Taipei Medical University Institutional Repository:Item 987654321/4244
90
0
0
全文
(2) Acknowledgements I must express my deep appreciation to Professor Hsieh Chang-Yao for his unreserved support and encouragement. Also I am indebted to Professors Hsu Tsuey-Ying, Lee Horng-Mo, and Tsai Yu-Hui, for being my committee members, and to Professors Shih Tzu-Bi, Leu Sy-Jye, Yeh Tien-Shun, Huang Huei-Mei and Lee Sheng-Yang for their encouragement with my Ph.D. program. I am particularly grateful to my advisor, Professor Chang Shwu-Fen, for her support over the years with the time consuming supervision and for her invaluable comments on this thesis. I am also grateful to my colleagues at the National Health Research Institute, the Taiwan Association of Gynecologic Oncologists, the Association of Chinese Gynecologic Oncologists, Cathay General Hospital, Fu-Jen Catholic University, and Taipei Medical University. Finally, I wish to thank my parents, Kung-Chung and Mu-Chi, my dear wife, Yu-Mei, my son, William, and my daughter, Phoebe, with heartfelt gratitude for their love and encouragement.. 2.
(3) Abbreviations used AGUS. atypical glandular cells of undetermined significance. ASCUS atypical squamous cells of undetermined significance CI. confidence interval. CIN. cervical intraepithelial neoplasias. CIS. carcinoma in situ. CT. computed tomography. FIGO. International Federation of Gynecology and Obstetrics. FISH. fluorescence in situ hybridization. HC2. hybrid capture 2. HPV. human papillomavirus. HR HPV high-risk types of human papillomavirus HSILS. high-grade squamous intraepithelial lesions. IRB. Institutional Review Board. ISH. in situ hybridization. LCR. long control region. LSILS. low-grade squamous intraepithelial lesions. LVSI. lymphovascular space involvement. OR. odds ratios. ORF. open reading frame. PCR. polymerase chain reaction. ROC. receiver operating characteristic (area under). SCC. squamous cell carcinoma. SCC-Ag squamous cell carcinoma-antigen TCOG. Taiwan Cooperative Oncology Group. 3.
(4) Contents. page. Abstract - Chinese ···································································································· 6-8 Abstract - English····································································································· 9-11 Chapter 1. General Introduction ···············································································12-23 Chapter 2. Materials and Methods············································································24-34 Chapter 3. Results and Discussion I. Detection and Quantitation of Human Papillomavirus Type 16, 18 and 52 DNA in the Peripheral Blood of Cervical Cancer Patients·············································35-40 I.A. HPV DNA type 16, 18, 52 tests using real-time PCR in cervical swab and blood I.B. Dynamic change of viral loads and median log of HPV DNA type 16, 18 and 52 in cervical swabs I.C. Viral loads of HPV 16, 18, 52 in blood in cervical cancer patients and its correlation to clinical outcomes I.D. Follow-up of HPV DNA positive in blood of cervical cancer patients I.E. Discussion ······························································· {Figures 1 (A), (B), (C) and Tables 1, 2} II. Integrated Human Papillomavirus Type 52 and 58 infrequently found in Cervical Cancer, and High Viral Loads predict risk of Cervical Cancer ·····························41-47 II.A. HPV DNA typing using genechip method II.B. Detection of physical status in HPV 16, 18, 52 and 58 DNA II.C. The median and median log of E2, E6 viral loads of HPV 16, 18, 52 and 58 DNA in CIN II-III and cervical cancer II.D. ROC curve predicts the assignment to CIN II-III or cervical cancer groups II.E. Discussion ················································································ {Table 1 and Figures 1-7} III. Human Papillomaviral Load Changes in Low-Grade Squamous Intraepithelial Lesions of the Uterine Cervix·············································································48-56. 4.
(5) III.A. Median E6 viral loads in low-grade squamous intraepithelial lesions III.B. Two-year cumulative risk with dynamic change of HPV III.C. Comparison of HPV viral load by HC2 and real-time PCR III.D. Physical status of HPV 16, 18, 52, and 58 DNA in women with LSIL and longitudinal follow-up III.E. Discussion ············································································{Tables 1, 2 and Figures 1-3} Chapter 4. Conclusions and Perspective···································································57 Chapter 5. References ······························································································58-71 Chapter 6. Figures and Tables ··················································································72-90. 5.
(6) 中文摘要 累積的研究證據顯示,在子宮頸癌病患的血液內可發現腫瘤去氧核醣核酸,而 血液內的腫瘤去氧核醣核酸具有診斷和臨床預後的價值。人類乳突病毒去氧核醣核 酸,在子宮頸癌病患的血清和血液中,被偵測到的比率是百分之七至四十五, 而這 差異可能是由於偵測樣品的不同,例如血清或血漿、萃取去氧核醣核酸的方法不同、 或是使用分析的工具不同,例如傳統的聚合酶反應 (PCR),即時定量 PCR、或是利 用酵素免疫的 PCR 和不同的引子 (primers),例如 L1、E6、E7,因此在過去的文獻 報告中,只有少數是有關在血液中偵測 HPV DNA 的比較。. 因為即時定量 PCR 可用來偵測在血液中 HPV DNA 的低病毒量,所以本論文的 第一部採用即時定量 PCR 來改善病毒的偵測率,提供一前瞻性的人類乳突病毒偵測 方法,使病人在被診斷出疾病的同一時間偵測其 HPV DNA,並討論其臨床意義。研 究的結果顯示:以即時定量 PCR 的方法可以在超過四分之一(27%)的子宮頸癌病患 血液中偵測到 HPV DNA。且在帶有 HPV 16, 18 或是 52 型的子宮頸癌病患中,幾乎 有百分之五十的病患,可在血液裡偵測到 HPV DNA。本研究提供了子宮頸癌病患在 治療後,其血液中 HPV DNA 病毒量連續追蹤的數據並強調其臨床意義的重要性。 在本研究中,有 6 位子宮頸癌病患於治療完成後,其血液中偵測不到 HPV DNA,且 在後續的追蹤中都沒有復發。而在連續追蹤中,有 10 位子宮頸癌病患在治療完後三 個月,仍可在血液裡偵測到 HPV DNA,其中有 8 位發生轉移,且有 7 位發生的是遠 端轉移。雖然本研究局限於不多的病人數,及追蹤時間不夠長,但經統計分析結果 顯示:在血液裡被偵測出定量的 HPV DNA 的確反應了腫瘤轉移與否,且具有其預 後價值。換言之、子宮頸癌病患在治療完後仍可在其血液中偵測到 HPV DNA,是可 用來預測該病患未來復發與否的一個有用指標,並可用以決定哪一些子宮頸癌病患 需要更積極的治療。. HPV DNA 嵌入宿主細胞基因體,被認為是子宮頸癌癌化轉變的重要事件,而且 發生在早期子宮頸癌的階段,然而大部分的研究報告都著重在 16 型 HPV 病毒,少 數著重在 18 型上。在美國、歐洲、非洲、及東南亞洲,52 型和 58 型發生在子宮頸 癌病患相對是較低的,而在台灣和亞洲地區,52 型和 58 型是較常見的致癌型別。. 6.
