Correspondence: Dr Tun-Jun Tsai, Department of Internal Medi-cine, National Taiwan University Hospital, No. 7 Chung Shan South Road, Taipei 100, Taiwan, R.O.C. Email: [email protected]
Accepted for publication 16 December 2002.
Original Article
Antibiotics induce apoptosis of human peritoneal
mesothelial cells
Cheng-Chung FANG,1 Chung-Jen YEN,2 Tun-Jun TSAI,2 Ruey-Hwa CHEN,3 Po-Huang LEE4 and Yasuhiko TOMINO51Department of Emergency Medicine and 2Internal Medicine, 3Institute of Molecular Medicine, 4Department of Surgery, National Taiwan University Hospital and National Taiwan University College of Medicine, Taipei, Taiwan and 5Division of Nephrology Department of Internal Medicine, Juntendo University School of Medicine, Tokyo, Japan
SUMMARY: The peritoneal mesothelial cell is a critical component of the peritoneal membrane. The intraperitoneal use of several antibiotics to treat bacterial peritonitis is current clinical practice. Our previous study showed that cephalothin (CPL) and cefotaxime (CFT) have cytotoxic effects on human peritoneal mesothelial cells (HPMC), however, the exact mechanism of cytotoxicity has not been elu-cidated. In the present study, flow cytometry, TdT-mediated dUTP nick-end labelling (TUNEL) staining and electron microscopy were used to detect the apoptosis of HPMCs. Immunofluorescent staining was used to evaluate the cytochrome c distribution pattern. Western blotting was used to assess apo-ptotic signalling proteins. We found that CPL (0.5 mg/mL) and CFT (1 mg/mL) induced apoptosis of HPMCs, whereas cefazolin (0.5 mg/mL) and ceftriaxone (0.5 mg/mL) failed to induce apoptosis of HPMCs. While the DNA content of CFT- or CPL-treated cells was reduced, as determined by flow cytometry, cefazolin and ceftriaxone had no such effect. The CFT- or CPL-treated cells displayed the features of apoptosis both under the electron microscope and by using TUNEL staining. However, cefazolin and ceftriaxone produced the same result as the medium controls. Furthermore, CFT and CPL increased the expression of Bax and p53, and caused the translocation of cytochrome c from the mitochondria to the cytoplasm. The HPMC treated by CFT but not by CPL induced the cleavage of procaspase-3 to form active caspase-3. In conclusion, cefotaxime and cephalothin induce apoptosis
of HPMCs in vitro. Signal transduction may be through the mitochondrial pathway.
KEY WORDS: antibiotics, apoptosis, p53, peritoneal mesothelial cell, signalling pathway.
INTRODUCTION
Continuous ambulatory peritoneal dialysis (CAPD) is successfully used as one of the maintenance regimens of end-stage renal disease. The peritoneal mesothelial cell (PMC) covers the entire peritoneal cavity surface and is
a critical component of the peritoneal membrane.1 It
performs many important functions, which are all needed to maintain the peritoneal membrane as a dialysing organ. Peritoneal mesothelial cells form a non-adhesive surface to facilitate movement between
appos-ing tissues. Injuries or infections within the peritoneal cavity cause fibrin to form, and adhesion formation was found to be inversely correlated with the fibrinolytic
activity of the peritoneum.2 The PMC modifies the
release of substances such as plasminogen activator and its inhibitor,3 and its fibrinolytic activity is the key factor
to prevent the formation of fibrous adhesions.4 Another
important function of mesothelial cells involves their role in the host defense mechanism. During peritonitis, bacteria and peritoneal macrophages activate PMCs,
which release chemokines5 and control the peritoneal
immune response by releasing prostaglandins and
cyto-kines such as IL-6, IL-8, MCP-1 and RANTES.6 The
PMCs also serve as antigen-presenting cells to activate
helper T-cells.7 Therefore, the integrity of peritoneal
Antibiotics induce mesothelial cell apoptosis NEPHROLOGY 143
Although the PMC is crucial for CAPD, CAPD itself has detrimental effects on PMCs. Peritoneal membranes undergo many structural and functional changes in
patients who received long-term CAPD treatment.8 One
of the most important changes is peritoneal fibrosis. The pathogenesis of peritoneal fibrosis is not clearly under-stood, but the cytokines released during bacterial perito-nitis may be one of the causes.9 The dialysate10–12 and
drugs13 administered into the peritoneal cavity during
CAPD have toxic effects on PMCs. The high glucose content in the dialysate affects PMCs via various
path-ways and results in extracellular matrix accumulation.14
These facts may partly explain that the severity of
peri-toneal fibrosis correlates with the duration of CAPD.15
Nevertheless, the severity and frequency of bacterial peritonitis during CAPD are more predictable of
long-term membrane survival.16
