ARTICLE NO. 0183
Risk Factors for Cervical Intraepithelial Neoplasia in Taiwan
PAIRDONGWANG, M.D., PH.D.,*,1
ANDRUEYS. LIN, M.D., DR.P.H.†
*Taipei Wanhwa District Health Center, Taipei, Taiwan; and †College of Public Health, National Taiwan University, Taipei, Taiwan Received May 15, 1995
reaction techniques have demonstrated high risks of cervical A population-based case – control study was conducted in Tai- cancer associated with human papillomavirus [7–9]. However, wan between July 1991 and June 1994 to evaluate the significance concentration on female sexual activity fails to explain the high between risk factors for cervical intraepithelial neoplasia (CIN) incidence of cervical cancer in Taiwan, since they traditionally among Taiwanese women. Personal interviews were compiled with
have few sex partners. Attention might therefore be directed 288 histologically confirmed CIN who were matched by age to 576
to the importance of a ‘‘husband factor.’’ randomly selected controls with normal cervical smears. Using
The sexual behavior of Taiwanese men and women differs logistic regression models to simultaneously evaluate the effects
from contemporary Western practices. There is a convectional of multiple factors as predictors of CIN, we found that the
strong-double standard for sexual behavior in Taiwan’s population. est risk was associate with HPV infection (OR Å 5.02). Other
While female virginity prior to marriage and fidelity subsequent significant risks included husband’s visiting prostitutes (OR Å
to marriage are highly valued, many husbands frequently visit 2.56), four or more vaginal deliveries (OR Å 2.01), two or more
prostitutes—a practice which is tolerated within society. Given induced abortions (OR Å 1.96), and multiple sex partners (OR Å
1.87). A protective effect was also noted with the use of condoms this pattern of sexual behavior, prostitutes may act as an infec-(OR Å 0.38). These data support the hypothesis that CIN is sexu- tious reservoir, and the husband’s sexual behavior may be a ally transmitted in Taiwan’s population and may have a viral major determinant of risk factors for cervical cancer in wives. etiology. Furthermore the results indicate the important role of The theory is that husband access to prostitutes may explain in the husband’s visiting prostitutes and the nonuse of condoms as part the high incidence of cervical cancer in Taiwan where contributing factors in the high incidence rate for CIN in a
popula-female sexual behavior is generally conservative [10, 11]. tion. q 1996 Academic Press, Inc.
In addition, other factors including the possible role of cigarette smoking [12, 13], oral contraceptive use [14, 15], parity [16, 17], venereal infections other than human
papillo-INTRODUCTION
mavirus (HPV) [18, 19], dietary factors [20], hygienic prac-tices [21], socioeconomic status [22], tumor suppressor gene Although the rate of cervical cancer has declined
signifi-of host [23, 24], and histocompatibility types [1] have been cantly in Western countries during the past three decades, it
suggested as putative causes of cervical cancer. However, remains as one of the most common female forms of cancer
available studies yielded largely contradictory results. in developing countries [1, 2]. In Taiwan, cervical cancer is
To investigate whether the higher incidence of this disease now the leading cancer incidence and the third leading cancer
in Taiwan may be due to risk factors which differ from those death among females, with cumulative incidence and mortality
typically occurring in Western populations, or to effects of rates to age 85 of 4.2 and 1.25%, respectively [3].
a different magnitude for known risk factors in the causation Although there remain many puzzling aspects in the
epide-of cervical intraepithelial neoplasia (CIN), we performed a miology of cervical cancer, its correlation with sexual activity
population-based case – control study in Taiwan during the has been well documented [4, 5]. At least in part, the relation
period 1991 – 1994. This study focused on how promiscuity between cervical cancer to some sexually transmitted and
prob-in husbands, condom use, vagprob-inal deliveries, prob-induced abor-ably infectious agent appears inescapable [6]. Three recent
epi-tions, and HPV infections are related as risk factors to the demiologic studies from different geographical areas, including
development of CIN. Brazil, China, Spain, and Colombia, using polymerase chain
SUBJECTS AND METHODS The Interview and the Questionnaire
1
To whom correspondence and reprint requests should be addressed at
Since 1989, we have been conducting a cervical cancer Wanhwa District Health Center, No. 152, Tung-Yuan Street, Taipei,
of this study have been reported elsewhere [25]. Briefly, 586). Reasons for nonparticipation were refusal (three cases, seven controls) and inability to locate (two cases, three con-questionnaires were administered to all participants during
a period from 1991 to 1994 at 12 district health centers by trols).
Two hundred and eighty-eight women with histologically standardly trained public health nurses. The mean interview
time was 20 min. Information was obtained concerning confirmed diagnosis of cervical intraepithelial neoplasia inci-dent cases were studied. Among intraneoplasia, 45.9% were health issues related to the etiology of CIN, including
ques-tions related to sociodemographic data, contraceptive and classified as CIN 1, (mild dysplasia), 41.2% as CIN 2 (mod-erate dysplasia), and 12.9% CIN 3 (severe dysplasia or carci-reproductive history, personal habits (tobacco, hygiene),
sex-ual behavior (women and their husband), as well as Pap noma in situ).