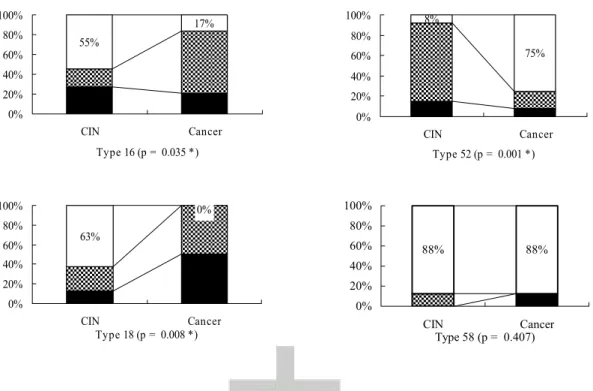
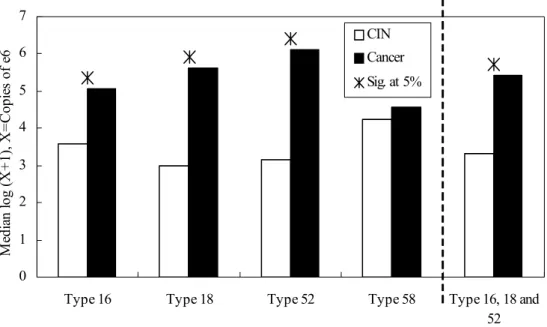
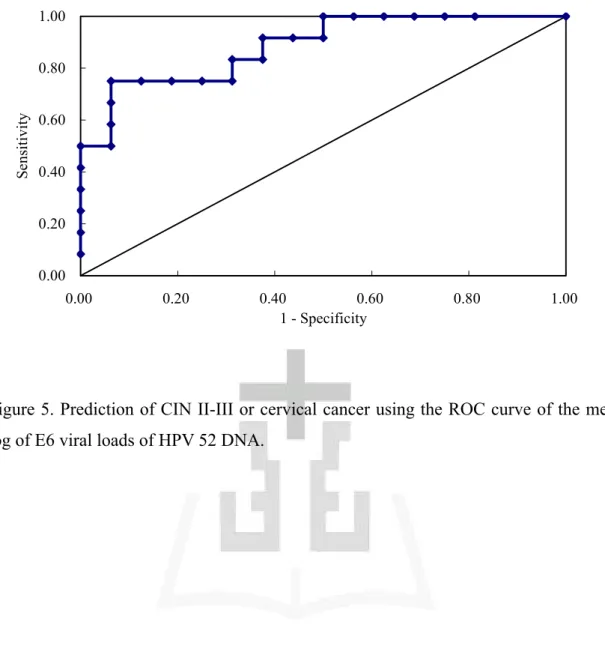
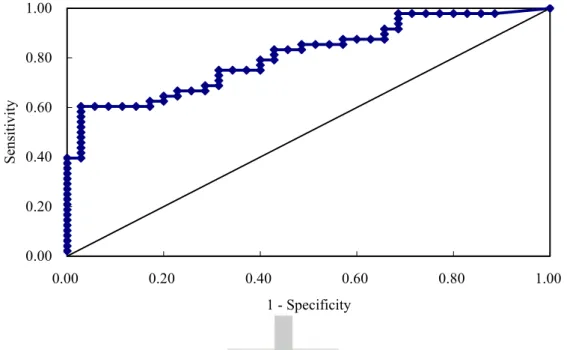
(7) 為瞭解 HPV 52 型及 58 型,是否和 16 型及 18 型一樣其嵌入宿主細胞基因體,或是 高病毒量是癌化過程中必要的,本論文第二部份的研究著重於 HPV 52 型和 58 型嵌 入宿主細胞基因體的致癌過程。分析子宮頸分泌物採自 178 位連續病患、包含 81 位 子宮頸癌和 97 位子宮頸中度至重度細胞病變之患者,利用基因晶片和定量即時 PCR 技術,檢查並判定 HPV16、18、52、58 型的盛行率,和其嵌入狀態和病毒量。. 研究結果發現,於台灣婦女子宮頸癌病患中並不常見到 HPV 52 型和 58 型病毒 DNA 嵌入到人類基因體中,可見病毒 52 型和 58 型其 DNA 嵌入宿主基因體並非是 子宮頸癌發展必須的因素。相反的,16 型及 18 型病毒 DNA 嵌入宿主基因體是導致 子宮頸癌非常重要的步驟。而 16、18、52 型的高 E6 病毒量,則具有預測高度細胞 病變轉變至子宮頸癌的能力。可見 HPV DNA 是否嵌入宿主基因體和其病毒量,在 子宮頸癌癌化過程中,可能因病毒型別的差異而扮演不同的角色。在此研究中我們 成功地利用 HPV 16、18、52 型的病毒量(the median log of viral loads) 來預測子宮頸 癌,選擇的分界點可以達到預測子宮頸癌 62.5% ~83.3% 的敏感度,及 0-25%的偽陽 性機率。ROC 曲線分析顯示所建立的模型能準確地預測、鑑別及診斷出高度細胞病 變,或是子宮頸癌發生在病人感染 HPV 16 型、18 型或 52 型分別達 73.8%,92.9%, 88.57%的正確率。. 最後本論文的研究著重在低度細胞病變與病毒的相關性。幾乎 50%的非典型鱗 狀上皮細胞和 80%的低度細胞病變,會被致癌型的 HPV 感染;而 HPV DNA 的測試 對非典型鱗狀上皮細胞患者,可提供訊息轉介這些病患做陰道鏡檢查並查出潛藏的 高度細胞病變和子宮頸癌。相反的,致癌型的 HPV DNA 檢測並無法提供低度細胞 病變更一步的訊息供臨床做進一步的選擇性處理;因為在低度細胞病變患者身上有 相當高的比率可偵測到 HPV DNA。而臨床上,對於低度細胞病變的處理是在 3 至 6 個月後重複做抹片檢查,或是直接陰道鏡切片檢查,所以發展出一個可供低度細胞 病變患者臨床處理選擇的模式,以區分哪些患者可能會進展到高度細胞病變,哪些 會自動痊癒,就非常有價值。. 本研究測試在低度及高度細胞病變中,於亞洲最常見的癌前病變致癌病毒型別 HPV 16、18、52、58 四型之病毒量,並評估 2 年累積進展到高度細胞病變的危險性, 7.
(8) 且探討病毒 DNA 嵌入宿主基因體是否為導致低度細胞病變進展到高度細胞病變的 主要原因。此外,並探討在 6 個月後重複做抹片檢查時,E6 病毒量的改變是否會導 致進展成高度細胞病變。研究結果發現低度細胞病變患者在 6 個月後,病毒量增加 者比病毒量沒有增加的患者有 45%的危險性會進展成高度細胞病變。利用定量即時 PCR 偵測病毒量,發現病毒量增加者比沒有增加的患者有大於 7 倍的危險性會進展 成高度細胞病變;若用 HC2 技術偵測病毒量發現病毒量增加者比病毒量沒有增加的 患者有大於 6 倍的危險性會進展成高度細胞病變。這兩種技術偵測到的病毒量是一 致的 (Person’s coefficient, r=0.687, p<0.001)。結果亦指出,6 個月後重複檢測的 HPV DNA 病毒量,病毒量的改變可用來預測感染 HPV DNA 16、18、52、58 型的低度細 胞病變患者,是否進展成高度細胞病變且與臨床結果相符。. 總結,本論文的研究對 HPV DNA 病毒量和嵌入宿主基因體的狀態,在子宮頸 癌癌化過程中所扮演的角色,提出其指標性的臨床運用,以預測癌前病變及子宮頸 癌患者的疾病進展。. 8.
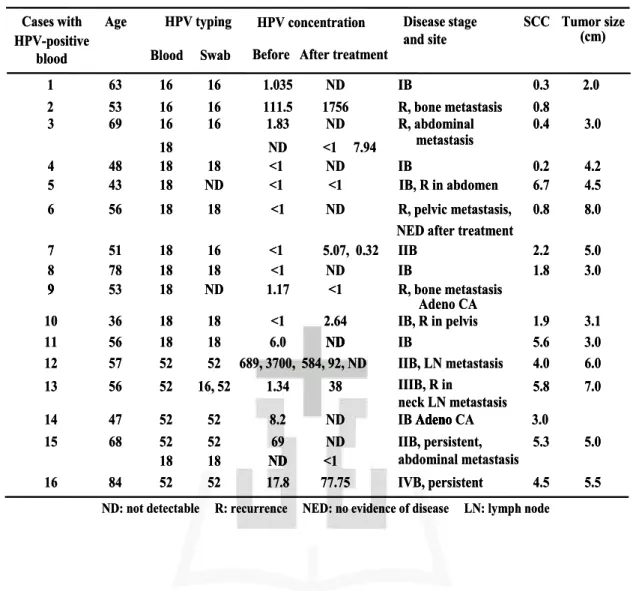
(9) Abstract Accumulating evidence shows that tumor DNA can be found in the circulation of patients with cervical cancer. The presence of such tumor DNA in the blood may be of diagnostic and prognostic value. HPV DNA has been found in serum or plasma samples from cervical cancer patients with detection rates varying from 7% to 45%. The discrepancy may be due to different target materials (serum or plasma), method of extracting DNA, tools of analysis (conventional PCR, real-time PCR, or PCR-enzyme immunoassay), and differing primers used (L1, E6, E7). Therefore, information regarding the comparison of detection rates of HPV DNA in circulating blood is limited. The first part of this study provides a prospective study of HPV DNA detection at a single diagnostic time point. Real-time PCR is used to detect the low viral loads of HPV DNA in blood. The results show that more than one-fourth (27%) of patients with invasive cervical cancer had HPV DNA detected in their blood samples. Approximately 50% of patients with confirmed HPV 16, 18 or 52 positive cervical cancers had HPV DNA detected in their blood. This study also used serial follow-up data on HPV DNA viral load among cervical cancer patients after treatment to understand its clinical significance. Six cervical cancer patients with HPV DNA viral loads undetectable in their blood after treatment showed no recurrence during follow-up. In longitudinal follow-up, eight out of ten cervical cancer patients with viral loads of HPV DNA detectable in the blood at 3 months after treatment were associated with recurrence. Among these, seven of eight patients had distant metastases. Although the study was limited to a small number of patients and a short period of follow-up, it is worth pointing out that detection of circulating HPV DNA after treatment could predict recurrence. It is postulated that blood HPV DNA might be a useful marker to select subsets of patients who need more aggressive treatment. The presence and quantity of HPV DNA in blood are likely to be a reflection of metastasis and may be of prognostic value. The second part of this study focuses on the role of integration of HPV type 52 and 58 in cervical cancer patients. The integration of HPV DNA into the host genome is thought to occur early in cancer development and to be an important event in malignant transformation of cervical cancer. However, most studies on the integration of HPV DNA focus on type 16 and a few on type 18. While HPV type 52 and 58 are oncogenic types 9.
