Volumetric Intensity-Modulated Arc (RapidArc) Therapy for Primary
Hepatocellular carcinoma: Comparison with Intensity-Modulated
Radiotherapy and 3-D Conformal Radiotherapy
Yu-Cheng Kuo1,2,4, Ying-Ming Chiu5, Wen-Pin Shih2, Hsiao-Wei Yu6, Chia-Wen
Chen3, Pei-Fong Wong7, Wei-Chan Lin1, Jeng-Jong Hwang*1
1
Dept. of Biomedical Imaging & Radiological Sciences, National Yang-Ming University, No. 155, Sec. 2, Li-Nong St., Bei-tou, Taipei 11221, Taiwan.
2
Dept. of Radiation Oncology, China Medical University Hospital, No. 2, Yuh-Der Rd.
Taichung, 404, Taiwan.
3
Dept. of Anesthesiology, China Medical University Hospital, No. 2, Yuh-Der Rd.
Taichung, 404, Taiwan.
4
Dept. of Biomedical Imaging & Radiological Sciences, China Medical University,
No. 2, Yuh-Der Rd. Taichung, 404, Taiwan.
5
Graduate Institute of Epidemiology, National Taiwan University, 5F, No.17,
Hsu-Chow Rd. Taipei, 100, Taiwan.
6
Dept. of Radiation Oncology, Wan-Fang Hospital, No. 111, Section 3, Hsing-Long
Rd.Taipei, 116, Taiwan .
7
Dept. of Radiation Physics, The University of Texas MD Anderson Cancer Center,
* Corresponding author Affiliation of the first author:
Yu-Cheng Kuo, MD, Dept. of Biomedical Imaging and Radiological Sciences,
National Yang-Ming University, No. 155, Sec. 2, Li-Nong St., Bei-tou, Taipei 11221,
Taiwan.
Tel: 886-2-2826-7064 Fax: 886-2-2820-1095
E-mail: [email protected]
Mailing address for correspondence and reprints:
Jeng-Jong Hwang, Ph.D., Professor
Dept. of Biomedical Imaging and Radiological Sciences, National Yang-Ming
University, No. 155, Sec. 2, Li-Nong St., Bei-tou, Taipei 11221, Taiwan.
Tel: 886-2-2826-7064
Fax: 886-2-2820-1095
E-mail: [email protected]
Other authors:
YM Chiu: [email protected] WP Shih: [email protected]
HW Yu: [email protected] CW Chen: [email protected]
Abstract
Background: To compare the RapidArc plan for primary hepatocellular carcinoma
(HCC) with 3-D conformal radiotherapy (3DCRT) and intensity-modulated
radiotherapy (IMRT) plans using dosimetric analysis.
Methods: Nine patients with unresectable HCC were enrolled in this study.
Dosimetric values for RapidArc, IMRT, and 3DCRT were calculated for total doses of
45~50.4 Gy using 1.8 Gy/day. The parameters included the conformal index (CI),
homogeneity index (HI), and hot spot (V107%) for the planned target volume (PTV) as
well as the monitor units (MUs) for plan efficiency, the mean dose (Dmean) for the
organs at risk (OAR) and the maximal dose at 1% volume (D1%) for the spinal cord.
The percentage of the normal liver volume receiving >40, >30, >20, and >10 Gy
(V40Gy, V30Gy, V20Gy, and V10Gy) and the normal tissue complication probability
(NTCP) were also evaluated to determine liver toxicity.
Results: All three methods achieved comparable homogeneity for the PTV. RapidArc
achieved significantly better CI and V107% values than IMRT or 3DCRT (p <0.05).
The MUs were significantly lower for RapidArc (323.8 + 60.7) and 3DCRT (322.3 +
28.6) than for IMRT (1165.4 + 170.7) (p < 0.001). IMRT achieved a significantly
lower Dmean of the normal liver than did 3DCRT or RapidArc (p = 0.001). 3DCRT had
Although the V10Gy to the normal liver was higher with RapidArc (75.8 + 13.1%) than
with 3DCRT or IMRT (60.5 + 10.2% and 57.2 + 10.0%, respectively; p < 0.01), the
NTCP did not differ significantly between RapidArc (4.38 + 2.69) and IMRT (3.98 +
3.00) and both were better than 3DCRT (7.57 + 4.36) (p = 0.02).
Conclusions: RapidArc provided favorable tumor coverage compared with IMRT or
3DCRT, but RapidArc is not superior to IMRT in terms of liver protection. Further
studies are needed to establish treatment outcome differences between the three
Background
Hepatocellular carcinoma (HCC) is the fifth most common malignancy and the third
most common cause of cancer-related death in the world [1]. Surgical resection has
been proven as the major treatment modality for HCC. However, most patients with
HCC have unresectable disease at diagnosis. These patients are treated with other
treatment modalities, such as percutaneous ethanol injection (PEI), radiofrequency
ablation (RFA) therapy, transcatheter arterial chemoradiotherapy (TACE), or sorafenib,
but the response to treatment is limited [2-6].
