行政院國家科學委員會專題研究計畫 成果報告
早期潛在性激痛點的發生研究
計畫類別: 個別型計畫 計畫編號: NSC93-2314-B-241-002- 執行期間: 93 年 08 月 01 日至 94 年 07 月 31 日 執行單位: 弘光科技大學物理治療系 計畫主持人: 洪章仁 共同主持人: 謝悅齡,高木榮 計畫參與人員: 謝悅齡 ,高木榮 報告類型: 精簡報告 處理方式: 本計畫可公開查詢中 華 民 國 94 年 11 月 1 日
行政院國家科學委員會補助專題研究計畫
; 成 果 報 告 □期中進度報告早期潛在性激痛點的發生研究
計畫類別:; 個別型計畫 □ 整合型計畫
計畫編號:
NSC 93-2314-B-241-002
執行期間: 93 年 8 月 1 日至 94 年 7 月 31 日
計畫主持人:洪章仁
共同主持人:謝悅齡
計畫參與人員: 高木榮
成果報告類型(依經費核定清單規定繳交):5精簡報告 □完整報告
本成果報告包括以下應繳交之附件:
□赴國外出差或研習心得報告一份
□赴大陸地區出差或研習心得報告一份
□出席國際學術會議心得報告及發表之論文各一份
□國際合作研究計畫國外研究報告書一份
處理方式:除產學合作研究計畫、提升產業技術及人才培育研究計畫、
列管計畫及下列情形者外,得立即公開查詢
□涉及專利或其他智慧財產權,□一年□二年後可公開查詢
執行單位: 弘光科技大學 物理治療系
中 華 民 國
94 年 10 月 30 日
ABSTRACT
This study is designed to assess the occurrence of latent myofascial trigger points (MTrPs) in the early life as compared to the adult subjects. Sixty normal adults and 60 infants (age 0- 12 months) were investigated. An algometer was used to measure the pressure pain threshold (PTT) on 3 different sites, including a mid-point (assumed to be the MTrP site), in the brachioradialis muscle. It was fond that the mean PPT values at the MTrP site was significantly lower than the other sites in the adult muscles. However, no significant differences in PPT values among these 3 sites were found in the infants. It was concluded that, in the adult subjects, the mid-point of brachiaoradialis muscle was not significantly more irritable than other sites and the mid-point was probably a latent MTrP. However, in the infants with age less than one year-old, such phenomenon could not observed in this study. It is very likely that the latent MTrPs might not exist in the early life, but develop in the later life.
INTRODUCTION
According to the classical definition, a myofascial trigger point (MTrP) is a hypersensitive spot in a taut band of skeletal muscle fibers [Simons et al 1999]. Latent MTrPs are tender but not painful. Active MTrPs are painful either spontaneously or in response to movement. Normal adults usually have latent MTrPs in the clinically “normal” (non-painful) muscles. The latent MTrPs may become active ones in response to a stimulation reflexively from a lesion in the other site or in the muscle itself as a consequence of central sensitization [Hong 1999, 2000; Hong & Simons 1998; Simons et al 1999].
The pathophysiology of the MTrP has now become better understood based on recent electrophysiological studies on both human and animal subjects [Hong 1994-b,-c, 1996, 1999; 2000, Hong & Torigoe 1994, Hong & Yu 1998; Hong et al 1995; Hong & Simons 1998; Hubbard & Berkoff 1993; Simons 1996, 1999; Simons & Dexter 1995; Simons et al 1996, 1999, 2002]. It has been demonstrated that there are multiple sensitive MTrP loci in an MTrP region [Hong 1994-b]. Histological study indicated that these sensitive loci are sensitized nociceptors [Hong et al 1996-a]. An MTrP is always
identified in the endplate zone (usually, the middle portion of the muscle fibers) [Simons et al, 1995, 2002]. Based on electrophysiological studies, a sensitive locus is always found in the vicinity of an endplate [Simons et al 1995, 2002]. The endplate near the sensitive locus of an MTrP is considered as a dysfunctional endplate with excessive acetylcholine leakage as demonstrated in the electrophysiological studies [Simons 1996; Simons et al 1995, 2002]. The endplate noise (EPN), instead of miniature endplate potentials, can be recorded frequently in an MTrP region, since MTrPs are always found in the endplate zone containing some dysfunctional endplates. The result of excessive secretion of acetylcholine, the contractue knot, has been well demonstrated in a histological study [Simons & stolov 1976; Simons et al 1999].
Base on the clinical observation and informal studies, Hong has claimed that newborn babies and infants may have no MTrPs, and, when they are growing up, latent MTrPs may develop gradually [Hong 1999, 2000, 2002]. However, there are no solid data to indicate such statement in the updated literature. This study is designed to investigate the occurrence of latent MTrP in early life. The hypothesis is that latent MTrPs can not be found in the early life, but may develop gradually when the newborns grow up.
