Title: Effects of Enzyme Replacement Therapy for Cardiac type Fabry Patients with
a Chinese Hotspot Late-onset Fabry Mutation (IVS4+919G>A)
Authors:
Hsiang-Yu Lin1,2,4†, Hao-Chuan Liu3,4†, Yu-Hsiu Huang1,3,4, Hsuan-Chieh Liao1,4,5, Ting-Rong Hsu1,3,4, Chia-I Shen3,4, Shao-Tzu Li3,4, Cheng-Fang Li3,4, Li-Hong Lee4,6, Pi-Chang Lee3, Chun-Kai Huang3,4, Chuan-Chi Chiang4,5, Ching-Yuang Lin4,7,8, Shuan-Pei Lin2, Dau-Ming Niu1,3,4*
Institutions:
1Institute of Clinical Medicine, National Yang-Ming University, Taipei, Taiwan; 2Department of Pediatrics, Mackay Memorial Hospital, Taipei, Taiwan; Mackay Medicine, Nursing and Management College, Taipei, Taiwan; and Department of Medicine, Mackay Medical College, New Taipei City, Taiwan; 3Department of Pediatrics, Taipei Veterans General Hospital, Taipei, Taiwan; 4Taiwan Clinical Trial Consortium in Fabry Disease; 5Neonatal Screening Center, Chinese Foundation of Health, Taipei, Taiwan; 6Nursing Department, Taipei Veterans General Hospital, Taipei, Taiwan; 7Clinical Immunological Center, China Medical University Hospital, Taichung, Taiwan; 8College of Medicine, China Medical University, Taichung, Taiwan
†Hsiang-Yu Linand Hao-Chuan Liu contributed equally to this study.
E-mail address: [email protected]
Dr. Dau-Ming Niu, Department of Pediatrics, Taipei Veterans General Hospital, No. 201, Section 2, Shih-Pai Road, Taipei 112, Taiwan
Acknowledgements
This study was partially supported by the National Science Council, Taiwan (No. NSC-100-2325-B-010-014, NSC-98-2917-I-010-103) and Taipei Veterans General Hospital (No. V101C-129). The authors thank Ms. Tsai-Feng Ho for her professional assistance in biostatistics. Shire HGT was given the opportunity to review this manuscript, but the opinions remain those of the authors.
Contributors
HYL and HCL performed acquisition, statistical analysis and interpretation of data, and drafting of the manuscript. DMN and YHH participated in design of the study, interpretation of the data and helped to draft the manuscript. HCL, TRH, CKH, and CCC performed biochemical analyses and revised the manuscript. CIS, STL, CFL, LHL, PCL, CYL, and SPL were responsible for patient screening. All authors contributed in interpreting data, revising drafts of the manuscript and in approval of the final manuscript.
Funding
This study was partially supported by the National Science Council, Taiwan (No. NSC-100-2325-B-010-014, NSC-98-2917-I-010-103) and Taipei Veterans General Hospital (No. V101C-129).
Competing interests
Patient consent
Obtained.
Ethics approval
Institute’s ethics committee.
Provenance and peer review
Not commissioned; externally peer reviewed.
Data sharing statement
Abstract
Objective: Current studies of newborn screening for Fabry disease in Taiwan have
revealed a remarkably high prevalence of cardiac type Fabry disease with a Chinese hotspot late-onset Fabry mutation (IVS4+919G>A).
Design: Retrospective cohort study. Setting: Tertiary medical center.
Participants: 21 patients with cardiac type Fabry disease (15 males and 6 females) as
well as 15 patients with classic Fabry disease (4 males and 11 females) treated with biweekly intravenous infusions of agalsidase beta (1 mg/kg) or agalsidase alpha (0.2 mg/kg) for at least 6 months.
Outcome measures: The data were collected at the time before enzyme replacement
therapy (ERT) began and followed up after ERT for at least 6 months, including patient demographics, medical history, parameter changes of cardiac status and renal function, plasma globotriaosylsphingosine (lyso-Gb3), and Mainz Severity Score Index.
Results: After 6-39 months of ERT, plasma lyso-Gb3 was found reduced in 89%
(17/19) and 93% (14/15) of patients with cardiac and classic types, respectively, indicated the improvement of the disease severity. For patients with cardiac type Fabry disease, echocardiography revealed reduction or stabilization of left ventricular mass index (LVMI), the thicknesses of intraventricular septum (IVS), and left
posterior wall (LPW) in 83% (15/18), 83% (15/18), and 67% (12/18) of patients, respectively; as well as 77% (10/13), 73% (11/15), and 60% (9/15) for those with the classic type. Most patients showed stable renal function after ERT. There were statistically significant improvements (p<0.05) between the data at baseline and those after ERT for values of plasma lyso-Gb3, LVMI, IVS, LPW, and Mainz Severity Score Index. No severe clinical events were reported during the treatment.
Conclusions: ERT is beneficial and appears to be safe for Taiwanese patients with
cardiac type Fabry disease, as well as for those with the classic type.
Key words: enzyme replacement therapy; Fabry disease; IVS4+919G>A;
globotriaosylsphingosine; hypertrophy
Running heads: Enzyme replacement therapy for cardiac type Fabry patients Abbreviations
ACR, albumin-to-creatinine ratio; α-Gal A, α-galactosidase A; eGFR, estimated glomerular filtration rate; ERT, enzyme replacement therapy; Gb3, globotriaosylceramide; IVS, intraventricular septum; LPW, left posterior wall; LVH, left ventricular hypertrophy; LVM, left ventricular mass; LVMI, left ventricular mass index; lyso-Gb3, globotriaosylsphingosine; MSSI, Mainz Severity Score Index
Article summary
Article focus
■ Retrospectively reviewed the clinical findings of enzyme replacement therapy
(ERT) in 21 Taiwanese patients with cardiac type Fabry disease (IVS4+919G>A), along with 15 patients with the classic type.
■ Evaluation of the safety and effects on disease stability for these patients under ERT.
Key messages
■ ERT improved or stabilized cardiac status, stabilized renal function, improved microalbuminuria, stabilized or improved overall severity of signs and symptoms according to Mainz Severity Score Index, while reducing plasma globotriaosylsphingosine concentration.
■ ERT is beneficial and appears to be safe for Taiwanese patients with cardiac type Fabry disease (IVS4+919G>A), as well as for those with the classic type.
Strengths and limitations of this study
■ The first report to demonstrate the efficacy and safety of ERT with agalsidase beta or agalsidase alfa in patients with cardiac type Fabry disease and a relatively large cohort study.
INTRODUCTION
Fabry disease (MIM 301500) is an X-linked inherited condition caused by absence or reduction of α-galactosidase A (α-Gal A) activity in lysosomes, leading to progressive accumulation of globotriaosylceramide (Gb3) and other neutral glycosphingolipids in lysosomes of all cells in the body. It is a complex, multisystemic disorder characterized clinically by acroparesthesias, hypohydrosis, angiokeratomas, corneal opacities, cardiomyopathy, progressive renal impairment, gastrointestinal disturbances, and cerebrovascular lesions.1 The first symptoms of classic Fabry disease usually appear in childhood, and by middle age, some degree of irreversible damage may already have occurred. Despite being an X-linked disorder, heterozygous females can be as severely affected as hemizygous males, although the range of symptoms varies widely. Life-threatening complications may develop in treated and untreated patients. The estimated incidence of classic Fabry disease is 1 in 40,000-117,000 live births in the general population.1-3
During the past decade, late-onset phenotypes of Fabry disease primarily involving the heart4-6, kidneys7-9 or cerebrovascular system10 have been reported. Patients with the cardiac variant often lack the classic symptoms of Fabry disease and present with left ventricular hypertrophy (LVH), arrhythmias, or hypertrophic cardiomyopathy in the fifth to eighth decades of life. Newborn screening for Fabry disease in Taiwan
revealed a surprisingly high incidence (about 1 in 1,500 males) of a cardiac variant
GLA mutation, IVS4+919G>A, in our population, and also found this mutation in a
number of adult patients with idiopathic hypertrophic cardiomyopathy. As a result, dozens of Taiwanese patients with cardiac type Fabry disease were identified in the recent years.11-13
There are two forms of enzyme replacement therapy (ERT) for Fabry disease: agalsidase alfa (Replagal®; Shire Human Genetic Therapies, Lexington, MA) and agalsidase beta (Fabrazyme®; Genzyme, Cambridge, MA). Previous studies showed that ERT was an effective treatment for neuropathic pain14 and can stabilize renal function, or at least, slow the decline of renal function in many patients with Fabry nephropathy15-22 and stabilize or improve surrogate parameters like cardiac size in those with cardiomyopathy.18,23-26 However, most study subjects were Caucasian patients with classic Fabry disease. Information on ERT in patients with cardiac type Fabry disease as well as in Asian patients is limited.27-29 In this study, we
retrospectively reviewed the clinical findings of ERT in 21 Taiwanese patients with cardiac type Fabry disease (IVS4+919G>A), along with 15 patients with the classic type. Our aim was to evaluate the safety and effects on disease stability for these patients under ERT.