The use of radiation therapy (RT) for the treatment of HCC was first investigated
more than 40 years ago, but the early trials reported poor results due to the low
tolerance of the whole liver to radiation and severe hepatic toxicity, or
radiation-induced liver disease (RILD) caused by whole liver irradiation [7, 8]. RILD,
a clinical syndrome characterized by ascites, anicteric hepatomegaly, and impaired
liver function, is developed in 5% of patients who received 30~33 Gy whole liver
irradiation and usually occurs 2 weeks to 4 months after completion of RT. RILD
usually resolves after supportive care. Unfortunately, severe RILD may develop into
hepatic failure and even death [9, 10]. The low hepatic tolerance to radiation also
limits the application of higher radiation doses to the tumor. In 1991, Emami et al.
for 1/3, 2/3, and the whole liver at 1.8~2 Gy/day were 50 Gy, 35 Gy, and 30 Gy,
respectively [11]. Dawson et al used the normal tissue complication probability
(NTCP) of the Lyman model to describe the relationship between irradiated liver
volume and radiation dose and they demonstrated that a higher radiation dose could
be delivered safely to liver tumors, with better outcomes, if only part of the liver was
irradiated [12]. As image-based treatment planning and engineering has advanced,
three-dimensional conformal radiotherapy (3DCRT) was developed to irradiate the
tumor accurately while minimizing the dose to the normal liver. A number of studies
have demonstrated encouraging results showing that a radiation dose could be safely
increased to part of the liver using 3DCRT [13]. For example, Park et al. reported a
significant relationship between the total dose to the liver tumor and the tumor
response (<40 Gy, 40–50 Gy, and >50 Gy giving responses of 29.2%, 68.6%, and
77.1%, respectively) without significant toxicity (rate of liver toxicity: 4.2%, 5.9%,
and 8.4%, respectively).
Despite improvements to 3DCRT, dose distribution remains suboptimal in some cases.
In the early 2000s, the development of inverse planning systems and multileaf
collimators (MLCs) culminated in a more sophisticated technique,
intensity-modulated radiotherapy (IMRT). Using an inverse planning algorithm to
dose to the tumor while delivering a relatively lower dose to the normal liver as
compared with 3DCRT. Cheng et al. suggested that IMRT might be able to preserve
acceptable target coverage and potentially reduce NTCP values (IMRT = 23.7% and
3DCRT = 36.6%, p = 0.009) compared with 3DCRT [14]. Fuss et al. reported that
IMRT allowed a dose escalation to 60 Gy, in which range 3DCRT had to reduce the
total dose to decrease the probability of RILD to acceptable levels [15].
The RapidArc technique, developed by Varian Medical Systems about 2 years ago, is
a volumetric intensity-modulated arc therapy that accurately and efficiently delivers a
radiation dose to the target using a one- or two-arc gantry rotation by simultaneously
modulating the MLC motion and the dose rates. RapidArc has been shown to be
equivalent or superior to IMRT for some malignancies, including head and neck
cancer and prostate cancer [16-18], but there has been no study to determine the
feasibility of using RapidArc for the treatment of primary HCC. The purpose of our
study was to compare the RapidArc radiation treatment plans for patients with HCC
with 3DCRT and IMRT plans using dosimetric analysis. The PTV coverage and
critical organ sparing for each technique were determined using dose-volume
Methods
Patient Characteristics
From April 2008 to July 2010, we enrolled nine patients who had primary HCC
diagnosed at China Medical University Hospital. All patients underwent
alpha-fetoprotein (AFP) examination, contrast-enhanced computed tomography (CT),
and ultrasonography to confirm the diagnosis. All patients were male and the median
age was 57 years (range, 38-81 years). Five patients had Child-Pugh score A cirrhosis
and 4 had Child-Pugh score B cirrhosis. Eight (88.9%) patients had American Joint
Committee on Cancer (6th edition) stage III disease, and 1 (11.1%) patient had stage
IV disease.
Immobilization, Simulation, and Target Delineation
The patients were immobilized using vacuum casts in a supine position with both
arms raised above their heads. Non-contrast CT simulation was performed with a
5-mm slice thickness and included whole liver and bilateral kidney scans. Respiratory
control and abdominal compression were not used. After simulation, the CT images
were transferred into the Eclipse treatment planning system (Version 8.6.15, Varian
Medical System, Inc., Palo Alto, CA, US), and target delineation was performed with
We defined the gross tumor volume (GTV) as the volume of primary tumor
evident on contrast-enhanced CT images. The clinical target volume (CTV) was
delineated on the basis of the GTV expanded by 5 mm. The planning target volume
(PTV) was defined as the CTV with a 5-mm radial expansion and a 10-mm
craniocaudal expansion to account for errors caused by the daily setup process and
internal organ motion. The normal liver volume was defined as the total liver volume
minus the GTV. All of the contours were drawn by the same physician.
Treatment Planning and Dose Delivery
In our study, we prescribed 95% of total dose to cover > 95% of the PTV
coverage in daily 1.8-Gy fractions while keeping the minimum dose > 93% of total
dose and maximum dose < 107% of total dose and normalized all plans to the mean
dose of PTV. The guidelines for dose prescription were as follows. When the normal
liver volume irradiated with >50% of the isocenter dose was < 25%, 25-50%, or
50-75%, the total dose prescribed was > 59.4 Gy, 45-54 Gy, and 41.4 Gy, respectively
[19]. No patient received whole liver irradiation. The constraints for the organs at risk
(OARs), can be seen in Table 1. These were imposed in terms of the TD5/5 to ensure
that the maximal tolerated doses to the normal liver, stomach, kidneys, and spinal
the tumor location, and the same energy was used for each patient and for all three
methods.
For each patient, three different plans (3DCRT, IMRT, and RapidArc) were
calculated using the Eclipse planning system with the 120-leaf multi-leaf collimator
(MLC) (Varian Medical Systems). For the 3DCRT and IMRT plans, all the gantry
angles and numbers of radiation fields (range, 4-5) were manually selected on the
basis of the morphological relationship between the PTV and OARs to cover at least
95% of the PTV and spare the OARs. A dose rate of 400 MU/min was used. For
RapidArc, the plans were optimized using the two-arc technique with gantry angle
running counterclockwise from 179° to 181° and clockwise from 181° to 179° and
with the dose rate varied between 0 MU/min and 600 MU/min (upper limit). The
optimization constraints for OARs using RapidArc were the same as the constraints in
Table 1.
