Natural Frequency Analysis of Periodontal Conditions in Human
Anterior Teeth
H
AW-M
INGH
UANG,
1S
HENG-Y
ANGL
EE,
2,3C
HING-Y
INGY
EH,
4M
AO-S
HENGW
ANG,
2W
EI-J
ENC
HANG,
2and C
HE-T
ONGL
IN21Graduate Institute of Medical Sciences, Taipei Medical University, Taipei, Taiwan,2Graduate Institute of Oral Rehabilitation
Sciences, Taipei Medical University, Taipei, Taiwan,3Dental Department of Wan-Fang Hospital, Taipei Medical University, Taipei, Taiwan, and4School of Medicine, Taipei Medical University, Taipei, Taiwan
(Received 21 February 2001; accepted 11 July 2001)
Abstract—The purpose of this study was to evaluate the pos-sibility of using natural frequency 共NF兲 analysis to detect the attachment loss of periodontal tissue. In this study, 698 anterior teeth were examined by a conventional probing method and also by NF analysis. The teeth were triggered to vibrate with an impulse hammer, and the vibrational response was detected by an acoustic sensor. Our results demonstrate no significant dif-ference in NF values between the upper–lower/left–right quad-rants of the tested teeth, although the mean natural frequency value of central incisors with periodontal disease was found to be 1.24⫾0.11 kHz which is significantly lower than that of teeth in a healthy condition (1.34⫾0.20 kHz; p⬍0.01). On the other hand, the mean frequency for periodontal disease involv-ing canines (1.28⫾0.09 kHz) was also significantly lower than the corresponding value for healthy analogs (1.35⫾0.17 kHz;
p⬍0.05). These results suggest that NF analysis appears to be
an effective method for assessing the periodontal condition of anterior teeth. Moreover, since this method is noninvasive, non-destructive, and necessitates minimal tooth contact, it can serve as an effective method for the early quantifiable testing and prevention of periodontal disease. © 2001 Biomedical
Engi-neering Society. 关DOI: 10.1114/1.1408925兴
Keywords—Natural frequency, Tooth, Stability, Periodontium.
INTRODUCTION
Early detection and diagnosis of altered periodontial conditions has always been a subject of concern for the dental researcher. Periodontal probe examination is the principle clinical method for the assessment of periodon-tal conditions in vivo, although the accuracy of this method is in doubt due to various factors such as vari-ability in the diameter of the probe and the probing force applied possibly affecting the measurement results.2,8,17,20,21 Radiographic image observation is an-other method for periodontal condition assessment.
How-ever, such a technique is not suitable for long-term tooth-mobility observation or the early diagnosis and prevention of periodontal disease. Therefore, there exists a strong clinical demand for a novel noninvasive tech-nique to evaluate the status of periodontal conditions.
The natural frequency 共NF兲 is an important dynamic response of a vibrating object, and it is related to the material properties and boundary conditions of a struc-ture. The proposed technique for NF value measurement, modal testing, is a noninvasive and nondestructive method of investigation. The use of a NF value as a parameter for the assessment of bone density status and implant stability has been widely discussed in much pub-lished orthopedic research.3,4,6,11,12,25,26Recently, many in vivo and in vitro studies also demonstrated that a strong relationship exists between the NF value of a dental implant and the boundary conditions associated with that implant subsequent to implant installation.5,13,14,19,22 These studies have concluded that the NF value corre-sponding to selected dental implants could be used as an index for monitoring dental-implant stability and the de-gree of alveolar bone loss.
