I
NTERESTING
I
MAGE
Huge Tumor Thrombus of Chondrosarcoma on FDG PET/CT
Cheng-Nan Hsu, MD,* Hui-Yi Chen, MD,* Yu-Chin Wu, MD,†‡ Chun-Fan Yang, MD,§
and Te-Chun Hsieh, MD†¶
Abstract: A 24-year-old woman presented with progressive pain in the left groin and left buttock for 4 months. The whole-body FDG PET/CT and MRI of the pelvis revealed a left pelvic mass and venous thrombosis in the left common iliac vein, inferior vena cava, and right atrium. Chondrosarcoma with venous tumor invasion of the inferior vena cava to the right atrium was documented surgically.
Key Words: chondrosarcoma, tumor thrombus, FDG PET/CT, MRI (Clin Nucl Med 2011;36: e142– e145)
REFERENCES
1. Blom JW, Doggen CJ, Osanto S, et al. Malignancies, prothrombotic muta-tions, and the risk of venous thrombosis. JAMA. 2005;293:715–722. 2. Khosa F, Otero HJ, Prevedello LM, et al. Imaging presentation of venous
thrombosis in patients with cancer. Am J Roentgenol. 2010;194:1099 –1108. 3. Lai P, Bomanji JB, Mahmood S, et al. Detection of tumour thrombus by
18F-FDG-PET/CT imaging. Eur J Cancer Prev. 2007;16:90 –94. 4. Sizemore AW, Jacobs MP, Mantil JC, et al. FDG uptake in inferior vena cava
tumor thrombus from renal cell carcinoma on positron emission tomography.
Clin Nucl Med. 2007;32:309 –311.
5. Rydberg JN, Sudakoff GS, Hellman RS, et al. Positron emission tomography-computed tomography imaging characteristics of an inferior vena cava tumor thrombus with magnetic resonance imaging correlation. J Comput Assist
Tomogr. 2004;28:517–519.
6. Snow D, Cohen D, Chapman WC, et al. Positron emission tomography enhancing tumor thrombus in patient with renal cell carcinoma. Urology. 2009;73:270 –271.
7. Nguyen BD. Pancreatic neuroendocrine tumor with portal vein tumor throm-bus: PET demonstration. Clin Nucl Med. 2005;30:628 – 629.
8. Gupta P, Kramer EL, Ponzo F. FDG uptake in tumor thrombus in inferior vena cava from rectal cancer on positron emission tomography. Clin Nucl
Med. 2005;30:342–343.
9. Strobel K, Steinert HC, Bhure U, et al. Tumour thrombus in the superior vena cava from anaplastic carcinoma of the thyroid: FDG-PET/CT imaging find-ings. Eur J Nucl Med Mol Imaging. 2007;34:813.
10. Tripathi M, Sharma R, Jaimini A, et al. Metastatic follicular carcinoma of the thyroid with tumor thrombus in the superior vena cava and right brachioce-phalic and internal jugular veins: FDG-PET/CT findings. Clin Nucl Med. 2008;33:426 – 428.
11. Purandare NC, Dua SG, Rangarajan V, et al. Pulmonary artery and femoral vein tumour thromboembolism in a patient with osteogenic sarcoma demon-strated by FDG PET/CT. Eur J Nucl Med Mol Imaging. 2010;37:653. 12. Tateishi U, Yamaguchi U, Terauchi T, et al. Extraskeletal osteosarcoma:
extensive tumor thrombus on fused PET-CT images. Ann Nucl Med. 2005; 19:729 –732.
13. Farsad M, Pernter P, Triani A, et al. Thromboembolism in pulmonary artery sarcoma. Clin Nucl Med. 2009;34:239 –240.
14. Batra S, Doval DC, Batra U, et al. Gallbladder cancer with tumor thrombus in the superior vena cava. Hepatobiliary Pancreat Dis Int. 2010;9:325–328. 15. Kurtovic J, Van Der Wall H, Riordan SM. FDG PET for discrimination between tumor extension and blood thrombus as a cause for portal vein thrombosis in hepatocellular carcinoma: important role in exclusion of trans-plant candidacy. Clin Nucl Med. 2005;30:408 – 410.