Plan Evaluation
1. PTV coverage
The dose to the PTV was evaluated using DVHs with the following parameters:
a. Vx% means the volume receiving >x% of the prescribed dose. For example, the
to represent the hot spot in the PTV.
b. The conformity index (CI) = (VPTV/TVPV)/(TVPV/VTV) = VPTV x VTV / TVPV2,
where VPTV is the volume of the PTV, TVPV is the portion of the VPTV within
the prescribed isodose line, and VTV is the treated volume of the prescribed
isodose line [17, 20]. The CI represented the dose fit of the PTV relative to the
volume covered by the prescribed isodose line. The smaller and closer the
value of CI is to 1, the better the conformity of the PTV.
c. The homogeneity index (HI) = D5%/D95%, where D5% and D95% are the minimum
doses delivered to 5% and 95% of the PTV [17, 21]. HI is a ratio that is used
to evaluate the homogeneity of the PTV. The smaller and closer the value of
HI is to 1, the better the homogeneity of the PTV.
2. OARs sparing
a. VnGy is the percentage of organ volume receiving > n Gy. In this study,
V40Gy was the percentage of the normal liver volume receiving > 40 Gy,
which represents high-dose exposure for the normal liver. In contrast, V10Gy
was the percentage of the normal liver volume receiving > 10 Gy, which
represented low-dose exposure for the normal liver.
b. We used the normal tissue complication probability (NTCP), from the
normal liver [22]. In the NTCP model,
(1)
(2)
where EUD is the equivalent uniform dose, converted from the dose-volume pairs [Di,
vi], to describe the dose which, if delivered uniformly to the entire organ, would
achieve the same effect as the given heterogeneous dose distribution demonstrated by
the DVH. The TD50(1) is the dose to the whole liver that would result in a 50%
probability of toxicity. The parameter “m” is the steepness of the dose–complication
curve for a fixed partial volume. The parameter “n” is the slope of the complication
probability, which determines the dose-volume relationship for the irradiated normal
liver. In this study, the following values for the parameters were used: n=0.32,
m=0.15, and TD50(1) = 40 Gy [23].
Statistical Analyses
The dosimetric differences among the three treatments for the nine patients were
analyzed using the Friedman test. When a significant difference (p < 0.05) was found,
the difference between two treatments for each effect was further examined by )] 2 ( 1 [ 2 1 ) 2 / exp( 2 1 2 x erf dt t NTCP=
∫
x − = + ∞ − π n i n i i D v EUD TD m TD EUD x × = × − =∑
1/ 50 50 , ( ) ) 1 ( ) 1 (Wilcoxon signed-rank test. All analyses were performed using SPSS software, version
Results
PTV Coverage, CI, and HI
The mean gross tumor volume (GTV) was 979.3 + 497.2 cm3 (range, 346.5-2019.3
cm3). The mean planned tumor volume (PTV) was 1734.2 + 923.0 cm3 (range,
859.6-3253.4 cm3). The mean normal liver volume was 1632.4 + 539.0 cm3 (range,
933.7-2270.6 cm3). None of the PTVs included the whole liver. The prescribed total
dose was 49.4 + 1.9 Gy (range, 45-50.4 Gy). The dose rate of RapidArc varied
between 0 MU/min and 461 MU/min. The typical dose distributions and dose-volume
histograms (DVH) for PTV and OARs are shown in Fig. 1 and Fig. 2, respectively. In
Fig. 1C, RapidArc achieved better conformality to the 95% isodose line of the PTV
than did 3DCRT and IMRT. In addition, RapidArc also achieved better spinal cord
sparing to the 50% isodose line than did 3DCRT and IMRT. However, RapidArc
resulted in higher coverage at the 30% isodose line in the normal liver as compared
with 3DCRT (Fig. 1A) or IMRT (Fig. 1B), which means higher low-dose exposure
occur for the normal liver with RapidArc. In Fig. 2, the right DVH showed that all of
the PTVs were fixed between V95% and V107%, without any significant differences.
The left DVH showed that the low-dose distribution in the normal liver was greater
for RapidArc than for 3DCRT or IMRT, and the high-dose distribution was greater for
Table 2 summarizes the results for the investigated DVH-parameters, including
CTV coverage, PTV coverage, monitor unit (MU) dose and OAR dose for the 9
patients. Table 3 shows the differences among the three methods with regard to the
DVH parameters. For target coverage, all V95% of CTV for these three techniques
gave at least 99% of the prescribed dose without any significant difference (p = 1.00).
For the PTV coverage, the mean CI of RapidArc (1.12 + 0.05) was significantly lower
than that of IMRT (1.19 + 0.06) and 3DCRT (1.286 + 0.11) (p < 0.05). The V95%, and
V100% valus for PTVs and HI were 95.50 + 2.41, 76.81 + 5.95 and 1.13 + 0.05
(3DCRT), 95.27 + 1.99, 77.88 + 4.27 and 1.13 + 0.04 (IMRT), and 95.31 + 1.64,
77.47 + 2.64 and 1.12 + 0.03 (RapidArc), respectively, with no significant differences
among methods (p = 1.00, 1.00 and 0.69, respectively). For the hot spot sparing, the
mean V107% of the PTV was significantly highest for 3DCRT (7.49 + 7.92) and the
lowest was RapidArc (1.74 + 2.82); this indicates that there was better hot-spot
sparing of the PTV with RapidArc than with IMRT or 3DCRT (p < 0.05).