The application of such a vibration technique to hu-man teeth is rare. In 1973, Noyes and Solt excited cen-tral incisors to vibrate by applying a sinusoidal force to the teeth. They found that the vibrational characteristics of a tooth are related to its mass and the nature of the tooth’s surrounding tissue, although, the detailed rela-tionship between NF and a tooth’s boundary conditions was not discussed in their report.15Okazaki et al. studied the mobility of human teeth by using a modal testing technique in 1996, wherein the viscous damping behav-ior of the periodontal membrane and artificial material was compared and discussed in their study.16 Although natural frequency analysis was not included in these au-thors’ study, their results demonstrated that the modal testing technique could serve as a useful tool for analyz-ing the material properties of the periodontal Address all correspondence to Professor Lee, Sheng-Yang,
Gradu-ate Institute of Oral Rehabilitation Sciences, Taipei Medical University, 250 Wu-Hsing Street, Taipei, Taiwan. Electronic mail: [email protected]
共10兲/915/6/$15.00
Printed in the USA. All rights reserved. Copyright © 2001 Biomedical Engineering Society
membrane.16 To evaluate the correlation between tooth’s NF values and its periodontium status, Lee et al. mea-sured the natural frequencies of healthy upper central incisors in vitro and noted that the NF value was lower when the relative condition of surrounding structures was poorer.9Their findings suggest that NF values might be a useful parameter for assessing periodontal conditions clinically. To clearly understand the vibrational behavior of a tooth, the natural frequencies of anterior teeth were examined in vivo in this study, in which differences in NF values between these teeth with either healthy or diseased periodontium were compared and discussed.
MATERIAL AND METHODS
To examine the changes in a tooth’s NF value when a pathological condition arises in the periodontium locat-ing that tooth, modal analysis and a periodontal-status examination, including a probing of the periodontal depth and x-ray radiation, were performed on 110 adult volunteers. Upper and lower central incisors and canines were chosen for examination for every volunteer. A total of 698 anterior teeth were tested in the entire study.
In the present study, the parameter ‘‘attachment loss’’ was used as an index for the assessment of the periodon-tal health condition, the term being defined as the sum of the probing depth and the extent of gingival recession. To examine the attachment loss, a Williams Probe 共945188 pw Hu-Friedy, Chicago, IL兲 was used to probe six positions adjacent to the tooth being assessed includ-ing the mesiobuccal, midbuccal, distobuccal, mesiolin-gual, midlinmesiolin-gual, and distolingual sides of the tested teeth.1According to Ramfjord’s classification, an attach-ment loss reaching 4 – 6 mm was noted as moderate periodontal disease requiring treatment.18 Therefore, a middle value of 5 mm was used as a threshold to judge the health status of the periodontal condition in this study. That is, if an attachment loss reaching 5 mm was detected in one of the six tooth-testing positions, then we gauged the tooth as exhibiting a diseased periodontium.
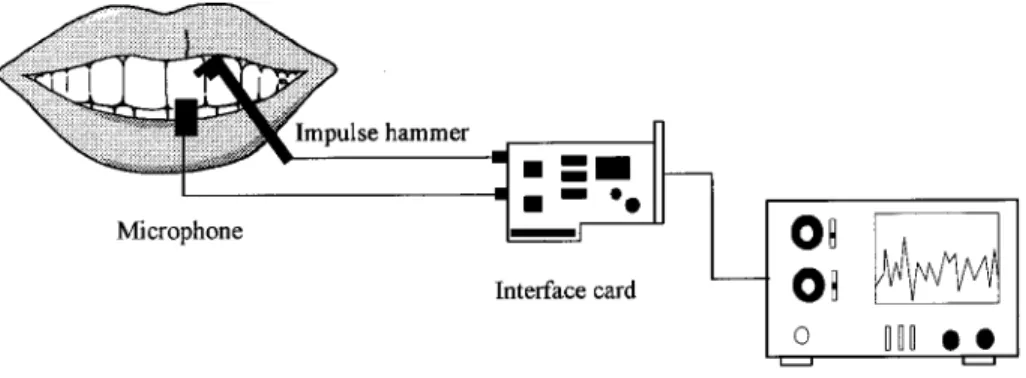
To measure the NF value of the tooth, the modal testing method was adopted in this study. As shown in Fig. 1, an impulse force was applied directly to the labial surface of the tested tooth with an impulse force hammer 共model GK291C80, PCB Piezotronics, Buffalo, NY兲. When the piezoelectronic tip of the hammer touched the tooth, an impact signal was transferred to the analyzer. According to our previous study,7 in order to minimize the mass effect of the sensor, a noncontact acoustic microphone 共FM-10B, FC Electronic, Taipei, Taiwan兲 was placed at a distance of about 1 cm away from the labial surface of the tested tooth to receive the vibra-tional signal.