PATIENTS AND METHODS Selection of subjects
Data from 21 patients with cardiac type Fabry disease (15 males and 6 females; age range, 25 to 67 years) and 15 patients with classic Fabry disease (4 males and 11 females; age range, 14 to 79 years) treated with biweekly intravenous infusions of agalsidase beta (1 mg/kg) or agalsidase alpha (0.2 mg/kg) for at least 6 months between December 2008 and June 2012 in Taipei Veterans General Hospital were retrospectively reviewed for this study. Seven of these 36 patients (patients No. 2, 3, 12, 15, 16, 18, 19) initially received agalsidase beta (1 mg/kg) treatment. However, since June 2009, viral contamination of Genzyme’s production facility resulted in a worldwide shortage of agalsidase beta leading to the switch to agalsidase alfa for these 7 patients with Fabry disease in Taiwan.30 All other 29 patients received only agalsidase alpha (0.2 mg/kg) throughout the treatment course. The patients’ ages when treatment began ranged widely, from 14 to 79 years, and the duration of ERT ranged from 6 to 39 months. Written informed consent was obtained from a parent for children and from patients over 18 years. The study was approved by the medical ethics committee of Taipei Veterans General Hospital, Taiwan.
Baseline and follow-up biochemical and clinical evaluation
All patients had clinical manifestations of the disease, and diagnosis was confirmed by plasma α-Gal A enzyme activity assay and GLA gene mutation analysis.11,12 The
data were collected retrospectively at the time before ERT began and followed up after ERT for at least 6 months, including patient demographics, such as gender, genotype, age at ERT, height and body weight, and medical history. Together with the relevant data pertaining to the left ventricular mass (LVM), left ventricular mass index (LVMI), the thicknesses of the intraventricular septum (IVS) and left posterior wall (LPW) obtained by serial echocardiographic assessments31-34, urine albumin-to-creatinine ratio (ACR), estimated glomerular filtration rate (eGFR) (based on serum creatinine concentration)35, plasma globotriaosylsphingosine (lyso-Gb3) concentration36,37, and severity of signs and symptoms of Fabry disease using the Mainz Severity Score Index (MSSI)38 were recorded. LVM was calculated according to the American Society of Echocardiography simplified cubed equation. LVM was indexed (LVMI) by height2.7 to normalize heart size to body size. LVH was defined as an LVMI higher than the upper normal limit (men, >51 g/m2.7; women, >48 g/m2.7). 31-34Microalbuminuria was defined as urinary albumin-to-creatinine ratio ≥2.0 mg/mmol
for men and ≥2.8 mg/mmol for women on at least two occasions, based on the National Kidney Foundation's Kidney Disease Outcome Quality Initiative working group definition.39 Adverse events were assessed by history; physical examination,
including vital signs during treatment; patient records of side effects; laboratory tests (chemistry, hematology, urinalysis); and electrocardiography.
Data analysis and statistics
Descriptive statistics, including means, standard deviations, and percentage change over time, were calculated. Changes in plasma lyso-Gb3, eGFR, urine ACR, LVM, LVMI, IVS, LPW, and MSSI before and after treatment were analyzed using Student’s paired t test. SPSS version 11.5 (SPSS Inc, Chicago, IL, USA) was used, and differences were considered to be statistically significant when the p value was < 0.05.
RESULTS Demographics
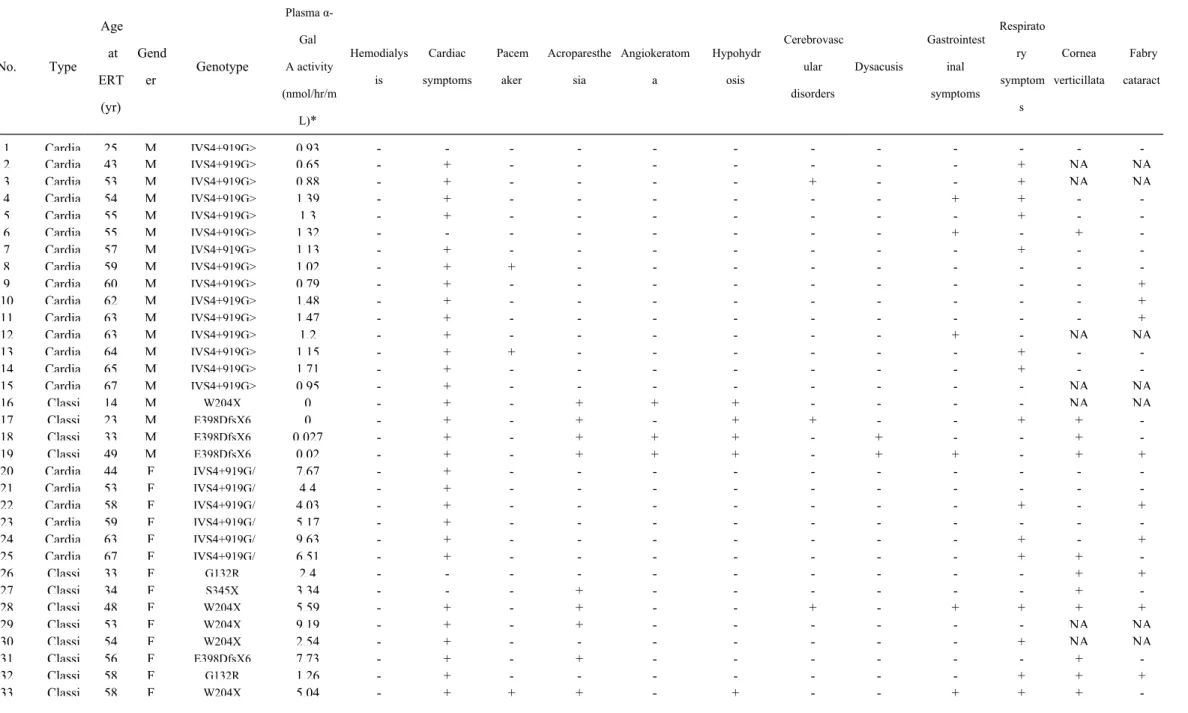
Details of the 36 patients’ backgrounds and clinical characteristics are shown in Table 1. The age at start of ERT was 53.4 ± 14.4 years. For cardiac type Fabry patients, the mean plasma α-Gal A activity for males and females were 1.16 and 6.24 nmol/hr/mL, respectively (reference range: 7.9 to 16.9 nmol/hr/mL). For classic Fabry patients, those were 0.01 and 4.66 nmol/hr/mL, respectively. No patient underwent hemodialysis. Thirty-two patients suffered from cardiac symptoms, and 3 of them underwent pacemaker implantation. Among 15 classic Fabry patients, 4 males and 7 females had acroparesthesia, 3 males had angiokeratoma, and 1 female and 4 males had hypohydrosis. Cerebrovascular disorders were present in 1 cardiac male, 1 classic male, and 2 classic females. Dysacusis, gastrointestinal symptoms, and respiratory symptoms were described in 2, 8, and 17 patients, respectively. Among 28 patients receiving slit-lamp examinations of the eye, 13 and 10 patients were found with cornea verticillata and Fabry cataract, respectively.