16. Davidson T, Goitein O, Avigdor A, et al. 18F-FDG-PET/CT for the diagnosis of tumor thrombosis. Isr Med Assoc J. 2009;11:69 –73.
17. Do B, Mari C, Biswal S, et al. Diagnosis of aseptic deep venous thrombosis of the upper extremity in a cancer patient using fluorine-18 fluorodeoxyglu-cose positron emission tomography/computerized tomography (FDG PET/CT).
Ann Nucl Med. 2006;20:151–155.
18. Miceli M, Atoui R, Walker R, et al. Diagnosis of deep septic thrombophlebitis in cancer patients by fluorine-18 fluorodeoxyglucose positron emission to-mography scanning: a preliminary report. J Clin Oncol. 2004;22:1949 –1956. 19. Murphey MD, Walker EA, Wilson AJ, et al. From the archives of the AFIP: imaging of primary chondrosarcoma: radiologic-pathologic correlation.
Ra-diographics. 2003;23:1245–1278.
20. Riedel RF, Larrier N, Dodd L, et al. The clinical management of chondro-sarcoma. Curr Treat Options Oncol. 2009;10:94 –106.
21. Brenner W, Conrad EU, Eary JF. FDG PET imaging for grading and prediction of outcome in chondrosarcoma patients. Eur J Nucl Med Mol
Imaging. 2004;31:189 –195.
22. Feldman F, Van Heertum R, Saxena C, et al. 18FDG-PET applications for cartilage neoplasms. Skeletal Radiol. 2005;34:367–374.
23. Purandare NC, Rangarajan V, Agarwal M, et al. Integrated PET/CT in evaluating sarcomatous transformation in osteochondromas. Clin Nucl Med. 2009;34:350 –354.
24. Ho L, Youngworth H, Henderson R, et al. Extraosseous myxoid chondrosar-coma with pulmonary and nodal metastases on FDG PET-CT. Clin Nucl Med. 2009;34:18 –19.
25. Makis W, Hickeson M, Lisbona R. Interesting image. Maffucci syndrome with extraosseous chondrosarcoma imaged with F-18 FDG PET-CT. Clin
Nucl Med. 2010;35:29 –31.
26. Aoki J, Watanabe H, Shinozaki T, et al. FDG-PET in differential diagnosis and grading of chondrosarcomas. J Comput Assist Tomogr. 1999;23:603– 608.
Received for publication January 4, 2011; revision accepted February 28, 2011. From the Departments of *Radiology, †Nuclear Medicine and PET Center, China Medical University Hospital, Taichung, Taiwan; ‡China Medical University, Taichung, Taiwan; §Department of Pathology, China Medical University Hospital, Taichung, Taiwan; and ¶Department of Biomedical Imaging and Radiological Science, China Medical University, Taichung, Taiwan. Conflicts of interest and sources of funding: none declared.
Reprints: Te-Chun Hsieh, MD, Department of Nuclear Medicine and PET Center, China Medical University Hospital, No. 2, Yuh-Der Road, Taichung 404, Taiwan. E-mail: [email protected].
Copyright © 2011 by Lippincott Williams & Wilkins ISSN: 0363-9762/11/3610-0142
Clinical Nuclear Medicine • Volume 36, Number 10, October 2011 e142 | www.nuclearmed.com
FIGURE 1. A 24-year-old woman presented with progressive pain in the left groin and left buttock for 4 months. There was
also swelling of the left lower extremity. Rather, the pulsation and perfusion of the left lower extremity seemed intact and there was no sign of pitting edema or lymphedema. The contrast-enhanced CT with multiplanar reconstruction disclosed an ill-defined mass in left pelvic cavity (arrowheads). The pelvic mass seemed closely contacting with the left pelvic bones, revealing inside calcification, causing periosteal reaction and being enhanced after intravenous administration of contrast medium. The CT features of the mass were thought to be a cartilage malignancy. Surprisingly, the CT also showed the dilated left common iliac vein and inferior vena cava. In addition, it seemed that a long segmental intravenous filling defect extended from the left pelvic mass to the right atrium and revealed inside punctate calcification and heterogeneous enhancement (asterisks). A huge tumor thrombus was suspected on the basis of the above findings.
