For Peer Review Only
A hierarchical Bayesian approach for risk assessment of melamine in infant formula based on cases of related
nephrolithiasis in children
Journal: Food Additives and Contaminants Manuscript ID: TFAC-2010-242.R1
Manuscript Type: Original Research Paper Date Submitted by the
Author: n/a
Complete List of Authors: Wang, I-Jen; Department of Pediatrics, Taipei Hospital Department of Health; College of Public Health, China Medical University; College of Medicine, Fu Jen Catholic University
Chen, Chu-Chih; Division of Biostatistics and Bioinformatics, Institutes of Population Health Sciences, National Health Research Institutes
Chan, Chang-Chuan; Institute of Occupational Medicine and Industrial Hygiene, National Taiwan University College of Public Health
Chen, Pau-Chung; Institute of Occupational Medicine and Industrial Hygiene, National Taiwan University College of Public Health Leonardi, Giovanni; Health Protection Agency, Center for Radiation, Chemical and Environmental Hazards, Chemical Hazards and Poisons Division
Wu, Kuen-Yuh; Institute of Occupational Medicine and Industrial Hygiene, National Taiwan University College of Public Health Methods/Techniques: Risk assessment, Risk assessment - modelling
For Peer Review Only
2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49For Peer Review Only
Abstract
Although the 2008 outbreak of nephrolithiasis in children due to melamine-contaminated infant formula has subsided, it remains uncertainwhether the present tolerable daily intake (TDI) of
melamine provides sufficient protection for young children. To conduct a safety assessment for melamine in infant formula, we established a dose-response relationship based on 13
nephrolithiasis cases selected from 932 children, all of whom were under five years of age and
had potentially been exposed to tainted milk in China or Taiwan. According to the children’s exposure history, distributions of individual daily melamine intake (mg/kg bw/d) were
reconstructed using Monte Carlo simulations to account for uncertainties in exposure duration
and melamine concentrations in the tainted milk. Based on the simulated individual average daily intake (AVDI) of melamine, subjects were further classified into four separate AVDI groups:
high, medium, low and a reference group. A statistical logistic model was then fitted for the dose-response relationship between nephrolithiasis incidence and daily melamine intakes using
Markov chain Monte Carlo (MCMC) simulations. Based on the background exposure,
spontaneous rate, and mode of action (MOA) of nephrolithiasis in children, the simulated lower bounds of the 95% CIs daily melamine intake ranged from0.008 to 0.03 mg/kg bw/d
corresponding toan additional risks of 0.1%is proposed as a plausible TDI,which is
approximately an order lower than the current WHO-suggested TDI level of 0.2 mg/kg bw/d. More stringent regulations on melamine levels in infant formula should be considered to protect
young children fully.
Keywords: average daily intake; dose-response; exposure assessment; Markov chain Monte Carlo simulation; Monte Carlo simulations; probabilistic modeling; uncertainty
Deleted: T Deleted: of
Deleted: daily melamine intakes of Deleted: the
Deleted: 1 Deleted: .0 × 10−4
, 5.0 × 10−4 and 1.0 × 10−5
Deleted: were 0.0034, 0.0019 and
0.0006 mg/kg bw/d, respectively
Deleted: ,
Deleted: which were two to Deleted: three Deleted: s Deleted: adopt 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49
For Peer Review Only
Introduction
Melamine, also known as cyanuramide, is a manmade substance commonly used in manufactured products, including dishes, housewares, plastic resins, dry erase boards and industrial coatings
(Ingelfinger 2008). Although melamine is of low acute toxicity, long-term excessive exposure in animals causes bladder stones, damage to the urinary system, and may induce bladder cancer
(IARC 1999).Young children are extremely vulnerable to melamine-related toxicity because of
the immaturity of their organs and the fact that infant formula may constitute their sole source of nutrition (US FDA/CFSAN 2008a). In addition, infants who consume adulterated formula with
high levels of melamine may receive inadequate protein in their diet. Because the basal serum
uric acid levels and urine-filtered levels of infants are higher than those of adults, they are therefore are more likely to form uric acid stones (WHO 2009a). The recent tainted milk scandal
in China that caused more than 50,000 cases of renal disease and the deaths of several children has raised serious public health concerns worldwide, especially after traces of melamine were
detected in top-selling U.S. infant formulas (Ingelfinger 2008; US FDA/CFSAN 2008b). Similar
concerns were also raised in Taiwan after it was discovered that dairy products imported from China were tainted with melamine.
In 2007, the US Food and Drug Administration (FDA) published a tolerable daily intake
(TDI) for melamine of 0.63 mg/kg bw/d. This information was released following numerous reports of kidney failure and death in pets due to consumption of pet foods contaminated with
high concentrations of melamine (US FDA/CFSAN 2008a). However, the assessment was based on an animal study of rats fed with melamine for 13 weeks (US FDA/CFSAN 2008a). Following
the finding that concomitant exposure to cyanuric acid and melamine may act synergistically to
produce crystalluria in animals (Reimschuessel et al. 2008), the FDA revised the TDI to 0.063
2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49
For Peer Review Only
mg/kg bw/d in October of 2008 by applying an additional tenfold safety factor for uncertainty
(US FDA/CFSAN 2008a). To set a TDI of melamine to protect consumers from adverse health
effects, the World Health Organization (WHOa) held an expert meeting in December of 2008; they suggested a TDI level of 0.2 mg/kg bw/d that would be applicable to the whole population,
including infants (WHO 2009). Much like the recommendation of the FDA, however, the dose-response assessment was based on a sub-chronic animal study. Because the renal systems of
young children are too immature to ward off the impact of the chemical, and because infants
depend mainly on formula as their source of nutrition (US FDA/CFSAN 2008a, 2008b), the recommended TDI level of 0.2 mg/kg bw/d said to be applicable for the entire population may
need to be reassessed. In addition, unlike the pet food contamination incident with comparable
levels of melamine and cyanuric acid, the levels of its analogues (cyanuric acid, ammeline, and ammelide) contained in the adulterated infant formula were found to be only about 0.1% of the
melamine levels (WHO 2009a). Furthermore, exposure in infants is chronic, occurs over several months, and is not mitigated by previous passage through the digestive system of an animal (US
FDA/CFSAN 2008a). Therefore, the exposure scenario of the diseased young children was quite
different from that of the pet food contamination episode and other animal studies. The establishment of a safe level of melamine content in infant formula is of great importance,
especially for infants and young children who are more susceptible to melamine exposure.
In this paper, incidents of melamine-related and unrelated nephrolithiasis diagnosed among 932 young children under five years of age were modeled based on their history of melamine
exposure to generate a safety assessment. A two-stage probabilistic approach in establishing the dose-response model was adopted. At the first stage, we estimated the distributions of AVDIs of
melamine using Monte Carlo (MC) simulation to serve as prior information for later model fitting.
At the second stage, individuals were categorized into disjoint AVDI groups based on the
Deleted: the 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49
For Peer Review Only
estimated AVDIs, and a statistical model was fitted for the dose-response relationship using
Markov chain Monte Carlo (MCMC) simulations. Using the mathematical convergence property
of MCMC simulations with the fitted dose-response model, the posterior distributions of the group mean AVDIs were narrowed down from the prior distributions. Thus, uncertainties in
determining the subgroup means of AVDI melamine intake were reduced to reliably assess the various additional risks of nephrolithiasis.
Materials and methods
Study population
A total of 1222 children who may have consumed melamine-tainted dairy products were screened at three Department of Health hospitals in Taiwan for possible kidney problems. All of the
participants were between 0 and 16 years of age, and screenings took place from September 24 to October 31, 2008. The majorities of the diseased young children were less than three years of age
and were mainly dependent on the tainted infant formula as their major nutrition source (US
FDA/CFSAN 2008a). Taking into account age susceptibility to melamine exposure, 932 children under five years of age were analyzed for the present study, which was approved by the hospital
ethics committee. Children born prematurely and those with congenital abnormalities of the
genitourinary tract or chronic diseases were excluded from participation. Figure 1 illustrates the procedure for screening and classifying the subjects.
