Intra-tracheal Administration of Budesonide/Surfactant to Prevent Bronchopulmonary Dysplasia.
Prevention of Bronchopulmonary Dysplasia in Very Low Birth Weight Infant-A New Therapeutic Regimen
Tsu F. Yeh1,2, Shou Y. Wu5, Zahid Ullah5, Tsai C. Li6,7, Wu S. Hsieh8, Chang H. Tsai2,9, Hung C. Lin2 Chung M. Chen1,3,4
1Maternal Child Health Research Center, College of Medicine, Taipei Medical University, Taipei, Taiwan; 2Department of Pediatrics, Children’s Hospital, China Medical University, Taichung, Taiwan; 3Department of Pediatrics, Taipei Medical University Hospital, Taipei, Taiwan; 4Department of Pediatrics, School of Medicine, College of Medicine, Taipei Medical University, Taipei, Taiwan. 5Division of Neonatology, John Stroger’s Hospital of Cook County, Chicago, USA; 6Graduate Institute of Biostatistics, College of Public Health, China Medical University, Taichung, Taiwan; 7Department of Healthcare Administration, College of Health Science, Asian University, Taichung, Taiwan, and 8Department of Pediatrics, College of Medicine, National Taiwan University and Hospital, Taipei, Taiwan; 9Department of Biotechnology, Asian University, Taichung, Taiwan.
Correspondence and requests for reprints should be addressed to Tsu F. Yeh, M.D., Ph.D., 252 Wu-Hsing Street, Taipei 110 or 2 Yuh Der Rd. Taichung, 40447, Taiwan. E-mail:
S.Y.W., W.S.H., and H.C.L. Acquisition of the data and statistical analyses: Z.U., S.Y.W., T.C.L., and C.H.T. Drafting the manuscript for important intellectual content: T.F.Y., C.M.C., Review and revision of manuscript: T.F.Y., S.Y.W., Z.U., T.C.L., W.S.H., C.H.T., H.C.L., and C.M.C.
Funding: This work was supported in part by National Health Research Institute, Taiwan, NHRI-EX98-9818PI, NHRI-EX99-9818PI, NHRI-EX100-9818PI, NHRI-EX101-9818PI
Running head: Intra-tracheal Budesonide/Surfactant Prevents BPD
Descriptor number: 14.7 Bronchopulmonary Dysplasia Total word count for the body of the manuscript:3490
At a Glance Commentary
Scientific Knowledge on the Subject: Bronchopulmonary dysplasia (BPD) is an important complication of mechanical ventilation in preterm infants and no definite therapy can eliminate this complication. Pulmonary inflammation plays a crucial role in its pathogenesis.
Glucocorticoid is one of the most effective therapies to treat or prevent BPD. However, systemic glucocorticoid therapy is not generally recommended because of long-term adverse events. What This Study Adds to the Field: Intra-tracheal administration of surfactant/budesonide compared with surfactant alone significantly decreased the incidence of BPD or death in very low birth weight infants with severe respiratory distress syndrome. The infants received intra-tracheal surfactant/budesonide had significantly lower interleukin levels in intra-tracheal aspirates compared with infants received intra-tracheal surfactant alone during the study period.
Abstract
Rationale: Bronchopulmonary dysplasia (BPD) is an important complication of mechanical ventilation in preterm infants and no definite therapy can eliminate this complication. Pulmonary inflammation plays a crucial role in its pathogenesis and glucocorticoid is one potential therapy to prevent BPD.
Objective: To compare intra-tracheal administration of surfactant/budesonide with that of surfactant alone on the incidence of death or BPD.
Methods: A clinical trial was conducted in 3 tertiary neonatal centers in the United States and Taiwan in which 265 very low birth weight infants with severe respiratory distress syndrome who required mechanical ventilation and inspired oxygen ≥50% within 4 hours after birth were randomly assigned into 2 groups (131 intervention and 134 control). The intervention infants received surfactant (100 mg/kg) and budesonide (0.25 mg/kg), and the control infants received surfactant only, until the infant required inspired O2 <30% or was extubated.
Measurements and Main Results: The intervention group had a significantly lower incidence of BPD or death [55/131 (42.0%) vs 89/134 (66%); risk ratio 0.58, 95% confidence interval 0.44 to 0.77, P<0.001; number needed to treat (NNT) 4.1 (95% confidence interval 2.8 to 7.8). The intervention group had significantly lower interleukin levels (IL-1, IL-6, IL-8) in tracheal aspirates at 12 hours and lower IL-8 at 3-5 and 7-8 days. No significant immediate adverse events were observed.
Conclusions: In very low birth weight infants with severe respiratory distress syndrome, intra-tracheal administration of surfactant/budesonide compared with surfactant alone significantly decreased the incidence of BPD or death without immediate adverse effect.
Word count for the abstract: 248
Keywords: bronchopulmonary dysplasia; very low birth weight infants; surfactant; budesonide; respiratory distress syndrome
Bronchopulmonary dysplasia (BPD) is the most important pulmonary complication following mechanical ventilation in preterm infants. Various strategies including the use of vitamin A and caffeine have been reported to be beneficial for BPD (1-3). However, no definite therapy can eliminate this complication.