Clinical Nuclear Medicine • Volume 36, Number 10, October 2011 Thrombus of Chondrosarcoma on FDG PET/CT
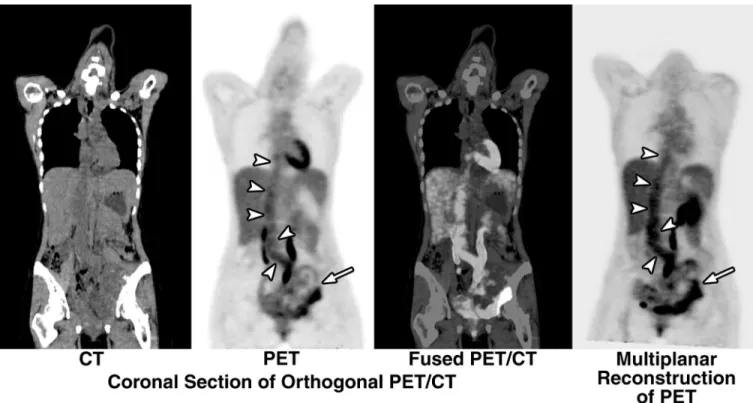
FIGURE 2. The FDG PET/CT showed heterogeneous distribution of abnormally increased FDG radioactivity (maximum SUV⫽
4.1) in the left pelvic cavity (arrows), corresponding to the pelvic mass disclosed on the contrast-enhanced CT. Nevertheless, there also seemed to be slightly increased FDG radioactivity (maximum SUV⫽ 3.0), in contrast to the blood-pool background radioactivity, along the left common iliac vein, inferior vena cava, and the right atrium of heart (arrowheads).
FIGURE 3. The MRI of the pelvis revealed hyperintensity on the short–inversion-time inversion recovery (STIR) images and
heterogeneous enhancement on the T1-weighted fat-suppressed contrast-enhanced images in both, pelvic (arrows) and intravenous lesions (arrowheads). The earlier MRI features, in accordant with the CT and FDG PET/CT findings, strongly suggested the highly probable malignant nature of the pelvic mass. On the other hand, the same MRI features, despite the equivocal CT and PET/CT findings, supported the diagnosis of tumor thrombus along the left common iliac vein, inferior vena cava, and the right atrium.
Hsu et al Clinical Nuclear Medicine • Volume 36, Number 10, October 2011
FIGURE 4. CT-guided biopsy of the pelvic tumor revealed hyaline cartilages and chondrocytes with hypercellularity as well as
marked cellular pleomorphism and hyperchromasia (hematoxylin and eosin stain, 100⫻). The immunohistochemical study showed positive for S-100 stain (100⫻). Grade 2 chondrosarcoma was diagnosed according to the radiologic and pathologic findings. After the multidisciplinary team discussion about the treatment strategy, neoadjuvant chemoradiation therapy followed by cytoreduction surgery was suggested because of the advanced stage of disease and clinical suspicion of occult tumor thrombi elsewhere. However, this patient hesitated for suggested treatment and lost follow-up after her insistence of hospital discharge for alternative therapy.