(10) with relatively low prevalence in cervical cancer in the Americas, Europe, Africa and Southeast Asia, they are as prevalent as the known high-risk (for cervical cancer) HPV types 16 and 18 in Taiwan and other Asian countries. To analyze whether integration or high viral loads of human papillomavirus (HPV) are essential for malignant transformation of HPV type 52 and 58 as well as type 16 and 18, cervical swabs from 178 consecutive patients, including 81 with invasive cervical cancers and 97 with cervical intraepithelial neoplasias (CIN) II-III, were collected and examined to determine the prevalence, physical status and viral load of HPV type 16, 18, 52 and 58 DNA using genechip and real-time PCR (polymerase chain reaction) analysis. The infrequent integration of HPV 52 and 58 DNA in cervical cancer suggests that it is not a prerequisite for progression to cervical cancer. By contrast, integration appears to be a critical step for carcinogenesis of HPV 16 and 18 DNA. High viral loads (E6) of HPV 16, 18 and 52 DNA may be predictive of the transition of CIN II-III to cervical cancer. The results indicate that both viral DNA physical status and viral loads of HPV are important factors in the carcinogenesis of different HPV types. This study successfully used the median log of viral loads of HPV 16, 18 and 52 DNA to predict the presence of cervical cancer. The selected cut-off values of the median log of viral loads in HPV 16, 18 and 52 DNA achieved 62.5-83.3% sensitivity and a 0-25% false positive rate in predicting the presence of cervical cancer. The ROC curve analyses indicated that the model could accurately predict the diagnostic group of CIN II-III or cervical cancer in 73.8%, 92.9%, and 88.5% of patients with positive HPV 16, 18 and 52, respectively. The third part of this study focuses on low-grade squamous intraepithelial lesions (LSILs). Approximately 50% of atypical squamous cells of undetermined significance (ASCUS) and 80% of LSILs are infected by oncogenic types of HPV. HPV DNA testing for patients with ASCUS provides useful information and allows referral of patients for immediate colposcopy to detect high-grade squamous intraepithelial lesions (HSILs) and cancer. By contrast, oncogenic HPV DNA testing is not informative for triage of patients with LSILs because a high percentage of LSIL patients are HPV positive. A repeat Pap smear in 3 to 6 months or direct biopsy under colposcopy is generally used in clinical practice. Development of alternative triage strategies for women with LSILs would be valuable in distinguishing women with LSILs that have high probabilities of progression to HSILs from women with LSILs that have spontaneously regressed. 10.
(11) The 2-year cumulative risks were evaluated for HSIL attributable to HPV 16, 18, 52, and 58, the most common oncogenic types in pre-invasive cervical lesions including LSILs and HSILs in Asia, and questioned as to whether the integration of HPV oncogenes into the host genome contributed to the risk of LSILs progressing to HSILs. In addition, it was determined whether or not E6 viral load and its change contributed to the risk of LSILs progressing to HSILs during the interval between baseline diagnosis of LSIL by Pap smear and a 6-month follow-up visit by repeat Pap smear. It was found that women with LSILs whose viral loads increased between baseline and 6 month follow-up had a 45% risk of developing HSIL, which was seven-fold greater than those without increased viral loads (OR = 7.6, 95% CI = 1.9 to 29.4, p < 0.01), as evaluated by real-time PCR. The risk was calculated at 44%, a six-fold greater risk than those without increased viral loads (OR = 6.1, 95% CI = 1.6 to 22.7, p < 0.01), as evaluated by HC2. The two viral load measures correlated well (Person’s coefficient, r = 0.687, p < 0.001). The results indicate that evaluation of viral load changes (increased or not increased) through repeat HPV DNA testing could predict progression of disease in LSIL cases of HPV types 16, 18, 52, and 58, which correlates to clinical implications. In summary, this research strives to understand the role of HPV DNA viral loads and integration in the carcinogenesis of cervical cancer by searching for a useful marker applicable in clinical practice to predict disease progression in pre-invasive and invasive cervical cancer.. 11.
(12) Chapter 1: General Introduction Epidemiology of cervical cancer Cervical cancer is a major health burden in women, with 493,000 women around the world diagnosed with cervical cancer and 273,000 dying from this cancer in the year 2002. Worldwide, cervical cancer is the second most common female cancer in the world, with a mean age standardized incidence rate of up to 18.8 per 100,000 women, and is a major cause of mortality for women in developing countries (Bosch et al, 2003). Of these, more than 80% of deaths occurred in the low and medium-resource countries of South and South-East Asia, sub-Saharan Africa, and South and Central America. In fact, one-third of the cervical cancer burden in the world is experienced in South Asia. It is also a serious health problem in Taiwan, with 2,061 new diagnosed cases and 874 mortality cases of cervical cancer in 2003, second in incidence only to breast cancer, as reported by the Bureau of Health Promotion, Department of National Health. The annual incidence of invasive cervical cancer in Taiwan was 17.2 per 100,000 (National Cancer Report, 2003). Based on strong epidemiological evidence and supported by basic experimental findings, there is no doubt that persistent infections with high-risk types of human papillomavirus (HR HPV) represent a necessary cause of cervical cancer (Walboomers et al, 1999; zur Hausen, 2002; Bosch et al, 2003; Munoz et al, 2003). High risk HPV DNA can be detected in up to 99.7% of cervical squamous cell carcinomas (SCC) (Walboomers et al, 1999; Munoz et al, 2003) and in 94-100% of cervical adenocarcinomas and adenosquamous carcinomas (Zielinski et al, 2003). The etiological role of most common high-risk HPV types, such as types 16 and 18 in pre-invasive and invasive cervical cancers has been demonstrated by epidemiological evidence and molecular studies (IARC, 1995; Walboomers et al, 1999). Cytology screening has been largely responsible for the significant decline in the burden of cervical cancer in developed countries over the last 5 decades. However, only around 50% annual screening rates have been achieved in Taiwan, in comparison with around 80% annual screening rates in Europe and America. Also, although the cytological screening system itself is improving, it has limited sensitivity and specificity for cervical cancer and up to 30% false-negative results still occur (Solomon et al, 2002). Women are 12.
(13) affected by the discomfort, complications and anxiety of the screening procedures, positive Pap smear results and follow-up investigations or treatments (Renshaw et al, 2004). In addition, adenocarcinomas develop deeper in cervical tissues than the surface cells taken for Pap smears and cervical adenocarcinoma may not initially be detected, leading to late-stage diagnosis (Schiller and Davies, 2004). With regard to prevention research, epidemiologists are currently evaluating the possibility of reinforcing screening programs by adding HPV tests to the cytology. Age at first intercourse, number of sexual partners, high parity, cigarette smoking, race, and low socioeconomic status has consistently been shown as significant risk factors for cervical cancer. However, all these factors are linked to sexual behavior and acquisition of HPV; none have been shown to be significant independent risk factors. Sexual behavior has been consistently identified as a major risk factor for cervical cancer and population-based studies have demonstrated that risk related to sexual activity is mediated by HPV infection (Ley, et al, 1991; Bauer et al, 1993; Hildesheim et al, 1993; Silins et al, 2000; Lazcano-Ponce et al, 2001). HPV infections are among the most common sexually transmitted infections in most populations, and estimates of exposure range from 15-20% in many European countries, to 70% in the US, 95% in high-risk populations in Africa, and 10-15% in general populations in Taiwan (unpublished data). Based on global statistics, life-time risk according to the US center for disease control for sexually active men and women is at least 50 percent (Centers for Disease Control and Prevention, 2004). By age 50, at least 80 percent of women will have acquired HPV infections. HPV infections are highly prevalent in young individuals, whereas invasive cervical cancer does not typically develop until the third decade of life or later. The overwhelming majority of women today with a diagnosis of cervical cancer have either not had regular Pap tests or they have not been followed up after detection of an abnormal smear. Not undergoing regular Pap tests is the single greatest risk factor for a poor outcome in women who develop cervical cancer. Choice of contraceptive methods also appears to affect the risk of acquiring cervical cancer and barrier mechanisms have been associated with reduced risk, whereas the use of oral contraceptives has been associated with an increased risk.. 13.
(14) Molecular mechanisms of cervical cancer Originally, it was thought that cervical SCC would always evolve from infected normal cervical epithelium via a continuum of long-lasting, consecutive CIN I, CIN II, and CIN III lesions. However, an alternative concept that finds increasing support is that many of the clinically relevant CIN II-III lesions may be rapidly induced within 2-3 years following infection (Winer et al, 2005), whereas it can be deduced from Wallin et al (1999) and Zielinski et al (2001) that it takes another 10-12 years to develop invasive cervical cancer. As a consequence, most CIN I lesions and some CIN II lesions should not be considered as true precursor stages of cervical cancer, but rather the cytopathological effect of a productive viral infection. Support for this comes from studies showing that low-grade CIN lesions harbor low-risk HPV types that confer a negligible risk of progression (Lungu et al, 1992). Moreover, CIN I and some CIN II lesions that harbor HR HPV types display viral expression patterns suggestive of productive viral infections (Stoler et al, 1992; Dürst et al, 1992). In these infections, active viral replication and virion production are strongly coupled to the differentiation program of the infected epithelium. Low levels of viral activity in the infected basal cells characterize this process, with monomeric episomes being co-replicated with the genome of the host cell. Upon differentiation, viral transcription, including that of the viral E6 and E7 oncogenes, is markedly increased while vegetative DNA amplification and assembly of new virions occurs only in squamous epithelia undergoing terminal differentiation. By contrast, some CIN II lesions, and CIN III lesions, exhibit a dramatic topographical change in viral gene expression, which includes an increase in E6/E7 expression in proliferating dysplastic cells (Stoler et al, 1992; Dürst et al, 1992). Although the mechanism underlying deregulated E6/E7 expression in proliferating cells is not yet understood, in vitro studies using epithelial raft cultures have shown that altered histone deacetylation may be a contributing factor (Zhao et al, 1999). In addition, high-grade CIN lesions and cervical carcinomas often show integration of the viral genome into that of the host cell (Klaes et al, 1999), a phenomenon that is accompanied by DNA aneuploidy (Melsheimer et al, 2004). In fact, integration may also interfere with the normal regulation of E6/E7 expression, either by interruption of transcriptional control mediated by the viral E2 protein, or by increased stability of chimeric E6/E7 host cell transcripts, or a 14.