Although the mechanism is not completely clear, pulmonary inflammation is believed to play a central role in the pathogenesis of BPD. Dexamethasone is one of the most effective therapies to treat or prevent BPD. However, systemic dexamethasone therapy is not generally recommended because of long-term adverse effects (4-5). Administering inhaled glucocorticoids to preterm infants is technically challenging and the effects are limited (6-8). It is therefore important to find a therapeutic method that reduces the systemic adverse events of
glucocorticoids while at the same time retaining local anti-inflammatory effects on the lungs. Budesonide is a glucocorticoid with strong local anti-inflammatory effects. A pilot study showed that intra-tracheal instillation of budesonide, using surfactant as a vehicle, significantly improved pulmonary status (9). A multi-center, randomized clinical trial was therefore undertaken to determine whether early intra-tracheal administration of budesonide / surfactant would reduce the incidence of BPD or death as compare with the use of surfactant alone. The results was presented in Pediatric Academic Societies (PAS) meeting, 2013 in Washington D.C. and in European Academy of Paediatric Societies, 2014; Barcelona..
Methods
Study Populations
Between April 1, 2009 and March 1, 2013, all infants with respiratory distress shortly after birth were assessed by the main investigators from 3 tertiary centers, John H. Stroger Jr. Hospital (JSH), Chicago, National Taiwan University Hospital (NTUH), Taipei, and China Medical
University Hospital (CMUH), Taichung, Taiwan for eligibility for the study. The inclusion criteria were determined within 4 hours after birth and included: 1) birth weight < 1500 gm, 2) radiographic evidence of severe respiratory distress syndrome (RDS) (grade III-IV) (10), 3) mechanical ventilation, 4) fractional inspired oxygen (FIO2) ≥0.5, and 5) absence of severe congenital anomalies or lethal cardiopulmonary disorders. Thus, the infants were considered to be at high risk for developing BPD. The study was approved by the Institutional Review Board of each participating hospital. Verbal consent was obtained from the mother before delivery and written consent was obtained within 4 hours after birth when inclusion criteria were determined. Intra-tracheal Budesonide/Surfactant Instillation
Infants were randomized into either the intervention or control group based on an assignment list designed by a statistician (TCL). Concealed randomization was generated by a computer with permuted blocks in random sizes of 2, 4, 6, and 8 to maintain balance. A list of patient
assignments was given to each participating hospital, with half of the infants assigned to intervention and half to control at each hospital. An outside independent observer (CMC) who was not aware of the study assignment followed the outcome of BPD or death of each infant. When the first dose was to be prescribed, the main investigator in the participating hospital would open the assignment list and prepare the appropriate syringe. The control group received surfactant only (Survanta, 100 mg or 4 ml/kg, Abbott Laboratory) and the intervention group received surfactant (100 mg or 4 ml/kg) and budesonide (Pulmicort neubulising suspension, Astra Zeneca) (0.25 mg or 1 ml/kg). This dosage provided a concentration ratio of surfactant to budesonide of >50:1, which was demonstrated in vitro study in Surfactometer and in High-Performance Liquid Chromatography (HPLC) that this mixture did not affect the biophysical and chemical properties of surfactant (11) (see appendix) Except for a difference in volume, the
solution in either syringe was clear and indistinguishable. The syringe was covered by adhesive tape so that the volume of the solution could not be identified. Before intra-tracheal instillation, the syringe was gently vortex, and surfactant or surfactant/budesonide mixture was administered in a manner similar to that of routine surfactant therapy. Repeated administration of
surfactant/budesonide or surfactant only was given every 8 hours to infants in the intervention or control groups, respectively, until they required <0.3 of FIO2 or were extubated.
Respiratory Care
During the study, only the main investigator of each participating hospital (TFY, SYW in JSH, HCL in CMUH and WSH in NTUH) was aware of the content of the syringe. The neonatology fellows and residents who were blinded to study assignment were the primary physicians in charge of the daily care. A general guideline for management of RDS and fluid therapy was followed as described previously (9). For infants who had respiratory distress shortly after birth, a trial of nasal continuous positive airway pressure (NCPAP) was initiated in the delivery room and infants with severe retraction or poor respiratory effort or apnea were intubated. The goal of ventilation therapy in the NICU was to maintain O2 saturation at 90-95%, PCO2 ≤50 mmHg, and pH ≥7.20. Infants who failed to respond adequately to NCPAP (FIO2 ≥ 0.6 and O2 saturation < 85%) were subsequently intubated. The respiratory care guideline focused on indications for using NCPAP, intermittent mandatory ventilation (IMV), high frequency oscillatory ventilation (HFOV), and weaning from mechanical ventilation. During the study, “assisted O2 therapy” was defined as requirement of any of the following: nasal cannula, NCPAP, IMV, or HFOV. Blood gases and acid-base measurements were obtained each morning. Nitric oxide was not given to very low birth weight infants during the study period. Indomethacin was given to infants who had significant patent ductus arteriosus (PDA). Clinically significant PDA was defined using a
scoring system described previously (12). Heart rate, peripheral pulse, precordial activity, chest radiograph and intensity of murmur were evaluated. A score > 3 was often associated with a left atrium/aortic root ratio 1.3. If the infant had PDA on echocardiogram and had a score > 3, he or she was considered as having clinically significant PDA. Postnatal systemic dexamethasone was reserved only for infants who had severe underlying lung disease and had intractable respiratory failure (on IMV with FIO2 1.0 or on HFOV). In such cases, a short course of dexamethasone (3 to 5 doses of 0.25 mg/kg every 12 hours) was given at the discretion of the attending physician.