The most frequent complication of CAPD is bacterial peritonitis. The number of PMC in dialysate effluent
increases during the episode of bacterial peritonitis.17
This implies that the exfoliation of the mesothelium is aggravated during the peritonitis, and that the number of PMC in the peritoneum is decreased. As stated before, PMCs play an important role in peritoneal immune response. Therefore, the use of any agents that might be harmful to the PMCs should be avoided during the course of peritonitis. The use of antibiotics via the intra-peritoneal route is the current recommended treatment for bacterial peritonitis.18 It is therefore important to
know whether these antibiotics have adverse effects on PMCs. Our previous study showed that cephalothin, cefotaxime, cefamandole, and cefuroxime, at the con-centrations of treating CAPD peritonitis via the intrap-eritoneal route, have cytotoxic effects on human
PMCs.19 Cephalothin (CPL) and cefotaxime (CFT) are
the two most obvious antibiotics to be cytotoxic to PMCs, but the exact mechanism of this cytotoxicity has not been elucidated. The present study is designed to clarify the cytotoxic mechanism of these two antibiotics in human PMCs.
Two modes of cell death have been differentiated: apoptosis and necrosis. Apoptotic cell death is an active
process under molecular control.20,21 The regulatory
pro-cess of apoptosis is now a matter of great concern. Apop-totic cells detach from the culture substrata separately and undergo cellular and nuclear shrinkage, but necrotic
cells swell and detach by the sheet.22 According to our
previous observations by light microscopy, cells undergo-ing antibiotic-induced cytotoxicity have the characteris-tic appearance of apoptocharacteris-tic cells. Therefore, we wanted to examine whether antibiotics might induce apoptosis of PMCs. In the present study, we demonstrated that CFT and CPL induced human PMC apoptosis, as opposed to cefazolin and ceftriaxone, which did not induce human PMC apoptosis. Furthermore, we also studied the signalling pathway of the apoptosis induced by CFT and CPL.
METHODS Materials
Trypsin-EDTA, RPMI-1640 medium, Proteinase K, and trypan blue were obtained from Invitrogen Life Technologies (New York, NY, USA). Culture flasks and plates were purchased from Corning (Corning, NY, USA) and precoated with Vigtrogen 100 (Celtrix Laboratory, Palo Alto, CA, USA) before cells were loaded into them. Fetal bovine serum (FBS) was obtained from Biochrom KG (Berlin, Germany). Triton X-100, bovine serum albumin, penicillin, streptomy-cin, insulin, propidium iodide, cefazolin, ceftriaxone, CFT, and CPL were purchased from Sigma (St Louis, MO, USA). Monoclonal anti-bodies to cytochrome c, Bax, and Bcl-2, and horseradish peroxidase-labelled goat antimouse immunoglobulin G (IgG) were purchased from Becton Dickinson Transduction Laboratories (San Diego, CA, USA). Monoclonal antibody to caspase 8 was supplied by Cell Signalling Technology Inc. (Beverly, MA, USA). Monoclonal antibody to p53 was bought from Oncogene Research Products (Boston, MA, USA). Monoclonal antibody to caspase 3 was from the Imgenex Corporation (San Diego, CA, USA). Fluorescein diisothiocyanate (FDIC)-labelled
goat F(ab’)2 fragment to mouse IgG was purchased from DAKO
(Glos-trup, Denmark). Agents used for western blot analysis were from Bio-Rad Laboratories Inc. (Hercules, CA, USA) unless otherwise specified.
Human peritoneal mesothelial cell culture
Specimens of human omentum were obtained from abdominal surgical procedures with the informed consent of the donors. These patients underwent elective abdominal surgery and the omentum was normal. The method of omentum enzymatic disaggregation was used as
previ-ously described.23 Briefly, a piece of omentum was washed in sterile
phosphate buffered saline (PBS) threefold and then incubated with
15 mL of trypsin-EDTA (0.125%) for 20 min at 37∞C with continuous
rotation. After incubation, the omentum and the suspension were
cen-trifuged at 50 g for 5 min at 4∞C. The supernatant was discarded and
the cell pellet was washed once in RPMI-1640 medium containing
20% FBS, penicillin (100 U/mL), streptomycin (100 mg/mL), and
insu-lin (30 mg/mL). After another centrifugation under the same
condi-tions, the cells were resuspended in the same medium and seeded into
a 75-cm2 flask. In 2–4 days, the cells became confluent and were
sub-cultured with medium containing 10% FBS. The cells were initially bipolar or multipolar but became cobblestone-like in appearance upon confluence. By using the immunofluorescence method, HPMC were identified by the presence of vimentin and cytokeratin, and the absence of desmin and factor VIII-related antigen. All experiments listed below were performed in passage 1–3 cells and repeated at least threefold using cells from different subjects.