(15) combination (Jeon and Lambert, 1995; zur Hausen et al, 2002). Although chromosomal instability is tightly linked to HPV 16 integration in cervical keratinocytes, it is still unclear whether integration represents the cause or simply the consequence of genomic instability (Pett et al, 2004). The molecular basis for oncogenesis in cervical cancer can be understood by the regulation and function of the two viral oncogenes, E6 and E7 (Mantovani and Banks, 2001; Munger et al, 2001). These two genes have been shown to posses transforming ability when transfected into epithelial cells (Dürst et al, 1987; Münger et al, 1989). Furthermore, the persistent expression of E6 and E7 is necessary for the maintenance of the malignant phenotype (Chen et al, 1993; Seagon and Durst, 1994; von Knebe Doeberitz et al, 1994). The E6 and E7 genes are under the regulation of the E2 gene product (Bernard et al, 1989; Dowhanick et al, 1995). The integration of the viral circular DNA into the patient’s genome is necessary for the malignant phenotype (Vernon et al, 1997). The E2 gene is often the site for integration resulting in disruption of the E2 gene and subsequent transcription of the E6 and E7. Viral DNA integration into host cell DNA usually disrupts the E1 and E2 open reading frames (ORFs). By contrast, the E6 and E7 ORFs and LCR (long control region), generally remain intact (Daniel et al, 1997; Lazo, 1997; Romanzuk and Howley, 1992; Syrjänen and Syrjänen, 2000). Increasing the expression of these oncoproteins (E6 and E7) was through three steps: (1), increase copy number of HPV DNA (Steenbergen et al, 1996); (2), mutations in the long control region (at YY1 motits) (Dong et al, 1994; Park et al, 1999); and (3), integration of HPV DNA into the cellular genome (zur Hausen et al, 2002; Jeon et al, 1995). Elimination of HPV 16 E2 protein expression due to integration results in up-regulation of the transcription of the E6 and E7 oncogenes possibly provides a selective growth advantage for the infected cell (Jeon et al, 1995; Jeon and Lambert, 1995). The E6 gene product binds to the resident p53 tumor suppressor gene and induces an ubiquitin-mediated proteolysis. E7 targets another tumor suppressor, the Rb gene product. By altering its phosphorylation state, E7 functionally inactivates this protein, which, like p53, functions in cell cycle control (Dyson et al, 1989; Munger and Howley, 2002). The interactions that are thought to be most relevant for their transforming functions are E6 binding, via the cellular protein E6-AP, to the tumor suppressor gene product p53, and E7, binding to the retinoblastoma tumor suppressor gene product pRb and its related pocket 15.
(16) proteins, p107 and p130 (Davies et al, 1993). In addition, HR HPV E6 can activate the telomere-lengthening enzyme telomerase independent of p53 binding, and E7 can induce abnormal centrosome duplication through a mechanism independent of inactivation of pRb and its family members (Munger et al, 2004). It is likely that these latter properties also contribute to the transforming characteristics of these viral oncoproteins. Cervical cancer is a multistep process initiated by a high-risk HPV (HR HPV) infection. Productive HPV infections are characterized by expression of the viral oncogenes E6/E7 in the differentiated cell layers, deregulated expression of E6/E7 in the dividing basal cells is suggested to represent the first step in the multistep process of HPV-mediated transformation (Munger and Howley, 2002). Interference of the viral oncogenes E6 and E7 with the apoptosis and cell cycle regulation p53 and pRb in the proliferating cells results in the induction of genomic instability (Dyson et al, 1989; Duensing et al, 2000). The genomically unstable environment provides the driving force for the acquisition of crucial alterations in oncogenes and tumor suppressor genes that are additive requirements for malignant transformation (Snijders et al, 2006). In vitro studies show HPV could make cell lines immortalized but non-tumorigenic (Choo et al, 1994; Yokoyama et al, 1995). Expression of the high risk HPVs may lead to aneuploidy (change of chromosome number) and contribute to the other cellular events necessary for full cancer development. Analysis of the transformation of epithelial cells in vitro has revealed at least four consecutive stages characterized by different phenotypes, i.e.,. extended. lifespan,. immortalization,. anchorage-independent. growth,. and. tumourigenicity in nude mice (Chen et al, 1993). Loss of tumor suppressor gene(s) at chromosome 11 has been implicated in the progression from an immortal to a tumourigenic phenotype, since introduction of chromosome 11 into SiHa cells abrogated their capacity to form tumors in nude mice, without affecting immortality (Koi et al, 1989). The significance of this finding was supported by allelotyping studies, showing frequent deletions at 11q loci, particularly 11q22-23, in cervical carcinomas (Hampton et al, 1994). Steenbergen et al (2004), collected functional evidence that the tumor suppressor in lung cancer 1 (TSLC1) gene (also named IGSF4 or NECL-2) may be the candidate suppressor of tumourigenicity on chromosome 11. TSLC1 gene was found to be silenced in 91% (10/11) of cervical cancer 16.
(17) cell lines, mostly as a result of promoter hypermethylation alone or combined with allelic loss (Steenbergen et al, 2004). TSLC1 promoter hypermethylation was also detected in 58% of cervical carcinomas and 35% of high-grade CIN lesions, but not in low-grade CIN lesions or normal cervix (Steenbergen et al, 2004). Moreover, ectopic expression of TSLC1 suppressed both tumor formation in nude mice and anchorage-independent growth of SiHa cells (Steenbergen et al, 2004). It is interesting that from a model system of non-tumorigenic hybrids of the HPV 18-containing cervical cancer cell line, HeLa with fibroblasts and their tumorigenic segregants, a change in the composition of the AP-1 complex emerged as being relevant for tumorigenicity (Soto et al, 1999; Finzer et al, 2000). Characteristics of human papillomavirus The HPV genome consists of eight kilobasepairs, and is a non-enveloped double-stranded DNA molecule. The genome can be divided into three regions; the long control region (LCR) without coding potential, the region of early proteins (E1-E8), and the region of late proteins (L1 and L2). E6 and E7 are the most important oncogenic proteins. Transcription of the E6 and E7 genes was observed always to occur in cervical carcinomas and this was the first indication of an important role for these genes in HPV-associated tumorigenesis. The E6 ORF encodes a small protein of approximately 150 amino acids with a molecular weight of 16-18 kD. The E6 protein of HR anogenital types shows only weak oncogenic potential in most established cell lines and cooperation with the E7 protein is required for full transforming and immortalizing capacity. The E7 ORF encodes for a small protein of approximately 100 amino acids with a molecular weight of 10 kD. E7 is the major transforming oncogene of HPVs (Burd, 2003). HPV’s belong to the family Papovaviridae. They consist of a 72-capsomere capsid containing the viral genome. The capsomeres are made of two structural proteins; the 57kDa late protein L1, which accounts for 80% of the viral particle, and the 43-53 kDa minor capsid protein L2. L1 is major capsid protein and has an immunogenic role. E6 and E7 are oncoproteins. E1 and E2 maintain a stable viral episome and initiate viral replication. The E1-E2 junction is the site of integration. E4 probably facilitates the release of newly formed virions from the cell. E5 results in neoplastic transformation in some experimental systems (Burd, 2003).. 17.