Outcome Measurements
Diagnosis of BPD was made at 36 weeks’ postmenstrual age by the attending physician and confirmed by the independent observer (CMC) if the infant continuously had respiratory distress since birth and on supplemental oxygen (>21% O2) at 36 weeks’ postmenstrual age. This
definition, designed by Shennan et al was used in this study because it was considered a better predictor of abnormal pulmonary outcome for very low birth weight infants (13). At the time of designing this study in early 2009, we used this traditional definition because of two reasons: 1) this definition has been used for many years in our units, our medical and nursing staffs were very familiar with this definition; and 2) this definition would provide a chance to compare BPD incidence with our previous study (9) and with those important studies reported from others (2, 3, 14-16). Because of the severe RDS shortly after birth and because of continuous respiratory distress since birth, our infants most likely represented a well establish underlying lung disease at the time of BPD diagnosis. At the end of study, a post hoc analysis was also done based on a current definition by National Institute of Child Health and Human Development (NICHD) in infants <32 weeks gestation (1). This definition was a severity-based definition. In this
definition, infants who required supplemental oxygen therapy at 28 postnatal days were
considered to have BPD. However, a moderate BPD was defined as the need for <30% oxygen and severe BPD was defined as the need for 30% oxygen at 36 weeks’ postmenstrual age. Tracheal aspirates were assayed (17) for interleukins (IL-1, IL-6 and IL-8) using commercial ELISA kits at 12 hours, 24 hours and between 3 to 5 days and 7-8 days after starting the study in the first 40 infants.
Animal Study
To investigate if surfactant can be used as a vehicle to facilitate budesonide delivery, Sprague-Dawley rats were intratracheally injected with 50 μL surfactant/18F-budesonide mixture (with a concentration ratio of 12.50:0.12 mg/mL by equal volume mixing, n = 3) or with 50 μL 18 F-budesonide only (0.12 mg/mL, n = 3). The 18F-budesonide biodistribution and radioactivity was visualized and measured at 15, 30, 45, and 60 min after injection by a Nano/PET/CT digital scan. Statistical Analysis
The primary outcome assessed was the incidence of BPD or death. Our previous experience indicated that about 60% of infants who fulfilled the inclusion criteria would develop BPD or die (9). We hypothesized that 60% in the control group and 40% in the intervention group would develop BPD or die. Allowing a 5% chance of type I error and a 10% chance of type 2 error, the number required in each group would be 130 (18). An estimated 140 patients was considered an adequate number for each group.
The secondary outcomes assessed were anti-inflammatory mediators (IL-1, IL-6, IL-8) in the tracheal aspirates during the first week. Adverse effects, including changes in serum electrolytes, glucose, blood urea nitrogen and blood pressure were measured on days 1, 3, 5, 7, 14, 21 and 28 according to the study protocol. Body weight was routinely measured daily but the length and
head circumference were measured at 2, 3 and 4 postnatal weeks. The incidence of
intra-ventricular hemorrhage, necrotizing enterocolitis, severe retinopathy of prematurity (grade III), and clinical sepsis or bacteremia were recorded from routine care. Cranial ultrasounds were taken routinely in these infants at least twice during the first week and subsequently taken if needed. Eye ground was examined by a pediatric ophthalmologist on a routine schedule in NICU for all infants <1500 gm. Mortality, BPD morbidity, requirement of assisted O2 therapy and the number of surfactant dose administered were also explored
All analyses were performed according to the intention-to-treat principle with missing data being imputed by last observation carried forward method. In addition, we performed sensitivity analysis by using multiple imputation for missing data. The results using multiple imputation were similar since few observations were missing. Results using last observation carried forward were more conservative and so are presented. The mean and standard deviation were reported for continuous variables, and the number and percentage were reported for categorical variables. The Chi-square test or Fisher exact test was used for categorical variables including death, BPD, BPD or death, and BPD severity. The risk ratio was calculated as the ratio of the cumulative incidence rates of an event occurring in the budesonide-treated group to the control group, and the number needed to treat (NNT) as the inverse of these 2 cumulative incidence rates.. For continuous variables, the mean values at each time point in each group for variables such as FIO2, PO2, PCO2, pH, oxygen index (OI) and mean airway pressure (MAP) were derived from a generalized linear model with generalized estimating equations (GEE) and differences in values over time were compared between the 2 groups (19). GEE was used to account for the dependence between outcomes of participants at different times. The Wilcoxon’s rank-sum test was used to compare interleukin levels in tracheal aspirates between the groups. Kaplan-Meier cumulative incidence
plots were generated to show time-to-event end points including being extubated and being weaned to room air. A post hoc analysis of the primary outcome was conducted to adjust for prenatal steroid, Apgar score and chorioamnionitis. For secondary outcomes and immediate side effects, no adjustments were made. All statistical analyses were performed using SAS for Windows (Version 9.2, SAS Institute, Inc). All P values were 2-sided and considered significant if P < 0.05.