Cardiac status, renal function, plasma lyso-Gb3 concentration, and MSSI at baseline and after ERT
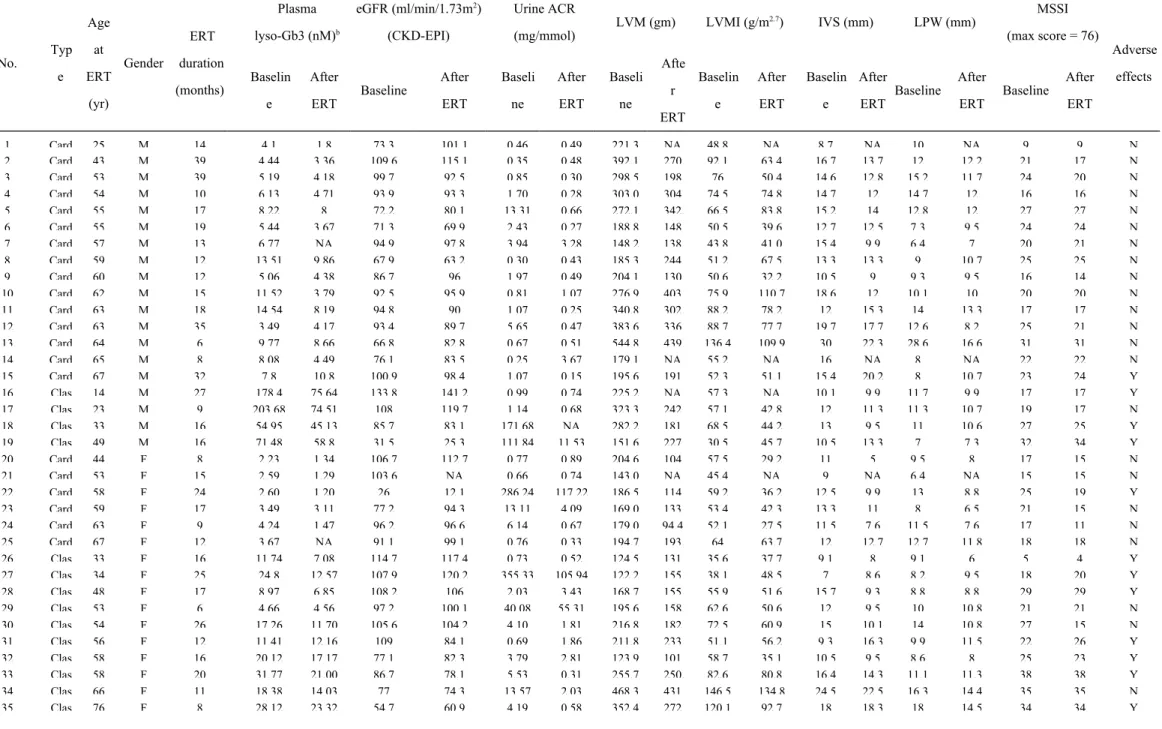
Table 2 shows the parameter changes of cardiac status, renal function, plasma lyso-Gb3 concentrations, and MSSI of these patients at baseline and after 6 to 39 months of ERT. LVH was present at baseline in 13 females (13/16, 81%) and 16 males
(16/21, 76%). The median ERT duration was 16 months. After ERT, plasma lyso-Gb3 was reduced in 89% (17/19) and 93% (14/15) of patients with cardiac and classic types, respectively, indicated the improvement of the disease severity. For patients with cardiac type Fabry disease, echocardiography revealed reduction or stabilization of LVMI, the thicknesses of IVS and LPW in 83% (15/18), 83% (15/18), and 67% (12/18) of patients, respectively; along with 77% (10/13), 73% (11/15), and 60% (9/15) for those with the classic type. For 16 patients with microalbuminuria at baseline, 15 patients (94%) showed some degree of improvement after ERT. Among 35 patients with available data for eGFR, most showed stable renal function after ERT. There were statistically significant differences (p<0.05) between the data at baseline and those after ERT for values of plasma lyso-Gb3, LVM, LVMI, IVS, LPW, and MSSI. No significant differences were found for values of eGFR and urine ACR after ERT (Table 2). We also subdivided these 21 cardiac and 15 classic Fabry patients into 4 groups according to the gender (Table 3 and Figures 1A to 1C). For the values of plasma lyso-Gb3, LVM, LVMI, LPW, and MSSI, the results after ERT revealed improvements compared with those of baseline. However, due to the small sample size in each group, only some items showed statistically significant differences (p<0.05) in certain groups. MSSI scores revealed that all 36 patients (range, 5-38) had mild-to-moderate Fabry disease at baseline (<20, mild; 20-40,
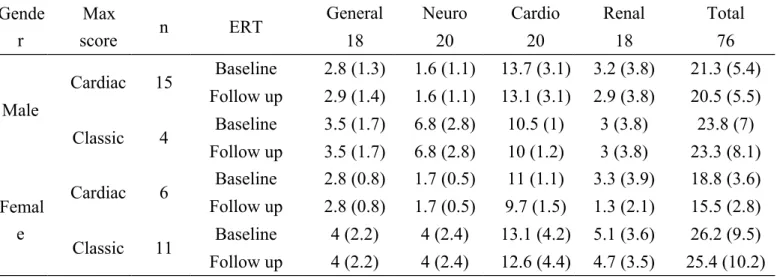
moderate; and >40, severe). After ERT, the total scores showed mild improvement or stabilization in all patients. All scores in general, neurological, cardiovascular, and renal components revealed mild improvements or stabilization after ERT except a slight worsening in the general score for males with the cardiac type (Table 4).
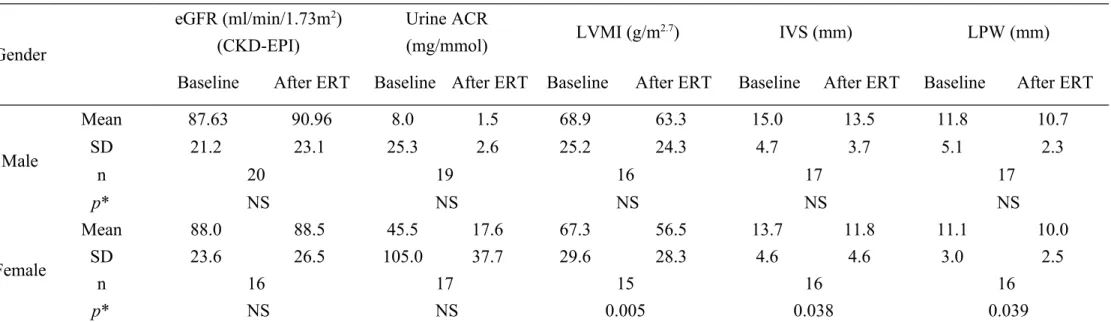
In addition, we also presented the renal and cardiac data for all the males together and females together and did statistical analysis again on these data (Table 5, Figures 2A and 2B). For the values of urine ACR, LVMI, IVS, and LPW, the results after ERT revealed improvements compared with those of baseline. However, due to the small sample size in each group, only some items (LVMI, IVS, and LPW in females) showed statistically significant differences (p<0.05).
Adverse events
Twelve patients (12/36, 33%) experienced at least one adverse events (tachycardia, dyspnea, chest pain, urticaria, diarrhea, fever) since the start of ERT (Table 2). However, with premedication with oral antihistamines, steroids, and antipyretics, they were able to tolerate the ERT. With continued treatment, including premedication, the reactions all abated. No severe clinical events were reported during the treatment.