Of the total number of 1,030,461 women in the 12 dis-smear history. Medical records were examined to validate
responses about the self-reported frequency of Pap smear tricts, 39,194 were screened during the study period. Two controls per case were drawn at random from a list of patients screening at 12 health centers. With regard to sexual
behav-ior, women were asked their age at the time of their first who had normal cervical smears at 12 health centers. Con-trols were matched to CIN cases within a 5-year age group sexual intercourse and the number of sex partners they had
had. One of the interviewers (Shu-Lian Kao), a well-trained and within the same month as when the case was diagnosed. Women who had undergone total hysterectomy were not nurse who was unaware of the case or control status,
inter-viewed the husbands of all subjects by telephone and asked included. A total of 576 control subjects were included in the study.
whether they had visited a prostitute, and, if so, how often, and whether they had been circumcised. She had the general
impression that husbands actually were embarrassed to give Studies on Microorganisms answers, since the theme of visiting prostitutes and perhaps
even circumcision is very private for some husbands. In addition to screening for cervical cancer, all smears were examined for the presence of infections and organisms. These included Candida (defined as hyphae identified in the Definition of Cases and Controls
stained smear), trichomonas (defined as an intact organism of appropriate size and configuration with an identifiable Patients were recruited to participate in the educational
and cervical cancer screening programs at the 12 public characteristic nucleus), and specific morphologic changes caused by such agents as human papillomavirus (defined as health centers during the study period. In this program the
importance of routine cervical cancer screening was ex- the presence of either koilocytosis or any two of the follow-ing features: nuclear wrinkfollow-ing, multinucleation, dysker-plained to the patient, and the patient then received a pelvic
examination and a Pap smear was administered with a plastic atosis, or the presence of epithelial spikes). Since vaginal cytologic screening is a routine procedure in Taiwan, the exocervic brush by the program physicians. Specimens were
mixed on one side of a glass slide and fixed with a spray prevalence of koilocytosis can be estimated. When polymer-ase chain reaction (PCR) tests were repeated, the prevalence fixative. Upon arriving at the cytopathology laboratory at
the Taipei pathological center, the smears were stained by of HPV DNA was higher than that of koilocytosis from stained smears in similar populations. However, a stained the standard Papanicolaou method. Smears were classified
using standard criteria as normal, benign atypia, or dysplastic smear is easily accomplished and can be a valuable by-product of cytologic screening for cervical cancer.
atypia. If the results of the Pap smear test were abnormal (dysplastic atypia), the women were referred to municipal
hospitals for a coloposcopically directed biopsy. All women Statistical Methods for whom biopsy was recommended were tracked by
pro-gram nurses to ensure that the biopsy was actually con- Initially, to estimate the risk of CIN with associated se-lected variables, the effects of individual factors and the ducted.
A total number of 386 cases were diagnosed as having presence of a trend for ordered variables were assessed by Mantel – Haenszel extension methods and the odds ratio, CIN at the 12 district health centers during the study period.
The eligibility criterion is the case with histologically con- their 95% confidence interval, and the x2
for trends were calculated. Subsequently, however, in our final prediction firmed diagnosis of CIN. Ninty-three patients were excluded
by the criterion. Incident cases were included in the study; model variables were selected because of biological plausi-bility or because they were statistically significant in univari-however, they did not include the interval (time between
two screenings) cases. ate analyses. A conditional logistic regression model was
then used to adjust for potential confounding variables, de-Approximately 98.3% of eligible cases (288/293) were
interviewed and included in these analyses. Participation by riving maximum likelihood estimates of relative risk and 95% confidence interval.
TABLE 1
Risk of Cervical Intraepithelial Neoplasia in Relation to Selected Sociodemographic Characteristics among Taiwanese Women, 1991 – 1994
Characteristic Cases (nÅ288) Controls (nÅ576) Odds ratio 95% CI
Education ú12 52 122 1.0 9 – 12 104 235 1.04 0.67 – 2.0 õ9 132 219 1.41 0.79 – 2.65 Trend test, PÅ0.11 Ethnicity Taiwanese 243 485 1.0 Mainlander 45 91 0.99 0.62 – 3.45
Frequency of Pap smear
Once a year 26 51 1.0
Once every 2 years 65 136 0.94 0.60 – 2.57
Once every 3 to 5 years 66 133 0.97 0.62 – 2.60
None 131 256 1.0 0.67 – 2.31 Trend test, PÅ0.47 Cigarette smoking Never 277 556 1.0 Ever 11 20 1.10 0.72 – 6.91 Husband circumcision Yes 84 208 1.0 No 204 368 1.37 1.0 – 2.78
Genital washes after coitus
Frequently or always 114 261 1.0
Never or rarely 174 315 1.31 1.0 – 2.80
RESULTS visiting prostitutes was statistically significant (Põ 0.01). In addition, a significant trend of increased risk was observed in wives with numerous of sex partners. Those with four Comparative analyses of characteristics in the case and
or more sex partners represented a 1.94-fold excess risk control population were performed to identify risk factors
compared with women reporting only one partner. However, for the presence of CIN. There were no missing data in the
the younger a women starts having sexual relations the results (Tables 1 – 6). Sociodemographic relationships with
greater her risk of CIN, with those õ20 years old at first risk factors using univariate analysis are shown in Table 1.