Results
Patient Population
During the study period, 1215 very low birth weight infants were treated for respiratory distress at birth; 858 infants required intubation within 4 hours and were admitted to NICU and thus were eligible for the study. However, only 287 met the inclusion criteria. Of these, 22 infants were excluded for various reasons. The final number included for analysis was 265; 131 in the treated group and 134 in the control group (Figure 1). Their baseline data were comparable (Table 1). Primary Outcomes
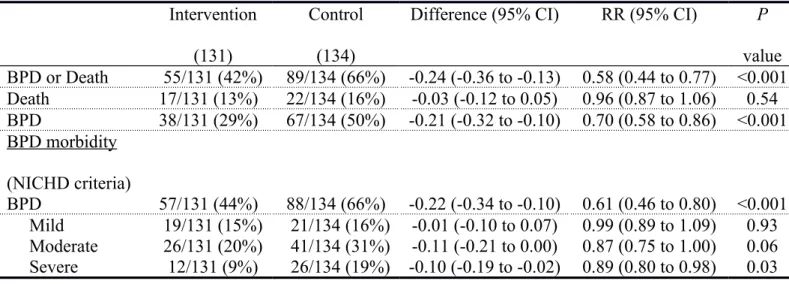
Infants in the intervention compared with controls had a lower incidence of BPD or death (55/131 [42.0%] vs 89/134 [66%], risk ratio 0.58, 95% confidence interval 0.44 to 0.77, P < 0.001); NNT 4.1 (95% confidence interval 2.8 to 7.8) (Table 2).
Secondary Outcomes
Of the 40 infants studied for tracheal aspirate interleukins, 2 were excluded because of
incomplete sampling. The intervention was associated with significantly lower median values for IL-1, IL-6, and IL-8 at 12 hours (all P < 0.05) and lower IL-8 on days 3-5 and days 7-8 as compared with surfactant alone (Table 3).
growth during the study. (Figure 2) The 2 groups were comparable in incidence of
intra-ventricular hemorrhage [53/131 (40.5%) vs 57/134 (42.5%), P = 0.80)], necrotizing enterocolitis [4/131 (3.1%) vs 7/134 (5.2%), P = 0.56], severe retinopathy of prematurity [7/131 (5.2%) vs 9/134 (6.8%), P = 0.79], clinical sepsis and/or bacteremia [29/131 (22%) vs 38/134 (28%), P = 0.31].
Exploratory Outcomes
The 2 groups were comparable in mortality; however, the intervention was associated with a significantly lower incidence of BPD compared with surfactant alone [38/131 (29.0%) vs 67/134 (50.0%), relative risk 0.70, 95% confidence interval 0.58 to 0.86, P < 0.001 (Table 2).
The intervention compared with surfactant alone was associated with a significantly lower OI on day 1 and day 5, and a lower FIO2 requirement on day 1 and lower MAP during the first 3 days (Figure 3) and a significantly (P = 0.03) higher chance of weaning to room air during the study (Figure 4). The intervention was associated with a significantly lower proportion of infants who required assisted O2 therapy compared with the control group on day 3 (93.0% vs 99.2%, relative risk and 95% confidence interval 0.94 (0.92 to 0.99), P = 0.017), day 7 (87.2% vs 96.0%, 0.91 (0.86 to 0.97), P = 0.021) and day 21 (70.9% vs 86.2%, 0.82 (0.73 to 0.95), P = 0.007). The intervention was associated with a lower incidence of significant PDA [(40/131 [30.5%] vs 59/134 [70.9%], 0.69 (0.49 to 0.97), P = 0.032)]. The total durations of IMV [median and range: 8 (4-62) vs 16 (9-58) days], and O2 therapy [32 (4-82) vs 48 (8-102) days] were not significantly different between groups. Four infants in the treated group and 9 infants in the control group received systemic dexamethasone therapy.
Infants in the intervention group required significantly fewer doses of surfactant than infants in the control group (1 dose: 85/131 [64.9%] vs 49/134 [36.6%]; P < 0.001; 2 doses: 43/131
[32.8%] vs 58/134 [43.3%]; P=0.09, 3 doses: 3/131 [2.3%] vs 23/134 [17.2%], P < 0.001; 4 doses: 0/131 [0%] vs 1/134 [0.7%]; 6 doses: 0/131 [0%] vs 3/134 [2.2%]).
Post Hoc Analyses
The post hoc analysis of the primary outcome adjusted for prenatal steroid, Apgar score and chorioamnionitis also showed a significant difference between the intervention and control group ( odd ratio 0.37, 95% confidence interval 0.22 to 0.54, p<0.01). Based on the NICHD
definition, infant in the intervention group had a significantly lower overall incidence of BPD and severe BPD than infant in the control group (Table 2)
Pulmonary Distribution of 18F-Budesonide
The radioactivity of 18F-budesonide was most strongly detected near the trachea at 15 min after intra-tracheal injection (Figure 5A). Almost no radioactivity was seen in the lung region of the rats injected with 18F-budesonide alone at 60 min. The radioactivity of 18F-budesonide was distributed more in the peripheral lung and stayed longer in rats supplemented with surfactant than in the rats without surfactant. Rats injected with surfactant/18F-budesonide mixture exhibited an approximately 200% increase in radioactivity compared with rats that received 18F-budesonide alone during the study period (Figure 5B). The detail results will be published elsewhere.
Discussion
This study demonstrated that in very low birth weight infants with severe RDS, intra-tracheal instillation of budesonide/ surfactant significantly reduced the incidence of BPD or death compared with surfactant alone. No serious adverse effects were seen. Budesonide plus surfactant was associated with better pulmonary status and lower MAP for ventilation in the early course of therapy and subsequently a decreased need for assisted and supplemental O2 therapy. The improvement in these parameters in the intervention group may account for the
subsequent lower incidence of BPD.
The mechanism to use surfactant as a vehicle was based on a physical phenomenon, the
“marangoni effect” (20). This effect is basically the mass transfer along an interface between two fluids due to surface tension gradient. Thus, when surfactant is instilled into the lungs of infants with RDS, a convection flow is generated that may facilitate the delivery of medications, such as budesonide, to the lung periphery. Various animal studies indicated that intra-tracheal
administration of surfactant and corticosteroid improved lung function (21-24) Direct intra-tracheal instillation of budesonide without using surfactant as vehicle has not been shown
effective (25). A recent clinical trial using high-dose inhaled budesonide has been registered but the result has not been reported (26).