(18) The evidence of HPV infection and cervical carcinogenesis is based on the E6 and E7 of high-risk HPV types can transform cells in culture (Munger and Howley, 2002). Integrated forms from HPV DNA 16 or 18 in cervical cancer was found in contrast to that of episomal forms from type 6 or 11 in condydoma (Badaracco et al, 2002; Thomas et al, 2001). The interaction of E6 of HPV 16 and 18 is from binding with p53 in contrast E7 with Rb. The integrated state revealed E2 disruption from E1-E2 junction and caused E6, E7 expression (Daniel et al, 1997; Lazo, 1997; Romanzuk and Howley, 1992; Syrjänen and Syrjänen, 2000). When HPV DNA integrated into host cellular genome, E2 function lost could not inhibit E6 and E7 function. The key action of HR E6 proteins is the inhibition of the function of p53, a tumor suppressor protein, by enhancing its degradation through the ubiquitin pathway (Mantovani and Banks, 2001). In non-infected cells, the ubiquitin mediated degradation of p53 is triggered by the mdm-2 protein, while in HR HPV infected cells the E6 AP complex replaces mdm2 in the control of cellular p53 levels (Huibregtse et al, 1993; Scheffner et al, 1990). Most E6 proteins from LR HPVs do not bind to p53, and none of them induce its degradation (Huibregtse et al, 1993). HR HPV E6 proteins lead to a down-regulation of p53-dependent transcription, and E7 acts by binding cellular proteins of the pRB tumor suppressor family, which, by interacting with the E2F family of transcription factors, control cell replication. Binding of E7 to the active form of pRB leads to the release of the E2F transcription factors, which stimulates entry into the S-phase of the cell cycle and leads to cell replication (Munger et al, 2001). In vitro studies show HPV can make cell lines immortalized but non-tumorigenic. Other factors are necessary for the development of cervical cancer such as environmental factors, host related factors and viral factors (Choo et al, 1994; Yokoyama et al, 1995; Tjalma, 2005). The environmental factors include smoking, parity, oral contraceptives, sexual transmitted disease and diet. The host related factors include endogenous hormones, immune response, and genetic susceptibility traits such as specific HLA alleles. The viral factors include HPV type and variant, viral load and viral integration (Choo et al, 1994; Yokoyama et al, 1995; Tjalma, 2005). As a consequence of chromosomal instability induced by deregulated viral gene expression, viral genomes or fragments may become integrated into the host cell 18.
(19) chromosomes. There is no specific integration locus within the host cell genome, although fragile sites are preferred as integration sites (Wentzensen et al, 2004). In contrast, the viral genome reveals few highly characteristic features. The consequences of HPV integration include increase of messenger RNA half-life, abrogation of the E2 repression effect, position effects on viral transcription, insertion mutagenesis and target for epigenetic modification (Bhattacharjee and Sengupta, 2006; Wilke et al, 1996; Jeon et al, 1995). In all analyzed cervical carcinoma cells, a cassette consisting of the viral promoter and enhancer element located in the upstream regulatory region, and the genes E6 and E7 are retained intact on integration (Jeon et al, 1995). The cassette is concisely transcribed, and the fusion of the viral sequences with cellular sequences that are co-transcribed at the 3’ end of the transcript favor the stability of these transcripts, resulting in a higher oncogenic potential (Jeon et al, 1995). Although HPV 16 and 18 are the most common HPV types in cervical cancer, a recently pooled analysis of case-control studies world-wide led to the classification of 15 different HPV types as HR HPV types, with another three types considered probably high risk (Munoz et al, 2003). HPV’s were originally classified into cutaneous types such as HPV 1, 4, 10, etc, and mucosal types such as HPV 6, 16, 18, etc (Chan et al, 1992). The anogenital HPV’s have been divided into two groups: the first is associated with a high risk for cervical cancer development the HR HPVs (16, 18, 26, 31, 33, 39, 45, 51, 52, 53, 56, 58, 59, 66, 68, 73 and 82), and the second group with a low carcinogenic potential - the low-risk (LR) HPV’s (6, 11, 40, 42, 43, 44, 54, 61, 72 and 81) (Munoz et al, 2003). Oncogenic properties of HPV It is well known that HR HPV infections, although necessary, are far from sufficient for the pathogenesis of cervical cancer. In fact, cervical cancer is only a rare complication of HR HPV infection and requires several additive conditions and events to accumulate once an infection has become evident. This is particularly exemplified by the fact that HPV infections are very common in young women but frequently resolve spontaneously. The life-time risk of contracting HPV is estimated to be 80% (Baseman and Koutsky, 2005), and at least 80% of the HR HPV infections are likely to be transient, not even giving rise to CIN lesions (Meijer et al, 2000). In recent decades, the oncogenic properties of HPV have been intensively studied and significant progress has been achieved in the investigation of HPV prevention. More 19.
(20) than 35 types of HPV infect the genital tract, type 16 and 18 inducing about 70% of cervical cancers and high-grade of cervical intraepithelial neoplasia, and HPV type 6 and 11 causing 90% of genital warts (Muñoz et al, 2004). A prophylactic vaccine that targets these types would substantially reduce the burden of HPV-associated clinical disease. The oncogenic properties of HPV probably require specific viral types in conjunction with specific environmental and host-defined factors. A multistep pattern of cervical cancer development postulates that specific types of HPV produce an infection months to years before the development of invasive carcinoma, but only selected patients proceed to develop the carcinoma, which is preceded by a series of precursor lesions. Originally, the transforming properties of HR HPV types in epithelial cells were established by studies showing their capacity to induce immortalization of primary human keratinocytes (Dürst et al, 1987). Upon prolonged culturing, it was found that fully tumorigenic clones could emerge from HPV-immortalized cells (Chen et al, 1993; Seagon and Durst, 1994). This is in line with the assumption that HR HPV alone can induce malignant growth as long as genomic instability triggered by its E6/E7 functions is allowed to proceed uninterrupted, leading to the accumulation of relevant additive (epi) genetic changes. The inactivation of Rb as a result of deregulated HR HPV expression is characterized by a permanent up-regulation of the cyclin dependent kinase inhibitor owing to a disruption of the Rb dependent negative feedback loop regulation p16INK4A expression (Lieskovska et al, 1999). In line with this, diffuse p16INK4A immuno-histochemical staining patterns can be found in HR HPV-containing high-grade CIN lesions, cervical carcinomas and carcinomas of other anogenital sites that are HR HPV related, such as penile carcinomas (Murphy et al, 2003). The uncontrolled cell proliferation resulting from the inactivation of Rb and concomitant induction of E2F is also reflected in an altered expression of proliferating markers, such as minichromosome maintenance proteins (MCMs), PCNA and Ki-67 in CIN lesions and cervical carcinomas (Keating et al, 2001; Williams et al, 1998). Viruses considered related to cervical cancer are human papillomavirus, herpes simplex virus, and human immunodeficiency virus. Several HPV related cancers are reported including cervical cancer, penile cancer, vulva cancer, vaginal cancer, colorectal cancer, esophageal cancer, lung cancer, and head and neck cancer.. 20.
(21) Biological Importance of this Study and Hypothesis Accumulated evidence shows that tumor DNA can be found in the circulation of patients with cervical cancer (Stroun et al, 2000; Anker et al, 1999). The presence of tumor DNA in the blood may be of diagnostic and prognostic value. Genetically or even epigenetically altered tumor DNA present in the primary tumor can also be detected in the serum or plasma (Nawroz et al, 1996; Sanchez-Cespedes et al, 2000). Cervical cancer is the leading cancer among women in Taiwan. Liaw et al studied the association between HPV infection and cervical cancer in Taiwanese women and found that 10% of low-grade and 33% of high-grade cervical neoplasias could be explained by infection with HPV subtypes 52 and/or 58 (Liaw et al, 1995). Huang et al reported that HPV-52 and -58 were as prevalent as the high-risk HPV types 16 and 18 in Chinese women (Huang et al, 1997).. HPV DNA has been found in serum or plasma samples from cervical cancer patients with detection rates ranging from 7% to 45% (Capone et al, 2000; Dong et al, 2002; Widschwendter et al, 2003; Pornthanakasem et al, 2001; Liu et al, 2001). The discrepancy in these rates may be due to differences in target materials (serum or plasma), methods used to extract DNA, tools used to analyze DNA (either conventional PCR, real-time PCR, or PCR-enzyme immunoassay) and in primers selected (L1, E6, E7). Few studies have compared detection rates of HPV DNA in circulating blood (Capone et al, 2000; Dong et al, 2002; Widschwendter et al, 2003; Pornthanakasem et al, 2001; Liu et al, 2001). In addition, several studies have suggested that HPV viral load might play an important role in the progression from HPV infection to cervical cancer development (Josefsson et al, 2000; Ylitalo et al, 2000). Testing of this hypothesis via prospective study with HPV DNA detection at diagnosis and during follow-up is mandatory. Therefore, whether the detection of HPV type 16, 18 and 52 DNA in the peripheral blood of patients with cervical cancer using real-time PCR is feasible and correlates with clinical prognosis will be examined in this study. Previous studies suggested that benign HPV lesions and CIN I lesions mostly contain the viral sequences only as episomes (Choo et al, 1987; Jeon et al, 1995). In contrast, viral DNA is integrated into the host genome in virtually all cases of cervical carcinomas and their derivate cell lines (Boshart et al, 1984; Vernon et al, 1997). Study by Peitsaro et al (2002), revealed that integrated HPV type 16 is frequently found in cervical cancer precursors, and rapid progression of the CIN lesions was closely associated with a heavy 21.