OARs Sparing
The mean doses to the normal liver for each method were 21.58 + 3.01 Gy
(3DCRT), 19.31 + 2.89 Gy (IMRT), and 21.97 + 2.61 Gy (RapidArc), with a
RapidArc (p < 0.05). The high-dose regions of the normal liver were higher for V40Gy
and V30Gy with 3DCRT (23.05 + 4.06 and 32.10 + 6.80) than with IMRT (18.61 + 4.13
and 26.23 + 5.87) (p < 0.01) or RapidArc (18.85 + 3.97 and 27.77 + 5.34) (p < 0.05).
The low-dose region of the normal liver was higher for V10Gy with RapidArc (75.77 +
13.13) than with IMRT (57.24 + 10.02) (p < 0.01) or 3DCRT (60.55 + 10.24) (p <
0.05). In Table 3, the NTCP value for 3DCRT (7.57 + 4.36) was significantly higher
than that for IMRT (3.98 + 3.00) (p < 0.01) or RapidArc (4.38 + 2.69) (p < 0.05), but
there was no significant difference in the NTCP between IMRT and RapidArc (p =
0.26). For the other OARs, there were no significant differences in dose among the
three methods, except for a lower mean dose to the stomach and left kidney,
respectively, with IMRT (20.63 + 15.26 Gy and 8.36 + 4.60 Gy) than with 3DCRT
(23.16 + 16.50 Gy and 11.37 + 6.62 Gy) (p < 0.05). The maximum dose to the spinal
cord (D1%) was equal for all three methods.
Efficiency Analysis
IMRT had three times the MUs (1165.44 + 170.68) of RapidArc (323.78 + 60.65)
and 3DCRT (322.33 + 28.62) (p < 0.01). There was no significant difference in the
Discussion
Historically, the role of RT in HCC has been limited because of the risk of RILD
caused by whole liver irradiation. Improved knowledge of partial liver RT has created
renewed in using RT with HCC and, furthermore, technical advancements in 3DCRT
have allowed higher doses to targeted to the tumors while minimizing exposure of
surrounding liver tissue. Recently, more and more types of conformal RT have been
developed to deliver highly conformal treatment with minimal damage to surrounding
normal liver parenchyma, including IMRT, image-guided radiotherapy (IGRT) and
stereotactic body radiotherapy (SBRT) [24]. RapidArc is a novel form of volumetric
intensity-modulated RT that has the advantages of a short treatment time, fewer MUs
and the availability of highly conformal treatment plans. Several investigations have
demonstrated the advantages of RapidArc. Verbakel et al. demonstrated that RapidArc
achieved similar PTV coverage and OAR sparing but lower MUs than IMRT in
patients with head and neck cancers. Besides, double arc plans yielded better PTV
coverage than single arc or IMRT [16]. Palma et al. reported that variable dose rate
volumetric modulated arc therapy achieved better dose distribution and lower MUs
than IMRT in patients with prostate cancers. This work was a pilot study to
investigate the dosimetric difference of a RapidArc plan for HCC compared to
In our study, the homogeneity of the PTV provided by all three techniques was similar,
but the RapidArc was able to achieve better conformity and hot-spot sparing of the
PTV compared to IMRT or 3DCRT (p < 0.05). For OARs sparing, the three methods
showed comparable results in terms of the mean dose to the stomach and kidneys and
maximum dose to the spinal cord. For the normal liver, 3DCRT provided the worst
dose distribution, with significantly worse Dmean, V40Gy, V30Gy, and NTCP values than
RapidArc or IMRT. Compared with IMRT, RapidArc provided comparable V40Gy,
V30Gy, and NTCP values for the normal liver, but RapidArc achieved significantly
higher Dmean, V20Gy and V10Gy values for the normal liver.
The Lyman NTCP model has been widely used to predict or estimate the probability
of normal tissue complication. This model supposed there is a sigmoid relationship
between a uniform radiation dose given to a part of the volume in an organ and the
probability of complication. More and more authors have used this model to predict
RILD. Burman et al. assigned the parameters to be as follows, n as 0.32, m as 0.15,
and TD50(1) as 40 Gy, in a model that predict the risked of RILD [23]. Cheng et al.
applied the values of n = 0.35, m = 0.35 and TD50(1) = 49.4 Gy in another model [25].
Dawson et al. further modified the parameter TD50(1) to 39.8 Gy for hepatobiliary
cancer and to 45.8 Gy for liver metastasis (n = 0.97 and m = 0.12) [26]. Although
different authors, they demonstrated the feasibility of partial liver irradiation. If the
TD50 is kept constant, the NTCP value is represented as a function of partial volume.
This organ demonstrates a “threshold type behavior” and the NTCP value will rise
only if a certain volume is irradiated. Furthermore, the NTCP value of the partial
volume depends on the dose. Therefore, we believe that the V40Gy and V30Gy influence
the NTCP values of the normal liver more than V20Gy and V10Gy do. In addition,
Dawson et al. also addressed whether those who had impaired liver function might
not be suitable for the Lyman NTCP model and whether a better understanding of the
mechanism of RILD may improve the accuracy of Lyman model in the future.
In addition to value used for NTCP, the V30Gy and Dmean of the normal liver play
important roles in predicting the risk of RILD. Dawson et al. demonstrated that the
Dmean of normal liver was associated with the risk of RILD [26]. Yamada et al.
reported a deterioration in the Child-Pugh Score in 5 out of 6 patients with a V30Gy >
40%, vs. 2 of 13 patients with a V30Gy < 40% (p < 0.01) [27].