Our pilot study indicated that more than 80% of budesonide may remain in the lungs for up to 8 hours after intra-tracheal instillation of survanta/budesonide (9). Besides using as a vehicle surfactant may also enhance the solubility of budesonide and increase budesonide absorption (27). Budesonide is not metabolized by lung cells; rather, it is conjugated extensively with fatty acids, resulting in the formation of budesonide esters at the C21-hydroxyl group (28). This conjugation process is reversible, and the conjugates can be hydrolyzed inside the cell, gradually releasing free budesonide into the surrounding medium. This reversible conjugation may improve airway selectivity and prolong its local anti-inflammatory action in the lungs, possibly explaining why budesonide was effective for days, even though only 1 or 2 doses were administered. Based on the pharmacokinetic data (9), we estimate that 5-10% of budesonide may still remain in the lungs by one week. Budesonide that is absorbed into the circulation is rapidly metabolized in liver to 16-α-hydroxyprednisolone, which has low glucocorticoid activity. The elimination half-life of plasma budesonide is about 4 hours (9). The results of our study also
suggest that a similar therapeutic method may be applied to shock lung, pneumonia, severe acute respiratory syndrome, or malignancy. The systemic adverse effects associated with steroids, antibiotics, and chemotherapeutic agents could be markedly reduced. Further studies are needed for this clinical implication..
The mechanism responsible for the effectiveness of budesonide is most likely due to its anti-inflammatory effects. The improvement was seen early after intra-tracheal
surfactant/budesonide instillation as opposed to 2-3 days following systemic administration of dexamethasone (29). The direct local anti-inflammatory effect may have played an important role for this rapid improvement. This rapid improvement may be also related to the higher volume of instillation in the intervention group (5 ml/Kg) as compared to the control infant (4 ml/Kg) that might facilitate surfactant/budesonide delivery. However, the higher volume could also dilute the surfactant concentration in the liquid-air surface and decrease the surface-tension reducing property of surfactant. Although there were small changes in FIO2, PO2 and PCO2 during the first few days, the intervention group needed less assisted O2 therapy on days 3, 7, and 21, suggesting a longer effect on the lungs. Lung inflammation occurs very early following mechanical ventilation and any therapy beneficial for BPD prevention has to be administered as early as possible. The results from our study indicated that budesonide was effective early in the course of therapy, which might translate to longer term effects on the lungs.
A major concern following glucocorticoid therapy is long-term adverse effects. Budesonide has been used in children with asthma for years without significant long term side effects (30-33). While the follow up study is still in progress, our preliminary data on 84 % of the survival up to 2-4 years indicates no apparent long term adverse effect on physical growth, and on
neuromotor and cognitive function. Based on our previous follow-up study (30) and the current preliminary results, and in view of the fact that majority of the infant (65%) in the intervention group received only one dose of budesonide and that there was no immediate adverse effect, the long-term side effects are probably negligible. A complete and longer follow up study is needed before this therapeutic regimen can be generally recommended
This study was done in 3 tertiary centers in 2 countries, which may raise the question of its general application. However, diagnostic criteria and assessment tools that have good predictive accuracy and have been evaluated across different hospital settings were used. All the
participating hospitals followed a standard protocol for respiratory care. In addition, an independent observer unaware of the treatment assignment monitored the outcome; this may decrease the study bias.
In conclusion, in very low birth weight infants with severe RDS, intra-tracheal administration of surfactant and budesonide compared with surfactant alone significantly decreased the incidence of BPD or death. Further large sample double blind trials are warranted.
Acknowledgement: The authors like to thank Roberta A. Ballard, MD, PhD, and Philip L. Ballard, MD, PhD, from UCSF, California, and William Oh, MD, from Brown University, Rhode Island, for their expertise comments; Ju C. Cheng, PhD, from Department of
Biotechnology, China Medical University, Taichung, Taiwan for interleukins assay. Mei H. Wang, PhD, from Institute of Nuclear Energy Research (INER), Longtan, Taiwan for Nano/PET digital scan of F-18 labeled budesonide in rats. We also thank Ms. Yu C. Pan and Hsiang T. Chou for manuscript preparation and all the NICU nursing staffs at John H. Stroger Jr. Hospital,
Chicago, and China Medical University Hospital, Taichung and National Taiwan University Hospital, Taipei, Taiwan for their cooperation. None of the names listed in the acknowledgement received compensation for their contribution.
References
1 Jobe AH, Bancalari E. Bronchopulmonary dysplasia. Am J Resp. Crit. Care Med 2001; 163:1723-1729.
2 Tyson JE, Wright LL, Oh W, Kennedy KA, Mele L, Ehrenkranz RA, Stoll BJ, Lemons JA, Stevenson DK, Bauer CR, Korones SB, Fanaroff AA. Vitamin A supplementation for extremely-low-birth-weight infants: National Institute of Child Health and Human Development Neonatal Research Network. N Engl J Med 1999; 340:1962-1968.
3 Schmidt B, Roberts RS, Davis P, Doyle LW, Barrington KJ, Ohlsson A, Solimano A, Tin W; Caffeine for Apnea of Prematurity Trial Group. Caffeine therapy for apnea of prematurity. N
Eng J Med 2006; 354:2112-2121.
