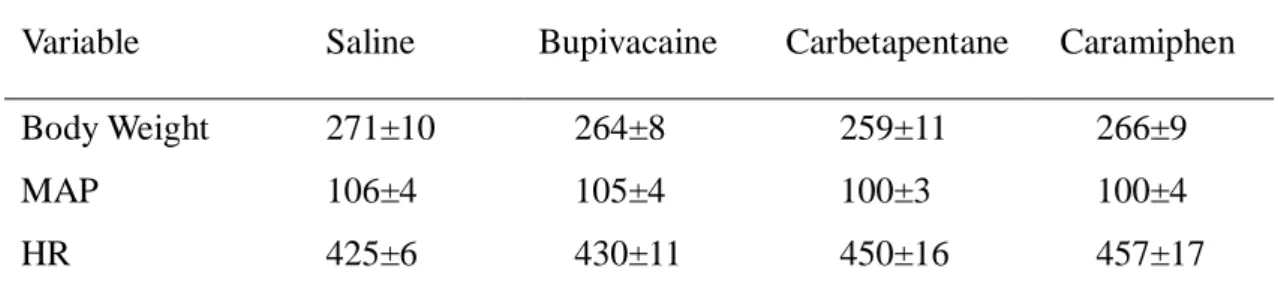
Table 3. Baseline data are showed as mean±SEM
Variable Saline Bupivacaine Carbetapentane Caramiphen
Body Weight 271±10 264±8 259±11 266±9
MAP 106±4 105±4 100±3 100±4
HR 425±6 430±11 450±16 457±17
There were no significant differences among the groups for these variables. MAP = mean arterial blood pressure; HR = heart rate.
Dose ( mol/kg )
1 10%MPE (
ma
xi
ma
l
po
ss
ib
le
effec
t)
0 20 40 60 80 100 Bupivacaine Carbetapentine CaramiphenFig. 1.
Time (min)
0 15 30 45 60 75 90 105 120 135 150%PE
(poss
ible
effect)
0 20 40 60 80 100 Bupivacaine 8.0 mol/kg Carbetapentane 11.4 mol/kg Caramiphen 16.0 mol/kg SalineFig. 2.
ED (effective dose)
25 50 75Full Re
covery T
ime (min)
0 15 30 45 60Bupivacaine
Carbetapentane
Caramiphen
Fig. 3.
Sa
line
Bu
pivaca
ine
Carbe
tapen
tane
Caram
iphe
n
Ti
me
to ca
us
e to
xi
ci
ty (mi
n)
0
5
10
15
20
25
30
35
Seizure
Apnea
Impending death
*
*
*
*
*
*
ND ND NDFig. 4.
-2 01 4 7 10 13 16 19 22 25 28
MAP (m
mHg
)
0 30 60 90 120Saline
Bupivacaine
Carbetapentane
Caramiphen
*
Time (min)
-2 01 4 7 10 13 16 19 22 25 28HR
(bp
m)
0 100 200 300 400 500*
*
*
Fig. 5.
FIGURE LEGENDS
Fig. 1. The dose—response curves of bupivacaine, carbetapentane, and caramiphen as
infiltrative cutaneous analgesia in rats (n = 8 at each testing point). Data are shown as
mean±SEM.
Fig. 2. Time courses of bupivacaine (8.0 μmol/kg), carbetapentane (11.4 μmol/kg),
caramiphen (16.0 μmol/kg), and saline (vehicle) on infiltrative cutaneous analgesia in
rats. Data are presented as mean±SEM; each group, n=8.
Fig. 3. Full recovery time (duration) of cutaneous analgesia of bupivacaine,
carbetapentane, and caramiphen at doses of ED25, ED50, and ED75 (n = 8 at each
testing point) in rats. Values are expressed as meanSEM. The differences in duration were evaluated by using two-way ANOVA followed by pairwise Tukey's HSD test.
Fig. 4. Time to cause toxicity of equipotent bupivacaine, carbetapentane, and
caramiphen at the onset of seizure, respiratory arrest, and time to cause impending
death. Saline group was not detected (ND) the toxicity symptoms. The symbol (*)
indicates P < 0.05 when carbetapentane or caramiphen compared with bupivacaine.
Data are presented as meanSEM; each group, n=8.
Fig. 5. Mean arterial blood pressure (MAP) and heart rate (HR) change during
infusion of either 1) bupivacaine at 8.0 μmol · kg-1 · min-1, carbetapentane at 11.4
μmol · kg-1
volume of 400 μL · kg-1
· min-1 (the same volume given to the animals in the drug
group) as infusion; 0 min is the start of infusion. Infusion was stopped when the time
to cause impending death was reached. The symbol (*) indicates P < 0.01 for
carbetapentane or caramiphen compared with bupivacaine. Data are presented as