coitus showing a significant 82% increase in risk. A trend of increasing risk with less education was observed,
The risks of CIN associated with selected reproductive although it was not statistically significant. Ethnicity was
factors are presented in Table 3. A significant trend in risk not found to be related to risk. The absence of regular prior
was observed in those reporting 2 to 3 vaginal deliveries Pap smear did not appear to increase risk. Among subjects,
having a ORÅ1.3, while$4 vaginal deliveries resulted in
a large number of women reported never having had a Pap
a ORÅ2.0 (for trend, Põ 0.01). In addition, the number smear, which was not associated with an elevation in risk.
of induced abortions was also related to increased risk (for No clear relationship was observed for cigarette smoking,
trend, Põ0.01). Women reporting induced abortions more although very few women in this population reported
smok-than two times had a 1.98-fold risk compared to those who ing. However, both the husband’s circumcision and genital
had reported never having an induced abortion. Other repro-washing following coitus were associated with reduced risks,
ductive measures investigated including stillbirths and spon-although the effects were only marginally significant.
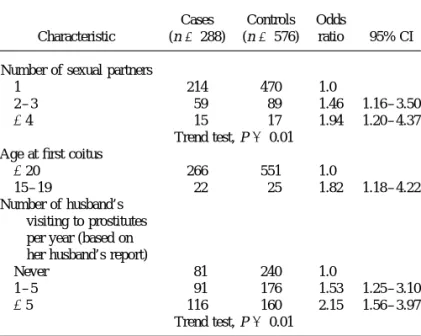
taneous abortions were not significantly identified as risks. Table 2 presents information on CIN risks associated with
Because sexual activity represents a strong risk factor for selected sexual behavior. The husband’s intercourse with
CIN, it is possible that certain methods of contraception may prostitutes was found to be a major risk factor for CIN in
afford some degree of protection against the disease. As this study. Those who visited prostitutesú5 times per year
Table 4 shows, a protective trend was observed for the dura-represented a 2.5-fold excess risk compared with those who
tion of condom use. Those using condoms for #5 years
had reported never visiting prostitutes while those visiting
showed a significant 59% reduction in risk (ORÅ0.41) and prostitutes 1 – 5 times per year yielded a 53% increased risk.
TABLE 2 was associated with a diminished risk (ORÅ0.38). Notably, Risk of Cervical Intraepithelial Neoplasia in Relation to Indicators although earlier age at first coitus was an important predictor of Sexual Activity among Taiwanese Women, 1991–1994 of risk in univariate analysis, it was not statistically signifi-cant after adjustment for other risk factors in this regression Cases Controls Odds
model. In addition, no measure of oral contraceptive use was Characteristic (nÅ288) (nÅ576) ratio 95% CI
found to be related to the risk of CIN after simultaneous adjustment for potentially confounding factors.
Number of sexual partners
1 214 470 1.0 It is believed that most CIN 1 are caused by HPV infection
2 – 3 59 89 1.46 1.16 – 3.50 and that an epidemiological study on the HPV infection of
$4 15 17 1.94 1.20 – 4.37
CIN should exclude women with CIN 1. We also analyzed Trend test, Põ0.01
the data including women with CIN 2 and CIN 3 (Table 6). Age at first coitus
The HPV infection was associated a 4.38-fold elevation in
$20 266 551 1.0
15 – 19 22 25 1.82 1.18 – 4.22 the odds ratio of CIN 2,3, but this increase was weaker than
Number of husband’s that seen for CIN analysis (ORÅ5.02). In contrast, observed
visiting to prostitutes
associations with other risk factors (sex partner, age at first per year (based on
coitus, husband’s ever visiting prostitutes, etc.) changed little her husband’s report)
for CIN 2,3.
Never 81 240 1.0
1 – 5 91 176 1.53 1.25 – 3.10
$5 116 160 2.15 1.56 – 3.97 DISCUSSION
Trend test, Põ0.01
This study utilized case – control methodology to investi-gate risk factors for the development of CIN in a population of cytologically screened women. Cases had histopathologi-the years of oral contraceptive use were related to increased
cally confirmed CIN and controls had normal cervical cytol-risk, with those having used the oral contraceptive for ú5
ogies. HPV infection was diagnosed using cytomorphology. years having a 1.46-fold elevation in risk compared with
Many risk factors which have been consistently linked with those who had never been users, although no significant
invasive cervical cancer were found to be associated with trend in risk was observed. No consistently increased risk
CIN in our study. As in several previous studies, CIN in-was observed in women who either used intrauterine devices
creased directly with number of sex partners [16, 26, 27], or had had tubal ligation.