4 American Academy of Pediatrics, Committee on Fetus and Newborn: Postnatal
corticosteroids to treat or prevent chronic lung disease in preterm infants. Pediatrics 2002; 109:330-338.
5 American Academy of Pediatrics, Committee on Fetus and Newborn: Postnatal
corticosteroids to prevent or treat bronchopulmonary dysplasia. Pediatrics 2010; 126:800-808.
6 Shah SS, Ohlsson A, Halliday HL, Shah VS. Inhaled versus systemic corticosteroids for preventing chronic lung disease in ventilated very low birth weight preterm neonates.
Cochrane Database Syst. Rev. 2012; (5):CD002058.
7 Cole CH, Colton T, Shah BL, Abbasi S, MacKinnon BL, Demissie S, Frantz ID 3rd. Early inhaled glucocorticoid therapy to prevent bronchopulmonary dysplasia. N Eng. J Med 1999; 340:1005-1010.
treatment of chronic lung disease in ventilated very low birth weight preterm infants.
Cochrane Database Syst. Rev. 2012; (5):CD002057.
9 Yeh TF, Lin HC, Chang CH, Wu TS, Su BH, Li TC, Pyati S, Tsai CH. Early intra-tracheal instillation of budesonide using surfactant as a vehicle to prevent chronic lung disease in preterm infants: a pilot study. Pediatrics 2008; 121:e1310-e1318.
10 Newman B. Imaging of medical disease of the newborn lung. Radiol. Clin North Am 1999;37:1049-1065.
11 Chen CM, Huang LT, Wang M, Yeh TF. Surfactant supplemented with budesonide for prevention of bronchopulmonary dysplasia-biophysical and chemical Stability of
surfactant/budesonide mixture. In: The 5th Congress of the European Academy of Paediatric Societies, October 17-21, 2014; Barcelona, Spain.
12 Yeh TF, Raval D, Luken J, Thalji A, Lilien L, Pildes RS. Clinical evaluation of premature infants with patent ductus arteriosus: A scoring system with echocardiogram, acid-base, and blood gas correlations. Crit Care Med 1981; 9:655-657.
13 Shennan AT, Dunn MS, Ohlsson A, Lennox K, Hoskins EM. Abnormal pulmonary outcomes in premature infants: prediction from oxygen requirement in the neonatal period. Pediatrics 1988; 82:527-532.
14 Mercier JC, Hummler H, Durrmeyer X, Sanchez-Luna M, Carnielli V, Field D, Greenough A, Van Overmeire B, Jonsson B, Hallman M, Baldassarre J; EUNO Study Group. Inhaled nitric oxide for prevention of bronchopulmonary dysplasia in premature babies (EUNO): a randomised controlled trial. Lancet 2010; 376:346-354.
15 Stoll BJ, Hansen NI, Bell EF, Shankaran S, Laptook AR, Walsh MC, Hale EC, Newman NS, Schibler K, Carlo WA, Kennedy KA, Poindexter BB, Finer NN, Ehrenkranz RA, Duara S,
Sánchez PJ, O'Shea TM, Goldberg RN, Van Meurs KP, Faix RG, Phelps DL, Frantz ID 3rd, Watterberg KL, Saha S, Das A, Higgins RD; Eunice Kennedy Shriver National Institute of Child Health and Human Development Neonatal Research Network. Neonatal outcomes of extremely preterm infants from the NICHD Neonatal Research Network. Pediatrics 2010; 126:443-456.
16 Gadhia MM, Cutter GR, Abman SH, Kinsella JP. Effects of early inhaled nitric oxide therapy and vitamin A supplementation on the risk for bronchopulmonary dysplasia in premature newborns with respiratory failure. J Pediatr. 2014; 164:744-748.
17 Wang JY, Yeh TF, Lin YJ, Chen WY, Lin CH. Early postnatal dexamethasone therapy may lessen lung inflammation in premature infants with respiratory distress syndrome on
mechanical ventilation. Pediatr. Pulmonol. 1997; 23:193-197.
18 Hintze JL. Kaysville, Utah, USA: 2008. Power analysis and sample size system (PASS) for windows User's Guide I. NCSS.
19 Liang KY, Zeger SL. Longitudinal data analysis using generalized linear models. Bionietrika 1986;73:13-22. Adamson AW. Introduction Marongoni convection. In: Adamson AW. Physical Chemistry of Surfaces. New York, NY: John Wiley and Sons; 1982:110
20 Adamson AW. Introduction Marangoni convection. In: Adamson AW. Physical Chemistry of Surfaces. New York, NY: John Wiley and Sons; 1982:110
21 Fajardo C, Levin D, Garcia M, Abrams D, Adamson I. Surfactant versus saline as a vehicle for corticosteroid delivery to the lungs of ventilated rabbits. Pediatr Res 1998;43:542-547. 22 Chen CM, Fang CL, Chang CH. Surfactant and corticosteroid effects on lung function in a rat
model of acute lung injury. Crit Care Med 2001;29:2169-5475.
budesonide supplementation in addition to surfactant improves pulmonary outcome in surfactant-depleted newborn piglets. Pediatr Pulmonol 2013;48:151-159.
24 Patole SK, Mohan MS, Jog SM, Muller R, Whitehall JS. Prophylactic intratracheal budesonide in preterm neonates at risk for chronic lung disease (CLD)-a pilot study.