(22) load of integrated HPV 16. HPV 16 DNA integration has been associated with malignant transformation, with increased frequency from CIN to invasive cancers (Nagao et al, 2002). In contrast, a significant proportion of advanced cancers containing only the episomal form of HPV DNA have demonstrated that HPV16 integration might not be essential for malignant transformation (Badaracco et al, 2002; Das et al, 1992). On the other hand, the presence of HPV 18 may be associated with an aggressive phenotype which more rapidly progresses from dysplasia to invasive cancer. One very important finding is that 100% of HPV 18 positive cervical carcinomas contain integrated viral DNA only (Badaracco et al, 2002). In addition to integration, heavy viral loads in CIN lesions have recently been shown to increase the risk of carcinoma development in situ by at least 60-fold (Josefsson et al, 2000). However, whether viral load or integration status of HPVis a risk factor for cervical cancer progression remains unclear due to the conflicting results obtained using different methodologies in previous studies. In addition, data on the physical state of HPV 52 and 58 DNA in patients with CIN II–III and invasive cervical cancer have not been reported. This study will analyze whether integration or high viral loads of human papillomavirus (HPV) is essential for malignant transformation of HPV types 52 and 58, as well as types 16 and 18. Approximately 50% of atypical squamous cells of undetermined significance (ASCUS) and 80% of LSILs are infected by oncogenic types of HPV (ALTS group, 2000; Solomon et al, 2001). HPV DNA testing for patients with ASCUS provides useful information and allows referral of patients for immediate colposcopy to detect high grade squamous intraepithelial lesions (HSILs) and cancer (Solomon et al, 2001). In contrast, oncogenic HPV DNA testing is not informative for triage of patients with LSILs because a high percentage of LSIL patients are HPV positive (ALTS group, 2000). A repeat Pap smear in 3–6 months or direct biopsy under colposcopy is generally used in clinical practice. Development of alternative triage strategies for women with LSILs would be valuable in distinguishing women with LSILs that have high probabilities of progression to HSILs from women with LSILs that have spontaneously regressed. Due to the lack of sufficiently large prospective longitudinal follow-up studies and the different geographic distributions of HPV types, it has not been established how the risk of HSILs differs during transition by the physical status of HPV 16, 18, 52, and 58 DNA (integrated versus episomal DNA) during longitudinal follow-up, the viral loads 22.
(23) (high vs. low) and the viral load change (increased vs. not increased) between baseline and follow-up among women with LSILs. Thus it is important to have better prediction of the risk of progression of low-grade squamous intraepithelial lesions (LSILs) of the uterine cervix in women with human papillomavirus (HPV) infections. Specific Aims Following questions are aims to achieve in this proposal: (1) Whether the genotype and viral load of HPV in blood and cervical swabs is correlated? (2) Whether the detection of HPV type 16, 18 and 52 DNA in the peripheral blood of patients with cervical cancer using real-time PCR is feasible and its correlation of clinical prognosis. (3) Whether integration or high viral loads of HPV is essential for malignant transformation of HPV types 52 and 58 as well as types 16 and 18? (4) Whether integration or high viral loads of HPV predict prospectively the risk of progression of low-grade squamous intraepithelial lesions (LSILs) of the uterine cervix in women with HPV infections.. 23.
(24) Chapter 2: Materials and Methods Evaluating the feasibility of detecting HPV type 16, 18 and 52 DNA in the peripheral blood of patients with cervical cancer using real-time PCR and to determine its clinical significance: A hospital-based study was performed to determine the prevalence of type 16, 18 and 52 HPV infections not only in cervical swabs but also in blood among women with pre-invasive and cervical cancer residing in Taipei, Taiwan. Blood and cervical swab specimens from 135 consecutive patients with 60 invasive cervical cancers, 10 microinvasions, 20 cervical intraepithelial neoplasias (CIN III, 10 CIN II, 10 CIN I) and 25 controls, were collected and examined for HPV type 16, 18 and 52 DNA using real-time PCR to investigate the prevalence and viral load of HPV DNA at the time of diagnosis and during follow-up in patients with positive blood samples. This study was designed to provide new information regarding the occurrence of cervical cancer in patients with HPV subtype 52 detected in circulating blood, a relatively uncommon finding among cervical cancers in the Americas, Europe, Africa and Southeast Asia. The study protocol was reviewed and approved by the Institutional Review Board and Research Grant Committee of Cathay General Hospital. A total of 135 patients treated in the gynecologic cancer center of Cathay General Hospital (CGH) from January 2003 to December 2003 were recruited. Patients were recruited consecutively from those diagnosed with CIN lesions during examinations between January and June 2003. Among the 135 patients, 25 patients with benign tumors who received a simple hysterectomy performed by the same surgeon were recruited between January and March 2003 to serve as controls. The controls had no pathological findings of CIN or cancer of the cervix. Justification of the sample size is that this study was designed to detect a clinically meaningful difference in the prevalence rates of positive test results for HPV DNA in blood samples between patients with invasive cervical cancer and patients with CIN or the controls. Assuming that the incidence rate of positive test results for HPV DNA in blood samples for patients with CIN or the controls is less than 2% (Dong et al, 2002), the selected sample size of 130 (65 per group) will give a 97% probability of correctly 24.
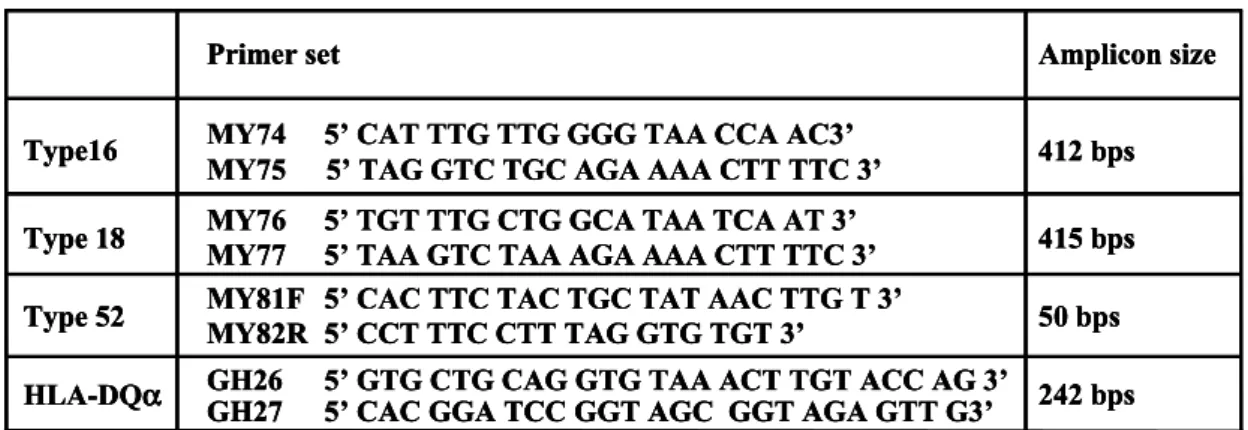
(25) detecting a 25% difference in the prevalence rate of positive test results for HPV DNA in blood samples at the 5% level of significance. Both blood specimens and cervical swabs were collected from all patients for the viral load detection of HPV types 16, 18 and 52 using real-time PCR. However, two of the 60 invasive cervical cancer specimens from cervical swabs could not be obtained due to lack of permission from patients. All patients underwent complete physical and gynecologic examination, and the cervical cancer was staged according to the guidelines of the International Federation of Gynecology and Obstetrics (FIGO). By the end of December 31, 2004, all patients had follow-up after primary treatment at 3-month intervals for the first two years or until death. All surviving patients were followed up for at least one year. The follow-up investigations included physical examination, cervical cytology, chemistry profiling and analysis of tumor markers such as serum squamous cell carcinoma antigen (SCC-Ag) or CA-125. Further examinations, such as computed tomography (CT) of the pelvis, bone scan, chest radiography or biopsy of any suspected lesions, were performed when clinically indicated. Distant metastasis was defined as disease that occurred outside the pelvis. The association was evaluated between the HPV DNA level in the blood and clinical parameters such as tumor size, clinical staging, tumor marker, lymph node metastasis, lymphovascular space involvement (LVSI), histological type and adjuvant therapy. Among patients with a HPV-positive blood sample, the correlation between the amount of HPV DNA in blood and clinical parameters was evaluated before treatment and at three months after treatment. DNA from cervical swab or blood samples was extracted using the QIAamp Blood Kit following the manufacturer’s instructions (Qiagen, Hilden, Germany). Quantitative real-time PCR fluorescent assays for each of the HPV genotypes and for the HLA-DQα gene were performed with the Qgene HPV 16, HPV 18, HPV 52 and housekeeping gene HLADQα detector kits (Qgene Biotechnology, Kaohsiung, Taiwan) along with SYBR Green dye using the ABI 5700 apparatus (Applied Biosystems, Foster City, CA). The cervical swab was taken with an Ayre spatula and agitated into 3 ml of Tris-HCl (pH 8.3), 0.2% Triton X-100, then stored at –20°C. Two ml of whole blood was obtained and stored in a tube containing citric acid. The real-time PCR assay had a dynamic range from 100 to more than 107 copies, allowing documentation of a wide range of HPV DNA copies found in the clinical specimens. 25.