(Figure 1)
Exposure information and case definition
2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49
For Peer Review Only
Parents were interviewed with questionnaires administered by pediatricians. Background
information, including age, sex, body weight (BW), residential history in China, past history of
urinary tract infection (UTI) or vesico-urethra reflux, family history of nephrolithiasis, and clinical symptoms (e.g., flank pain, dysuria, urinary frequency, decreased urine output,
unexplained fever, etc.) were collected. Possible consumption of melamine-tainted dairy products, including infant formula, milk drinks, yogurt, ice cream, chocolate biscuits, and powdered cheese,
were also itemized in the questionnaires, along with average quantities of products consumed per
day, frequency of feeding, and consumption periods of the products on the list (e.g., milk powder brands Sanlu, Mengniu, Yili and Yashili produced in China or other brands imported from China)
(IFSAN 2008; Taipei Bureau of Health 2008). Parents were asked to estimate the amount of milk
consumption using the volume of the feeding bottle or the sample spoon included with the infant formula.
According to the subjects’ exposure history, eight contaminated dairy products on the questionnaire list were identified, with melamine concentrations ranging from 0.1 to 2563 mg
kg-1 (IFSAN 2008). More recent analyses showed that individual samples ranged up to 4700 mg/kg (WHO 2009a). Based on the brand(s) of milk powder they consumed, subjects were classified into the high exposure group, who consumed highly contaminated dairy products in
China with melamine levels > 2.5 mg/kg; the low exposure group, who consumed other brands of
less-tainted milk powder ranged from 0.123 to 2.02 mg/kg (Taipei Bureau of Health 2008) imported from China; and the control group, who consumed milk powder with no detectable
melamine (<0.05 mg/kg detection limit). Blood pressure, urinalysis, urine calcium and creatinine, renal function tests, parathyroid hormone test, and renal ultrasonography were evaluated. Renal
ultrasonography was performed by experienced pediatricians. Positive findings were
cross-checked by experienced urologists before being reported. Cases of melamine-related
Formatted: Left, Indent: First
line: 1.5 ch 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49
For Peer Review Only
nephrolithiasis were defined as nephrolithiasis in children who were fed with melamine-tainted
infant formula. Details of the clinical diagnosis are described in Wang et al. (2009).
Probabilistic modeling of individual average daily intake of melamine
Because of great uncertainties involved in determining individual exposure duration as well as melamine content(s) in the infant formula(s), it was more appropriate to adopt a probabilistic
approach for estimating the corresponding AVDI. Probabilistic exposure assessment has recently
become popular for assessing pesticide residues or mycotoxins in food consumptions (rather than deterministic approach); this approach has the advantages of taking into account the probabilistic
distribution of the exposure and the ability to quantify variability and uncertainty (Claeys et al.
2008; Jensen et al. 2008; Kuiper-Goodman et al. 2010).
We performed Monte Carlo simulations to generate the empirical distribution of individual
AVDI using the equation:
AT BW ED I C AVDI M M × × × = , (1)
where CM is the melamine content in milk powder, IM is the daily consumption rate of milk
powder, ED is the exposure duration of the tainted milk powder consumption, BW is the child’s
current body weight, and AT is the average time that the child was diagnosed with a kidney stone.
To avoid possible recall bias, the individual exposure duration and the amount of melamine intake were estimated based on the questionnaire. A lognormal distribution was then fitted
separately to each of the variables, CM, IM, ED and BW, using MC simulation to obtain the
individuals’ empirical AVDIs and account for uncertainties. The corresponding means and
standard deviations (SDs) were determined from information on the questionnaire. The
lognormal distribution of the melamine content was found to be appropriate for Klim, Nesalac
Formatted: Font: Italic Formatted: Font: Italic
Formatted: Font: Italic Formatted: Font: Italic
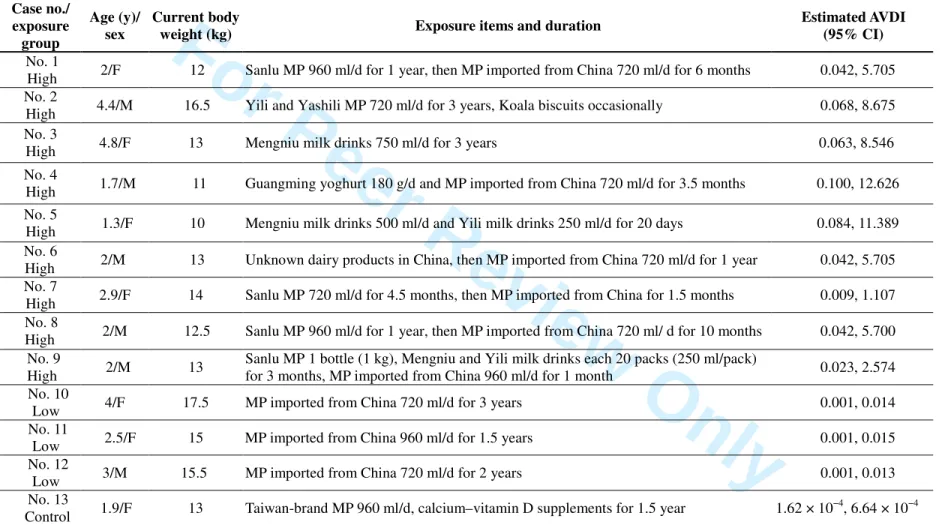
Deleted: Table 1 summarizes the
backgrounds and exposure histories of the cases.¶ (Table 1) Deleted: following Deleted: (Table 1) 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49
For Peer Review Only
and other milk powders manufactured in China (IFSAN 2008; Taipei Bureau of Health 2008).
The melamine contents of the 22 brands of melamine-tainted milk powder were officially
analyzed and released by either the Chinese government or the individual manufacturer (IFSAN 2008). The melamine content means (SD) for the less-tainted Klim and Neslac milk powder
imported from China and sold in Taiwan were 0.59 (0.34) (n = 9) and 0.57 (0.44) (n = 15) mg/kg, respectively. The mean (SD) of milk powder such as Sanlu, Yili and Yashili (produced in China)
was 181 (546.50) (n = 22) mg/kg. Table 1 summarizes the range, mean, and SD of the melamine
concentrations used in simulating the individual AVDIs. (Table 1)
The consumption rates of milk powder per day likely varied with age but were also assumed
to have a lognormal distribution based on the producers’ daily recommendation. However, because the possible continuous melamine exposure lasted less than one year (US FDA/CFSAN
2008b), the current consumption rate was assumed as the mean of the lognormal distribution. The mean and SD of the lognormal distribution of the children’s ED were estimated based on their
residential history in China and the possible continuous exposure to adulterated melamine that
could have lasted up to 12 months (US FDA/CFSAN 2008b). Similar assumptions were made about individuals’ body weight (mean (SD) of 10 (2) kg) due to weight changes occurring
between zero and five years of age (with the exception of case No. 9, who had a bodyweight of
13 kg at the clinic and consumed Sanlu milk powder for only one month). For children who consumed milk powder with undetectable melamine, the mean melamine content was taken to be
one-half of the limit of detection and quantitation (LOD/LOQ), measured by liquid
chromatography coupled with tandem mass spectrometry (LC-MS/MS). This value is reported to
vary from 0.004 to 0.5 mg/kg (Chan et al. 2009; Tittlemier 2010; WHO 2009a). Ten thousand
MC simulations were repeatedly sampled from the corresponding lognormal distributions of CM,
Formatted: Centered Formatted: Indent: First line:
1.5 ch
Formatted: Font: Italic
2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49
For Peer Review Only
IM, ED, and BW using Crystal Ball software (Decisioneering, Denver, Col). Based on the
empirical distribution of the simulation outcomes, a lognormal distribution was assigned with
mean and SD determined from the obtained sample. This information served as the prior
distribution of the individual AVDI for the second stage statistical modeling. Because of a lack of
detailed milk consumption information for the children without nephrolithiasis in the low exposure and control groups (Wang et al. 2009), it was impossible to determine the individual
AVDIs of these two groups. Therefore, subjects could only be classified into disjoint exposure
categories for subsequent statistical modeling. The simulated AVDI distributions of the cases were assumed to be representative of the daily melamine intake of children in the corresponding
exposure subgroup.Table 2 summarizes the backgrounds and exposure histories of the individual
cases for the simulations.