DISCUSSION
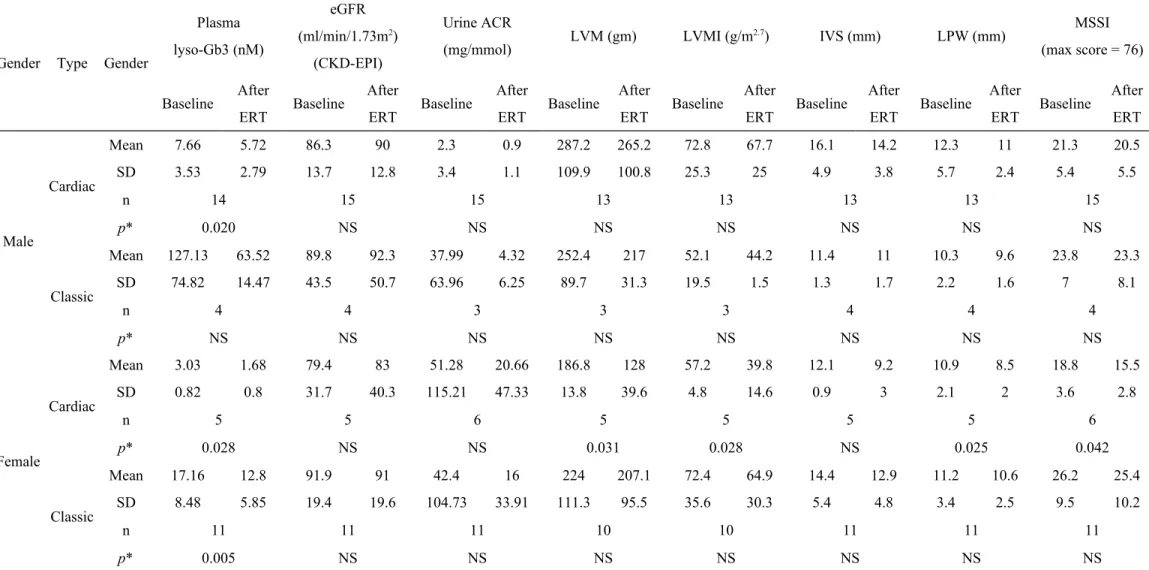
There are numerous clinical reports describing the beneficial effects of ERT for patients with classic Fabry disease, however, there is limited literature reporting those for patients with cardiac type Fabry disease. In order to clarify this point, we subdivided these 21 cardiac and 15 classic Fabry patients into 4 groups according to the gender. For the values of plasma lyso-Gb3, LVM, LVMI, LPW, and MSSI, the results after ERT all revealed improvements compared to baseline, including both cardiac and classic types of different genders. However, due to the small sample size in each group, only some items showed statistically significant differences (p<0.05) in certain groups (Table 3). The results showed ERT for cardiac type Fabry disease also had beneficial effects as well as that for classic Fabry disease.
To the best of our knowledge, this is the first report to demonstrate the efficacy and safety of ERT with agalsidase beta or agalsidase alfa in patients with cardiac type Fabry disease. For most patients in this study, including both cardiac and classic types, ERT reduced plasma lyso-Gb3 concentration, stabilized or improved surrogate parameters, such as LVM, LVMI, the thicknesses of IVS and LPW in those with LVH, improved microalbuminuria, stabilized renal function in those with Fabry nephropathy, and stabilized or improved overall severity of signs and symptoms according to MSSI. Our results were consistent with those of previous studies for
classic Fabry patients.15-26,38,40
Beck et al18 reported a 20% reduction in LVM after 12 months of agalsidase alfa treatment with the standard dose (0.2 mg/kg/biweekly). Our results showed similar improvements. For cardiac type Fabry patients, there was an average decrease of 12% (68.5 to 60 g/m2.7) in LVMI for 18 patients after ERT, as well as 14% (15 to 12.8 mm) and 13% (11.9 to 10.3 mm) decreases in the thicknesses of IVS and LPW, respectively; along with 11% (67.7 to 60.1 g/m2.7), 9% (13.6 to 12.4 mm), and 5% (10.9 to 10.3 mm) decreases for those with the classic type. Schiffmann et al16 described stabilization in patients with preserved renal function, but gradual worsening in advanced kidney disease following 4-4.5 years of agalsidase alfa therapy. In our study, most patients revealed stable renal function after ERT. Microalbuminuria occurs when the kidney leaks small amounts of albumin into the urine, and it is a marker of vascular endothelial dysfunction. There is a handful of literature reporting the change of urine ACR after ERT. In our study, 15 of the 16 patients showed improvement of microalbuminuria after treatment, with the average urine ACR decreased from 56.6 to 19.27 mg/mmol (-66%). These results show that ERT has a potentially positive effect for kidney disease of these patients. Plasma lyso-Gb3 elevation is a hallmark of Fabry disease, and is associated with clinical manifestations.36,37 The average baseline plasma lyso-Gb3 concentration values of 14
male cardiac type patients and 4 male classic patients were 7.66 nM, and 127.13 nM, respectively (reference range <0.01-0.5 nM). Similar values were also seen in female patients. Plasma lyso-Gb3 is also a reliable marker for monitoring the therapeutic outcomes of ERT.41-43 In our study, plasma lyso-Gb3 showed reductions of 28% (6.4 to 4.7 nM) and 43% (46.5 to 26.3 nM) for patients with cardiac and classic types, respectively, suggesting the improvement in disease severity.
MSSI is a sensitive and useful tool for objectively assessing the severity of Fabry disease and for monitoring the effects of ERT. In our study, MSSI scores revealed the severity of signs and symptoms of Fabry disease remained stable or showed mild improvement after ERT in both cardiac and classic types with average scores of 20.6 to 19.1, and 25.5 to 24.8, respectively (max score=76). Given the progressive nature of Fabry disease, stabilization can be seen as a positive outcome following treatment. Our results were in accordance with those of previous studies.38,40
Adverse events, such as pyrexia, dyspnea, and skin rash, were reported in clinical trials of agalsidase beta and agalsidase alfa treatments for Fabry disease. However, the frequency and severity of adverse events diminish over time in most patients due to infusion rate optimization, preinfusion medication, and, possibly, increased tolerance to the exogenous protein since antibody titers often decline with time.15,16 Twelve of our 36 patients (33%) had similar symptoms after receiving ERT, but the reactions
were easily managed. None of them had serious sequelae, and they were all able to continue with treatment. We were unable to measure IgG antibodies against these two products, but we assume our patients’ reactions occurred by the same mechanism.
Limitations
As an uncontrolled retrospective study, we could not compare the results of ERT in our patients with any untreated control subjects. For 7 patients who underwent the switch of ERT from agalsidase beta (1 mg/kg) to agalsidase alfa (0.2 mg/kg), assessments for biochemical and clinical response were not available at regular time intervals during treatment. Thus, partial parameters of cardiac status and renal function, and plasma lyso-Gb3 were not available for certain patients at the time point of switch. The results of ERT for these 7 patients could only showed the overall effects of ERT with agalsidase beta (1 mg/kg) and agalsidase alfa (0.2 mg/kg). Meanwhile, the results were reported after 6-39 months of treatment. This period could not be enough to display the effects of ERT since Fabry disease is a pleomorphic and long-lasting pathology and the clinical outcome requires a long time to be evaluated. In addition, the small sample size of each type reflected the rare nature of this genetic disorder, and the range of age at which treatment began was quite wide, as was the degree of disease severity. Therefore, studies in larger cohorts with a longer follow-up are warranted. However, our experience reflects the problem
that clinicians are likely to encounter when treating patients with Fabry disease, since each patient presents with a quite different condition.
CONCLUSION
In our study, for patients with cardiac type Fabry disease, along with those with the classic type, ERT improved or stabilized cardiac status, stabilized renal function, improved microalbuminuria, stabilized or improved overall severity of signs and symptoms according to MSSI, while reducing plasma lyso-Gb3 concentration. ERT was well tolerated, even among the patients who had hypersensitivity reactions. ERT for treatment of Fabry disease has been endorsed by the National Health Insurance program in Taiwan since April 2002. Our clinical experience confirms that ERT is beneficial and safe for patients with a Chinese hotspot late-onset Fabry mutation (IVS4+919G>A) as well as for those with the classic type. Whether the stabilization or improvement in disease severity and quality of life are durable remains to be seen on further follow-up.