The relationship between various infections and CIN was
also investigated (Table 5). A strong risk factor was found TABLE 3
for the HPV infection. Compared with women without HPV Risk of Cervical Intraepithelial Neoplasia in Relation to Selected infection, the odds ratio of CIN was 9.10 among those with Reproductive Factors among Taiwanese Women, 1991–1994 HPV infection. In contrast, for CIN 2,3, the HPV infection
Cases Controls associated with elevation in odds ratio (ORÅ6.26) tended
Characteristic (nÅ288) (nÅ576) Odds ratio 95% CI to be slightly weaker than that seen with CIN. In addition,
for CIN, neither candidial nor trichomonal infection was
Number of vaginal significantly related to risk. Odds ratio for CIN 2,3 varied deliveries
little with candidial or trichomonal infection and remained 0 – 1 31 92 1.0
2 – 3 128 293 1.30 1.01 – 2.96
close to the odds ratio of those who had never been infected.
$4 129 191 2.0 1.16 – 3.27
To further evaluate the relative importance of variables
Trend test, Põ0.01 found to be associated with CIN, we performed multivariate
Number of stillbirths
logistic regression analysis (Table 6). To determine which 0 275 551 1.0
factors were independently associated with likelihood of $1 13 25 1.04 0.71 – 4.76
Number of spontaneous CIN, we created models incorporating number of sex
part-abortions ners, age at first coitus, husband’s frequency of visiting
pros-0 254 506 1.0
titutes, HPV infection, oral contraceptive use, condom use,
$1 34 70 0.97 0.70 – 3.57
vaginal deliveries$4, and induced abortion$2. Using this
Number of induced model, we found HPV infection (OR Å 5.02), husband’s abortions
0 138 356 1.0
frequency of visiting prostitutes (ORÅ2.56), vaginal
deliv-1 91 143 1.65 1.23 – 3.14
eries (ORÅ2.01), induced abortions$2 (ORÅ1.96), and
$2 59 77 1.98 1.45 – 3.72
multiple sex partners (ORÅ1.87) as factors associated with
Trend test, Põ0.01 a significantly elevated risk of CIN, while use of condoms
TABLE 4
Risk of Cervical Intraepithelial Neoplasia in Relation to Selected Contraceptive Methods among Taiwanese Women, 1991 – 1994
Characteristic Cases (nÅ288) Controls (nÅ576) Odds ratio 95% CI
Years of use of oral contraceptive
Nonuser 258 526 1.0
#5 20 36 1.13 0.83 – 3.87
ú5 10 14 1.46 0.95 – 4.42
Trend test, PÅ0.07 Years of use of condoms
Nonuser 264 469 1.0
$5 14 60 0.41 0.16 – 0.98
ú5 10 47 0.38 0.12 – 0.98
Trend test, PÅ0.01 Years of use of intrauterine device
Nonuser 132 266 1.0
$5 60 115 1.05 0.60 – 2.95
ú5 96 195 0.99 0.62 – 2.74
Trend test, PÅ0.53 Years of tubal ligation
No 270 545 1.0
$10 5 10 1.0 0.47 – 4.89
ú10 13 21 1.25 0.63 – 4.57
Trend test, PÅ0.75
supporting a hypothesized infectious etiology. However, much more importance in the Taiwanese population than in Western cultures. It is of interest to note that age at first Taiwan has a double standard of sexual morality resulting
in a prevalence in prostitution. A woman’s risk of CIN will coitus does not persist as a significant risk factor of CIN in the multiple regression model, although the relationship was depend less on her own behavior than on that of her husband.
In agreement with a British study by Buckley et al. [28], observed in univariate analysis. While this finding fails to support Coppleson’s hypotheses that adolescence is a period we noted that among subjects in our study there was strong
correlation between husband’s visiting prostitutes and CIN, when the cervex is most vulnerable to the effects of sexual behavior [31], it is in agreement with the results of the study with 71.9% of husbands of cases reporting having visited
prostitutes compared with 58.3% of husbands of controls of CIN by Harris et al. [32]. Nevertheless, it is in contrast to some case – control studies of invasive cancer which have reporting having visited prostitutes. These figures are
rela-tively high, compared to a U.S. study of 6.7% [29] and a shown independent effects after adjustment for other poten-tial confounding factors [33, 34]. It is possible that exposure Denmark study of 7.7% [30]. Therefore, the sexual
back-ground of the husband in the genesis of CIN may be of of the cervix at a younger age is more predictive of invasive
TABLE 5
Risk of Cervical Intraepithelial Neoplasia in Relation to Selected Infection among Taiwanese Women, 1991 – 1994
CIN CIN 2, 3
No. of No. of No. of
Characteristic cases Odds ratio 95% CI cases Odds ratio 95% CI controls
HPV infection Negative 217 1.0 120 1.0 556 Positive 71 9.10 2.67 – 15.73 27 6.26 1.98 – 13.60 20 Candidial infection Negative 280 1.0 142 1.0 557 Positive 8 0.84 0.51 – 5.64 5 1.03 0.60 – 5.95 19 Trichomonal infection Negative 282 1.0 144 1.0 565 Positive 6 1.09 0.53 – 5.73 3 1.07 0.52 – 5.70 11
TABLE 6
Adjusted Odds Ratio for Cervical Intraepithelial Neoplasia According to Various Risk Factors among Taiwanese Women, 1991 – 1994
CIN CIN 2, 3
Risk factor Adjusted odds ratio 95% CI Adjusted odds ratio 95% CI
ú1 sex partner 1.87 1.13 – 2.46 2.01 1.26 – 2.57
First coitusõ20 years 1.08 0.77 – 1.86 1.09 0.80 – 1.95
Husband’s ever visiting prostitutes 2.56 1.68 – 3.82 2.33 1.59 – 3.74
HPV infection 5.02 2.54 – 8.01 4.38 2.26 – 7.80
Oral contraceptive use 1.20 0.81 – 4.50 1.31 0.93 – 4.87
Condom use 0.38 0.16 – 0.95 0.34 0.14 – 0.91
$4 vaginal deliveries 2.01 1.50 – 3.84 1.93 1.42 – 3.69
$2 induced abortions 1.96 1.45 – 3.77 2.05 1.58 – 3.94
cervical cancer, and this idea is supported by Terris et al. use was found to be unrelated to risk of CIN. Simultaneous adjustment for potentially confounding factors changed the [35], who addressed the progression of invasive cancer
in-volving a period of increased vulnerability of the cervix at risk estimates very little, strengthening the impression that CIN was unrelated to OC use. When other contraceptive earlier ages.