(Table 2)
Hierarchical Bayesian modeling using Markov chain Monte Carlo simulations for dose-response
Following the preliminary estimation of individual melamine AVDIs, it was determined that the mean AVDIs belonged to four disjoint categories. To improve statistical model fitting in the
second stage, subjects were further classified into four AVDI groups according to estimated mean
AVDIs: high, medium, low and a reference group (>0.7; <0.7 but >0.1; <0.01 but >0.001; and <0.001 (mg/kg bw/d), respectively). None of the children presented estimated mean AVDIs that
fell within the range of 0.01 to 0.1 mg/kg bw/d. Children classified into the same AVDI group were assumed to share the same overall exposure histories and durations, and thus were expected
to have a common group mean, µ
[ ]
i , of melamine intake. The group mean, µ[ ]
i , was againFormatted: Font color: Auto Formatted: Centered Deleted: deriv Deleted: 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49
For Peer Review Only
assumed to have a lognormal distribution with mean and SD from their prior information. A
linear logistic model,
[ ]
[ ]
i[ ]
i p i p µ α α * 1 log = 0+ 1 − , (2)withµ
[ ]
i as the estimated dosage was then fitted for the corresponding risk, p[ ]
i , of kidney stones for the AVDI group, i , where i = 1, 2, 3 and 4 denotes the estimated mean AVDI group of <0.001, <0.01 but >0.001, <0.7 but >0.1, and >0.7 (mg/kg bw/d), respectively. Estimates of the model parameters, as well as the mean melamine intakes of each group, µ[ ]
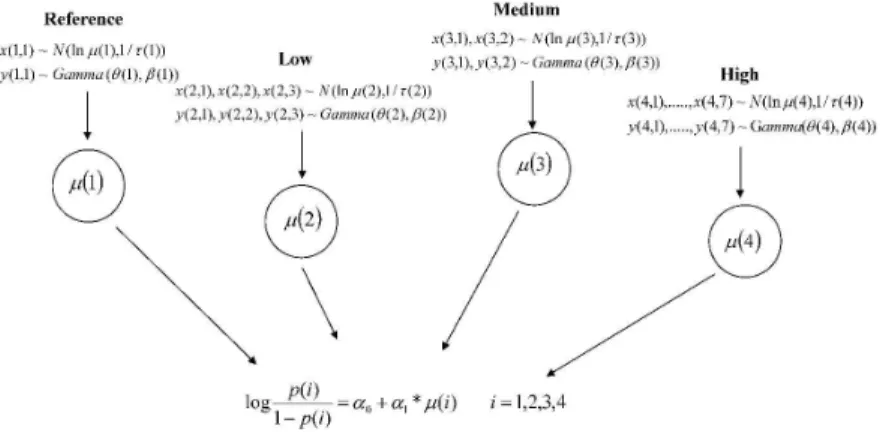
i , were obtained using a hierarchical Bayesian MCMC simulation procedure. Figure 2 illustrates the hierarchical Bayesian statistical modeling. The MCMC simulations were programmed using WinBUGS 1.4.3 software (MRC Biostatistics Unit 2008). Twenty thousand repeated samples from the stationary posterior distributions after convergence with a burn-in period of 10,000 were collected. The criterion that the Monte Carlo error for each parameter of interest be less than 5% of the sample SD was adopted in monitoring convergence of the Markov Chain process (WinBUGS user manual). Following the spirit of benchmark dose (BMD) calculation (Crump 1984; Crump et al. 2000; Wijngaarden et al. 2006), the BMD and the lower 95% CI bound (BMDL) corresponding to various levels of additional risk or benchmark response (BMR) were obtained. Specifically, based on the MCMC simulation outcomes, 95% CIs of µ[ ]
i , together with the AVDIscorresponding to the additional risks to the background risk, p[1], of the reference group at 10%, 1%, 1 × 10−3, 5 × 10−4, and 1 × 10−4, were estimated. For example, the dosage corresponding to an additional risk of 0.1 (denoted as td10) should satisfy the following equation:
( ) ( )1 * 10 9 . 0 1 . 0 1 ln 0 1 td p p α α + = − + . (3)
Details of the hierarchical structure of the model parameters are given in the Appendix.
Deleted: B Deleted: 5 Deleted: 5 × 10−3, Deleted: , 5 × 10−5 and 1 × 10−5 Deleted: assess Deleted: e Deleted: 05 Deleted: 05 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49
For Peer Review Only
(Figure 2)Sensitivity analyses
We conducted several sensitivity analyses to examine the impact of alternate exposure metrics and a dose-response model on calculating the corresponding risks. First, the estimated mean prior AVDIs of the high exposure group were lower than those reported by WHO (8.6 to 23.4 mg/kg bw/d) (WHO 2009a), and may have been underestimated for model fitting. We deliberately multiplied the prior mean AVDIs of two of the nine cases in the high exposure group by five and ten (separately) to observe the difference in estimated model parameters. Also, for sensitivity to the adopted LOD/LOQ level for the reference group, the melamine content was taken to be a constant 0 and a random variable (lognormal distributed) with alternative means 0.0025 and 0.25 mg/kg (half of the reported LOD/LOQs) separately.
For the impacts due to model uncertainty, we also fitted a probit model, (p
[ ]
i) α0 α1*µ[ ]
i 1 + = Φ− , (4)a commonly employed dose-response model alternative to a logistic model, where −1
( )
. Φ is theinverse of the cumulative distribution Φ( ). of a standard normal distribution.
Other sensitivity analyses involved exclusion criteria of the nephrolithiasis cases. No
instances of hypercalciuria, hyperparathyroidism, family history of nephrolithiasis, or past history of UTI were noted in our cases, with the exceptions of No. 3 (previous history of UTI) and No.
12 (family history of nephrolithiasis). A separate analysis was performed without these two cases.
Results 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49
For Peer Review Only
Of the 932 children who were screened, 13 were diagnosed with nephrolithiasis (12
melamine-related in the high and low exposure groups and one unrelated in the control group);
their mean age was 2.7 years (range = 1.3-4.8 years). Among the nephrolithiasis cases, nine were from the group of 34 children who consumed highly contaminated dairy products while residing
in China, three were from the group of 521 children who consumed other brands of
less-contaminated milk powder, and one was from the group of 377 children who consumed milk
without detectable melamine. Four of the nine cases in the high exposure group had been back in
Taiwan for more than six months (Nos. 1, 3, 6, and 8). Regarding clinical symptoms, most were asymptomatic; two cases involved urinary frequency (Nos. 2 and 3) (Table 2).
Probabilistic distribution and grouping average daily intake of melamine
AVDIs of melamine were reconstructed using Monte Carlo simulation. The empirical
distributions of the simulation outcomes conformed to the log-normal distributional assumption (not shown here). Although 34 of the children screened had spent time in China and consumed
highly tainted milk powder, the estimated mean AVDIs varied between 0.21 and 2.41 mg/kg
bw/d. The estimated mean AVDIs for the low exposure group and the control group were 0.006 and 3.6 × 10−4 mg/kg bw/d, respectively.