Flow cytometry
Human peritoneal mesothelial cells were cultured to subconfluence in
a 50-cm2 dish with 10% FBS-containing RPMI. The media were then
changed to 2% FCS-containing RPMI with and without antibiotics (cefazolin (0.5 mg/mL), ceftriaxone (0.5 mg/mL), CFT (1 mg/mL), or CPL (0.5 mg/mL)). After incubations for 40, 48, and 56 h, the cells (including those cells suspended in the medium) were harvested by using trypsinization. Cells were resuspended in PBS at a concentration
of 1 ¥ 106/mL and fixed in 2 mL methanol for 30 min at 4
∞C. After
HPMC were fixed, the mixture was incubated in 0.5 mL of propidium iodide solution (0.05 mg/mL in 3.8 mol/L Na citrate) and 0.5 mL of RNAse A (0.5 mg/mL) at room temperature for 30 min. Finally, the
HPMC were resuspended in 1 mL PBS and analysed by using flow cytometry (FACScan; Coulter, Fullerton, CA, USA) according to the manufacturer’s instructions. The cells in the subdiploid peak were
considered as apoptotic.24
In situ detection of apoptosis
Human peritoneal mesothelial cells were cultured to subconfluence in a four-chamber slide with 10% FBS-containing RPMI. The media was then changed to 2% FBS-containing RPMI with and without antibi-otics (cefazolin (0.5 mg/mL), ceftriaxone (0.5 mg/mL), CFT (1 mg/ mL), or CPL (0.5 mg/mL)). After incubation for 48 h, the cells were fixed by 4% paraformaldehyde. Apoptotic cells were detected by using
a fluorescence in situ cell-death detection kit (Roche Molecular
Bio-chemicals, Mannheim, Germany). This kit uses terminal deoxynucle-otidyltransferase (TdT) for the incorporation of labelled nucleotides (or the TUNEL (TdT-mediated dUTP nick-end labelling) technique)
into DNA strand breaks in situ. Fluorescein labels incorporated in
nucleotide polymers are detected and quantified by using fluorescence microscopy. For evaluation by fluorescence microscopy, an excitation wavelength of 455 nm and detection wavelength of 510 nm are used. Apoptosis is defined by morphological criteria. Cells containing
frag-mented nuclear chromatin will exhibit bright green nuclear staining.25
Transmission electron microscopy
Human peritoneal mesothelial cells were cultured to subconfluence in
a 50-cm2 dish with 10% FBS-containing RPMI. The medium then was
changed to 2% FBS-containing RPMI with and without antibiotics (cefazolin (0.5 mg/mL), ceftriaxone (0.5 mg/mL), CFT (1 mg/mL), or CPL (0.5 mg/mL)). After incubation for 48 h, the cells (including cells suspended in the medium) were trypsinized and fixed. The cells were then processed for examination under the electron microscope.
Western blotting
Human peritoneal mesothelial cells were cultured to subconfluence in
a 50-cm2 dish with 10% FBS-containing RPMI. The media was then
changed to 2% FBS-containing RPMI with and without antibiotics (CFT (1 mg/mL) or CPL (0.5 mg/mL)). After incubations for 40, 48, and 56 h, the cells (including cells suspended in the medium) were lysed by ice-cold lysing solution (65 mmol/L Tris base, pH 8.0, contain-ing 154 mmol/L NaCl, 1 mmol/L EDTA, 1% (octylphenoxy)poly-ethoxyethanol, 1 mmol/L phenylmethanesulfonyl fluoride, leupeptin
(1 mg/mL), pepstatin (1 mg/mL), aprotinin (1 mg/mL), and 0.25% Na
deoxycholate). Samples were rotated for 15 min at 4∞C and then
cen-trifuged at 12 000 g for 5 min at 4∞C. The supernatant was recovered,
and protein concentration was measured by using the bicinchoninic acid assay (Bio-Rad), with bovine serum albumin as the standard.