(26) Samples were stratified by type of cervical disease, viral type and the range of viral DNA copies per microgram of cellular DNA, also the ability of these parameters to predict the progression of cervical carcinoma was analyzed. Blood and cervical swabs from women with CIN or cervical cancer were tested for the presence of HPV type 16, 18 and 52 DNA using real-time quantitative PCR and the presence and viral load of HPV NDA in blood and cervical swabs was correlated with CIN lesion status and the different stages of cervical cancer.. Preparation of DNA from blood and cervical swabs DNA was extracted for PCR by adding a 400-μl aliquot of a swab sample to 500 μl of DNA extraction solution (Qiagen, Hilden, Germany) with proteinase K, and then incubated at 56°C for 1 h. The Proteinase K was then heat inactivated at 100°C for 30 minutes. After centrifugation at 10,000 xg for 10 minutes at 4°C, the supernatant was collected and transferred to a new microcentrifuge tube. Next, 400 μl of the solution from the cervical swab sample was processed using the QIAamp Blood Kit (Qiagen) according to the protocol recommended by the manufacturer. For blood samples, a 400-μl aliquot lysate was incubated with the Qiagen protease and buffer AL from the QIAamp Blood Kit (Qiagen) at 56°C for 10 minutes. The lysate was applied to a QIAamp spin column, and finally eluted with 100 μl nuclease free water (QIAamp Blood DNA mini kit protocol), and vortexed for one minute before PCR amplification. Real-time quantitative PCR of HPV type 16, 18, 52 and HLA-DQα DNA Real-time PCR was performed with the Qgene HPV 16, HPV 18, HPV 52 and housekeeping gene HLA-DQα detector kits (Qgene Biotechnology, Kaohsiung, Taiwan) in a 15 μl reaction mixture and was monitored after each elongation step by SYBR Green 1 dye binding to amplify product using the ABI 5700 apparatus (Applied Biosystems, Foster City, CA). Highly specific primers were selected and hot start PCR was used to reduce the interference of non-specific primer annealing. Quantitation was done using an external standard curve. The HPV type 16 viral DNA fragment (415 bp) was amplified from genome of the CaSki cell line (Baker et al, 1987), and a 415-bp long HPV 18 viral DNA fragment was amplified from the genome of 26.
(27) a HeLa cell line (Schwarz et al, 1985). A 50-bp long HPV type 52 viral DNA was amplified from the positive clinical samples. The accurate molecular weight and copy numbers of each viral DNA fragment were determined based on UV absorption at a wavelength of 260 nm, and then used as the template DNA for establishment of the standard curve. A standard curve with each template at 106, 105, 104, 103, 102, 101, 100 copy numbers was generated in parallel with the clinical samples. Concentrations of HPV DNA were expressed as copies of HPV genome per 1 μg of cellular genome from the cervical swab or copies of HPV genome in each ml of blood. The HPV 16, HPV 18, HPV 52 and HLA-DQα primer sequences from each kit are shown in Table 1. An aliquot of 5 μl of DNA sample was added to 10 μl of PCR reagent mixture consisting of HPV optimal buffer (15 mM KCl, 20 mM Tris-HCl (pH 8.3), 0.2% Triton X 100, nuclease-free bovine serum albumin, and MgCl2), which was optimized to obtain a specific and efficient amplification - 0.3 pmol/μl of each primer, 1 mM each dATP, dCTP, dTTP, dGTP, 3.75 μl 1X SYBR Green and 0.07 U/μl AmpliTaq Gold (Roche Molecular Systems, Foster City, CA). Following the addition of the sample, the microamp tubes were capped and then centrifuged at 1,000 xg briefly. The reaction was started with a 10 minute incubation at 95°C to activate the AmpliTaq Gold, followed by 50 cycles at 95°C for 30 seconds, then 60oC for 30 seconds and finally 72°C for 45 seconds. The specificity was verified on the dissociation curve as well as by electrophoresis on 2% agarose gel. A linear plot of the log of copy numbers vs. numbers of threshold cycles was consistently obtained for HPV type 16, 18 and 52 genes, and the correlation coefficient for each target gene was between 0.995 and 1.00 in each run. Validation of Real-time PCR quantitation Both the HPV and HLA-DQα PCR reactions were performed in duplicate. Multiple negative water blanks were included in every analysis. Standard curves were run in parallel with each analysis using DNA extracted from HPV-positive cell lines (CaSki cells were derived from HPV 16 integrated human cervical carcinoma and HeLa cells from HPV 18 integrated human cervical adenocarcinoma; both obtained from the ATCC). The PCR product of HPV DNA 52 was obtained as type 52 positive controls from a clinical sample confirmed by direct sequencing. CaSki DNA and HeLa DNA were used to further validate the accuracy of the real-time PCR. CaSki cells are known to contain about 600 copies of HPV 16 genome per cell (equivalent to 6.6 pg of DNA/genome) 27.
(28) (Baker et al, 1987). Because the weight of one genome per cell is approximately equal to 1.1 (6.6/600) pg, the total cellular CaSki DNA was estimated to contain about 10,000 copies of the HPV genome. The real-time PCR results revealed that at 1.1 ng of CaSki DNA input, the amplification plot overlapped with the standard at 10,000 copies of amplified DNA from genomes of the Caski cell line and also of the HeLa cells. The normal and affected samples from the 135 patients were run in duplicate. Primers and probes to a housekeeping gene (HLA-DQα) were run in parallel to standardize the input DNA. Concentrations of blood HPV DNA were expressed as copies of HPV genome/ml of blood and were calculated using the following equation (Lo et al, 1999) C = Q x Vdna/Vpcr x 1/Vext, where C represents the target concentration in blood, expressed as copies/ml; Q represents the copy number as determined by the sequence detector; Vdna represents the total volume of DNA obtained after DNA extraction (50 μl); Vpcr represents the volume of DNA used for the PCR reaction (5 μl); and Vext represents the volume of blood used to extract the DNA. Direct sequencing of products of the Real-time PCR All products of the real-time PCR were purified using a pre-sequencing kit and then sequenced with the HPV type 16, 18 and 52 specific primers (Table 1) and a DNA sequencing kit. Finally, the sequencing products were purified using ethanol precipitation and were analyzed using an ABI PRISM 310 Genetic Analyzer (Applied Biosystems, Foster, CA). Sequence alignments were obtained using returned results from the GeneBank on-line Blast server (from URL: http://www.ncbi.nlm.nih.gov/BLAST/). Differences in proportions were evaluated using Fisher’s Exact Test. A value p<0.05 was considered significant. Statistical analysis was performed using Statistical Package for the Social Sciences software (SPSS, Chicago, IL). Analyzing whether integration or high viral loads of human papillomavirus (HPV) is essential for malignant transformation of HPV type 52 and 58 as well as type 16 and 18: Sample collections The study protocol was reviewed and approved by the Institutional Review Board 28.
(29) and Research Grant Committee of Cathay General Hospital (CGH). This prospective study was conducted to determine the prevalence, physical status and viral load of the HPV types 16, 18, 52 and 58 DNA in the cervical swabs of patients with CIN II-III and cervical cancer using genechips and real-time PCR analysis. Between January 2003 and March 2004, at the gynecologic cancer center of CGH, cervical swabs were collected at the time of diagnosis of cervical carcinoma from 81 consecutive Taiwanese patients and from 97 consecutive Taiwanese patients at the time of their diagnosis with CIN II-III. Informed consent for participation was obtained from each patient. The cervical swab was collected with an Ayre spatula and agitated into 3 ml of Tris-HCl (pH 8.3), 0.2% Triton X-100, then stored at -20oC. DNA Extraction DNA was extracted with the QIAamp DNA Blood Mini Kit (Qiagen Catalog No.51106) according to the manufacturer’s instructions. Extracted DNA was eluted with 100 μl AE buffer (10 mM Tris, pH8.5) and stored at -20oC until analysis. Diagnosis of disease and follow-up of patients All patients with CIN II-III or cervical cancer were examined by colposcopy and the diagnosis was confirmed by biopsy. All patients underwent complete physical and gynecologic examination, and the cervical cancer was staged according to the guidelines of the International Federation of Gynecology and Obstetrics (FIGO). All patients were followed up after primary treatment at 3 month intervals for the first 2 years or until death. Follow ups, including physical examination, cervical cytology, blood chemistry profile, and tumor marker detection such as SCC or CA-125, and further work up such as computer tomography (CT) scans of the pelvis, bone scan, chest radiograph, or biopsy of any suspected lesions, were performed when clinically indicated. Associations were evaluated between HPV status and viral load in swabs and clinical parameters such as tumor size, clinical staging, tumor marker, lymph node metastasis, lymphovascular space involvement (LVSI), histological type, adjuvant therapy and clinical outcome. HPV DNA genotyping The frequency of HPV DNA and genotypes were determined by a polymerase chain reaction-based (PCR) genechip method with HPV L1 gene MY11/Gp6+ consensus primers as previously described (Huang et al, 2004). The MY11/GP6+ consensus primers 29.