The number of subjects reclassified into the high, medium, low and reference AVDI groups
were 14, 19, 522 and 377, with seven, two, three and one case(s), respectively. Figure 1
summarizes the classification procedure of the participants. The exposure estimates of the group
AVDI means and the corresponding estimated risks with 95% CIs are summarized in Table 3. To help to interpret by policy makers and health investigators, Table 3 also lists the raw and the estimated relative risks (RR) of the exposed groups to the reference group. The reasonably close
mean estimated risks and the observed incidences (0.508, 0.076, 0.005 and 0.0049 versus 0.50,
Deleted: 1 Deleted: 4 Deleted: 59 Deleted: 0 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49
For Peer Review Only
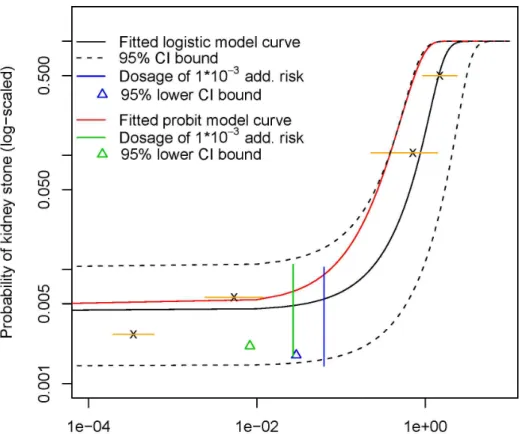
0.1053, 0.0057 and 0.0027 for the four groups, respectively) indicated that the model fitting was
quite successful, as shown in Figure 3. Although the prior distribution of individual melamine
AVDIs of the high AVDI group had a wide range due to great uncertainties in melamine contents (Table 2), the convergent posterior distribution had a relatively narrow 95% CI of (0.933, 2.38),
obtained from the 20,000 simulated MCMC samples. Similarly, the corresponding posterior 95% CIs of the medium, low and reference groups: (0.230, 1.40), (0.002, 0.012) and (1.96 × 10−4, 5.95 × 10−4), respectively, were much narrower than the individual values previously obtained. The raw and estimated RRs of the high exposure group to the reference group were approximately 189 and 104, indicating a strong dose-response effect of the melamine exposure. Similarly, the RRs of the medium exposure group exhibited a significant effect of the exposures. However, the estimated RR of 1.02 of the low exposure group compared to the reference group was
non-significant. Therefore, a likely point of departure (POD) of the kidney calculi due to melamine exposure could be slightly higher than the low exposure group estimated AVDI of 0.0058 mg/kg bw/d.
(Figure 3)
(Table 3)
Simulated melamine levels corresponding to different additional risks
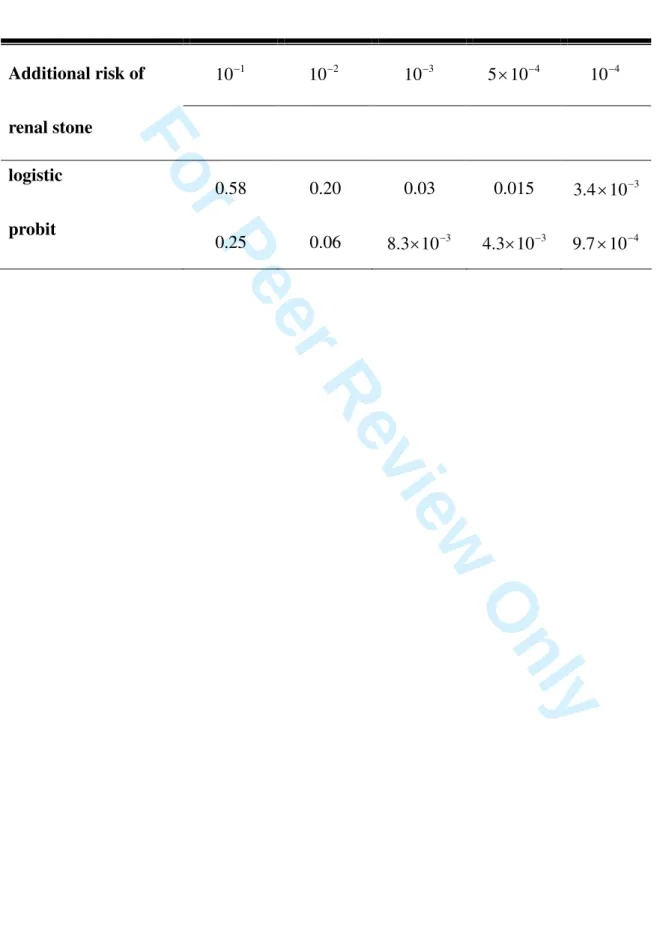
Based on the MCMC simulation results, the estimated median AVDIs of melamine at additional risks of nephrolithiasis, 1 × 10−2, 1 × 10−3 and 1 × 10−4, were 0.33, 0.056 and 6.5 × 10−3 (mg/kg bw/d), with corresponding lower bounds of 95% CI: 0.20, 0.03 and 3.4 × 10−3, respectively (Table4). Although we assumed a lognormal distribution for the group mean melamine daily
intake, µ
[ ]
i , the convergent posterior distributions had different shapes that were close to normalDeleted: . The closeness in model
fitting can also be observed
Deleted: 1 Deleted: 27 Deleted: 8 Deleted: 39 Deleted: 1 Deleted: 6.02 Deleted: di Deleted: 4 Deleted: 5 Deleted: 5 Deleted: 5 Deleted: 0065 Deleted: 035 Deleted: 9.87 Deleted: 4 Deleted: 0034 Deleted: 019 Deleted: 6 Deleted: 2 Deleted: 4 Deleted: Figure Deleted: 3 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49
For Peer Review Only
distributions (not shown here). Therefore, the simulation results were insensitive to the lognormal
prior distributional assumption of AVDIs at the first stage. The additional risk and its
corresponding AVDI are summarized in Table 4. (Table 4)
Sensitivity analyses
We deliberately multiplied the prior mean AVDIs of two of the nine cases in the high exposure
group by fivefold and tenfold (separately) for sensitivity to the relatively low simulated AVDIs in
our study. Only the estimated slope parameter (α ) of the fitted logistic model (Equation 2) was 1
slightly altered, and the lower 95% CIs of daily intakes corresponding to various additional risks
in Table 4 were essentially unaffected (slightly higher values were obtained). This finding can be explained by the fact that the fitted logistic model was rather flat at the lower end of the daily
intake range, though it may have differed in the slope parameter estimate (Figure 3). Therefore, the safety assessment conclusions remain approximately the same. Because the prior mean
AVDIs for individuals in the low exposure group were obtained with relatively precise
information, the possible underestimation problem of the AVDIs did not exist for individuals in this group.
The sensitivity analyses of the alternative LOD/LOQs showed that the lower 95% CIs of
daily intakes corresponding to different additional risks increased with the adopted melamine content level for the control group. However, there was little difference between the simulated
outcomes, except that those with an assumed content level of 0.25 mg/kg were one order higher.
Because most LC-MS/MS techniques have a LOD/LOQ lower than 0.05 mg/kg, we only reported the results based on the mean melamine content of 0.025.
Deleted: Details of the simulation
outcomes are given in the supplementary material. Deleted: 2 Deleted: 2 Deleted: 2 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49
For Peer Review Only
Regarding sensitivity to model uncertainty, the alternative probit model curve obtained from
MCMC simulations was essentially parallel to the logistic curve at low AVDI range (Figure 3),
and the whole curve fell within the 95% CI of the logistic curve. Thus, results of the two model fittings are similar as suggested by Agresti (1996), though the probit model fitting with further
departure from the observations was somewhat inferior (Figure 3). Notice that the probit model fitting suggested a smaller point of departure than that of the logistic model fitting. To compare for the differences, Table 4 lists the lower 95% CI bounds of the additional risks obtained from the probit and logistic model fittings together. Other than this, because of the wide 95% CI band of the logistic curve, additional statistical model fittings may also lie within this band (Figure 3).
Consequently, TDI calculations may be insensitive to different model fittings, much like the
probit model fitting. Finally, the dosages corresponding to various additional risks after case No. 3 and No. 12 were removed from the analysis were slightly higher than those obtained with the
inclusion of these subjects. However, the differences were negligible (not shown here).