Slattery et al. [36] postulated that the regular use of con- measures were analyzed, we were unable to demonstrate either a protective or adverse effect for the use of intrauterine doms may protect the cervix from opportunistic transmission
by an infectious agent. Consistent with this hypothesis and devices or tubal ligation, as reported by Williams et al. [16]. Increasing evidence suggests that HPV plays a major role with findings from other studies [37, 38], we found condom
use to be associated with a reduction in risk in which pro- in the etiology of cervical cancer [7 – 9]. Our findings, as previously reported for invasive cancer [41], found HPV longed use correlated with risk reduction. It is clear that
high-risk husband behavior is characterized by intercourse infection to be the strongest risk factor associated with CIN, with aú5-fold excess risk in women with HPV infection with prostitutes without condoms who constitute a reservoir
of infection. If he contracts viral agents he may subsequently compared to those without HPV infection, supporting a more primary etiologic role for HPV in CIN. In the present study, pass the agents to his wife. This may account, at least in
part, for the high risk of CIN in their wives. However, only husbands of cases were more likely to have visited prosti-tutes compared to the husbands of controls. These data sup-8.3% of cases and 18.5% of controls in the present study
reported ever having used a condom during any part of their port previous studies which have addressed the existence of an infectious agent and possibly reflect viral transmission sexually active period compared with some 40% of the
gen-eral population in Denmark [30]. Therefore, it should be from the husbands to their wives [42]. In addition, our previ-ous study of contraceptive use among Taiwanese women useful for public health workers to emphasize that, in
addi-tion to birth control and reducing sexually transmitted dis- showed that 19% of women had never used any contracep-tion [43]. This figure is relatively high compared to those eases (including AIDS), frequent condom use may help to
protect women against cervical neoplasia. in Denmark (3.5%) [30]. In all probability some difference may be explained by a higher prevalence of infertility caused The causal role of oral contraceptive in CIN, however,
remains more equivocal [39]. Since the use of oral contracep- by multiple genital infections in this population, in line with the high-incidence area of cervical cancer (Taiwan) con-tives is highly correlated with number of sexual partners and
age at first intercourse, residual confounding was likely in taining a higher proportion of women who have never used contraception [30].
many previous studies [39]. Recently, a metaanalysis based
on the pooled statistical analysis of 21 studies resulted in a When the relation of infection with HPV to occurrence of CIN was assessed from all Pap smears, we observed that slightly increased risk for ever users compared to nonusers,
particularly among long-term users [40]. In contrast to this the presence of HPV infection was related to an increased adjusted odds ratio of CIN (OR Å 5.02, 95% CIÅ 2.54 – report, however, Coker et al. showed a protective effect for
OC use and high-grade dysplasia in North Carolina women, 8.01) but to a weaker increase in adjusted odds ratio of CIN 2,3 (OR Å 4.38, 95% CI Å 2.26 – 7.80). At present, it is although the relationship was not statistically significant
after adjustment for multiple factors [13]. Some studies have believed that the virus may infect an epithelial cell and be incorporated into the DNA, which then produces viral pro-found a positive association between OC and cervical cancer
dyskeratosis, multinucleation, nuclear wrinking, and/or epi- similar to those of the other studies on the etiology of inva-sive cancer [35]. Thus, we suggest that CIN and invainva-sive thelial spikes. If the cellular atypic condition progresses with
the development of the morphologic changes of dysplasia, cancer should be considered to be stages in a continuum of one single disease.
the characteristics of the koilocyte are lost. Thus,
koilo-cytosis is found more frequently in CIN 1 with CIN 2 and In summary, the incidence of cervical cancer, as of any other sexually transmitted diseases, can be expected to be CIN 3.