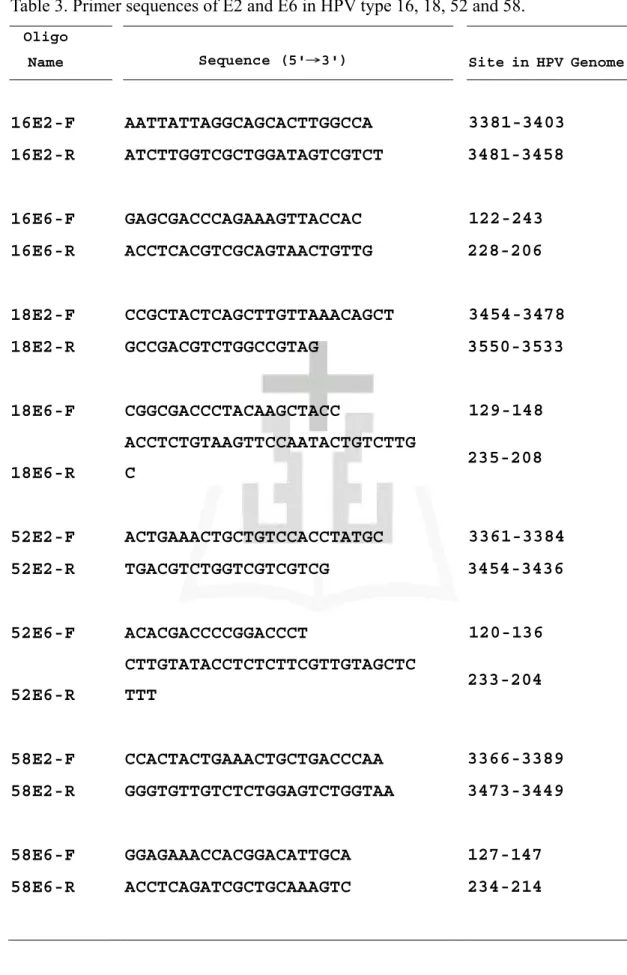
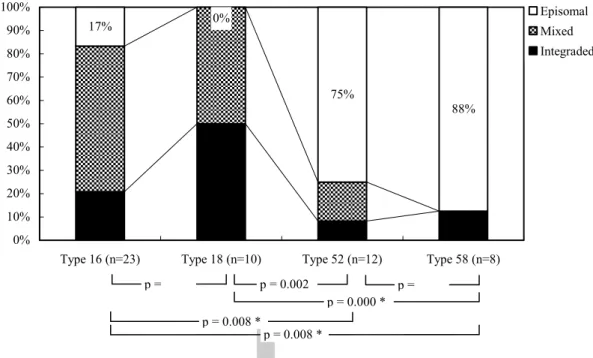
(30) were used to amplify a fragment of 190 bp in the L1 open reading frame. E2, E6 viral load absolute quantitation of HPV type 16, 18, 52 and 58 using real-time PCR DNA amplifications were carried out in a 96-well plate in an ABI Prism 5700 Sequence Detection System (Applied Biosystems). Both E2 and E6 real-time polymerase chain reactions were carried out in triplicate for each sample. Amplification and quantification of the E2 and E6 genes were carried out simultaneously in separate reactions in a 96-well PCR plate. Additionally, one sibling control sample, which had been quantified previously, was included in each reaction to serve as quality assurance of the quantification system. Numbers of the threshold cycle (Ct) obtained from E2 PCR and those from E6 PCR were regressed to the standard curve to obtain the HPV copy number. For evaluation of triplicate data, the mean value and standard deviation (SD) were calculated. Data between the ranges of mean ±1.96x SD was considered acceptable. Multiple negative water blanks were included in every analysis. The reaction was performed in a 25 μl mixture containing 1x reaction buffer (HPTM HotStart Taq SYBR Green Kit Cat No.PTM767B, Protech) and 100 nM of primers for both E2 and E6 regions. Fifty nanograms of total DNA were added to the reaction mixture. The primer sequences of E2 and E6 for HPV type 16, 18, 52 and 58 were as shown in Table 3. The amplification conditions were as follows: 10 min at 95oC, a two-step cycle at 95oC for 10s and 60oC for one minute for a total of 45 cycles. The specificity was verified by the additional dissociation curve and followed by 2% agarose gel electrophoresis. Two standard curves were obtained by amplification of serial dilutions (ranging from 10 to 10,000,000 copies per μl) of cloned plasmid containing either partial HPV 16 (from base 28 to base 3890), HPV 18 (from base 45 to base 3993), HPV 52 (from base 95 to base 3895) or HPV 58 (from base 45 to base 3994) DNA, which included equivalent amounts of E2 and E6 genes in pGEM T-Easy vector (Promega). The number of threshold cycles for E2 PCR and E6 PCR were equivalent in each run. A linear plot of the log of the copy number vs. number of threshold cycles was consistent for both genes, and the correlation coefficient was between 0.995 and 1.00 in each run. Assumptions of physical status using E2/E6 ratio The real-time PCR methods used in this study were developed based on the 30.
(31) following assumptions: (1) preferential disruption of E2 will cause the absence of E2 gene sequences in the PCR product following integration, (2) copy numbers of both genes (E2 and E6) should be equal when viral DNA presents in episomal forms, and (3) E2 gene copy numbers will be smaller than that for E6 when viral DNA presents in concomitant form. Measurement of E2/E6 ratio in relation to physical status Concentrations of HPV DNA were expressed as copies of HPV genome in 50 ng of cellular DNA. Ratios of E2 to E6 less than one indicated the presence of both integrated and episomal forms. The amount of integrated E6 was calculated by subtracting the copy numbers of E2 (episomal). The ratio of E2 to integrated E6 represented the amount of the episomal form in relation to the integrated form. Statistical analysis Statistical analysis was mainly performed using SAS 9.1.3 software. The viral load was analyzed using a Wilcoxon rank sum test based on log transformed data (y = log(x+1)) to compare differences between groups. The frequency distribution of physical status was analyzed by Fisher’s exact test. A diagnostic test based on log transformation of E6 viral loads was used to perform receiver operating characteristic (ROC) curve analysis. Analyzing whether integration or high viral loads of HPV predict prospectively the risk of progression of low-grade squamous intraepithelial lesions (LSILs) of the uterine cervix in women with human papillomavirus (HPV) infections: To examine this issue, the 2-year cumulative risk were evaluated for HSIL attributable to HPV 16, 18, 52, and 58, the most common oncogenic types in pre-invasive cervical lesions including LSILs and HSILs in Asia, and questioned whether the integration of HPV oncogenes into a host genome contributed to the risk of LSILs progressing to HSILs. In addition, it was determined if E6 viral load and its change contributed to the risk of LSILs progressing to HSILs during the 6 month interval between baseline diagnosis of LSIL by Pap smear and the 6 month follow-up visit by repeat Pap smear.. 31.
(32) Subjects and Methods The Taiwan Cooperative Oncology Group (TCOG) (T1899), a multicenter study, was conducted under the supervision of the National Health Research Institute of Taiwan. A total of 1246 women with abnormal Pap smears, including those diagnosed with ASCUS or AGUS (n = 431), LSIL (n = 437), and HSIL (n = 373), from August 1999 to March 2004, were enrolled. The details of the study design and population have been published (Chen et al, 2006; Sun et al, 2005). Of the 1246 participants, 936 underwent cervical biopsies for histologic examination. Women with LSIL (n = 437) had Pap smears, HPV testing, and colposcopic examinations every 3 months during the follow-up period. Participants were excluded from the study if they had no follow-up data (n = 60), baseline cancer on pathological examination (n = 1), fewer than 4 follow-up visits (n = 82), or no baseline HPV data (n = 2). Women with histologically confirmed HSIL were defined as having disease progression and were treated and exited from the study. Women with LSIL with two consecutive normal Pap smears and who showed HPV clearance during the follow-up period were defined as in remission and also exited. Women with LSIL not in remission or progression were defined as having persistent disease. HPV persistence was defined as HPV positivity for a given type tested on two consecutive occasions versus clearance. A total of 294 women with LSIL, having at least four follow-up visits every 3 months, and 460 women with HSIL were tested for HPV DNA using both HC2 and PCR-reverse line blotting and were included in the longitudinal follow-up study (unpublished data). Among the 294 patients with LSIL, 187 specimens from 65 women with HPV 16 (n = 14), 18 (n = 8), 52 (n = 30) and 58 (n = 13) were collected at baseline and followed up every 6 months until follow-up showed disease progression. The specimens were further tested for viral load, E2/E6 ratio and viral load change using real-time PCR. Four who lacked samples of follow-up HPV DNA were excluded from final analysis. In addition, 212 HSIL positive patients with HPV 16 (n = 92), 18 (n = 5), 52 (n = 57), or 58 (n = 58) infections were also obtained and tested for viral load, E2/E6 ratio, and physical status of HPV DNA using real-time PCR to compare with data from LSIL specimens. Specimens for viral load and viral load change by hybrid capture two were also tested and these results compared to those obtained by real-time PCR to predict disease progression. 32.
數據


+7
相關文件
How would this task help students see how to adjust their learning practices in order to improve?..
It is well-known that, to deal with symmetric cone optimization problems, such as second-order cone optimization problems and positive semi-definite optimization prob- lems, this
Due to rising prices in winter clothing and footwear, as well as increasing housing rent and expenses of house maintenance, indices of Clothing and footwear; and Rent and
Attributable to increasing rent of housing and expenses of house maintenance, rising prices in summer clothing and footwear, as well as fresh vegetables, the indices of Clothing
The Composite CPI for March 2008 dropped slightly by 0.08% month-to-month, with lower charges for outbound package tours and hairdressing services, as well as lower prices of
Microphone and 600 ohm line conduits shall be mechanically and electrically connected to receptacle boxes and electrically grounded to the audio system ground point.. Lines in
Generic methods allow type parameters to be used to express dependencies among the types of one or more arguments to a method and/or its return type.. If there isn’t such a
Thus, emotional intelligence and social support are main elements to reduce teacher stress and interpersonal conflict, as well as to increase job