Discussion
Epidemiological versus toxicological data in melamine risk assessment
To our knowledge, this is the first safety assessment of melamine in infant formula based on
clinical kidney stone screenings of young children. Although expert panels have stated that human data should be central to or given preference over animal data in risk assessment (Samet
et al. 1998; Swaen 2006), the current TDI level suggested by the WHO (2009a) is based on toxicological data from animal studies. It has been reported that dose-response information
cannot be generated due to the following factors: wide variation in the concentrations of
melamine in infant formula both between and within brands, unknown amounts of consumption,
Deleted: B 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49
For Peer Review Only
and various durations of exposure to different brands. Therefore, the available human data are
insufficient for the characterization of the human health risks related to melamine in food (WHO
2009a). We adopted a probabilistic approach to deal with this issue. The probabilistic modeling for melamine risk assessment was accomplished with two stages: (1) individual AVDIs were
reconstructed using Monte Carlo simulations to account for uncertainties and variations in melamine intakes; (2) given prior individual AVDI distributions, a great deal of uncertainty was
then further reduced via statistical modeling using MCMC simulations.
Several issues of concern may be present in our study subjects. Animal studies show that melamine is rapidly excreted from body with a half-life of around three hours (OECD 1998).
Although 12 cases were diagnosed with melamine-related nephrolithiasis, four of them had been
back in Taiwan for more than six months. Therefore, there may be some cumulative lag effects of melamine in human body. Also, because the youngest case (No. 5, 1.3 years old) consumed
melamine-tainted milk powder for only 20 days, there may be an age-related susceptibility in melamine-related nephrolithiasis (Guan et al. 2009). Because children with a history of preterm
birth, congenital abnormalities of the genitourinary tract, or chronic diseases were excluded from
the study, our results should not be confounded by other risk factors. We did not assume a threshold level or a no-observed-adverse-effect level (NOAEL), nor did we apply some of the
uncertainty factors commonly adopted in non-carcinogen toxicological data. Rather, similar to
the benchmark dose approach in assessing methyl mercury exposures with data from children (Crump et al. 2000; Wijngaarden et al. 2006), the lower 5% of the simulated additional risks were
listed for suggestion of TDI to safeguard the majority from melamine exposure.
Inherent uncertainties might remain in the current WHO suggested TDI level of 0.2 mg/kg
bw/d (based on animal studies). These include extrapolation from high to low dose, across
species, and from adults to infants due to immature kidney function. Taking into account
Deleted: both our findings and
2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49
For Peer Review Only
potential synergistic effects between melamine and cyanuric acid, similar problems also exist for
the US FDA suggested TDI level of 0.63 mg/kg bw/d from May of 2007 (US FDA 2008a) and
the revised level of 0.063 mg/kg bw/d from October of 2008 (US FDA 2008b). Because only 10 rats were used for each dosing group, it is possible that the NOAEL would have been lower if a
larger sample size had been used (Crump 1984). Eight cases of renal stones or deposits with estimated melamine AVDIs ranging from 0.01 to 0.21 mg/kg bw/d, obtained in a cross-sectional
study in Hong Kong (Lam et al. 2008), also question the assumption that a TDI level of 0.2 or
even 0.063 mg/kg bw/d is low enough to protect young children.
Comparison with other studies
A prerequisite for the determination of the dose-response relationship using epidemiology data is to have several exposure groups with differentiable exposure concentrations and durations. The
dataset of the study provides a unique composition of high, low and control groups with distinguishable exposure histories of the screened children. As shown in the results, the low
AVDI exposure group played a key role in determining the tolerable daily intakes corresponding
to various additional risks. Although a similar grouping was adopted in the Peking Hospital screening data (Guan et al. 2009), the moderate exposure group with melamine content less than
150 mg/ kg is still relatively high compared to the value used in the current study. Similarly, the
melamine concentrations were very high (150 to 4700 mg/kg) in the tabulated age and duration of Sanlu milk consumption and in the incidence of kidney stones (Tables 7 and 8) in a
cross-sectional study in Gansu, China (WHO 2009a). On the other hand, children in the Hong Kong study were essentially exposed to low doses of melamine (Lam et al. 2008). Therefore, the
other datasets might be insufficient to establish a dose-response relationship for risk assessment.
2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49
For Peer Review Only
The response rate of the reference AVDI group of the current study was 0.0027 (≅1/377),
which is similar to the rate of 0.0025 ( ≅ 8/3170, including the seven suspected renal deposits)
used in the Hong Kong screening data (Lam et al. 2008). However, the Hong Kong study’s estimated AVDI of 0.01 to 0.21 mg/kg bw/d fell within the range of our medium AVDI group,
which had a much higher response rate of 0.105 (≅2/19). Several factors may have contributed to this difference. First, the children recruited for the current study were much younger (five
rather than 12) and may therefore have been more susceptible to melamine exposure. Second,
little information regarding individual AVDIs is provided in the Hong Kong study. Consequently, it is possible that the cases were exposed to higher melamine relative to other children in the
same study.
Mode of action of nephrolithiasis in children and tolerable daily intake of melamine
The mechanism of kidney failure in animals developing melamine-cyanurate crystals is thought to be similar to acute uric acid nephropathy in humans, which is “a mechanical obstruction that results in renal damage due to the uric acid crystal spherulites” (WHO 2009b). Increased purine catabolism can also result in the deposition of uric acid crystals within the kidney, and the precipitation is thought to occur due to the increased uric acid concentration in the filtered plasma and the increased acidity in the tabular lumen (Conger 1990; WHO 2009b). Experiment in rodents administered with chemicals including melamine that produces urinary tract calculi also show that it is a high-dose (threshold) phenomenon, which appears to occur more readily in rodents than in primates including humans (Cohen et al. 2002).
The renal stones formed in infants ingesting melamine-tainted formula were composed primarily of uric acid and melamine with a ratio of 2 to 1. Infants and children also have higher normal uric acid concentrations and urinary uric acid clearance than adults, which make them
Formatted: Font: Bold, Italic
Formatted: Font: Bold, Italic
2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49
For Peer Review Only
more susceptible to developing hyperuricosuria and more likely to develop urinary uric acid precipitates (WHO 2009b). The kidney stone cases in children drinking adulterated formula with diluted protein content and the fact that infant basal serum uric acid levels and urine filtered levels are higher than those of adults all increased the likelihood of uric acid stone formation (WHO 2009b). These factors of infant physiology suggest that the calculi formation is acting by a mode of action (MOA) related to acute or subchronic cumulative exposure to melamine that results in uric acid precipitation.
Because the nephrolithiasis cases in children of the study aged from 1.3 to 4.8 years old, depending on individual susceptibility and physiological maturity, the threshold of cumulative melamine exposure to form renal stone may vary across individuals. Thus, it is quite possible that there is a low-dose linear population response due to the heterogeneous individual thresholds and background additivity, which corresponds to the conceptual dose-response model 1 proposed by the National Research Council (NRC 2009, Chapter 5). The fitted logistic and probit models without incorporation of a threshold term are applicable in such case.
Finally, because the background risk of 1/377≅0.0027of the reference group (Figure 1) and the corresponding estimated SD of 0.0023 was of the order of 0.1%, additional risk lower than this order would be difficult to be distinguished from the spontaneous rate of nephrolithiasis. Furthermore, the estimated relative risk of 1.02 of the low exposure group to the reference group was non-significant. Together with the consideration of MOA of nephrolithiasis in children, the lower 95% CI bound corresponding to an additional risk of 0.1% should be sufficient to define the TDI of melamine exposure. Figure 3 also suggested that the selection of 0.008 and 0.03 was a reasonable POD of the fitted probit and logistic model curves, respectively. Notice that the range 0.008 to 0.03 mg/kg bw/d is approximately an order lower than the WHO suggested TDI level of
Formatted: Indent: First line: 1 ch 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49
For Peer Review Only
0.2 mg/kg bw/d, but is higher than the estimated AVDI (0.006 mg/kg bw/d) of the low exposure group.