Another issue that should be kept in mind is the higher low-dose irradiation to normal
liver compared with 3DCRT or IMRT when RapidArc is used. Shueng et al. published
a case of cholangiocarcinoma with bone metastasis who had received palliative RT for
bone pain who developed radiation pneumonitis [28]. They demonstrated that, in this
radiation pneumonitis. One of the possible causes is an interaction between
radiation-induced inflammation within the previously irradiated field and
chemotherapy. Yamashita et al. has reported that the incidence of lung toxicity will
become higher if large amount of low dose radiation is delivered [29]. In addition to
the dosimetric impact, several investigators reported that some biological factors are
associated with RILD. For example, Cheng et al. reported that the HBV carriers or
cases with Child-Pugh B cirrhosis were correlated with the risk of RILD after
3D-CRT [25]. Xu et al. also reported that the Child-Pugh classification was associated
with RILD [30]. In the current study, the potential risk of RILD caused by low-dose
irradiation is unclear, but HCC patients in Taiwan usually have hepatitis B or C
infection and liver cirrhosis and they usually received TACE, PEI or targeted therapy
before RT. Radiation oncologists should be aware of the potential risk of higher
low-dose exposure to the normal liver when RapidArc is used.
From the view of dosimetric comparison, one of the reasons that RapidArc is not
better than IMRT for liver protection may be that HCC is always surrounded by
normal liver parenchyma, which is the major concern when using the volumetric
RapidArc technique. In our study, we found that RapidArc increased the V10Gy , V20Gy
and Dmean of the normal liver compared to IMRT and, therefore, we suggest that the
RapidArc and IMRT achieve equivalent V30Gy for the normal liver and have similar
NTCP values.
Another advantage of RapidArc over IMRT were the reduction in the number of MUs.
Several studies have reported that the disadvantages of IMRT include higher MUs,
longer delivery times, and more low-dose exposure of organs at risk (OARs), all of
which increase the risk of a radiation-induced second malignancy. Hall reported that
IMRT, as compared with 3DCRT, might double the incidence of solid cancers in
long-term survivors, especially children [31]. Zwahlen studied the cancer risk after
IMRT for cervical and endometrial cancer and reported that cumulative second cancer
risks (SCR) relative to 3DCRT for 6-MV and 18-MV IMRT plans were +6% and
+26%, respectively [32]. There is no sufficient data to demonstrate that the lower
MUs associated with RapidArc might reduce the risk of radiation-induced second
malignancy. Furthermore, radiation-induced second malignancy occurs only in those
who have long-term survival after treatment. Xu et al. reported that the 5-year
survival rate for HCC patients receiving TACE plus RT was only 13% with a median
survival time of 18 months [33]. Thus this advantage of RapidArc may have little
influence on the prevention of radiation-induced second malignancy for HCC patients.
Verbakel WF et al. [16] and Wagner et al. [34] compared RapidArc with IMRT for
IMRT were the lower MUs and the shorter treatment time, which can be beneficial to
the reduction of intra-fractional movement, improving patient comfort, and higher
patient throughput.
Although RapidArc has been demonstrated the advantages on the treatment of
other kinds of malignancies, the dosimetric advantage of RapidArc in our study is not
always better than IMRT. Therefore it is not convincing that IMRT should be replaced
by RapidArc when treating HCC. The limitations of our study include small patient
numbers, relatively coarse 5 mm-slice thickness and a lack of respiratory control or
abdominal compression. These limitations would possibly cause some errors in the
dose calculation and analysis. Clinical trials and long-term follow-up are required to
draw more definite conclusions. Therefore, we suggest that if PTV conformity and
percentages of NTCP, Dmean, V30Gy and V10Gy of the normal liver are acceptable,
RapidArc may be selected on the basis of fewer MUs. If PTV coverage is not
adequate or each of the above parameters related to liver toxicity is too high with
RapidArc, then IMRT should be used.
In conclusion, RapidArc obtained favorable tumor coverage compared with
IMRT and both RapidArc and IMRT achieved significantly better quality in terms of
treatment plan when compared with 3DCRT. However, RapidArc is not superior to
optimization of its algorithm is still in its early stages (about 2 years of clinical
experience), whereas 3DCRT and IMRT have been well-investigated and routinely
used for more than 10 years. It is expected that more comprehensive planning systems
for RapidArc are being developed and these might advance the optimization process
Competing interests
The author(s) declare that they have no competing interests.
Authors' contributions
Yu-Cheng Kuo and Hsiao-Wei Yu contributed significantly to study design and
concept. Yu-Cheng Kuo also contributed to manuscript writing and study coordinator.
Ying-Ming Chiu and Chia-Wen Chen contributed to statistical analysis. Wen-Pin Shih
and Wei-Chan Lin contributed significantly to the acquisition of data and optimization
of treatment plans. Pei-Fong Wong and Jeng-Jong Hwang contributed to final revision
of manuscript. All authors read and approved the final manuscript.
REFERENCES
1. Bosch FX, Ribes J, Diaz M, Cleries R: Primary liver cancer: worldwide
incidence and trends. Gastroenterology 2004, 127:S5-S16.