Many earlier studies failed to document an association highest in Taiwan, where many men, not using condoms, have intercourse with a small number of prostitutes who between reproductive factors and invasive cancer risk [44,
45]. However, more recent studies among Hispanic women constitute a reservoir of infection. It is clear that ‘‘common source transmission from prostitutes’’ in Taiwanese popula-in the United States and popula-in Latpopula-in America [46, 47], popula-in which
multiple births are more common, indicate that the number tion differs in transmission mode from ‘‘propagate transmis-sion from extramarital sex partners’’ in Western populations. of births has an independent and relevant role in invasive
disease. We observed a linear relationship between CIN risk This theory may explain, at least in part, a high incidence of cervical cancer in Taiwan in which females have had few and number of vaginal deliveries, with women reporting four
or more vaginal deliveries being at a twofold excess risk sex partners. Surprisingly, however, we found some 58% of husbands reported having visited prostitutes, but only 8.3% compared with women with one or no vaginal deliveries,
even when adjusting for potential confounding factors. of cases and 18.5% of controls reported ever having used a condom during sexual intercourse. From our data, we also Hypotheses related to the development of CIN resulting from
trauma of the cervix during childbirth were supported by estimated some 60% of the CIN in women can be attributed to the nonuse of a condom in this population. There is no our data, as we observed a relationship between the number
of vaginal deliveries and CIN. From a mechanistic perspec- question that unsafe prostitution without condom use has been a prominent epidemiological feature of cervical neopla-tive, in support of this hypothesis was the finding in our study
that the number of induced abortions (including mechanical sia in Taiwan. process of dilatation and curretage) was related to risk. In
contrast, spontaneous abortion and stillbirth did not exhibit ACKNOWLEDGMENTS
a similar association with CIN.
The authors thank all the cytotechnicians involved in this study, 16 public Most published studies which have examined the role of
health nurses for their interview, and Professor Yuh Y. Pan for computer socioeconomic indicators in cervical neoplasm have
con-programming. cluded that educational status is also a risk factor for invasive
disease [48]. In contrast to these reports, however, we found
REFERENCES
that educational status did not affect CIN risk, as reported by Harris et al. [32] and Jones et al. [22].
1. Ponten, J., Adami, H. O., Bergstrom, R., Dillner, J., Friberg, L. G., Although Winkelstin found that 15 of 18 studies since
Gustafsson, L., Miller, A. B., Parkin, D. M., and Trichopoulos, D. 1966 have noted an association of smoking with the in- Strategies for global control of cervical cancer, Int. J. Cancer 60, 1 – creased risk of invasive disease [49], the present study did 26 (1995).
not find a similar association with CIN. It is possible that 2. Parkin, D. M., Muir, C. S., Whelan, S. L., Gao, Y. T., Ferlary, J., and Powell, J. Cancer incidence in five continents, International Agency too few study subjects (11 cases and 20 controls) were
smok-for Research on Cancer, Lyon, Vol. VI, IARC scientific publication ing to allow a meaningful analysis of effects of smoking as
No. 120 (1992). a risk factor for CIN (because only a 3.2% prevalence of
3. Department of Health, Executive Yuan. Cancer registry annual report Taiwanese women ever smoked cigarettes), indicating a
cig-in Taiwan area, 1986. Department of Health, Executive Yuan, Taipei arette smoking-mediated effect on one of the latter stages (1991).
of the process of carcinogenesis. 4. Brisson, J., Morin, C., Fortier, M., Roy, M., Bouchard, C., Leclerc, J., CIN is usually asymptomatic and is discovered only as a Christen, A., Guimont, C., Penault, F., and Meisels, A. Risk factors result of Pap smear screening. Screening tends to increase for cervical intraepithelial neoplasia: Differences between low- and
high-grade lesions, Am. J. Epidemiol. 140, 700 – 710 (1994). diagnosis of CIN while reducing the incidence of invasive
5. Armstrong, B., Munoz, N., and Bosch, F. X. Epidemiology of cancer disease. Thus, frequency of Pap smear exerted positive
con-of the cervix, in Gynecology Oncology (M. Coppleson, M. J. Monaghan, founding on CIN risk, while exerting negative confounding
C. P. Morrow, and M. I. N. Tattershall, Eds.), Churchill Livingstone, on the risk of invasive cancer. Although La Vecchia found Edinburgh, Vol. 1, 2nd ed., pp. 11 – 29 (1992).
that longer Pap screening intervals were associated with
in-6. Howley, P. M. Role of the human papillomaviruses in human cancer, vasive disease [50], our data were not consistent with this Cancer Res. 51(Suppl.), 5019 – 5022 (1991).
Pap smear effect, partly because of only a 14% coverage 7. Eluf-Neto, J., Booth, M., Munoz, N., Bosch, F. X., Melier, rate of Pap smear among Taiwanese women. C. J. L. M., and Walboomers, J. M. M. Human papillomavirus and invasive cervical cancer in Brazil, Br. J. Cancer 69, 114 – 119 (1994). The risk factors identified for CIN in our study are quite
8. Peng, H., Liu, S., Mann, V., Rohan, T., and Rawls, W. Human papillo- integration in adenocarcinoma of the uterine cervix and uterine isthmus, Int. J. Cancer 59, 601 – 606 (1994).
mavirus types 16 and 33, herpes simplex virus type 2 and other risk
factors for cervical cancer in Sichuan Province, China, Int. J. Cancer 25. Wang, P. D., and Lin, R. S. Induced abortion in Taiwan, J. R. Soc.