Sam-ples were incubated for 5 min at 95∞C in loading buffer (12 mmol/L
Tris-HCl, pH 6.8, with 25% glycerol, 2% sodium dodecyl sulfate, 14.4 mmol/L 2-mercaptoethanol, and 0.1% bromophenol blue), and
50 mg of protein were loaded on SDS-polyacrylamide gels of different
percentages (and exclusion limits) corresponding to the molecular weight of the target proteins. After electrophoresis, the proteins were transferred to polyvinylidene difluoride membrane by electroblotting. The membrane was blocked in 1% BSA/0.05%Tween/PBS solution
overnight at 4∞C. Mouse antihuman monoclonal antibodies to Bcl-2,
Bax, p53, caspase 8 or caspase 3 were used as primary antibodies. A horseradish peroxidase-labelled goat antimouse IgG was used as a
sec-ondary antibody. Blots were developed by incubation in a chemilumi-nescence substrate and were exposed to X-ray films.
Immunofluorescent stain
Human peritoneal mesothelial cells were cultured to subconfluence in a four-chamber slide with 10% FBS-containing RPMI. The media were then changed to 2% FCS-containing RPMI with and without antibi-otics (CFT (1 mg/mL) or CPL (0.5 mg/mL)). After incubation for 48 h, the cells were fixed by using 4% paraformaldehyde. Cells were perme-abilized with 0.2% Triton X-100 and then blocked by 10% FBS in PBS. Cells were incubated with mouse antihuman cytochrome c antibody and then with FDIC-labelled antimouse IgG antibody. Slides were observed under a fluorescence microscope, using an excitation wave-length of 455 nm and a detection wavewave-length of 510 nm.
Statistical analysis
All data are expressed as mean ± SEM. The comparison of drug effects
was conducted by using a Student’s t-test. A P-value less than 0.05 was
considered to be significant.
RESULTS
To correlate the clinical situation, the antibiotics were
tested in vitro by adding the same concentrations as
sug-gested by the Ad Hoc Advisory Committee on
Peritoni-tis Management18,26 to the dialysate. According to our
previous study,19 CFT (1 mg/mL) and CPL (0.5 mg/mL)
have cytotoxic effects on HPMCs. Cefazolin, which is the same as CPL, is a first generation cephem, and was chosen to compare against CPL. Ceftriaxone, which is the same as CFT, is a third generation cephem, and was chosen to compare against CFT. Both cefazolin (0.5 mg/mL) and ceftriaxone (0.5 mg/mL) are not toxic
to HPMC according to our previous report.19 After
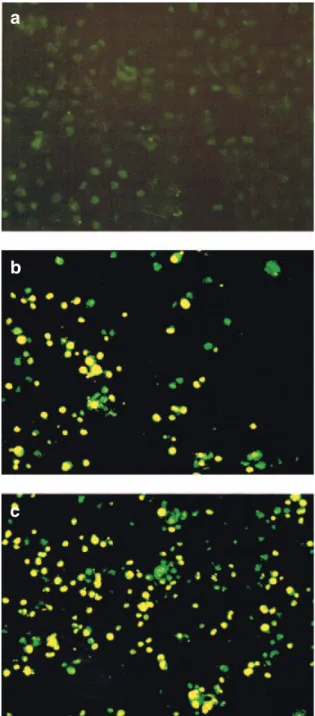
incu-bating with CFT for 48 h or CPL for 40 h, the DNA content of HPMCs became noticeably reduced, whereas cefazolin or ceftriaxone did not have such an effect. To determine the amount of DNA in each cell, flow cytom-etry was used with propidium iodide staining. The per-centages of subdiploid (apoptotic) cells over time are shown in Table 1. In addition to the flow cytometry technique, the antibiotics-induced apoptosis could also be demonstrated by using TUNEL staining. The nuclei of HPMCs displayed bright green fluorescence after 48 h of CFT or CPL treatment, but cefazolin- or ceftriaxone-treated cells showed faint fluorescent staining of the nuclei, similar to the medium controls (Fig. 1). After 48 h of CFT or CPL treatment, the apoptotic features (such as condensation of the nuclear chromatin, wrin-kling of the nuclear membrane, dilation of endoplasmic reticulum, and relatively normal structure of the mitochondria) can also be verified by using electron microscopy (Fig. 2). The cells treated with cefazolin or ceftriaxone for 48 h had the same result as the medium
Antibiotics induce mesothelial cell apoptosis NEPHROLOGY 145
controls, which did not display ultrastructural changes of apoptosis. All these data indicated that CFT (1 mg/mL) and CPL (0.5 mg/mL) could induce the apoptosis of HPMCs, whereas cefazolin or ceftriaxone failed to induce apoptosis of HPMCs.