2. Ohto M, Yoshikawa M, Saisho H, Ebara M, Sugiura N: Nonsurgical treatment
of hepatocellular carcinoma in cirrhotic patients. World J Surg 1995,
3. Cheng AL, Kang YK, Chen Z, Tsao CJ, Qin S, Kim JS, Luo R, Feng J, Ye S,
Yang TS, Xu J, Sun Y, Liang H, Liu J, Wang J, Tak WY, Pan H, Burock K, Zou
J, Voliotis D, Guan Z: Efficacy and safety of sorafenib in patients in the
Asia-Pacific region with advanced hepatocellular carcinoma: a phase III
randomised, double-blind, placebo-controlled trial. Lancet Oncol 2009,
10:25-34.
4. Kuvshinoff BW, Ota DM: Radiofrequency ablation of liver tumors: influence
of technique and tumor size. Surgery 2002, 132:605-612.
5. Camma C, Schepis F, Orlando A, Albanese M, Shahied L, Trevisani F, Andreone
P, Craxi A, Cottone M: Transarterial chemoembolization for unresectable
hepatocellular carcinoma: meta-analysis of randomized controlled trials.
Radiology 2002, 224:47-54.
6. Tateishi R, Shiina S, Teratani T, Obi S, Sato S, Koike Y, Fujishima T, Yoshida H,
Kawabe T, Omata M: Percutaneous radiofrequency ablation for
hepatocellular carcinoma. An analysis of 1000 cases. Cancer 2005,
103:1201-1209.
7. Stillwagon GB, Order SE, Guse C, Klein JL, Leichner PK, Leibel SA, Fishman
EK: 194 hepatocellular cancers treated by radiation and chemotherapy
Study. Int J Radiat Oncol Biol Phys 1989, 17:1223-1229.
8. Lawrence TS, Robertson JM, Anscher MS, Jirtle RL, Ensminger WD, Fajardo
LF: Hepatic toxicity resulting from cancer treatment. Int J Radiat Oncol Biol
Phys 1995, 31:1237-1248.
9. Tse RV, Guha C, Dawson LA: Conformal radiotherapy for hepatocellular
carcinoma. Crit Rev Oncol Hematol 2008, 67:113-123.
10. Dawson LA, McGinn CJ, Normolle D, Ten Haken RK, Walker S, Ensminger W,
Lawrence TS: Escalated focal liver radiation and concurrent hepatic artery
fluorodeoxyuridine for unresectable intrahepatic malignancies. J Clin Oncol
2000, 18:2210-2218.
11. Emami B, Lyman J, Brown A, Coia L, Goitein M, Munzenrider JE, Shank B,
Solin LJ, Wesson M: Tolerance of normal tissue to therapeutic irradiation.
Int J Radiat Oncol Biol Phys 1991, 21:109-122.
12. Dawson LA, Ten Haken RK: Partial volume tolerance of the liver to radiation.
Semin Radiat Oncol 2005, 15:279-283.
13. Park HC, Seong J, Han KH, Chon CY, Moon YM, Suh CO: Dose-response
relationship in local radiotherapy for hepatocellular carcinoma. Int J Radiat
Oncol Biol Phys 2002, 54:150-155.
Huang AT: Dosimetric analysis and comparison of three-dimensional
conformal radiotherapy and intensity-modulated radiation therapy for
patients with hepatocellular carcinoma and radiation-induced liver disease.
Int J Radiat Oncol Biol Phys 2003, 56:229-234.
15. Fuss M, Salter BJ, Herman TS, Thomas CR, Jr: External beam radiation
therapy for hepatocellular carcinoma: potential of intensity-modulated and
image-guided radiation therapy. Gastroenterology 2004, 127:S206-217.
16. Verbakel WF, Cuijpers JP, Hoffmans D, Bieker M, Slotman BJ, Senan S:
Volumetric intensity-modulated arc therapy vs. conventional IMRT in
head-and-neck cancer: a comparative planning and dosimetric study. Int J
Radiat Oncol Biol Phys 2009, 74:252-259.
17. Yoo S, Wu QJ, Lee WR, Yin FF: Radiotherapy treatment plans with
RapidArc for prostate cancer involving seminal vesicles and lymph nodes.
Int J Radiat Oncol Biol Phys 2010, 76:935-942.
18. Palma D, Vollans E, James K, Nakano S, Shaffer R, Mckenzie M, Morris J, Otto
K: Volumetric modulated arc therapy for delivery of prostate radiotherapy:
comparison with intensity-modulated radiotherapy and three-dimensional
conformal radiotherapy. Int J Radiat Oncol Biol Phys 2008, 72:996-1001.
in radiotherapy for unresectable hepatocellular carcinoma: a retrospective
study of 158 patients. Int J Radiat Oncol Biol Phys 2003, 55:329-336.
20. Cahlon O, Hunt M, Zelefsky MJ: Intensity-modulated radiation therapy:
supportive data for prostate cancer. Semin Radiat Oncol 2008, 18:48-57.
21. Wang X, Zhang X, Dong L, Liu H, Gillin M, Ahamad A, Ang K, Mohan R:
Effectiveness of noncoplanar IMRT planning using a parallelized
multiresolution beam angle optimization method for paranasal sinus
carcinoma. Int J Radiat Oncol Biol Phys 2005, 63:594-601.
22. Warkentin B, Stavrev P, Stavreva N , Field C, Fallone BG: A TCP-NTCP
estimation module using DVHs and known radiobiological models and
parameter sets. J Appl Clin Med Phys 2004, 5:50-63.
23. Burman C, Kutcher GJ, Emami B, Goitein M: Fitting of normal tissue
tolerance data to an analytic function. Int J Radiat Oncol Biol Phys 1991,
21:123-135.
24. Wulf J, Guckenberger M, Haedinger U, Oppitz U, Mueller G, Baier K, Flentje M:
Stereotactic radiotherapy of primary liver cancer and hepatic metastases.