To diminish artifacts and any spurious responses caused by background noise, the microphone was not turned on until the analyzer had received the hammer-striking signal. The vibrational signal was then trans-ferred to a frequency spectrum analyzer 共Probel II, Pro-wave Engineering, Hsinchu, Taiwan兲. The specific natural frequency of the tested tooth was determined as being that frequency corresponding to the peak vibra-tional amplitude value of the tooth. Each datum point was obtained by averaging the frequencies of five re-peated measurements.
Statistical software 共Stastica, Statosoft, Tulsa, OK兲 was used for comparisons of measured NF values and the variables corresponding to the tested teeth. The tested teeth were divided into four groups according to their position in the four intraoral quadrants as upper left 共UL兲, upper right 共UR兲, lower left 共LL兲, and lower right 共LR兲. One-way analysis of variance was computed to test if the quadrant location of the tooth was related to the value of its natural frequency for both healthy and dis-eased groups of teeth. On the other hand, comparisons of NF values with healthy and diseased periodontium were made with the use of the Student’s t-test with p values below 0.05 being considered to indicate a statistically significant difference between the means of test popula-tions.
FIGURE 1. Instruments and test-ing methods used in this study.
RESULTS
In total, 698 anterior teeth were tested in this study. After an attachment-loss examination was performed, we determined that there were 523 teeth with healthy peri-odontium 共including 257 central incisors and 266 ca-nines兲 and 75 teeth exhibiting periodontal disease 共in-cluding 42 central incisors and 33 canines兲. The distributions by health status of the tested teeth are listed in Table 1.
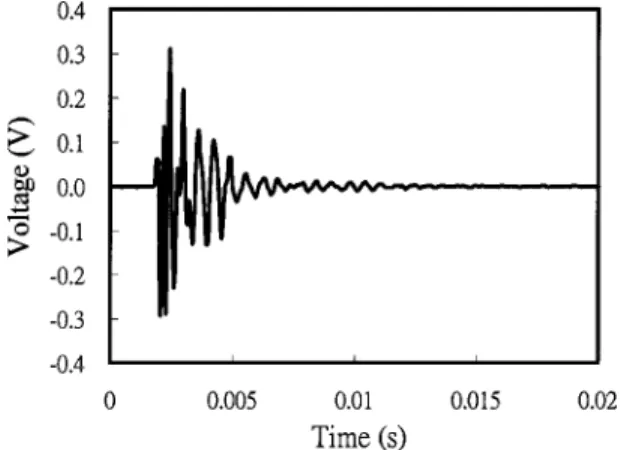
Figure 2 illustrates a typical signal of a tested incisor received by an acoustic microphone. The amplitude of the vibrational spectrum decayed in 10 ms due to the damping effect of the surrounding tissue. While the vi-brational signal was converted from the time domain to the frequency domain, the natural frequency of the test incisor could be clearly identified through the peak value of its mobility 共Fig. 3兲.
The NF values corresponding to tested teeth at differ-ent locations within the oral cavity with healthy and diseased periodontia are listed in Tables 2 and 3, respec-tively. When the NF values of tested teeth are grouped according to their location in different sites of the four quadrants, regardless of whether a tooth is healthy or diseased, no significant difference in NF was noted be-tween the various quadrants. According to these findings, the tested teeth in the various quadrants were merged in the following analysis.