REFERENCES
1. Desnick RJ, Ioannou YA, Eng CM. α-galactosidase A deficiency: Fabry disease. In: Scriver CR, Beaudet AL, Sly WS, Valle D, eds. The Metabolic and Molecular Bases of Inherited Disease. New York: McGraw-Hill, 2001;3733-74.
2. Zarate YA, Hopkin RJ. Fabry's disease. Lancet 2008;372:1427-35.
3. Meikle PJ, Hopwood JJ, Clague AE, Carey WF. Prevalence of lysosomal storage disorders. JAMA 1999;281:249-54.
4. Monserrat L, Gimeno-Blanes JR, Marín F, Hermida-Prieto M, García-Honrubia A, Pérez I, Fernández X, de Nicolas R, de la Morena G, Payá E, Yagüe J, Egido J. Prevalence of Fabry disease in a cohort of 508 unrelated patients with hypertrophic cardiomyopathy. J Am Coll Cardiol 2007;50:2399-403.
5. Nakao S, Takenaka T, Maeda M, Kodama C, Tanaka A, Tahara M, Yoshida A, Kuriyama M, Hayashibe H, Sakuraba H, Tanaka H. An atypical variant of Fabry's disease in men with left ventricular hypertrophy. N Engl J Med 1995;333:288-93. 6. Sachdev B, Takenaka T, Teraguchi H, Tei C, Lee P, McKenna WJ, Elliott PM.
Prevalence of Anderson-Fabry disease in male patients with late onset hypertrophic cardiomyopathy. Circulation 2002;105:1407-11.
7. Kotanko P, Kramar R, Devrnja D, Paschke E, Voigtlander T, Auinger M, Pagliardini S, Spada M, Demmelbauer K, Lorenz M, Hauser AC, Kofler HJ, Lhotta K, Neyer U, Pronai W, Wallner M, Wieser C, Wiesholzer M, Zodl H,
Födinger M, Sunder-Plassmann G. Results of a nationwide screening for Anderson-Fabry disease among dialysis patients. J Am Soc Nephrol 2004;15:1323-9.
8. Nakao S, Kodama C, Takenaka T, Tanaka A, Yasumoto Y, Yoshida A, Kanzaki T, Enriquez AL, Eng CM, Tanaka H, Tei C, Desnick RJ. Fabry disease: detection of undiagnosed hemodialysis patients and identification of a "renal variant" phenotype. Kidney Int 2003;64:801-7.
9. Tanaka M, Ohashi T, Kobayashi M, Eto Y, Miyamura N, Nishida K, Araki E, Itoh K, Matsushita K, Hara M, Kuwahara K, Nakano T, Yasumoto N, Nonoguchi H, Tomita K. Identification of Fabry's disease by the screening of alpha-galactosidase A activity in male and female hemodialysis patients. Clin Nephrol 2005;64:281-7.
10. Rolfs A, Böttcher T, Zschiesche M, Morris P, Winchester B, Bauer P, Walter U, Mix E, Löhr M, Harzer K, Strauss U, Pahnke J, Grossmann A, Benecke R. Prevalence of Fabry disease in patients with cryptogenic stroke: a prospective study. Lancet 2005;366:1794-6.
11. Lin HY, Chong KW, Hsu JH, Yu HC, Shih CC, Huang CH, Lin SJ, Chen CH, Chiang CC, Ho HJ, Lee PC, Kao CH, Cheng KH, Hsueh C, Niu DM. High incidence of the cardiac variant of Fabry disease revealed by newborn screening in the Taiwan Chinese population. Circ Cardiovasc Genet 2009;2:450-6.
12. Lin HY, Huang CH, Yu HC, Chong KW, Hsu JH, Lee PC, Cheng KH, Chiang CC, Ho HJ, Lin SP, Chen SJ, Lin PK, Niu DM. Enzyme assay and clinical assessment in subjects with a Chinese hotspot late-onset Fabry mutation (IVS4+919G→A). J Inherit Metab Dis 2010;33:619-24.
13. Hwu WL, Chien YH, Lee NC, Chiang SC, Dobrovolny R, Huang AC, Yeh HY, Chao MC, Lin SJ, Kitagawa T, Desnick RJ, Hsu LW. Newborn screening for Fabry disease in Taiwan reveals a high incidence of the later-onset GLA mutation c.936+919G>A (IVS4+919G>A). Hum Mutat 2009;30:1397-405.
14. Schiffmann R, Kopp JB, Austin HA 3rd, Sabnis S, Moore DF, Weibel T, Balow JE, Brady RO. Enzyme replacement therapy in Fabry disease: a randomized controlled trial. JAMA 2001;285:2743-9.
15. Germain DP, Waldek S, Banikazemi M, Bushinsky DA, Charrow J, Desnick RJ, Lee P, Loew T, Vedder AC, Abichandani R, Wilcox WR, Guffon N. Sustained, long-term renal stabilization after 54 months of agalsidase beta therapy in patients with Fabry disease. J Am Soc Nephrol 2007;18:1547-57.
16. Schiffmann R, Ries M, Timmons M, Flaherty JT, Brady RO. Long-term therapy with agalsidase alfa for Fabry disease: safety and effects on renal function in a home infusion setting. Nephrol Dial Transplant 2006;21:345-54.
17. Banikazemi M, Bultas J, Waldek S, Wilcox WR, Whitley CB, McDonald M, Finkel R, Packman S, Bichet DG, Warnock DG, Desnick RJ; Fabry Disease
Clinical Trial Study Group. Agalsidase-beta therapy for advanced Fabry disease: a randomized trial. Ann Intern Med 2007;146:77-86.
18. Beck M, Ricci R, Widmer U, Dehout F, de Lorenzo AG, Kampmann C, Linhart A, Sunder-Plassmann G, Houge G, Ramaswami U, Gal A, Mehta A. Fabry disease: overall effects of agalsidase alfa treatment. Eur J Clin Invest 2004;34:838-44.
19. Thofehrn S, Netto C, Cecchin C, Burin M, Matte U, Brustolin S, Nunes AC, Coelho J, Tsao M, Jardim L, Giugliani R, Barros EJ. Kidney function and 24-hour proteinuria in patients with Fabry disease during 36 months of agalsidase alfa enzyme replacement therapy: a Brazilian experience. Ren Fail 2009;31:773-8. 20. Schwarting A, Dehout F, Feriozzi S, Beck M, Mehta A, Sunder-Plassmann G;
European FOS Investigators. Enzyme replacement therapy and renal function in 201 patients with Fabry disease. Clin Nephrol 2006;66:77-84.
21. Hoffmann B, Beck M, Sunder-Plassmann G, Borsini W, Ricci R, Mehta A; FOS European Investigators. Nature and prevalence of pain in Fabry disease and its response to enzyme replacement therapy-a retrospective analysis from the Fabry Outcome Survey. Clin J Pain 2007;23:535-42.
22. West M, Nicholls K, Mehta A, Clarke JT, Steiner R, Beck M, Barshop BA, Rhead W, Mensah R, Ries M, Schiffmann R. Agalsidase alfa and kidney dysfunction in Fabry disease. J Am Soc Nephrol 2009;20:1132-9.
23. Weidemann F, Breunig F, Beer M, Sandstede J, Turschner O, Voelker W, Ertl G, Knoll A, Wanner C, Strotmann JM. Improvement of cardiac function during enzyme replacement therapy in patients with Fabry disease: a prospective strain rate imaging study. Circulation 2003;108:1299-1301.
24. Imbriaco M, Pisani A, Spinelli L, Cuocolo A, Messalli G, Capuano E, Marmo M, Liuzzi R, Visciano B, Cianciaruso B, Salvatore M. Effects of enzyme-replacement therapy in patients with Anderson-Fabry disease: a prospective long-term cardiac magnetic resonance imaging study. Heart 2009;95:1103-7.