47, 711 – 716 (1991). Health 115, 100 – 108 (1996).
9. Bosch, F. X., Munoz, N., De Sanjose, S., Navarro, C., Moreo, P., 26. La Vecchia, C., Franceschi, S., Decarii, A., Fasoli, M., Gentile, A., Ascunce, N., Gonzalez, L. C., Tafur, L., Ghi, M., Larranaga, I., Viladiu, Parazzini, F., and Regallo, M. Sexual factors, venereal diseases, and P., Danief, R. W., Alonso De Ruiz, P., Aristizabal, N., Saniamaria, M., the risk of intraepithelial and invasive cervical neoplasia, Cancer 58, Guerrero, E., and Shak, K. V. Human papillomavirus and CIN. III. A 935 – 941 (1986).
case – control study in Spain and Colombia, Cancer Epidemiol.
Bio-27. Brock, K., Berry, G., Brinton, L., Kerr, C., Maclennan, R., Mock, R., markers Prevent. 2, 405 – 422 (1993).
and Shearman, R. Sexual, reproductive and contraceptive risk factors 10. Skegg, D. C. G., Corwin, P. A., Paul, C., et al. Importance of the male for carcinoma in situ of the uterine cervix in Sydney, Med. J. Aust.
factor in cancer of the cervix, Lancet 2, 581 – 583 (1982). 150, 125 – 130 (1989).
11. Kjaer, S. K., De Villiers, E. M., Dahl, C., et al. Case – control study of 28. Buckley, J. D., Harris, R. W. C., Doll, R., Vessey, M. P., and Williams, risk factors for cervical neoplasia in Denmark. I. Role of the ‘‘male P. T. Case – control study of the husbands of women with dysplasia or factor’’ in women with one lifetime sexual partner, Int. J. Cancer 48, carcinoma of the cervix uteri, Lancet 2, 1010 – 1014 (1981).
39 – 44 (1991). 29. Tanfer, K. Sex and disease, Sex. Transmitted Dis. 21(Suppl.), s65 – s83 12. Phillips, A. N., and Smith, G. D. Cigarette smoking as a potential cause (1994).
of cervical cancer: Has confounding been controlled? Int. J. Epidemiol. 30. Kjaer, S. K., Teisen, C., Haugaard, B. J., et al. Risk factors for cervical
23, 42 – 49 (1994). cancer in Greenland and Denmark: A population-based cross-sectional
13. Coker, A. K., Rosenberg, A. J., McCann, M. F., and Hulka, B. S. study, Int. J. Cancer 44, 40 – 47 (1989).
Active and passive cigarette smoke exposure and cervical intraepithelial 31. Coppleson, M., Ried, B., and Pixley, E., Preclinical Carcinoma of the neoplasia, Prevention 1, 349 – 356 (1992). Cervix Uteri, Its Nature, Origin, and Management, Pergamon Press, 14. Becker, T. M., Wheeler, C. M., Mcgough, N. S., Stidley, C. A., Par- New York (1967).
menter, C. A., Dorin, M. H., and Jordan, S. W. Contraceptive and 32. Harris, R. W. C., Brinton, L. A., Cowdell, R. H., Skegg, D. C. G., reproductive risks for cervical dysplasia in southwestern Hispanic and Smith, P. G., Vessey, M. P., and Doll, R. Characteristics of women non-Hispanic white women, Int. J. Epidemiol. 3, 913 – 930 (1994). with dysplasia or carcinoma in situ of the cervix uteri, Br. J. Cancer 15. Parazzini, F., Vecchia, C. L., Negri, E., Fedele, L., Franceschi, S., and 42, 359 – 369 (1980).