Strengths of the two-stage probabilistic approach adopted for risk assessment
Uncertainty in historical exposure is the main theme in epidemiological studies. The first stage Monte Carlo simulations for the probabilistic individual AVDIs has the advantages of weighing uncertainties in different factors with variability in the resulting empirical distributions, which has recently become more popular in exposure assessment of pesticide residues and mycotoxins in food consumption (Claeys et al. 2008; Jensen et al. 2008; Kuiper-Goodman et al. 2010).
To establish the dose-response relationship, the MCMC simulations used in the second stage went a step further, thereby greatly diminishing some of the uncertainty typically encountered in exposure assessment. This was a major advantage of the approach adopted in the present study. For example, the posterior 95% CI (0.933, 2.377) (mean 1.541 and SD 0.373) of the mean melamine daily intake, µ
[ ]
4 , of the high AVDI group was relatively narrow compared to that of the prior 95% CI (0.170, 10.280) (mean 1.576 and SD 3.032) from the first stage. Whereas the posterior mean (1.541) remained approximately the same as the prior mean (1.576), the posterior SD (0.373) was much smaller than the prior SD (3.032). The results for other AVDI groups were similar. This is due to the adjustment of posterior AVDI group means, µ[ ]
i , to best fit the chosen dose-response model. In addition, the mathematical property of MCMC simulations ensures the Markov chain process approaching the posterior stationary distributions upon convergence (Roberts 1996). Thus, the assessed AVDI levels corresponding to various additional risks were estimated with much more precision than would have been possible using simple MC simulations in the first stage.Deleted: 2 Deleted: 08 Deleted: 5 Deleted: T Deleted: 508 Deleted: 57 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49
For Peer Review Only
Another important strength of the proposed procedure is that the individual AVDIs within each group were considered randomly distributed rather than given constants. Unlike animal bioassay studies with prescribed constant dosage for study animals in each dose group, the melamine intake of the children classified into the same AVDI group were essentially different but still shared a similar exposure background and, thus, the same group (or subpopulation) mean AVDI. The hierarchical Bayesian statistical framework regarding individual AVDIs asrealizations of a random group mean AVDI, µ
[ ]
i , thus becomes a natural approach for such a data structure. This approach might have great implications for health risk assessment with epidemiological or environmental epidemiological data of grouped exposure categories due to uncertainties in exposure. The appropriate choice of representative exposure scores for the resulting categorical regression would become problematic (Il’yasova et al. 2005; Loomis et al. 2005), and, most often, odds ratios or standardized mortality ratios with confidence intervals for epidemiological studies can only be given without an overall dose-response model (Guan et al. 2009; Lubin et al. 2008). As a result, risk characterization for the corresponding health risk assessment may be difficult to obtain using a categorical regression model.Limitations of the study
The assessment of individual AVDIs of the tainted milk undoubtedly suffered from great uncertainties in the estimation of melamine contents in the milk powder. In addition, there were uncertainties related to exposure duration (ED), given that we were unsure of when the
contamination began. Furthermore, the melamine contents may not have been the same before and after the outbreak scandal. However, because the uncertainties in melamine contents were taken into account by the large SDs in the probabilistic approach using a lognormal distribution,
2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49
For Peer Review Only
these factors should not have posed serious problems in determining AVDIs. Also, although the exact melamine adulteration period is unknown, some of our nephrolithiasis cases in the high AVDI group had only resided in China for a period of a few months. These were subjects for whom we had precise ED information, which provided conservation in estimating the subgroup mean AVDIs.Other limitations include dose-response model uncertainty, misclassification bias of the study participants and recall bias of parents who completed the questionnaire. The study dataset shared a common limitation with most epidemiological data in its ability to discriminate among
alternative models for risk assessment (Samet et al. 1998). However, sensitivity analysis using a probit model did not yield substantially different results. Because of the distinct definition in categorizing the exposure history of the children, the problem of misclassification should be minimal. Though recall bias is unavoidable, many uncertainties were accounted for using probabilistic exposure assessment.
Finally, the results are applicable only to children under the age of five who were given infant formula as a primary source of nutrition. No inference could be made regarding the safety level of melamine in other foods for older children or adults. In addition, the calculated melamine AVDIs for various additional risks were suitable for melamine intake only. We therefore concluded that concomitant exposure to melamine and cyanuric acid may be more toxic than exposure to a single chemical compound. However, it appears that melamine was typically the sole contaminant in milk powder during the outbreak, with the possible coexistence of very low concentrations of cyanuric acid (compared to the 2007 pet food contamination incident in the USA; WHO 2009a). Because of lack of related data, risk assessment concerning the coexistence of cyanuric acid in the melamine-tainted milk powder remains uncertain.
2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49
For Peer Review Only
Conclusion
In conclusion, we have successfully established the dose-response relationship using a hierarchical Bayesian probabilistic approach based on screening data of melamine exposure in infant formula. This analysis may provide more direct evidence for risk assessment than toxicological-based data. The simulated lower 95% CIs of the AVDIs corresponding to various additional risks showed that the current TDI of 0.2 mg/kg bw/d (recommended by the WHO), with an additional risk of 0.01 or higher (Table 4), may not safeguard young children who are potentially more vulnerable than adults. More stringent regulation to lower the melamine TDI of infant formula to a level of 0.008 to 0.03 mg/kg bw/d is recommended.
Acknowledgements
The authors would like to thank Professors Trong-Neng Wu, Chow-Feng Chiang, and
Hung-Lung Chiang for providing suggestions for this paper; Dr. Chih-Jung Chen for collecting the data; and Ms. Chia-Yen Yu for statistical programming and plots. This work was supported by the National Science Council of Taiwan (NSC 97-2314-B-192-001-MY2). The authors declare that they have no conflicts of interest.
Deleted: 2
Deleted: Because the ADI levels
listed in Table 2 are essentially only slightly higher than the estimated baseline dietary exposure of 0.54–1.6µg/kg bw/d in infant formula (WHO 2009), m Deleted: s Deleted: on Deleted: Deleted: level Deleted: are 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49
For Peer Review Only
Appendix
The hierarchical Bayesian structure of the logistic model fitting using MCMC simulations Let lnµ
[ ]
i be the logarithm of the i-th AVDI group mean µ[ ]
i . Given the reconstructed AVDI log-transformed mean x[ ]
i,j ofthe individual j of the i-th AVDI group, it is regarded as an observation from the i-th AVDI group, which is normally distributed with group mean lnµ[ ]
i and variance 1/τ[ ]
i , i.e.,[ ]
i j N(
[ ]
i[ ]
i)
x , ~ lnµ ,1/τ .
The log-transformed group mean lnµ
[ ]
i is assumed to have a normal distribution with sub-parameters mean M[i] and variance 1/W[i], i.e.,[ ]
i ~N(M[ ]
i,1/W[ ]
i)lnµ .
Similarly, the log-transformed variance y
[ ]
i,j is assumed to have a gamma distribution with parameters θ[ ]
i and β[ ]
i , i.e.,[ ]
i j Gamma([ ] [ ]
i i)y , ~ θ ,β ,
and θ
[ ]
i and β[ ]
i are assumed to have uniform distribution with subparameters sa[ ] [ ]
i,sbiand ba
[ ] [ ]
i,bbi respectively, i.e.,[ ]
i ~Uniform(
sa[ ] [ ]
i,sbi)
θ ,[ ]
i ~Uniform(
ba[ ] [ ]
i,bbi)
β ,[ ]
i(
θ[ ]
i β[ ]
i)
τ = /1 × .Finally, the number of cases T
[ ]
i of the i-th AVDI group of total number of subjects n[ ]
i is binomially distributed with mean p[ ]
i , i.e.,Formatted: Font: Italic
Formatted: Font: Italic
Formatted: Font: Italic
Formatted: Font: Italic
2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49
For Peer Review Only
[ ]
i Bin(
n[ ] [ ]
i pi)
T ~ , . 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49For Peer Review Only
References
Agresti A. 1996. An introduction to categorical data analysis. New York: Wiley. pp. 79–80. Bureau of Health, Taipei City Government. 2008 . Results of investigation in dietary products with Melamine (in Chinese), October 8. Available from:
http://www.health.gov.tw/Default.aspx?tabid=36&mid=442&itemid=21734.