After the findings of HPMC apoptosis were con-firmed, we further studied the signalling pathway of apoptosis induced by CFT and CPL. First, we examined several proteins involved in apoptosis by Western blot-ting. The protein level of Bcl-2 did not alter, but Bax and p53 expression increased after CFT or CPL treatment (Fig. 3). The procaspase-3 (32 kDa) expression did not change significantly. While the active forms of caspase-3 (17 and 12 kDa) were produced after the treatment with CFT, the CPL treatment did not generate the same active form (Fig. 4). The expression of the caspase 8 active form did not change after CFT or CPL treatment (Fig. 5). Second, the results of immunofluorescence staining could discern a change in the distribution of cytochrome c after treatment with CFT or CPL. Cyto-chrome c is generally found normally distributed within the mitochondria, and therefore under normal condi-tions, the mitochondria are stained while the nuclei remained unstained (Fig. 6a). In contrast, after the treat-ment of HPMC with CFT or CPL, cytochrome c was released into the cytoplasm and the whole cells, includ-ing the nuclei, were covered by fluorescent stain (Fig. 6b,c).
DISCUSSION
It is well known that peritoneal dialysate10,12 and drugs13
used in CAPD have adverse effects on HPMCs. How-ever, there are few studies examining the induction of
apoptosis by these agents in HPMC.11,27 The present
study demonstrated that CFT and CPL induced HPMC
apoptosis in vitro, whereas cefazolin and ceftriaxone did
not. When we consider the important functions of the HPMC, with the same antimicrobial activity, cefazolin
Table 1 Percentages of human peritoneal mesothelial cells (HPMC) in sub-G1 group (apoptosis) after treatment with cefazolin, ceftriaxone, cefotaxime or cephalothin for various time periods
Hours after incubation
40 48 56 Control 1.8 ± 0.4 2.6 ± 0.6 3.3 ± 0.6 Cefazolin (0.5 mg/mL) 1.8 ± 0.5 2.7 ± 0.5 2.8 ± 0.5 Ceftriaxone (0.5 mg/mL) 1.7 ± 0.4 2.6 ± 0.3 2.3 ± 0.7 Cefotaxime (1 mg/mL) 6.6 ± 1.5 11.6 ± 2.4* 13.2 ± 2.5* Cephalothin (0.5 mg/mL) 8.2 ± 1.0* 14.6 ± 1.7* 23.8 ± 4.0*
Data are expressed as mean ± SEM. n= 3; *P < 0.05 versus the
control.
Fig. 1 Antibiotic-induced apoptosis was demonstrated by the TdT-mediated dUTP nick-end labelling (TUNEL) staining. The control cells showed faint fluorescent staining of the nuclei (a). The nuclei of the human peritoneal mesothelial cells (HPMC) displayed bright green fluorescence after 48 h of exposure to (b) cefotaxime (CFT; 1 mg/mL) or (c) cephalothin (CPL; 0.5 mg/mL) treatment. The cells treated by cefazolin (0.5 mg/mL) or ceftriaxone (0.5 mg/mL) for 48 h showed the same results as the control (data not shown).
a
b
and ceftriaxone would be the better choices with regards to the treatment of bacterial peritonitis via the intrap-eritoneal route. At present, no animal or clinical studies have been conducted to compare the differences regard-ing the short- or long-term membrane functions between the two groups of antibiotics. Our study warrants an
in vivo research regarding the relationship between the
cytotoxicity of antibiotics and peritoneal membrane function.
The signalling pathway of apoptosis on HPMC has not been studied. In general, the signalling pathway of apoptosis is complex, but can be divided largely into a Fas/Fas ligand and a mitochondrial pathway (reviewed in21). The tumour suppressor p53 is a transcriptional
fac-tor that is involved in apoptosis partly by inducing Bax expression.28,29 Bax is a death promoter, which is
neutral-ized by heterodimerization with Bcl-2. Bax translocates into the outer mitochondrial membrane and then a leakage of cytochrome c from the mitochondria into the
cytosol follows.30 Caspase-9 and caspase-3 are activated
sequentially, and this event then leads to the breakdown of chromosomal DNA. In the present study, we first dem-onstrated that CFT and CPL induced the apoptosis of HPMC at the concentration that was administered
intra-peritoneally to our CAPD patients. It was then found that the CFT and CPL increased the expression of p53 and Bax, while the expression of Bcl-2 was only slightly changed. We also demonstrated that cytochrome c was released from the mitochondria into the cytoplasm. After treatment of CFT or CPL, caspase 8 was not acti-vated; this precluded the Fas/Fas ligand pathway involv-ment. All these data support the hypothesis that the signalling of apoptosis induction by CFT and CPL is through the mitochondrial pathway.