Presented at the Annual Conference of the Perinatal Society of Australia and New Zealand; March 2–3, 2001; Canberra, Australia; No. 1590
25 Lin YJ, Lin HC, Lin CH, Su BH, Yeh TF. Early endotracheal instillation of budesonide (B) for prevention of CLD in preterm infant with RDS-a double blind clinical trial. Ped Res. 2001; 49(4):278A
26 Bassler D., Halliday H. L., Plavka R., Hallman M., Shinwell E. S., Jarreau P. H., Camielli V., Van den Anker J., Schwab M., Poets C. F., The Neonatal European Study of Inhaled steroids (NEUROSIS): An Eu-Funded International Randomized Control trial in Preterm Infants Neonatology 2009 July 7, 97(1):52-55
27 Wiedmann TS, Bhatia R, Wattenberg LW. Drug solubilization in lung surfactant. J Control
Release 2000;65:43-47.
28 Miller-Larsson A, Mattsson H, Hjertberg E, Dahlback M, Tunek A, Brattsand R. Reversible fatty acid conjugation of budesonide. Novel mechanism for prolonged retention of topically applied steroid in airway tissue. Drug Metab. Dispos. 1998; 26:623-630.
29 Yeh TF, Torre JA, Rastogi A, Aryebuno MA, Pildes RS. Early postnatal dexamethasone therapy in premature infants with severe respiratory distress syndrome: a double-blind, controlled study. J Pediatr.1990; 117:273-282.
30 Kuo HT, Lin HC, Tsai CH, Chouc IC, Yeh TF. A follow-up study of preterm infants given budesonide using surfactant as a vehicle to prevent chronic lung disease in preterm infants. J
Pediatr 2010;156:537-541.
31 Hvizdos KM, Jarvis B. Budesonide inhalation suspension: a review of its use in infants, children and adults with inflammatory respiratory disorders. Drugs 2000; 60:1141-1178. 32 Agertoft L, Pedersen S. Effects of long-term treatment with an inhaled corticosteroid on
growth and pulmonary function in asthmatic children. Resp. Med 1994; 88:373-381. 33 Agertoft L, Pedersen S. Effect of long-term treatment with inhaled budesonide on adult
Figure Legends
Figure 1 Patient disposition. VLBW = very low birth weight; IMV = intermittent mandatory ventilation; RDS = respiratory distress syndrome; IVH = intraventricular homorrhage
Figure 2 Comparison of systolic and diastolic blood pressure (BP), serum electrolytes, glucose, body weight (BW), length (L), and head circumference (HC) between the groups during the study. There was no significant difference in any of these variables between the groups.
Figure 3 Changes of blood gases and oxygen index (OI) and mean airway pressure (MAP) status during the study. The mean values, derived from a generalized linear model with generalized estimating equations are presented for each group. Infants in the intervention group had significantly lower FIO2 on day 1 [mean difference (95% confidence interval)] [-6.1 (-4.06 to -3.12), P = 0.04], higher PO2 on day 2, [5.6 (4.26 to 19.4), P = 0.04], lower PCO2 on day 1, [-5.1 1.8 to -4.5), P = 0.01], lower OI on day 1 [-0.07 1.71 to -1.06), P = 0.01] and day 5 [-2.1 (-2.94 to -1.35), P = 0.01], and lower MAP on day 1 [-1.08 (-2.61 to -0.46), P=.002], day 2 [-0.66 (-2.27 to -0.94), P = 0.04], and day 3 [-1.37 (-3.22 to -0.48), P = 0.02]. 0 day in the × axis represents less than 24 hours as all blood samples for blood gases were obtained in each morning before the morning round.
Figure 4 The number and proportion of infant extubated (A) or weaned to room air (B) over time during the study. Kaplan-Meier cumulative incidence plots were generated to show time-to-event for all end points. Infants in the intervention group had a significantly higher chance to be weaned to room air than infants in the control group.
Figure 5 The 18F-budesonide bio-distribution (A) and radioactivity (B) in the Sprague-Dawley rats intra-tracheal injected with surfactant/18F-budesonide (n = 3) or 18F-budesonide alone (n = 3). The 18F-budesonide was distributed more into the peripheral lungs and the accumulated 18
F-budesonide radioactivity was higher in the rats supplemented with S than in the rats without S during the study period. B = 18F-budesonide, BS = surfactant/18F-budesonide.