General Design
The pressure pain threshold (PPT) was measured with a pressure algometer on 3 different sites (the mid point was assumed to be the site of latent MTrP) to see if the MTrP site was more irritable (with lower PPT) than the other sites.
Subjects
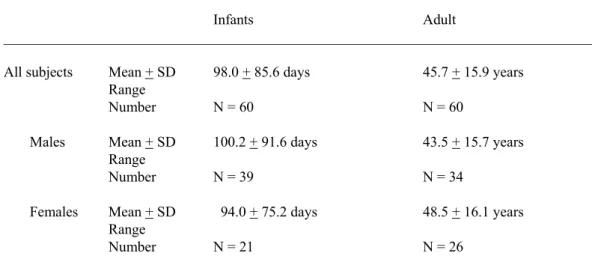
Sixty infants with age less than one year and 60 adults were recruited for this study. They or their legal guardians signed the informed consent forms ha were approved by the institutional review board of a university hospital. The mean age of the subjects and the age distribution of the infants were shown in Table 1 and Figure 1 respectively.
The exclusion criteria to select the subjects included any acute or serious illness, any recent trauma to the upper limb, any deformity in the upper limb, and any emotional instability.
Identification of the Brachioradialis Muscle
Brachioradialis muscle is a typical fusiform muscle with an endplate zone in the middle portion of the muscle. It attaches proximally to both the lateral supracondylar ridge of the humerus and to the lateral intermuscular septum, distal to where the radial nerve penetrates the septum at mid-arm level. Distally the brachioradialis tendon expands laterally as it approaches the styloid process of the radius and connects with the
neighboring ligaments. It is then anchored by a tendinous attachment to the styloid process. When the subject attempts to flex the elbow against resistance with elbow at 90 degrees of flexion, this muscle can be identified easily. When the infant’s hand is held tightly, the withdrawal reflex of the elbow can be induced and the brachiordialis muscle can be identified. [Simons et al 1999]
In this study, the brachioradialis muscle was identified by palpation based on the anatomical landmarks and maneuver as described above. The distance between the lateral epicondyle and the styloid process was measured. The mid-point of this distance was considered as the junction of muscle and tendon. The MTrP was approximately at the proximal one third between this junction site and the lateral epicondyle. [Simons e al 1999]. Three spots were measured for pressure pain threshold with a pressure algometer: “A” point was the site just above the lateral epicondyle (since the exact origin site of brachioradialis is difficult to identify), “B” point was the assumed MTrP site and “C” point was at the junction of muscle and tendon (Figure 2).
Equipment
A pressure algometer described by Fischer [1986] was used for the measurement of pressure pain threshold. This algometer has been considered as reliable and valid measure of MTrP sensitivity [Ohrback & Gale 1989-a & -b; Reeve et al 1986].
Measurement of the Pressure Pain Threshold
To measure the PPT, a pressure algometer was placed on the site to be measured, perpendicular to the surface of the skin. Then, the pressure of compression was increased gradually until the subject began to feel any pain or discomfort. In the measurement of the infant, the pressure of compression was increased gradually until the infant began to withdraw or cry or make a unpleasant facial expression, whichever comes first. At this
point, he examiner stopped the compression and read the scale in the algometer (Kg/cm2)
to find the PPT at that site. Three measurements were performed on each site, and totally 9 measurements were performed for each muscle. At lease one minute was lasted
between two consecutive measurements. The sequence of measurement on the 3 sites was randomly assigned. Two different well-trained examiners did the measurements on infants and adult subjects separately.
Palpation of taut Bands
After completion of the PTT measurements, the MTrP site was examined for the existence of taut band by the same examiners who did PPT measurements. They had also been well trained in the examination of MTrPs.
Data Analysis
The differences of PPT among the 3 sites were analyzed by ANOVA. The sex differences and the differences between two sides were analyzed with T test. A p value less than 0.05 was considered as statistically significant.
RESULTS
Differences among 3 measured sites
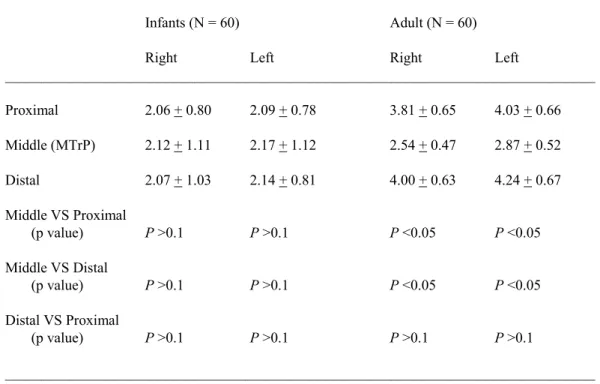
In the adult subjects, the mean PPT value was significantly lower (P < 0.01) in the MTrP site than other sites in either right or left side (Table 2). However, in the infants, there were no significant differences (P > 0.1) in the mean values of PPT among the 3 sites. In each infant, we were unable to see remarkable differences among the 3 measured spots as usually found in the adult subjects. For each adult subject, the MTrP site was always the most painful site with lowest PPT value as compared with other 2 sites. However, for each infant, the responses to the pressure stimuli at 3 different sites were the same.