Caspases belong to a family of cysteine proteases. They are essential components of a proteolytic cascade that is involved in the execution stages of apoptosis. Our data regarding caspase-3 activation by these two antibi-otics were different. Cefotaxine clearly induced the expression of an active form of caspase-3, whereas CPL did not. Although caspase-3 was thought of as the com-mon executive protease during apoptosis, several studies have demonstrated that caspase-3 is dispensable in
apo-ptosis (reviewed in31). Recently, the study of
caspase-3-deficient cells showed that caspase-3 deficiency does
not affect Bax-induced apoptosis.32 Our data on
CPL-induced apoptosis further confirmed that apoptosis may occur without caspase-3 activation.
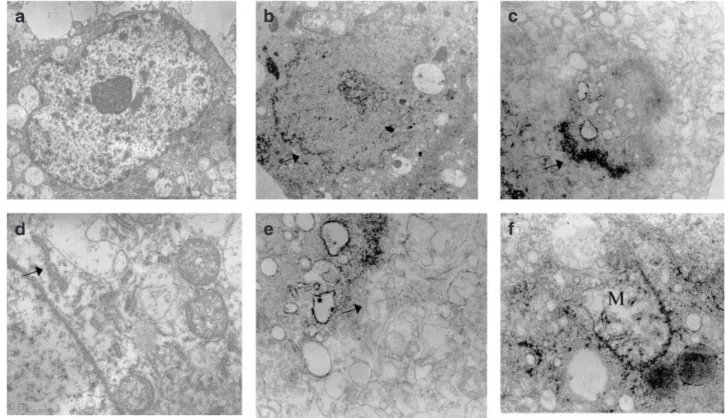
Fig. 2 After a 48 h incubation with and without cefotaxime (CFT; 1 mg/mL; the same picture was noted after treatment with ceph-alothin (CPL; 0.5 mg/mL)), the human peritoneal mesothelial cells (HPMC) were examined by electron microscopy. The control cell displayed a (a) normal nucleus and an endoplasmic reticulum (arrow in Fig. 2d). The CFT-treated cells showed wrinkling of the nuclear membrane (arrow in Fig. 2b), condensation of the nuclear chromatin (arrow in Fig. 2c), dilation of the endoplasmic reticulum (arrow in Fig. 2e), and the relatively normal structure of the mitochondria (M in Fig. 2f).
a
b
c
Antibiotics induce mesothelial cell apoptosis NEPHROLOGY 147
To the best of our knowledge, there is no previous report on the cytotoxicity of CFT and CPL. In the liter-ature, cephaloridine is the most frequently studied ceph-alosporin known to induce toxicity. Cephaloridine has
been shown to deplete renal glutathione33 and reduce
tubular cell numbers and mitochondrial carnitine trans-port (i.e. it is toxic to mitochondrial fatty acid
metabo-lism).34 Our data suggested that CFT and CPL induced
apoptosis by affecting mitochondria. It is reasonable to propose that CFT and CPL might affect mitochondrial redox status. The effects of CFT and CPL on mitochon-drial oxidative and fatty acid pathways in HPMC warrant further study.
In conclusion, cefotaxime and cephalothin induce
apoptosis of human peritoneal mesothelial cells in vitro.
The signalling transduction may be through the mito-chondrial pathway.
ACKNOWLEDGEMENTS
This study was supported by a grant from The National Science Council, NSC 90–2314-B-002–269, Ta-Tung Kidney Foundation and the Mrs Hsiu-Chin Lee Kidney Research Fund. Part of the study has been presented in poster form at the ASN/ISN World Congress of Neph-rology, in San Francisco, October 2001. The authors wish to thank Professor Wan-Yu Chen, Professor Min-Liang Kuo, Dr Chien-Chen Tsai, Ms. Shu-Ying Chou, Ms. Chen-Chih Chang, and Ms. Su-Li Hung for their kind assistance.