Chan M, Lo CK, Cheng LS, Cheung TC, Wong YC. 2009. Evaluation of testing capabilities for the determination of melamine in milk through an interlaboratory proficiency test programme during the melamine crisis. Food Addit Contam. 26(11): 1450–1458.
Claeys WL, De Voghel S, Schmit JF, Vromman V, Pussemier L. 2008. Exposure assessment of the Belgian population to pesticide residues through fruit and vegetable consumption. Food Addit Contam. 25(7): 851–863.
Cohen SM, Johansson SL, Arnold LL, Lawson TA. 2002. Urinary tract calculi and thresholds in carcinogenesis. Food Chem Toxicol. 40: 793–799.
Conger JD. 1990. Acute uric acid nephropathy. Med Clin North Am. 74(4): 859–871.
Crump KS. 1984. A new method for determining allowable daily intakes. Fundam Appl Toxicol. 4:857–871.
Crump KS, Van Landingham C, Shamlaye C, Cox C, Davidson PW, Myers GJ, Clarkson TW. 2000. Benchmark concentrations for methylmercury obtained from the Seychelles child development study. Environ Health Perspect. 108(3): 257–263.
Guan N, Fan Q, Ding J, Zhao Y, Lu J, Ai Y, Xu G, Zhu S, Yao C, Jiang L, Miao J, Zhang H, Zhao D, Liu X, Yao Y. 2009. Melamine-contaminated powdered formula and urolithiasis in young children. N Engl J Med. 360:1067–1074.
Il’yasova D, Hertz-Picciotto I, Peters U, Berlin JA, Poole C. 2005. Choice of exposure scores for
Formatted: Font color: Auto
Formatted: Font: (Default) Times New Roman, 12 pt
Formatted: Font: (Default)
Times New Roman, 12 pt
Formatted: Font: (Default)
Times New Roman, 12 pt
Formatted: Font: (Default) Times New Roman, 12 pt
Formatted: Font: (Default)
Times New Roman, 12 pt
2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49
For Peer Review Only
categorical regression in meta-analysis: a case study of a common problem. Cancer CausesControl. 16: 383–388.
Ingelfinger JR. 2008. Melamine and the global implications of food contamination. N Engl J Med. 359:2745–2748.
International Agency for Research on Cancer (IARC). 1999. Some chemicals that cause tumors of the kidney or urinary bladder in rodents and some other substances. Available from: http://monographs.iarc.fr/ENG/Monographs/vol73/volume73.pdf.
International Food Safety Authorities Network (IFSAN). 2008. List of milk products that are confirmed to be positive for melamine, October 2. Available from:
http://www.moh.gov.bn/download/list-of-confirmed-contaminated-products.pdf.
Jensen, BH, Andersen JH, Petersen A, Christensen T. 2008. Dietary exposure assessment of Danish consumers to dithiocarbamate residues in food: a comparison of the deterministic and probabilistic approach. Food Addit Contam. 25(6): 714–721.
Kuiper-Goodman T, Hilts C, Billiard SM, Kiparissis Y, Richard IDK, Hayward S. Health risk assessment of ochratoxin A for all age-sex strata in a market economy. Food Addit Contam. 27(2): 212–240.
Lam HS, Ng PC, Chu WC, Wong W, Chan DF, Ho SS, Wong KT, Ahuja AT, Li CK. 2008. Renal screening in children after exposure to low dose melamine in Hong Kong:
cross-sectional study. Br Med J. 337:a2991.
Loomis D, Richardson DB, Elliott L. 2005. Poisson regression analysis of ungrouped data. Occup Environ Med. 62: 325–329.
Lubin JH, Moore LE, Fraumeni Jr JF, Cantor KP. Respiratory cancer and inhaled inorganic arsenic in copper smelters workers: a linear relationship with cumulative exposure that increases with concentration. Environ Health Perspect. 116(12): 1661–1665.
2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49
For Peer Review Only
MRC Biostatistics Unit. WinBUGS 1.4.3, 2008. Available from:http://www.mrc-bsu.cam.ac.uk/bugs.
National Research Council. 2009. Science and Decisions: Advancing Risk Assessment. Washington DC, US: The National Academies Press.
Organization for Economic Co-operation and Development (OECD). 1998. Screening information data set for melamine, CAS No. #108-78-1. Available from:
http://www.chem.unep.ch/irptc/sids/OECDSIDS/108781.pdf.
Reimschuessel R, Gieseker C, Miller RA, Rummel N, Ward J, Boehmer J, Heller D, Nochetto C, De Alwis H, Bataller N, Andersen W, Turnipseed SB, Karbiwnyk CM, Satzger RD, Crown J, Reinhard MK, Roberts JF, Witkowski M. 2008. Evaluation of the renal effects of experimental feeding of melamine and cyanuric acid to fish and pigs. Am J Vet Res. 69(9):1217–1228. Roberts GO. 1996. Markov chain Monte Carlo in practice. Gilks WR, Richardson S,
Spiegelhalter DJ eds. Boca Raton, FL: CRC Press. Chapter 3, Markov chain concepts related to sampling algorithms; pp 45–57.
Samet JM, Schnatter R, Gibb H. 1998. Epidemiology and risk assessment. Am J Epidemiol. 25: 147–155.
Swaen GM. 2006. A framework for using epidemiological data for risk assessment. Hum Exp Toxicol. 25: 147–155.
Tittlemier SA. 2010. Methods for the analysis of melamine and related compounds in foods: a review. Food Addit Contam. 27(2): 129–145.
US Food and Drug Administration/ Center for Food Safety and Applied Nutrition (US FDA/CFSAN). 2008a. Interim safety and risk assessment of melamine and its analogues in food for humans, October 3. Available from: http://www.cfsan.fda.gov/~dms/melamra.html. US Food and Drug Administration/Center for Food Safety and Applied Nutrition (US
Formatted: Font color: Auto Formatted: Indent: Left 0 ch,
First line: 0 ch 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49
For Peer Review Only
FDA/FSAN). 2008b. Update—interim safety and risk assessment of melamine and its analogues in food for humans, Noverber 28. Available from:http://www.cfsan.fda.gov/~dms/melamra.html.
Van Wijngaarden E, Beck C, Shamlaye CF, Cernichiari E, Davidson PW, Myers GJ, Clarkson TW. 2006. Benchmark concentrations for methyl mercury obtained from the 9-year follow-up of the Seychelles child development study. Neurotoxicology. 27: 702–709.
Wang IJ, Chen PC, Hwang KC. 2009. Melamine and nephrolithiasis in children in Taiwan. N Engl J Med. 360:1157–1158.
World Health Organization. 2009a. Toxicological and health aspects of melamine and cyanuric acid: report of a WHO expert meeting in collaboration with FAO supported by Health Canada, April 16. Available from:
http://www.who.int/foodsafety/fs_management/infosan_events/en.