Table 4 lists the mean NF values for incisors and canines after combining all the quadrant groups. The mean NF values for both central incisors and canines varied quite obviously as a result of the occurrence of periodontal disease. The measured natural frequencies of healthy central incisors 共with an average of 1.34 ⫾0.20 kHz兲 and the diseased group 共with an average of 1.24⫾0.11 kHz兲 ranged from 0.93 to 1.82 and 1.02 to 1.54 kHz, respectively. The Result obtained from the statistics showed that the NF value of healthy incisors differed substantially from the corresponding vibration frequency for analogous teeth demonstrating periodontal disease ( p⬍0.01). In addition, the same tendency was also noted for the canine groups. The measured natural frequencies of healthy canines 共with an average of 1.35 ⫾0.17 kHz兲 and the diseased group 共with an average of 1.28⫾0.09 kHz兲 ranged from 0.96 to 1.82 and 1.11 to 1.51 kHz, respectively. The mean frequency for healthy canines 共Hz兲 also differed notably from the correspond-ing value for analogous teeth demonstratcorrespond-ing periodontal disease ( p⬍0.05). According to traditional classifica-tions, central incisors and canines were combined as an-terior teeth to test the natural frequency changes with the occurrence of periodontal disease. The mean frequency for the periodontal involved grouped anterior teeth (1.26⫾0.10 kHz) was significantly lower than the corre-sponding value for analogous teeth revealing healthy pe-riodontia (1.34⫾0.18 kHz; p⬍0.01).
DISCUSSION
An accelerometer is the most common transducer used for detecting vibrational signals in modal testing experiments. Both Noyes and Solt15and Okazaki et al.16 used an accelerometer as a signal detector in their
vibra-TABLE 1. Number of examined teeth distributed by the tooth group and general periodontal health condition. UL, upper
left; UR, upper right; LL, lower left; and LR, lower right.
Tooth
Healthy Diseased
UL UR LL LR UL UR LL LR
Incisors 56 80 77 44 6 8 15 13
Canines 57 81 81 47 5 7 11 10
FIGURE 2. Vibrational signal of a tested incisor as received by the acoustic microphone.
FIGURE 3. Frequency response spectrum of a vibrating in-cisor. A specific tooth’s natural frequency was identified by the mean of the resonance frequency corresponding to the peak value of the vibration amplitude for replicate experi-ments.
tional analyses of teeth. However, due to the relatively small size of human teeth by comparison to the acceler-ometer, using an accelerometer as a detector may cause unexpected errors. On the other hand, when an acceler-ometer is used, it needs to be firmly attached to the surface of the test object. Therefore, the use of an accel-erometer as a signal detector for the vibrational analysis of tested teeth is not suitable for intraoral practices. To eliminate the unnecessary mass effect of the accelerom-eter, Lowet et al. used a microphone as a transducer to measure the natural frequency of the tibia. These authors discussed how using a microphone as a sensor reflects certain advantages in examining the vibrational behavior of hard tissue of living creatures.11 In our study, a non-contact acoustic microphone was used to collect the vi-brational responses of tested teeth. Our results indicated that a microphone can also serve as an effective tool for the testing of NF values for human teeth due to its absence of contact with the tooth being tested and, if selected appropriately, its highly sensitive characteristics. As indicated by the data listed in Tables 2 and 3, no difference was found between the NF values for teeth on the basis of the quadrant in which they were located. This would likely be the case since the normal human dentition reveals a generally equivalent symmetrical geo-metric shape and distribution between the four quadrants inside the oral cavity. Although the results of Noyes and Solt indicated that an observable difference of natural frequencies of teeth existed between the lower and upper central incisors,15 this observation may be questionable due to the small sampling size adopted in their analysis. The results of the Okazaki et al. analysis revealed that incisors exhibit similar vibrational characteristics regard-less of whether the teeth were located on the left side or the right side.16 These results are similar to our findings. The effect of this finding shows that when periodontal disease occurs, we can use a person’s contralateral analo-gous healthy tooth as a basis for a reference value to test
the level of periodontal attachment for corresponding teeth.