25. Hughes DA, Elliott PM, Shah J, Zuckerman J, Coghlan G, Brookes J, Mehta AB. Effects of enzyme replacement therapy on the cardiomyopathy of Anderson-Fabry disease: a randomised, double-blind, placebo-controlled clinical trial of agalsidase alfa. Heart 2008;94:153-8.
26. Motwani M, Banypersad S, Woolfson P, Waldek S. Enzyme replacement therapy improves cardiac features and severity of Fabry disease. Mol Genet Metab 2012;107:197-202.
27. Tsuboi K. Enzyme replacement therapy in patients with Fabry's disease. J Int Med Res 2007;35:574-81.
28. Eto Y, Ohashi T, Utsunomiya Y, Fujiwara M, Mizuno A, Inui K, Sakai N, Kitagawa T, Suzuki Y, Mochizuki S, Kawakami M, Hosoya T, Owada M, Sakuraba H, Saito H. Enzyme replacement therapy in Japanese Fabry disease
patients: the results of a phase 2 bridging study. J Inherit Metab Dis 2005;28:575-83.
29. Choi JH, Cho YM, Suh KS, Yoon HR, Kim GH, Kim SS, Ko JM, Lee JH, Park YS, Yoo HW. Short-term efficacy of enzyme replacement therapy in Korean patients with Fabry disease. J Korean Med Sci 2008;23:243-50.
30. Smid BE, Rombach SM, Aerts JM, Kuiper S, Mirzaian M, Overkleeft HS, Poorthuis BJ, Hollak CE, Groener JE, Linthorst GE. Consequences of a global enzyme shortage of agalsidase beta in adult Dutch Fabry patients. Orphanet J Rare Dis 2011;6:69.
31. Devereux RB, Alonso DR, Lutas EM, Gottlieb GJ, Campo E, Sachs I, Reichek N. Echocardiographic assessment of left ventricular hypertrophy: comparison to necropsy findings. Am J Cardiol 1986;57:450-8.
32. Lang RM, Bierig M, Devereux RB, Flachskampf FA, Foster E, Pellikka PA, Picard MH, Roman MJ, Seward J, Shanewise JS, Solomon SD, Spencer KT, Sutton MS, Stewart WJ; Chamber Quantification Writing Group; American Society of Echocardiography's Guidelines and Standards Committee; European Association of Echocardiography. Chamber Quantification Writing Group; American Society of Echocardiography's Guidelines and Standards Committee; European Association of Echocardiography. Recommendations for chamber quantification: a report from the American Society of Echocardiography's
Guidelines and Standards Committee and the Chamber Quantification Writing Group, developed in conjunction with the European Association of Echocardiography, a branch of the European Society of Cardiology. J Am Soc Echocardiogr 2005;18:1440-63.
33. de Simone G, Daniels SR, Devereux RB, Meyer RA, Roman MJ, de Divitiis O, Alderman MH. Left ventricular mass and body size in normotensive children and adults: assessment of allometric relations and impact of overweight. J Am Coll Cardiol 1992;20:1251-60.
34. de Simone G, Devereux RB, Daniels SR, Koren MJ, Meyer RA, Laragh JH. Effect of growth on variability of left ventricular mass: assessment of allometric signals in adults and children and their capacity to predict cardiovascular risk. J Am Coll Cardiol 1995;25:1056-62.
35. Levey AS, Stevens LA, Schmid CH, Zhang YL, Castro AF 3rd, Feldman HI, Kusek JW, Eggers P, Van Lente F, Greene T, Coresh J; CKD-EPI (Chronic Kidney Disease Epidemiology Collaboration). A New Equation to Estimate Glomerular Filtration Rate. Ann Intern Med 2009;150:604-12.
36. Aerts JM, Groener JE, Kuiper S, Donker-Koopman WE, Strijland A, Ottenhoff R, van Roomen C, Mirzaian M, Wijburg FA, Linthorst GE, Vedder AC, Rombach SM, Cox-Brinkman J, Somerharju P, Boot RG, Hollak CE, Brady RO, Poorthuis BJ. Elevated globotriaosylsphingosine is a hallmark of Fabry disease. Proc Natl
Acad Sci U S A 2008;105:2812-7.
37. Rombach SM, Dekker N, Bouwman MG, Linthorst GE, Zwinderman AH, Wijburg FA, Kuiper S, Vd Bergh Weerman MA, Groener JE, Poorthuis BJ, Hollak CE, Aerts JM. Plasma globotriaosylsphingosine: diagnostic value and relation to clinical manifestations of Fabry disease. Biochim Biophys Acta 2010;1802:741-8.
38. Whybra C, Kampmann C, Krummenauer F, Ries M, Mengel E, Miebach E, Baehner F, Kim K, Bajbouj M, Schwarting A, Gal A, Beck M. The Mainz Severity Score Index: a new instrument for quantifying the Anderson-Fabry disease phenotype, and the response of patients to enzyme replacement therapy. Clin Genet 2004;65:299-307.
39. National Kidney Foundation. K/DOQI clinical practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Am J Kidney Dis 2002;39:S1-266.
40. Parini R, Rigoldi M, Santus F, Furlan F, De Lorenzo P, Valsecchi G, Concolino D, Strisciuglio P, Feriozzi S, Di Vito R, Ravaglia R, Ricci R, Morrone A. Enzyme replacement therapy with agalsidase alfa in a cohort of Italian patients with Anderson-Fabry disease: testing the effects with the Mainz Severity Score Index. Clin Genet 2008;74:260-6.
Suzuki K, Kitagawa T, Sakuraba H. Plasma globotriaosylsphingosine as a biomarker of Fabry disease. Mol Genet Metab 2010;100:257-61.
42. Togawa T, Kawashima I, Kodama T, Tsukimura T, Suzuki T, Fukushige T, Kanekura T, Sakuraba H. Tissue and plasma globotriaosylsphingosine could be a biomarker for assessing enzyme replacement therapy for Fabry disease. Biochem Biophys Res Commun 2010;399:716-20.
43. van Breemen MJ, Rombach SM, Dekker N, Poorthuis BJ, Linthorst GE, Zwinderman AH, Breunig F, Wanner C, Aerts JM, Hollak CE. Reduction of elevated plasma globotriaosylsphingosine in patients with classic Fabry disease following enzyme replacement therapy. Biochim Biophys Acta 2011;1812:70-6.