World Health Organization. 2009b. Background paper on toxicology of melamine and its analogues: report of a WHO expert meeting in collaboration with FAO supported by Health Canada. Available from: http://www.who.int/foodsafety/fs_management/Melamine_5.pdf
Formatted: Font color: Auto
Formatted: Font: Not Bold Formatted: Left: 70.9 pt, Right:
70.9 pt, Top: 70.9 pt, Bottom: 70.9 pt, Width: 612 pt, Height: 792 pt, Header distance from edge: 36 pt, Footer distance from edge: 36 pt
Deleted: Section Break (Next Page)
2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49
For Peer Review Only
AbstractAlthough the 2008 outbreak of nephrolithiasis in children due to melamine-contaminated infant formula has subsided, it remains uncertainwhether the present tolerable daily intake (TDI) of melamine provides sufficient protection for young children. To conduct a safety assessment for melamine in infant formula, we established a dose-response relationship based on 13
nephrolithiasis cases selected from 932 children, all of whom were under five years of age and had potentially been exposed to tainted milk in China or Taiwan. According to the children’s exposure history, distributions of individual daily melamine intake (mg/kg bw/d) were
reconstructed using Monte Carlo simulations to account for uncertainties in exposure duration and melamine concentrations in the tainted milk. Based on the simulated individual average daily intake (AVDI) of melamine, subjects were further classified into four separate AVDI groups: high, medium, low and a reference group. A statistical logistic model was then fitted for the
dose-response relationship between nephrolithiasis incidence and daily melamine intakes using Markov chain Monte Carlo (MCMC) simulations. Based on the background exposure,
spontaneous rate, and mode of action (MOA) of nephrolithiasis in children, the simulated lower bounds of the 95% CIs daily melamine intake ranged from 0.008 to 0.03 mg/kg bw/d
corresponding to an additional risks of 0.1% is proposed as a plausible TDI, which is
approximately an order lower than the current WHO-suggested TDI level of 0.2 mg/kg bw/d. More stringent regulations on melamine levels in infant formula should be considered to protect 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49
For Peer Review Only
IntroductionMelamine, also known as cyanuramide, is a manmade substance commonly used in manufactured products, including dishes, housewares, plastic resins, dry erase boards and industrial coatings (Ingelfinger 2008). Although melamine is of low acute toxicity, long-term excessive exposure in animals causes bladder stones, damage to the urinary system, and may induce bladder cancer (IARC 1999).Young children are extremely vulnerable to melamine-related toxicity because of the immaturity of their organs and the fact that infant formula may constitute their sole source of nutrition (US FDA/CFSAN 2008a). In addition, infants who consume adulterated formula with high levels of melamine may receive inadequate protein in their diet. Because the basal serum uric acid levels and urine-filtered levels of infants are higher than those of adults, they are therefore are more likely to form uric acid stones (WHO 2009a). The recent tainted milk scandal in China that caused more than 50,000 cases of renal disease and the deaths of several children has raised serious public health concerns worldwide, especially after traces of melamine were detected in top-selling U.S. infant formulas (Ingelfinger 2008; US FDA/CFSAN 2008b). Similar concerns were also raised in Taiwan after it was discovered that dairy products imported from China were tainted with melamine.
In 2007, the US Food and Drug Administration (FDA) published a tolerable daily intake (TDI) for melamine of 0.63 mg/kg bw/d. This information was released following numerous reports of kidney failure and death in pets due to consumption of pet foods contaminated with 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49
For Peer Review Only
mg/kg bw/d in October of 2008 by applying an additional tenfold safety factor for uncertainty (US FDA/CFSAN 2008a). To set a TDI of melamine to protect consumers from adverse health effects, the World Health Organization (WHOa) held an expert meeting in December of 2008; they suggested a TDI level of 0.2 mg/kg bw/d that would be applicable to the whole population, including infants (WHO 2009). Much like the recommendation of the FDA, however, the
dose-response assessment was based on a sub-chronic animal study. Because the renal systems of young children are too immature to ward off the impact of the chemical, and because infants depend mainly on formula as their source of nutrition (US FDA/CFSAN 2008a, 2008b), the recommended TDI level of 0.2 mg/kg bw/d said to be applicable for the entire population may need to be reassessed. In addition, unlike the pet food contamination incident with comparable levels of melamine and cyanuric acid, the levels of its analogues (cyanuric acid, ammeline, and ammelide) contained in the adulterated infant formula were found to be only about 0.1% of the melamine levels (WHO 2009a). Furthermore, exposure in infants is chronic, occurs over several months, and is not mitigated by previous passage through the digestive system of an animal (US FDA/CFSAN 2008a). Therefore, the exposure scenario of the diseased young children was quite different from that of the pet food contamination episode and other animal studies. The
establishment of a safe level of melamine content in infant formula is of great importance, especially for infants and young children who are more susceptible to melamine exposure.
In this paper, incidents of melamine-related and unrelated nephrolithiasis diagnosed among 932 young children under five years of age were modeled based on their history of melamine 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49
For Peer Review Only
estimated AVDIs, and a statistical model was fitted for the dose-response relationship using Markov chain Monte Carlo (MCMC) simulations. Using the mathematical convergence property of MCMC simulations with the fitted dose-response model, the posterior distributions of the group mean AVDIs were narrowed down from the prior distributions. Thus, uncertainties in determining the subgroup means of AVDI melamine intake were reduced to reliably assess the various additional risks of nephrolithiasis.
Materials and methods
Study population
A total of 1222 children who may have consumed melamine-tainted dairy products were screened at three Department of Health hospitals in Taiwan for possible kidney problems. All of the
participants were between 0 and 16 years of age, and screenings took place from September 24 to October 31, 2008. The majorities of the diseased young children were less than three years of age and were mainly dependent on the tainted infant formula as their major nutrition source (US FDA/CFSAN 2008a). Taking into account age susceptibility to melamine exposure, 932 children under five years of age were analyzed for the present study, which was approved by the hospital ethics committee. Children born prematurely and those with congenital abnormalities of the genitourinary tract or chronic diseases were excluded from participation. Figure 1 illustrates the procedure for screening and classifying the subjects.
2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49
For Peer Review Only
Parents were interviewed with questionnaires administered by pediatricians. Background information, including age, sex, body weight (BW), residential history in China, past history of urinary tract infection (UTI) or vesico-urethra reflux, family history of nephrolithiasis, and clinical symptoms (e.g., flank pain, dysuria, urinary frequency, decreased urine output,
unexplained fever, etc.) were collected. Possible consumption of melamine-tainted dairy products, including infant formula, milk drinks, yogurt, ice cream, chocolate biscuits, and powdered cheese, were also itemized in the questionnaires, along with average quantities of products consumed per day, frequency of feeding, and consumption periods of the products on the list (e.g., milk powder brands Sanlu, Mengniu, Yili and Yashili produced in China or other brands imported from China) (IFSAN 2008; Taipei Bureau of Health 2008). Parents were asked to estimate the amount of milk consumption using the volume of the feeding bottle or the sample spoon included with the infant formula.
According to the subjects’ exposure history, eight contaminated dairy products on the questionnaire list were identified, with melamine concentrations ranging from 0.1 to 2563 mg kg-1 (IFSAN 2008). More recent analyses showed that individual samples ranged up to 4700 mg/kg (WHO 2009a). Based on the brand(s) of milk powder they consumed, subjects were classified into the high exposure group, who consumed highly contaminated dairy products in China with melamine levels > 2.5 mg/kg; the low exposure group, who consumed other brands of less-tainted milk powder ranged from 0.123 to 2.02 mg/kg (Taipei Bureau of Health 2008)
imported from China; and the control group, who consumed milk powder with no detectable 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49
For Peer Review Only
nephrolithiasis were defined as nephrolithiasis in children who were fed with melamine-tainted infant formula. Details of the clinical diagnosis are described in Wang et al. (2009).
Probabilistic modeling of individual average daily intake of melamine
Because of great uncertainties involved in determining individual exposure duration as well as melamine content(s) in the infant formula(s), it was more appropriate to adopt a probabilistic approach for estimating the corresponding AVDI. Probabilistic exposure assessment has recently become popular for assessing pesticide residues or mycotoxins in food consumptions (rather than deterministic approach); this approach has the advantages of taking into account the probabilistic distribution of the exposure and the ability to quantify variability and uncertainty (Claeys et al. 2008; Jensen et al. 2008; Kuiper-Goodman et al. 2010).
We performed Monte Carlo simulations to generate the empirical distribution of individual AVDI using the equation:
AT BW ED I C AVDI M M × × × = , (1)
where CM is the melamine content in milk powder, IM is the daily consumption rate of milk
powder, ED is the exposure duration of the tainted milk powder consumption, BW is the child’s current body weight, and AT is the average time that the child was diagnosed with a kidney stone. To avoid possible recall bias, the individual exposure duration and the amount of melamine intake were estimated based on the questionnaire. A lognormal distribution was then fitted 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49