Gallotta, L. Risk factors for cervical intraepithelial neoplasia, Cancer 33. Clarke, E. A., Hatcher, J., Mckeown-Eyssen, G. E., and Lickrish,
69, 2276 – 2282 (1992). G. M. Cervical dysplasia: Association with sexual behavior, smoking,
and oral contraceptives? Am. J. Obstet. Gynecol. 515, 612 – 616 (1985). 16. Williams, M. A., Kenya, P., Mati, J. K. G., and Thomas, D. B. Risk
factors for invasive cervical cancer in Kenyan women, Int. J. Epidemiol. 34. Brinton, L. A., Hamman, R. F., Huggins, G. R., Lehman, H. F., Levine,
5, 906 – 912 (1994). R. S., Mallin, K., and Fraumeni, J. F. Sexual and reproductive risk
factors for invasive squamous cell cervical cancer, J. Natl. Cancer Inst. 17. Mukherjee, B. N., Sengupta, S., Chaudhuri, S., Biswas, L. N., and
79, 23 – 30 (1987). Maiti, P. A case – control study of reproductive risk factors associated
with cervical cancer, Int. J. Cancer 59, 476 – 482 (1994). 35. Terris, M., Wilson, F., and Nelson, J. H. Comparative epidemiology of invasive carcinoma of the cervix, carcinoma in situ, and cervical 18. Lorincz, A. T., Reid, R., Jenson, A. B., Greenberg, M. D., Lancaster,
dysplasia, Am. J. Epidemiol. 112, 253 – 257 (1980). W., and Kurman, R. J. Human papillomavirus infection of the cervix:
Relative risk associations of 15 common anogenital types, Obstet. Gy- 36. Slattery, M. L., Overall, J. C., Abbott, T. M., French, T. K., Robinson, necol. 79, 328 – 337 (1992). L. M., and Gardner, J. Sexual activity, contraception, genital infections, and cervical cancer: Support for a sexually transmitted disease hypothe-19. Zhang, Z. F., and Begg, C. B. Is trichomonas vaginalis a cause of
sis, Am. J. Epidemiol. 130, 248 – 258 (1989). cervical neoplasia? Results from a combined analysis of 24 studies,
Int. J. Epidemiol. 4, 682 – 690 (1994). 37. Peters, R. K., Thomas, D., Hagan, D. G., Mack, T. M., and Henderson, B. E. Risk factors for invasive cervical cancer among Latins and non-20. Guo, W. D., Hsing, A. W., Li, J. Y., Chen, J. S., Chow, W. H., and
Latins in Los Angeles County, J. Natl. Cancer Inst. 77, 1063 – 1077 Blot, W. J. Correlation of cervical cancer mortality with reproductive
(1986). and dietary factors and serum markers in China, Int. J. Epidemiol. 6,
1127 – 1132 (1994). 38. Fasal, E., Simmons, M. E., and Kampert, J. B. Factors associated with high and low risk of cervical neoplasia, J. Natl. Cancer Inst. 66, 631 – 21. Zhang, Z. F., Parkin, D. M., Yu, S. Z., Esteve, J., and Yang, X. Z.
636 (1981). Risk factors for cancer of the cervix in a rural Chinese population, Int.
J. Cancer 43, 762 – 767 (1989). 39. Piper, J. M. Oral contraceptives and cervical cancer, Gynecol. Oncol. 22, 1 – 14 (1985).
22. Jones, C. J., Brinton, L. A., Hamman, R. F., Storley, P. D., Lehman,
H. F., Levine, R. S., and Mallin, K. Risk factors for in situ cervical 40. Francechi, S., La Vecchia, C., and Talamini, R., Oral contraceptives cancer: Results from a case – control study, Cancer Res. 50, 3657 – 3662 and cervical neoplasia: Pooled information from retrospective and
pro-(1990). spective epidemiological studies, Tumori 72, 21 – 30 (1986).
23. Busby-Earle, R. H. C., Steel, C. M., Williams, A. R. W., Cohen, B., 41. Azocar, J., Abad, S. M. J., Acosta, H., Hernandez, R., Gallegos, M., and Bird, C. C. p53 mutations in cervical carcinogenesis — Low fre- Pifano, E., Blanck, R., and Kramar, A. Prevalence of cervical dysplasia quency and lack of correlation with human papillomavirus status, Br. and HPV infection according to sexual behavior, Int. J. Cancer 45, J. Cancer 69, 732 – 737 (1994). 622 – 625 (1990).
42. Peto, R., and Zur Hausen, H. Viral Etiology of Cervical Cancer, Cold 24. Jiko, K., Jsuda, H., Sato, S., and Hirohashi, S. Pathogenetic significance
43. Wang, P. D. Prevalence of use of contraceptive methods for women R. C., Gaitan, E., and Tenorio, F. Screening for cervical cancer in Latin America: A case – control study, Int. J. Epidemiol. 21, 1050 – in Taipei area, in preparation (1996).
1056 (1992). 44. Rotkin, I. D. A comparison review of key epidemiological studies in
cervical cancer related to current searches for transmissible agents, 48. Brinton, L. A., and Fraumeni, J. F. Epidemiology of uterine cervical Cancer Res. 33, 1353 – 1367 (1973). cancer, J. Chronic Dis. Epidemiol. 39, 1051 – 1065 (1986).
45. Lombard, H. L., and Potter, E. A. Epidemiological aspects of cancer 49. Winkelstein, W. Cigarette smoking and cancer of the uterine cervix, of the cervix, Cancer 3, 960 – 968 (1950). Banbury Rep. 23, 329 – 341 (1986).
46. Brinton, L. A., Reeves, W. C., Brenes, M. M., et al. Parity as a risk 50. La Vecchia, C., Decarli, A., Gentile, A., Franceschi, S., Fasoli, M., factor for cervical cancer, Am. J. Epidemiol. 130, 486 – 496 (1989). and Tognoni, G. ‘‘Pap’’ smear and the risk of cervical neoplasia: Quan-titative estimates from a case – control study, Lancet 2, 779 – 782 (1984). 47. Herrero, R., Brinton, L. A., Reeves, W. C., Brenes, M. M., De Brinton,