Table 1. Baseline demographics and clinical characteristics of 36 Taiwanese patients with Fabry disease received enzyme replacement therapy (ERT) with agalsidase beta (1 mg/kg/biweekly) or agalsidase alfa (0.2 mg/kg/biweekly) for 6-39 months
No. Type Age at ERT (yr) Gend er Genotype Plasma α-Gal A activity (nmol/hr/m L)* Hemodialys is Cardiac symptoms Pacem aker Acroparesthe sia Angiokeratom a Hypohydr osis Cerebrovasc ular disorders Dysacusis Gastrointest inal symptoms Respirato ry symptom s Cornea verticillata Fabry cataract 1 Cardia 25 M IVS4+919G> 0.93 - - - -2 Cardia 43 M IVS4+919G> 0.65 - + - - - + NA NA 3 Cardia 53 M IVS4+919G> 0.88 - + - - - - + - - + NA NA 4 Cardia 54 M IVS4+919G> 1.39 - + - - - + + - -5 Cardia 55 M IVS4+919G> 1.3 - + - - - + - -6 Cardia 55 M IVS4+919G> 1.32 - - - + - + -7 Cardia 57 M IVS4+919G> 1.13 - + - - - + - -8 Cardia 59 M IVS4+919G> 1.02 - + + - - - -9 Cardia 60 M IVS4+919G> 0.79 - + - - - + 10 Cardia 62 M IVS4+919G> 1.48 - + - - - + 11 Cardia 63 M IVS4+919G> 1.47 - + - - - + 12 Cardia 63 M IVS4+919G> 1.2 - + - - - + - NA NA 13 Cardia 64 M IVS4+919G> 1.15 - + + - - - + - -14 Cardia 65 M IVS4+919G> 1.71 - + - - - + - -15 Cardia 67 M IVS4+919G> 0.95 - + - - - NA NA 16 Classi 14 M W204X 0 - + - + + + - - - - NA NA 17 Classi 23 M E398DfsX6 0 - + - + - + + - - + + -18 Classi 33 M E398DfsX6 0.027 - + - + + + - + - - + -19 Classi 49 M E398DfsX6 0.02 - + - + + + - + + - + + 20 Cardia 44 F IVS4+919G/ 7.67 - + - - - -21 Cardia 53 F IVS4+919G/ 4.4 - + - - - -22 Cardia 58 F IVS4+919G/ 4.03 - + - - - + - + 23 Cardia 59 F IVS4+919G/ 5.17 - + - - - -24 Cardia 63 F IVS4+919G/ 9.63 - + - - - + - + 25 Cardia 67 F IVS4+919G/ 6.51 - + - - - + + -26 Classi 33 F G132R 2.4 - - - + + 27 Classi 34 F S345X 3.34 - - - + - - - + -28 Classi 48 F W204X 5.59 - + - + - - + - + + + + 29 Classi 53 F W204X 9.19 - + - + - - - NA NA 30 Classi 54 F W204X 2.54 - + - - - + NA NA 31 Classi 56 F E398DfsX6 7.73 - + - + - - - + -32 Classi 58 F G132R 1.26 - + - - - + + +
34 Classi 66 F E398DfsX6 6.91 - + - + - - - - + - + +
35 Classi 76 F E398DfsX6 3.91 - + - + - - - + +
-36 Classi 79 F W204X 3.31 - + - - - - + - + + NA NA
ERT, enzyme replacement therapy; α-Gal A, α-galactosidase A; NA, not available. *Reference range: 7.9-16.9.
Table 2. Parameter changes of cardiac status and renal function, plasma lyso-Gb3, and Mainz Severity Score Index (MSSI) at baseline and after 6-39 months of enzyme replacement therapy (ERT) for 36 Taiwanese patients with Fabry disease
No. Typ e Age at ERT (yr) Gender ERT duration (months) Plasma lyso-Gb3 (nM)b eGFR (ml/min/1.73m2) (CKD-EPI) Urine ACR (mg/mmol) LVM (gm) LVMI (g/m 2.7) IVS (mm) LPW (mm) MSSI (max score = 76) Adverse effects Baselin e After ERT Baseline After ERT Baseli ne After ERT Baseli ne Afte r ERT Baselin e After ERT Baselin e After ERT Baseline After ERT Baseline After ERT 1 Card 25 M 14 4.1 1.8 73.3 101.1 0.46 0.49 221.3 NA 48.8 NA 8.7 NA 10 NA 9 9 N 2 Card 43 M 39 4.44 3.36 109.6 115.1 0.35 0.48 392.1 270 92.1 63.4 16.7 13.7 12 12.2 21 17 N 3 Card 53 M 39 5.19 4.18 99.7 92.5 0.85 0.30 298.5 198 76 50.4 14.6 12.8 15.2 11.7 24 20 N 4 Card 54 M 10 6.13 4.71 93.9 93.3 1.70 0.28 303.0 304 74.5 74.8 14.7 12 14.7 12 16 16 N 5 Card 55 M 17 8.22 8 72.2 80.1 13.31 0.66 272.1 342. 66.5 83.8 15.2 14 12.8 12 27 27 N 6 Card 55 M 19 5.44 3.67 71.3 69.9 2.43 0.27 188.8 148 50.5 39.6 12.7 12.5 7.3 9.5 24 24 N 7 Card 57 M 13 6.77 NA 94.9 97.8 3.94 3.28 148.2 138. 43.8 41.0 15.4 9.9 6.4 7 20 21 N 8 Card 59 M 12 13.51 9.86 67.9 63.2 0.30 0.43 185.3 244. 51.2 67.5 13.3 13.3 9 10.7 25 25 N 9 Card 60 M 12 5.06 4.38 86.7 96 1.97 0.49 204.1 130 50.6 32.2 10.5 9 9.3 9.5 16 14 N 10 Card 62 M 15 11.52 3.79 92.5 95.9 0.81 1.07 276.9 403. 75.9 110.7 18.6 12 10.1 10 20 20 N 11 Card 63 M 18 14.54 8.19 94.8 90 1.07 0.25 340.8 302. 88.2 78.2 12 15.3 14 13.3 17 17 N 12 Card 63 M 35 3.49 4.17 93.4 89.7 5.65 0.47 383.6 336 88.7 77.7 19.7 17.7 12.6 8.2 25 21 N 13 Card 64 M 6 9.77 8.66 66.8 82.8 0.67 0.51 544.8 439 136.4 109.9 30 22.3 28.6 16.6 31 31 N 14 Card 65 M 8 8.08 4.49 76.1 83.5 0.25 3.67 179.1 NA 55.2 NA 16 NA 8 NA 22 22 N 15 Card 67 M 32 7.8 10.8 100.9 98.4 1.07 0.15 195.6 191 52.3 51.1 15.4 20.2 8 10.7 23 24 Y 16 Clas 14 M 27 178.4 75.64 133.8 141.2 0.99 0.74 225.2 NA 57.3 NA 10.1 9.9 11.7 9.9 17 17 Y 17 Clas 23 M 9 203.68 74.51 108 119.7 1.14 0.68 323.3 242 57.1 42.8 12 11.3 11.3 10.7 19 17 N 18 Clas 33 M 16 54.95 45.13 85.7 83.1 171.68 NA 282.2 181. 68.5 44.2 13 9.5 11 10.6 27 25 Y 19 Clas 49 M 16 71.48 58.8 31.5 25.3 111.84 11.53 151.6 227. 30.5 45.7 10.5 13.3 7 7.3 32 34 Y 20 Card 44 F 8 2.23 1.34 106.7 112.7 0.77 0.89 204.6 104 57.5 29.2 11 5 9.5 8 17 15 N 21 Card 53 F 15 2.59 1.29 103.6 NA 0.66 0.74 143.0 NA 45.4 NA 9 NA 6.4 NA 15 15 N 22 Card 58 F 24 2.60 1.20 26 12.1 286.24 117.22 186.5 114 59.2 36.2 12.5 9.9 13 8.8 25 19 Y 23 Card 59 F 17 3.49 3.11 77.2 94.3 13.11 4.09 169.0 133. 53.4 42.3 13.3 11 8 6.5 21 15 N 24 Card 63 F 9 4.24 1.47 96.2 96.6 6.14 0.67 179.0 94.4 52.1 27.5 11.5 7.6 11.5 7.6 17 11 N 25 Card 67 F 12 3.67 NA 91.1 99.1 0.76 0.33 194.7 193. 64 63.7 12 12.7 12.7 11.8 18 18 N 26 Clas 33 F 16 11.74 7.08 114.7 117.4 0.73 0.52 124.5 131. 35.6 37.7 9.1 8 9.1 6 5 4 Y 27 Clas 34 F 25 24.8 12.57 107.9 120.2 355.33 105.94 122.2 155. 38.1 48.5 7 8.6 8.2 9.5 18 20 Y 28 Clas 48 F 17 8.97 6.85 108.2 106 2.03 3.43 168.7 155. 55.9 51.6 15.7 9.3 8.8 8.8 29 29 Y 29 Clas 53 F 6 4.66 4.56 97.2 100.1 40.08 55.31 195.6 158 62.6 50.6 12 9.5 10 10.8 21 21 N 30 Clas 54 F 26 17.26 11.70 105.6 104.2 4.10 1.81 216.8 182 72.5 60.9 15 10.1 14 10.8 27 15 N 31 Clas 56 F 12 11.41 12.16 109 84.1 0.69 1.86 211.8 233 51.1 56.2 9.3 16.3 9.9 11.5 22 26 Y 32 Clas 58 F 16 20.12 17.17 77.1 82.3 3.79 2.81 123.9 101. 58.7 35.1 10.5 9.5 8.6 8 25 23 Y 33 Clas 58 F 20 31.77 21.00 86.7 78.1 5.53 0.31 255.7 250. 82.6 80.8 16.4 14.3 11.1 11.3 38 38 Y 34 Clas 66 F 11 18.38 14.03 77 74.3 13.57 2.03 468.3 431. 146.5 134.8 24.5 22.5 16.3 14.4 35 35 N
36 Clas 79 F 12 11.55 10.36 72.5 73.2 36.34 1.41 NA NA NA NA 21 16 9 11 34 34 N Mea n SD 53.4 14.4 17 8.8 24.1 44.9 14.2 19.6 87.9 22 89.5 24.6 30.4 79.4 9.3 27.2 247.2 102.9 219. 7 97.1 68.2 26.9 60 26.1 14.3 4.6 12.6 4.2 11.5 4.1 10.3 2.4 22.7 7.1 21.5 7.7 p valuea 0.043 NS NS 0.015 0.008 0.006 0.024 0.019 n 34 35 35 31 31 33 33 36
ERT, enzyme replacement therapy; lyso-Gb3, globotriaosylsphingosine; eGFR, estimated glomerular filtration rate; ACR, albumin-to-creatinine ratio; LVM, left ventricular mass; LVMI, left ventricular mass index; IVS, intraventricular septum; LPW, left posterior wall; MSSI, Mainz Severity Score Index; NA, not available; SD, standard deviation; NS, not significant.