Sex differences and differences between two sides
For each measured site, there was no significant difference (p>0.1) in PPT value between male and female subjects or between right and left side.
Existence of Taut Band
Upon palpation of the MTrP site, one ore more taut bands could be identified in all (100%) of adult subjects. On the other hand, no taut band could be identified in all infants.
DISCUSSION
Existence of Latent MTrP
In this study, we had found that every adult subject had a hyperirritable spot in the middle portion of taut band(s) in the barchioradialis muscle which could be a latent MTrP or at a vicinity of the latent MTrP. In an earlier study [Hong et al 1996-b], it was found that a site in the taut band but not the latent MTrP also had reduced PPT as compared to the normal muscle site. Therefore, the assumed MTrP site in our study might not be exactly the real MTrP site. At least we know that some spots may be more irritable than others in this muscle. However, we are unable to detect this phenomenon in the infants. No taut band could be identified in each infant. Therefore, we could not confirm the existence of latent MTrPs in the infant with age less than one year, since all 3 measured sites had the same irritability. This finding further support the hypothesis that latent MTrPs do not exist in the early life and probably develop later gradually, since we were
unable to distinguish a relatively hyperirritable spot in every infant in this study. As soon as a latent MTrP developed in the center of the muscle fibers (end-plate zone), it would be the most sensitive spot (most tender site) in muscle fibers. The findings in the adult subjects in this study have strongly supported that.
Formation of Latent MTrPs
The exact mechanism of MTrP formation is still uncertain. Gun has suggested that radiculopathy is the basic cause of MTrP formation [Gunn 1997]. Hong has agreed with this hypothesis for a latent MTrP formation, but not for the process of the activation of a latent MTrP to became an active one [Hong 2000-b]. At least we known that the latent MTrP is not inherent based on the findings in our study. The mechanism of MTrP formation is still unclear. Gunn [1997] considered that neuropathic lesion is the primary mechanism of MTrP formation. This is probably not true for the formation of active MTrPs [Hong 2000– letters to editor], since there were evidences that a latent MTrP can be activated to become an active MTrP via central sensitization [Hong 2000-a; Mense 1993, 1994, 1996]. However, it is very likely that the formation of a latent MTrP is due to minor radiculopathy from minor repetitive stress to the spine when the baby is growing up (Figure 3). The minor radiculopathy may cause excessive secretion of acetylcholine in the neuromuscular junction, and subsequently induced electrotonic potentials (endplate noise) in the neuromuscular junction to cause focal contracture of sarcomeres in the endplate zone (contracture knot).
Conclusion
In this study on the brachioradialis muscle, it was found that the assumed MTrP site was much irritable than other sites in the adult subjects, but not in the young infants (less than one year-old). Latent MTrPs probably do not exist in the newborn or young infant, but develop in the later life.
Table 1. Mean Ages of the Subjects
_________________________________________________________________________________ Infants Adult
_________________________________________________________________________________ All subjects Mean + SD 98.0 + 85.6 days 45.7 + 15.9 years
Range
Number N = 60 N = 60 Males Mean + SD 100.2 + 91.6 days 43.5 + 15.7 years Range
Number N = 39 N = 34 Females Mean + SD 94.0 + 75.2 days 48.5 + 16.1 years Range
Number N = 21 N = 26
Table 2. Mean Pressure Pain Threshold (Kg/cm2) at Different Sites
_________________________________________________________________________________ Infants (N = 60) Adult (N = 60)
Right Left Right Left
_________________________________________________________________________________ Proximal 2.06 + 0.80 2.09 + 0.78 3.81 + 0.65 4.03 + 0.66 Middle (MTrP) 2.12 + 1.11 2.17 + 1.12 2.54 + 0.47 2.87 + 0.52 Distal 2.07 + 1.03 2.14 + 0.81 4.00 + 0.63 4.24 + 0.67 Middle VS Proximal (p value) P >0.1 P >0.1 P <0.05 P <0.05 Middle VS Distal (p value) P >0.1 P >0.1 P <0.05 P <0.05 Distal VS Proximal (p value) P >0.1 P >0.1 P >0.1 P >0.1 _________________________________________________________________________________
Figure 1 Age Distribution of the Infants