Fig. 3 After 40–56 h of incubation with cefotaxime (CFT; 1 mg/mL) or cephalothin (CPL; 0.5 mg/mL), the protein expressions of (a) Bcl-2, (b) Bax, and (c) p53 were examined by using western blotting. Lanes 1, 2 and 3 represent the control, CFT and CPL treatment for 40 h, respectively. Lanes 4, 5 and 6 represent the control, CFT and CPL treatment for 48 h, respectively. Lanes 7, 8 and 9 represent the control, CFT and CPL treatment for 56 h, respectively. Data are expressed as mean ± SEM. n = 3, *P < 0.05 versus the control.
(a)
(b)
(c)
Fig. 4 After 40–56 h of incubation with cefotaxime (CFT; 1 mg/mL) or cephalothin (CPL; 0.5 mg/mL), the protein expressions of procaspase 3 (32 kDa) and active forms of caspase 3 (17 and 12 kDa) were examined by using Western blotting. Lanes 1, 2 and 3 represent the control, CFT and CPL treatment for 40 h, respectively. Lanes 4, 5 and 6 represent the control, CFT and CPL treatment for 48 h, respectively. Lanes 7, 8 and 9 represent the control, CFT and CPL treatment for 56 h, respectively. Data are expressed as mean ± SEM. n = 3,
*P < 0.05 versus the control.
Fig. 5 After 40–56 h of incubation with cefotaxime (CFT; 1 mg/mL) or cephalothin (CPL; 0.5 mg/mL), the protein expressions of active forms of caspase 8 (18 kDa) were exam-ined by using western blotting. Lanes 1, 2 and 3 represent the control, CFT and CPL treatment for 40 h, respectively. Lanes 4, 5 and 6 represent the control, CFT and CPL treatment for 48 h, respectively. Lanes 7, 8 and 9 represent the control, CFT and CPL treatment for 56 h, respectively. Data are expressed as mean ± SEM, n = 3.
REFERENCES
1. Nagy JA. Peritoneal membrane morphology and function. Kidney
Int. 1996; 50 (Suppl. 56): S2–11.
helial cells. Blood 1990; 75: 1490–7.
4. Raftery AT. Regeneration of peritoneum: a fibrinolytic study. J.
Anat. 1979; 129: 659–64.
5. Topley N, Liberek T, Davenport A, Li FK, Fear H, Williams JD. Activation of inflammation and leukocyte recruitment into the peritoneal cavity. Kidney Int. 1996; 50 (Suppl. 56): S17–21. 6. Topley N. The cytokine network controlling peritoneal
inflamma-tion. Perit. Dial. Int. 1995; 15 (Suppl. 7): S35–40.
7. Rapoport J, Hausmann MJ, Chaimovitz C. The peritoneal immune system and continuous ambulatory peritoneal dialysis.
Nephron 1999; 81: 373–80.
8. Krediet RT. The peritoneal membrane in chronic peritoneal dial-ysis. Kidney Int. 1999; 55: 341–56.
9. Dobbie JW, Anderson JD, Hind C. Long-term effects of peritoneal dialysis on peritoneal morphology. Perit. Dial. Int. 1994; 14 (Suppl. 3): S16–20.
10. Brunkhorst R, Mahiout A. Pyruvate neutralizes peritoneal dialysis cytotoxicity: Maintained integrity and proliferation of cultured human mesothelial cells. Kidney Int. 1995; 48: 177–81. 11. Yang AH, Chen JY, Lin YP, Huang TP, Wu CW. Peritoneal
dialysis solution induces apoptosis of mesothelial cells. Kidney Int. 1997; 51: 981–99.
12. Pedersen FB. Biocompatibility studies with bicarbonate-based solutions. Adv. Perit. Dial. 1994; 10: 245–50.
13. Tsai TJ, Yen CJ, Fang CC, Yang CC, Lee PH, Yen TS. Effect of intraperitoneal agents on human peritoneal mesothelial cell growth. Nephron 1995; 71: 23–8.
14. Ha H, Lee HB. Peritoneal mesothelial cell biology in peritoneal dialysis. Nephrology 2002; 7: 220–6.
15. Williams JD, Craig KJ, Topley N et al. Morphologic changes in the peritoneal membrane of patients with renal disease. J. Am.
Soc. Nephrol. 2002; 13: 470–9.
16. Davies SJ, Bryan J, Phillips L, Russell GI. Longitudinal changes in peritoneal kinetics: The effects of peritoneal dialysis and peritoni-tis. Nephrol. Dial. Transplant. 1996; 11: 498–506.