Table 3. Parameter changes of cardiac status and renal function, plasma lyso-Gb3, and Mainz Severity Score Index (MSSI) at baseline and after enzyme replacement therapy (ERT) for 36 Taiwanese patients with Fabry disease subdivided into 4 groups according to the gender and the type (cardiac or classic)
Gender Type Gender
Plasma lyso-Gb3 (nM) eGFR (ml/min/1.73m2) (CKD-EPI) Urine ACR (mg/mmol) LVM (gm) LVMI (g/m 2.7) IVS (mm) LPW (mm) MSSI (max score = 76) Baseline After ERT Baseline After ERT Baseline After ERT Baseline After ERT Baseline After ERT Baseline After ERT Baseline After ERT Baseline After ERT Male Cardiac Mean SD 7.66 3.53 5.72 2.79 86.3 13.7 90 12.8 2.3 3.4 0.9 1.1 287.2 109.9 265.2 100.8 72.8 25.3 67.7 25 16.1 4.9 14.2 3.8 12.3 5.7 11 2.4 21.3 5.4 20.5 5.5 n 14 15 15 13 13 13 13 15 p* 0.020 NS NS NS NS NS NS NS Classic Mean SD 127.13 74.82 63.52 14.47 89.8 43.5 92.3 50.7 37.99 63.96 4.32 6.25 252.4 89.7 217 31.3 52.1 19.5 44.2 1.5 11.4 1.3 11 1.7 10.3 2.2 9.6 1.6 23.8 7 23.3 8.1 n 4 4 3 3 3 4 4 4 p* NS NS NS NS NS NS NS NS Female Cardiac Mean SD 3.03 0.82 1.68 0.8 79.4 31.7 83 40.3 51.28 115.21 20.66 47.33 186.8 13.8 128 39.6 57.2 4.8 39.8 14.6 12.1 0.9 9.2 3 10.9 2.1 8.5 2 18.8 3.6 15.5 2.8 n 5 5 6 5 5 5 5 6 p* 0.028 NS NS 0.031 0.028 NS 0.025 0.042 Classic Mean SD 17.16 8.48 12.8 5.85 91.9 19.4 91 19.6 42.4 104.73 16 33.91 224 111.3 207.1 95.5 72.4 35.6 64.9 30.3 14.4 5.4 12.9 4.8 11.2 3.4 10.6 2.5 26.2 9.5 25.4 10.2 n 11 11 11 10 10 11 11 11 p* 0.005 NS NS NS NS NS NS NS
ERT, enzyme replacement therapy; lyso-Gb3, globotriaosylsphingosine; eGFR, estimated glomerular filtration rate; ACR, albumin-to-creatinine ratio; LVM, left ventricular mass; LVMI, left ventricular mass index; IVS, intraventricular septum; LPW, left posterior wall; MSSI, Mainz Severity Score Index; SD, standard deviation; NS, not
significant.
Table 4. Mainz Severity Scores Index (MSSI) at baseline and after 6-39 months of enzyme replacement therapy (ERT) for 36 Taiwanese patients with Fabry disease subdivided into 4 groups according to the
gender and the type (cardiac or classic) Gende
r
Max
score n ERT
General Neuro Cardio Renal Total
18 20 20 18 76 Male Cardiac 15 Baseline 2.8 (1.3) 1.6 (1.1) 13.7 (3.1) 3.2 (3.8) 21.3 (5.4) Follow up 2.9 (1.4) 1.6 (1.1) 13.1 (3.1) 2.9 (3.8) 20.5 (5.5) Classic 4 Baseline 3.5 (1.7) 6.8 (2.8) 10.5 (1) 3 (3.8) 23.8 (7) Follow up 3.5 (1.7) 6.8 (2.8) 10 (1.2) 3 (3.8) 23.3 (8.1) Femal e Cardiac 6 Baseline 2.8 (0.8) 1.7 (0.5) 11 (1.1) 3.3 (3.9) 18.8 (3.6) Follow up 2.8 (0.8) 1.7 (0.5) 9.7 (1.5) 1.3 (2.1) 15.5 (2.8) Classic 11 Baseline 4 (2.2) 4 (2.4) 13.1 (4.2) 5.1 (3.6) 26.2 (9.5) Follow up 4 (2.2) 4 (2.4) 12.6 (4.4) 4.7 (3.5) 25.4 (10.2)
Data are mean (standard deviation). Max, maximum possible score; Neuro, neurological; Cardio, cardiovascular.
Table 5. Parameter changes of cardiac status and renal function at baseline and after enzyme replacement therapy (ERT) for 36 Taiwanese subdivided into 2 groups according to the gender.
Gender eGFR (ml/min/1.73m2) (CKD-EPI) Urine ACR (mg/mmol) LVMI (g/m 2.7) IVS (mm) LPW (mm)
Baseline After ERT Baseline After ERT Baseline After ERT Baseline After ERT Baseline After ERT
Male Mean 87.63 90.96 8.0 1.5 68.9 63.3 15.0 13.5 11.8 10.7 SD 21.2 23.1 25.3 2.6 25.2 24.3 4.7 3.7 5.1 2.3 n 20 19 16 17 17 p* NS NS NS NS NS Female Mean 88.0 88.5 45.5 17.6 67.3 56.5 13.7 11.8 11.1 10.0 SD 23.6 26.5 105.0 37.7 29.6 28.3 4.6 4.6 3.0 2.5 n 16 17 15 16 16 p* NS NS 0.005 0.038 0.039
ERT, enzyme replacement therapy; eGFR, estimated glomerular filtration rate; ACR, albumin-to-creatinine ratio; LVMI, left ventricular mass index; IVS, intraventricular septum; LPW, left posterior wall; SD, standard deviation; NS, not significant.
FIGURE LEGENDS
Figure 1. Effects of enzyme replacement therapy (ERT) on (A) left ventricular mass index (LVMI), (B) intraventricular septum (IVS), and (C) left posterior wall (LPW) in patients with Fabry disease subdivided into 4 groups according to the gender and the type (cardiac or classic). Values shown are mean ± standard deviation. *Asterisk represents statistically significant difference between the data of baseline and that after ERT (p<0.05).
Figure 2. Effects of enzyme replacement therapy (ERT) on left ventricular mass index (LVMI) in male (A) and female (B) patients with Fabry disease.