In our previous study, a finite-element model was used to study the vibrational characteristics of maxillary central incisors. The first four modes the of NF values and the corresponding mode shapes were calculated. We found that the first vibration mode of the model is a single bending mode.9 According to the above finding and considering the mechanical structure of a tooth共free on one end, and fixed on the other兲, thus, with regards to its vibrational behavior, we can analyze a tooth’s natural frequency by using a cantilever beam theory as follows:11,13,24
fn⫽␣
冑
EI
4. 共1兲
Equation 共1兲 expresses the natural frequency of a vibrat-ing cantilever beam, where fn is the natural frequency of
the beam, is the effective length of its oscillation, E is Young’s modulus, I is the moments of inertia, is the mass per unit effective length, and ␣ is the relevant constant of the boundary term. According to the previous classification, the alveolar bone can be divided into four different types.10 Different alveolar bone types will thus provide different boundary conditions for teeth, and for this reason, teeth with these different bone types will exhibit different values of␣. Although the exact effect of surrounding tissue on the value of ␣ is still unknown, however, in the presence of the same alveolar bone type, the value of␣can be assumed to be a fixed value. In this study, x-ray images of the tested teeth were examined for bone quality. All the tested teeth selected in this study were confirmed to not show bone density decreases. Be-cause the structural properties affecting the natural fre-quency, i.e., Young’s modulus, density, and the shape of the cross section, should not vary in a wide range
be-TABLE 2. Natural frequencies of healthy teeth in different locations„meanÁSD, kHz…within the oral cavity. No significant difference in NF was noted between the various quadrants.
Tooth UL UR LL LR pvalue
Incisors 1.34⫾0.19 1.35⫾0.20 1.34⫾0.20 1.32⫾0.020 0.9304 Canines 1.32⫾0.17 1.35⫾0.18 1.38⫾0.16 1.32⫾0.18 0.1165
TABLE 3. Natural frequencies of periodontal disease involving teeth in different locations „meanÁSD, kHz…within the oral cavity. No significant difference was noted between the various
quadrants.
Tooth UL UR LL LR pvalue
Incisors 1.25⫾0.07 1.24⫾0.12 1.27⫾0.11 1.22⫾0.12 0.6554 Canines 1.32⫾0.15 1.29⫾0.10 1.26⫾0.07 1.27⫾0.08 0.6203
tween individuals. Therefore, the natural frequencies of the teeth will only be affected by the effective length of vibration 共兲. On the other hand, because the material properties of tested teeth, such as Young’s modulus and tooth density, are not likely to change despite the pres-ence of periodontal disease, it would appear that the main factors that influence the NF values derive prima-rily from the tooth’s boundary factors and the value of the effective vibrational length of the tooth. In this study, we found that the natural frequency of both central inci-sors and canines was lower when the teeth had an at-tachment level loss larger than 4 mm.
The extent of the attachment level loss is essentially the decrease in the contact surface between the root and the surrounding tissue, thus, a decrease in the height of the periodontium results in an increase of exposed tooth height, i.e., the effective vibration height. Such a result enhances the ease with which the tooth may vibrate when stimulated appropriately. Therefore, according to Eq. 共1兲, the NF values of a tooth should decrease when the tooth’s attachment level is reduced. As shown in Table 4, our results demonstrate a significant tendency for the NF value of a tooth to decrease subsequent to the occurrence of periodontal attachment loss. This finding matches the vibration theories well. However, for each type of tooth studied, the mean of the diseased data set was within one standard deviation of the mean for the normal data set. Also, the mean for the normal data set was within one standard deviation of the mean for the diseased data set. This may be because attachment loss reaching 5 mm in one of the six tooth-testing positions was detected. We then assess the tooth as one having a diseased periodontium. In fact, mechanically, a 5 mm loss in a single location probably does not influence the natural frequency as much as a 4 mm loss in a number of locations. To better understand the effect of surround-ing tissue on the vibrational characteristics, the NF val-ues of the tested teeth were plotted versus the sum of the fixation loss for both types of teeth. These data are dem-onstrated in Fig. 4. Regardless of the type of teeth, the results of the regression analysis indicate a statistically significant negative linear relationship between the NF value and the sum of the attachment loss.