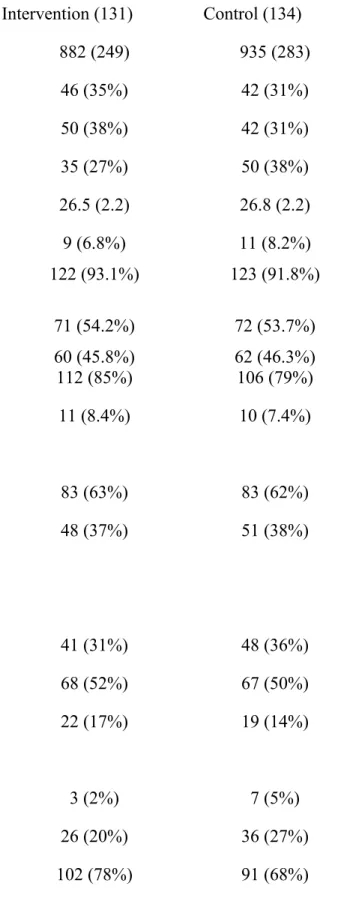
Table 1 Baseline Characteristics
Perinatal Characteristics Intervention (131) Control (134)
Birth weight (g) 882 (249) 935 (283)
500-749 46 (35%) 42 (31%)
750-999 50 (38%) 42 (31%)
1000-1499 35 (27%) 50 (38%)
Gestational age (postmenstrual weeks) 26.5 (2.2) 26.8 (2.2) SGA AGA 9 (6.8%) 122 (93.1%) 11 (8.2%) 123 (91.8%) Gender male female 71 (54.2%) 60 (45.8%) 72 (53.7%) 62 (46.3%) Prenatal steroid 112 (85%) 106 (79%) Chorioamnionitis 11 (8.4%) 10 (7.4%) Mode of delivery Cesarean Section 83 (63%) 83 (62%) Vaginal delivery 48 (37%) 51 (38%) Apgar Score 1 min ≤3 41 (31%) 48 (36%) 4-6 68 (52%) 67 (50%) >6 22 (17%) 19 (14%) 5 min ≤3 3 (2%) 7 (5%) 4-6 26 (20%) 36 (27%) >6 102 (78%) 91 (68%)
Table 1 (continued)
Clinical and Laboratory Characteristics at Time of Entry into Study
Age (hrs) 2.0 (1.5) 1.8 (1.4) IMV 131 134 FIO2 0.61 (0.25) 0.63 (0.26) MAP (cm H2O) 7.1 (4.8) 7.2 (1.5) OI 8.0 (4.3) 8.1 (5.1) PO2 (mm Hg) 70.6 (57.9) 68.5 (43.3) PCO2 (mm Hg) 48.1 (10.5) 49.7 (18.5) pH 7.25 (0.12) 7.24 (0.14) Blood Pressure (mmHg) Systolic 48.1 (11.9) 46.6 (9.2) Diastolic 29.4 (9.6) 27.5 (8.4) Hematocrit (%) 42.4 (6.6) 42.6 (6.7)
IMV=intermittent mandatory ventilation; MAP = mean airway pressure; OI = oxygen index. Data are expressed as mean (SD) or number (%).
SGA and AGA was defined if the births weight less than 10th percentile and between 10th and 90th percentile in intrauterine growth chart, respectively.
Table 2 Mortality and BPD Morbidity Intervention
(131)
Control (134)
Difference (95% CI) RR (95% CI) P
value BPD or Death 55/131 (42%) 89/134 (66%) -0.24 (-0.36 to -0.13) 0.58 (0.44 to 0.77) <0.001 Death 17/131 (13%) 22/134 (16%) -0.03 (-0.12 to 0.05) 0.96 (0.87 to 1.06) 0.54 BPD 38/131 (29%) 67/134 (50%) -0.21 (-0.32 to -0.10) 0.70 (0.58 to 0.86) <0.001 BPD morbidity (NICHD criteria) BPD 57/131 (44%) 88/134 (66%) -0.22 (-0.34 to -0.10) 0.61 (0.46 to 0.80) <0.001 Mild 19/131 (15%) 21/134 (16%) -0.01 (-0.10 to 0.07) 0.99 (0.89 to 1.09) 0.93 Moderate 26/131 (20%) 41/134 (31%) -0.11 (-0.21 to 0.00) 0.87 (0.75 to 1.00) 0.06 Severe 12/131 (9%) 26/134 (19%) -0.10 (-0.19 to -0.02) 0.89 (0.80 to 0.98) 0.03
Table 3 Interleukins concentration (pg/ml/mg urea) in tracheal aspirates and baseline characteristics
Intervention group Control group
(n=18) (n=20) P value Birth weight (g) 809 (196) 886 (232) 0.56 Gestational age (weeks) 26.2 (2.4) 26.3 (1.6) 0.86 FIO2 0.64 (0.19) 0.59 (0.20) 0.57 MAP (cm H2O) 6.9 (0.87) 6.9 (0.99) 0.94 OI 6.7 (3.7) 7.0 (4.0) 0.44 Death 2 (11.1%) 5 (25.0%) 0.41 BPD 6 (33.3%) 11 (55%) 0.21 Death or BPD 8 (44.4%) 16 (80%) 0.042
Interleukins (pg/ml/mg urea) Z value P value
IL-1 12 hours 2.0 (1.4-4.4) 16.5 (6.2-21.0) -2.33 0.02 24 hours 10.7 (1.5-15.0) 24.0 (2.3-53.0) -13.5 0.18 3-5 day 13.5 (9.2-23.0) 61.5 (18.0-86.0) -1.43 0.15 7-8 day 14.2 (7.1-29.0) 17.1 (9.2-26.2) -0.04 0.97 IL-6 12 hours 32.0 (2.1-60.0) 79.0 (65.0-112.0) -2.57 0.01 24 hours 27.0 (7.3-30.0) 27.5 (13.0-47.0) -0.94 0.35 3-5 day 20.0 (15.0-27.0) 44.5 (18.0-53.0) -1.47 0.14 7-8 day 9.0 (3.4-12.0) 7.4 (4.0-10.0) -0.12 0.90 IL-8 12 hours 53.0 (20.0-86.0) 198.0 (56.0-405.0) -2.12 0.03 24 hours 40.0 (21.0-49.0) 152.0 (29.0-540.0) -1.72 0.09 3-5 day 60.0 (48.0-105.0) 422.0 (180.0-580.0) -2.49 0.01 7-8 day 146.0 (86.0-210.0) 785.0 (160.0-1200.0) -2.25 0.02 Data are expressed as mean (SD) of baseline characteristics on admission to study, or median (Q1-Q3) of interleukins.