Venous thrombosis is a multifactorial disorder. Compared with the general population, there are several folds of increasing incidence and progression of venous thrombosis in patients with cancer.1The pathogenesis of thrombotic disorders in patients with
cancer includes hypercoagulability, venous stasis, and vessel wall damage.2Tumor thrombosis is a relatively rare complication of
solid cancers and the reported incidence of occult inferior vena cava tumor thrombosis is about 0.11%.3Tumor thrombosis
diagnosed by FDG PET has been reported sporadically in various types of cancer, including renal cell carcinoma,4 – 6pancreatic
cancer,7colon cancer,8adrenocortical carcinoma,7thyroid cancer,9,10osteosarcoma,11,12Ewing sarcoma,3leiomyosarcoma,13
gallbladder cancer,14hepatocellular carcinoma,3,15,16and lymphoma.3,16Typically, tumor thrombosis presents with high FDG
uptake. However, the infectious or bland thrombosis may also appear with increased FDG radioactivity,17,18causing difficulties in
correct diagnosis based on FDG PET only.
Contrast-enhanced CT may be useful in detecting venous thrombosis but greatly depends on an adequate bolus of contrast with faster injection rate for optimal vessel opacification.2However, the routine contrast-enhanced CT is usually done with a slower
injection rate of contrast because the most majority of venous thromboses, usually unsuspected, in patients with cancers is found incidentally. Therefore, the abilities to detect and characterize the venous thrombosis with routine contrast-enhanced CT are usually compromised. On the other hand, MRI is helpful in differentiating the bland and tumor thrombus. Several characters can be used to distinguish the tumor thrombus from the bland one, such as gross direct invasion of tumor parenchyma into the adjacent veins, abnormal contrast enhancement within the thrombus, and irregular venous lumen expansion.2
Chondrosarcoma is a malignant tumor with cells that produce cartilage matrix. Primary chondrosarcoma is the third most common primary malignant tumor of bone, constituting 20% to 27% of all primary malignant osseous neoplasms.19It
predominantly affects middle-aged individuals with a predilection for the proximal femur and pelvis.20Radiographic findings
often suggest the diagnosis of chondrosarcoma because of identification of typical “ring-and-arc” chondroid matrix
mineralization on the plain radiograph and CT and aggressive features of deep endosteal scalloping and soft-tissue extension on the plain radiograph and MRI.19
The histologic features of chondrosarcoma reveal abundant hyaline cartilage stroma with chondrocytes residing in lacunar spaces. The chondrocyte may have a relatively inconspicuous cytoplasm but a various-sized nucleus. The increasing deviation from the appearance of normal hyaline cartilage represents the increasing dedifferentiation of chondrosarcoma and is characterized as increasing overall cellular density, increasing nuclear size, increasing nuclear pleomorphism, presence of bi- and multinucleate chondrocytes, and changes in the density of the extracellular chondroid matrix.20
Several reports have mentioned about the utility of FDG PET in assessment of chondrosarcoma.21–26Many of these
reports have found that there is a wide range of FDG uptake of the chondrosarcoma.21–23In addition, they have also found
that the pathologic grade and prognosis of these tumors are relevant to the degree of FDG uptake. Chondrosarcomas with higher SUV tend to have higher pathologic grade and poorer prognosis.21–23,26
Surgical resection remains the primary and preferred treatment for localized chondrosarcoma. Radiation therapy may play an adjunct role in the treatment of positive surgical margins or palliation of disease-related symptoms. However, the treatment for advanced, metastatic disease is still challenging because the conventional chemotherapy has been proven to be ineffective in most circumstances, but may be considered in variant forms such as mesenchymal or dedifferentiated chondrosarcomas.20
Our case presents a unique picture of chondrosarcoma with huge tumor thrombosis. The whole-body scanning character of FDG PET/CT provides the initial thorough view of disease extent. On the other hand, the MRI reinforces
evidences indicating the malignant nature of these lesions. To the best of our knowledge, the current case is the first reported tumor thrombosis of chondrosarcoma demonstrated on the FDG PET/CT.
Clinical Nuclear Medicine • Volume 36, Number 10, October 2011 Thrombus of Chondrosarcoma on FDG PET/CT