Referring to the previous observation, the contact sur-face of the posterior tooth is almost twice as large as that of the anterior teeth.23Since the root numbers and shapes
of the anterior and posterior teeth are completely differ-ent, their dynamic behaviors under induced vibration will also be different.16 However, the vibrational characteris-tics of posterior teeth were not assessed in this study because the use of an impulse force hammer in this study was not a simple procedure for posterior teeth examination.16 For the purposes of developing a new clinical diagnostic method for detecting the degree of periodontal health, a novel force-triggering device for individual teeth and suitable for intraoral performance is undoubtedly needed.
In conclusion, we find that the mean natural frequency of anterior teeth will indeed significantly decrease in value as a result of tooth periodontium attachment loss greater than 4 mm. The findings of this research show that the NF analysis for an anterior tooth has the poten-tial to be regarded as a novel noninvasive,
nondestruc-TABLE 4. Comparison of natural frequency„meanÁSD, kHz… between healthy and periodontal disease involving anterior
and posterior teeth.
Tooth Healthy Diseased pvalue Incisors 1.34⫾0.20 1.24⫾0.11 ⬍0.01 Canines 1.35⫾0.17 1.28⫾0.09 ⬍0.05 Anterior teeth 1.34⫾0.18 1.26⫾0.10 ⬍0.01
FIGURE 4. Relationships between NF value and the sum of fixation loss in tested incisor „a… and canine „b…. Scatter plots show the relationship between NF value and sum of fixation loss. Solid lines represent the best-fit linear regres-sion.
tive, minimum-contact, and instant method for clinical periodontal condition assessment.
ACKNOWLEDGMENTS
This study was supported by a grant 共TMC 89-Y05-A105兲 from Taipei Medical University, Taipei, Taiwan, and, in part, by a grant 共NSC 87-2815-C-038-003-B兲 from the National Science Council, Taipei, Taiwan. The authors also wish to thank Prowave Engineering, Inc., for their assistance and for providing instrumentation for use in this study.
REFERENCES
1Armitage, G. C., R. J. Genco, H. M. Goldman, and D. W.
Cohen. Clinical Periodontal Examination. St. Louis: CV Mosby, 1990, pp. 341–344.
2Armitage, G. C., G. K. Svanberg, and H. Lo¨e. Microscopic
evaluation of clinical measurements of connective tissue at-tachment level. J. Clin. Periodontol. 4:173–190, 1977.
3Christensen, A. B., F. Ammitzboll, C. Dyrbye, M.
Cornelis-sen, P. CornelisCornelis-sen, and G. Van der Perre. Assessment of tibia stiffness by vibration testing in situ. I. Identification of mode shapes in different supporting conditions. J. Biomech. 19:53– 60, 1986.
4Cornelissen, P., M. Cornelissen, and G. Van der Perre.
As-sessment of tibial stiffness by vibration testing in situ. II. Influence of soft tissues, joints, and fibula. J. Biomech. 19:551–561, 1986.
5Friberg, B., L. Sennerby, B. Linden, K. Gro¨ndahl, and U.
Lekhilm. Stability measurements of one-stage Bra˚nemark im-plants during healing in mandibles. Int. J. Oral Maxillofac.
Surg. 28:266 –272, 1999.
6Hobatho, M. C., R. Damana, P. Pastor, J. J. Barrau, S.
Laroze, and J. P. Morucci. Development of a three-dimensional finite-element model of a human tibia using ex-perimental model analysis. J. Biomech. 24:371–383, 1991.
7
Huang, H. M., L. C. Pan, S. Y. Lee, C. L. Chiu, K. H. Fan, and K. N. Ho. Assessing the implant/bone interface by using natural frequency analysis: An in vitro study. Oral Surg.,
Oral Med., Oral Path. 90:285–291, 2000.