Acta Oncol 2006, 45:838-847.
25. Cheng JC, Wu JK, Lee PC, Liu HS, Jian JJ, Lin YM, Sung JL, Jan GJ:
radiotherapy to radiation-induced liver disease. Int J Radiat Oncol Biol Phys
2004, 60:1502-1509.
26. Dawson LA, Normolle D, Balter JM, McGinn CJ, Lawrence TS, Ten Haken RK:
Analysis of radiation-induced liver disease using the Lyman NTCP model.
Int J Radiat Oncol Biol Phys 2002, 53:810-821.
27. Yamada K, Izaki K, Sugimoto K, Mayahara H, Morita Y, Yoden E, Matsumoto S,
Soejima T, Sugimura K: Prospective trial of combined transcatheter arterial
chemoembolization and three-dimensional conformal radiotherapy for
portal vein tumor thrombus in patients with unresectable hepatocellular
carcinoma. Int J Radiat Oncol Biol Phys 2003, 57:113-119.
28. Shueng PW, Lin SC, Chang HT, Chong NS, Chen YJ, Wang LY, Hsieh YP, Hsieh
CH: Toxicity risk of non-target organs at risk receiving low-dose radiation:
case report. Radiat Oncol 2009, 4:71.
29. Yamashita H, Nakagawa K, Nakamura N, Koyanagi H, Tago M, Igaki H,
Shiraishi K, Sasano N, Ohtomo K: Exceptionally high incidence of
symptomatic grade 2-5 radiation pneumonitis after stereotactic radiation
therapy for lung tumors. Radiat Oncol 2007, 2:21.
30. Xu ZY, Liang SX, Zhu J, Zhu XD. Zhao JD, Lu HJ, Yang YL, Chen L, Wang AY,
normal-tissue complication probability model in three-dimensional
conformal radiation therapy for primary liver carcinoma. Int J Radiat Oncol
Biol Phys 2006, 65:189-195.
31. Hall EJ: Intensity-modulated radiation therapy, protons, and the risk of
second cancers. Int J Radiat Oncol Biol Phys 2006, 65:1-7.
32. Zwahlen DR, Ruben JD, Jones P, Gagliardi F, Millar JL, Schneider U: Effect of
intensity-modulated pelvic radiotherapy on second cancer risk in the
postoperative treatment of endometrial and cervical cancer. Int J Radiat
Oncol Biol Phys 2009, 74:539-545.
33. Xu LT, Zhou ZH, Lin JH, Chen Z, Wang K, Wang P, Zhu XY, Shen YH, Meng
ZQ, Liu LM: Clinical study of transarterial chemoembolization combined
with 3-dimensional conformal radiotherapy for hepatocellular carcinoma.
Eur J Surg Oncol 2011, 37:245-251.
34. Wagner D, Christiansen H, Wolff H, Vorwerk H: Radiotherapy of malignant
gliomas: comparison of volumetric single arc technique (RapidArc),
dynamic intensity-modulated technique and 3D conformal technique.
Figure Legends
Figure 1: The comparison of isodose distributions of PTV and OAR in 3DCRT,
IMRT and RapidArc. A: 3DCRT, B: IMRT and C: RapidArc. RapidArc achieved
better conformality to the 95% isodose line (red line) of the PTV and better spinal
cord sparing to the 50% isodose line (yellow line) as compared with 3DCRT and
IMRT. However, RapidArc obtained higher 30%-isodose coverage (blue line) of
volume of the normal liver than did 3DCRT and IMRT.
Figure 2: The comparison of DVHs for PTV and normal liver in 3DCRT, IMRT and
RapidArc. Right figure = DVHs of PTV. These three techniques produced similar