17. Lai K, Lai K, Lam C, Chan T, Li F, Leung J. Changes of cytokine profiles during peritonitis in patients on continuous ambulatory peritoneal dialysis. Am. J. Kidney Dis. 2000; 35: 644–52. 18. Keane WF, Bailie GR, Boeschoten E et al. Adult peritoneal
dialysis-related peritonitis treatment recommendations: 2000 update. Perit. Dial. Int. 2000; 20: 396–411.
19. Yen CJ, Tsai TJ, Chen HS et al. Effects of intraperitoneal antibi-otics on human peritoneal mesothelial cell growth. Nephron 1996;
74: 694–700.
20. Fiers W, Beyaert R, Declercq W, Vandenabeele P. More than one way to die: apoptosis, necrosis and reactive oxygen damage.
Onco-gene 1999; 18: 7719–30.
21. Saikumar P, Dong Z, Mikhailov V, Denton M, Weinberg JM, Venkatachalam MA. Apoptosis: definition, mechanisms, and relevance to disease. Am. J. Med. 1999; 107: 489–506. 22. Lieberthal W, Triaca V, Levine J. Mechanisms of death induced by
cisplatin in proximal tubular epithelial cells: apoptosis vs. necrosis.
Am. J. Physiol. 1996; 270: F700–8.
23. Fang CC, Yen CJ, Chen YM et al. Hydralazine inhibits human peritoneal mesothelial cell proliferation and collagen synthesis.
Nephrol. Dial. Transplant. 1996; 11: 2276–81.
Fig. 6 Distribution of cytochrome c was changed after treat-ment with cefotaxime (CFT) or cephalothin (CPL). The fluorescent stain remained in the mitochondria while failing to stain the nuclei of control cells (a). After the treatment of human peritoneal mesothelial cells (HPMC) with (b) CFT (1 mg/mL) or (c) CPL (0.5 mg/mL) for 48 h, cytochrome c was released into the cytoplasm, causing the fluorescent stain to cover the whole cells, including their nuclei.
b
Antibiotics induce mesothelial cell apoptosis NEPHROLOGY 149
24. Zamai L, Falcieri E, Zauli G, Cataldi A, Vitale M. Optimal detec-tion of apoptosis by flow cytometry depends on cell morphology.
Cytometry 1993; 14: 891–7.
25. Gavrieli Y, Sherman Y, Ben-Sasson SA. Identification of pro-grammed cell death in situ via specific labeling of nuclear DNA fragmentation. J. Cell Biol. 1992; 119: 493–501.
26. Keane WF, Alexander SR, Bailie GR, Boeschoten E, Gokal R, Golper TA. Peritoneal dialysis-related peritonitis treatment rec-ommendations: 1996 update. Perit. Dial. Int. 1996; 16: 557–73. 27. Zheng ZH, Ye RG, Bergstrom J, Lindholm B. Effect of dialysate
composition on the apoptosis and proliferation of human perito-neal mesothelial cells and protein expression of Fas and c-Myc.
Adv. Perit. Dial. 2000; 16: 31–5.
28. Stewart ZA, Pietenpol JA. p53 Signaling and cell cycle check-points. Chem. Res. Toxicol. 2001; 14: 243–63.
29. Amundson SA, Myers TG, Fornace AJ Jr. Roles for p53 in growth arrest and apoptosis: putting on the brakes after genotoxic stress.
Oncogene 1998; 17: 3287–99.
30. Rosse T, Olivier R, Monney L et al. Bcl-2 prolongs cell survival after Bax-induced release of cytochrome c. Nature 1998; 391: 496– 9.
31. Donovan M, Carmody RJ, Cotter TG. Light-induced photorecep-tor apoptosis in vivo requires neuronal nitric-oxide synthase and guanylate cyclase activity and is caspase-3-independent. J. Biol.
Chem. 2001; 276: 23 000–8.
32. Kagawa S, Gu J, Honda T et al. Deficiency of caspase-3 in MCF7 cells blocks Bax-mediated nuclear fragmentation but not cell death. Clin. Cancer Res. 2001; 7: 1474–80.
33. Kuo C-H, Hook JB. Depletion of renal glutathione content and nephrotoxicity of cephaloridine in rabbits, rats, and mice. Toxicol.
Appl. Pharmacol. 1982; 63: 292–302.
34. Tune BM, Hsu CY. Toxicity of cephaloridine to carnitine transport and fatty acid metabolism in rabbit renal cortical mitochondria: structure-activity relationships. J. Pharmacol. Exp.