8Listgarten, M. A.. Periodontal probing: What does it mean? J. Clin. Periodontol. 7:65–176, 1980.
9Lee, S. Y., H. M. Huang, and C. Y. Lin. In vivo and in vitro
natural frequency analysis of periodontal conditions, an inno-vative method. J. Periodontal 74:632– 640, 2000.
10Lekholm, U., and G. A. Zarb. Patient selection and
prepara-tion. In: Tissue-Integrated Prostheses: Osseointegration in Clinical Density, edited by P. I. Bra˚nemark, G. A. Zarb, and
T. Albrektsson. Chicago: Quintessence, 1985, pp. 199–209.
11Lowet, G., X. Dayuan, and G. Van der Perre. Study of the
vibrational behavior of a healing tibia using-finite element modeling. J. Biomech. 29:1003–1010, 1996.
12Lowet, G., R. Van Audekercke, G. Van der Perre, P. Geusens,
J. Dequeker, and J. Lammens. The relation between resonant frequencies and torsional stiffness of long bones: In vitro validation of a simple beam model. J. Biomech. 26:689– 696, 1993.
13Meredith, N., D. Alleyne, and P. Cawley. Quantitative
deter-mination of the stability of the implant-tissue interface using resonance frequency analysis. Clin. Oral Impl. Res. 7:261– 267, 1996.
14Meredith, N., K. Book, B. Friberg, T. Jemt, and L. Sennerby.
Resonance frequency measurements of implant stability in
vivo. Clin. Oral. Impl. Res. 8:226 –233, 1997.
15Noyes, D. H., and C. W. Solt. Measurement of mechanical
mobility of human incisors with sinusoidal forces. J.
Bio-mech. 6:439– 442, 1973.
16Okazaki, M., M. Fukumoto, and J. Takahashi. Damped
oscil-lation analysis of natural and artificial periodontal membrane.
Ann. Biomed. Eng. 24:234 –240, 1996.
17Polson, A. M., J. G. Caton, R. N. Yeaple, and H. A. Zander.
Histological determination of probe tip penetration into gin-gival sulcus of humans using an electronic pressure-sensitive probe. J. Clin. Periodontol. 7:479– 488, 1980.
18Ramfjord, S. P. Indices for prevalence and incidence of
pe-riodontal disease. J. Pepe-riodontal. 30:51–59, 1959.
19Rasmusson, L., N. Meredith, I. H. Cho, and L. Sennerby. The
influence of simultaneous versus delayed placement on the stability of titanium implants in onlay bone grafts. Int. J.
Oral Maxillofac. Surg. 28:224 –231, 1999.
20Robinson, P. J., and R. M. Vitek. The relationship between
gingival inflammation and resistance to probe penetration. J.
Periodontal. Res. 14:239–243, 1979.
21Saglie, R., J. R. Johansen, and L. Flotra. The zone of
com-pletely and partially destructed periodontal fibers in patho-logical pockets. J. Clin. Periodontol. 2:198 –202, 1975.
22Sennerby, L., and N. Meredith. Resonance frequency
analy-sis: Measuring implant stability and osseointegration.
Com-pendium 19:493–502, 1998.
23Shillingburg, Jr., H. T., S. Hobo, L. D. Whitsett, R. Jacobi,
and S. E. Brackett. Fundamental of Fixed Prosthodontics. Chicago: Quintessence, 1997, pp. 85–103.
24Thomson, W. T. Theory of Vibration with Applications.
Englewood Cliffs, NJ: Prentice-Hall, 1988, pp. 221–224.
25Van der Perre, G., R. Van Audekerke, M. Martens, and J. C.
Mulier. Identification of in vivo vibration modes of human tibiae by modal analysis. J. Biomed. Eng. 105:244 –248, 1983.
26Wong, F. Y., S. Pal, and S. Saha. The assessment of in vivo
bone condition in humans by impact response measure. J.