homogeneity of the PTV. Left figure = DVHs of normal liver. RapidArc obtained the
higher low-dose distribution in the normal liver compared with 3DCRT and IMRT. On
the other hand, 3DCRT obtained the high-dose distribution in the normal liver
Table 1 The dose constraints of organ at risk
OAR Dose constraints
Normal liver Mean dose < 26Gy
Stomach Maximum dose < 54 Gy
Kidney At least one side of kidney < 23 Gy (mean dose)
Spinal cord Maximum dose < 47 Gy
(Maximum dose of spinal cord plus 5-mm margin < 45 Gy)
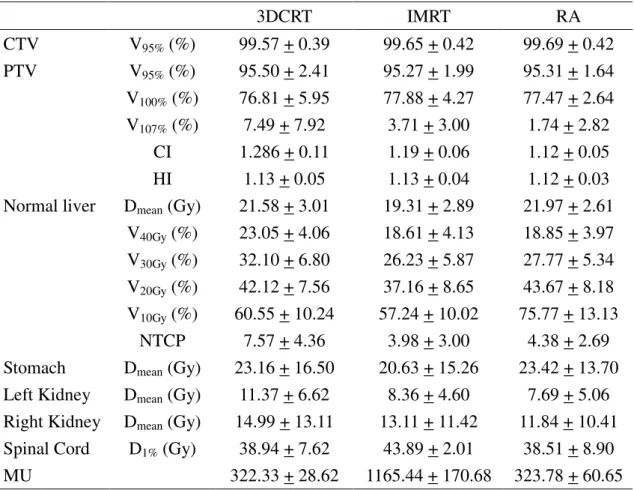
Table 2 The summary of all investigated DVH-parameters as mean values + standard deviation (SD) 3DCRT IMRT RA CTV V95% (%) 99.57 + 0.39 99.65 + 0.42 99.69 + 0.42 PTV V95% (%) 95.50 + 2.41 95.27 + 1.99 95.31 + 1.64 V100% (%) 76.81 + 5.95 77.88 + 4.27 77.47 + 2.64 V107% (%) 7.49 + 7.92 3.71 + 3.00 1.74 + 2.82 CI 1.286 + 0.11 1.19 + 0.06 1.12 + 0.05 HI 1.13 + 0.05 1.13 + 0.04 1.12 + 0.03
Normal liver Dmean (Gy) 21.58 + 3.01 19.31 + 2.89 21.97 + 2.61
V40Gy (%) 23.05 + 4.06 18.61 + 4.13 18.85 + 3.97
V30Gy (%) 32.10 + 6.80 26.23 + 5.87 27.77 + 5.34
V20Gy (%) 42.12 + 7.56 37.16 + 8.65 43.67 + 8.18
V10Gy (%) 60.55 + 10.24 57.24 + 10.02 75.77 + 13.13
NTCP 7.57 + 4.36 3.98 + 3.00 4.38 + 2.69
Stomach Dmean (Gy) 23.16 + 16.50 20.63 + 15.26 23.42 + 13.70
Left Kidney Dmean (Gy) 11.37 + 6.62 8.36 + 4.60 7.69 + 5.06
Right Kidney Dmean (Gy) 14.99 + 13.11 13.11 + 11.42 11.84 + 10.41
Spinal Cord D1% (Gy) 38.94 + 7.62 43.89 + 2.01 38.51 + 8.90
MU 322.33 + 28.62 1165.44 + 170.68 323.78 + 60.65
PTV: planned tumor volume; MU: monitor unit; 3DCRT: 3-D conformal radiation therapy; IMRT: intensity-modulated radiation therapy; RA: RapidArc.
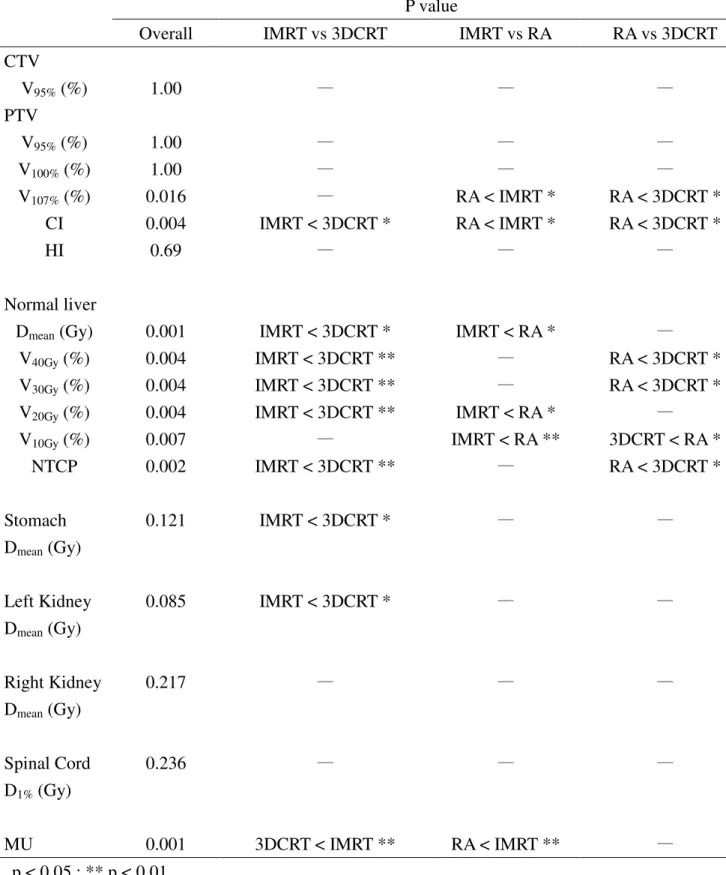
Table 3 All differences among three methods with regard to the DVH-parameters P value
Overall IMRT vs 3DCRT IMRT vs RA RA vs 3DCRT
CTV V95% (%) 1.00 — — — PTV V95% (%) 1.00 — — — V100% (%) 1.00 — — — V107% (%) 0.016 — RA < IMRT * RA < 3DCRT * CI 0.004 IMRT < 3DCRT * RA < IMRT * RA < 3DCRT * HI 0.69 — — — Normal liver
Dmean (Gy) 0.001 IMRT < 3DCRT * IMRT < RA * —
V40Gy (%) 0.004 IMRT < 3DCRT ** — RA < 3DCRT *
V30Gy (%) 0.004 IMRT < 3DCRT ** — RA < 3DCRT *
V20Gy (%) 0.004 IMRT < 3DCRT ** IMRT < RA * —
V10Gy (%) 0.007 — IMRT < RA ** 3DCRT < RA * NTCP 0.002 IMRT < 3DCRT ** — RA < 3DCRT * Stomach Dmean (Gy) 0.121 IMRT < 3DCRT * — — Left Kidney Dmean (Gy) 0.085 IMRT < 3DCRT * — — Right Kidney Dmean (Gy) 0.217 — — — Spinal Cord D1% (Gy) 0.236 — — — MU 0.001 3DCRT < IMRT ** RA < IMRT ** — p < 0.05 ; ** p < 0.01
PTV: planned tumor volume; Vx%: the volume receiving > x% of the prescribed dose;
VnGy: the percentage of organ volume receiving > n Gy; CI: conformity index; HI:
volume for the organ; MU: monitor unit; 3DCRT: 3-D conformal radiation therapy; IMRT: intensity-modulated radiation therapy; RA: RapidArc.