Original Articles
Clonal Dissemination of Invasive and Colonizing Clonal complex 1 of Serotype VI Group B Streptococcus in Central Taiwan
Hsiao-Chuan Lin,a,b,c Chao-Jung Chen,d,eKai-Hung Chiang,f Ting-Yu Yen,cCheng-Mao Ho,g Kao-Pin Hwang,b,c Bai-Horng Su,b,h Hung-Chih Lin,h,i Tsai-Chung Li,j,k Jang-Jih Lu,l,m,n#
aDepartment of Public Health, College of Public Health, China Medical University, Taichung, Taiwan
bCollege of Medicine, China Medical University, Taichung, Taiwan
cDepartment of Infectious Diseases, Children’s Hospital, China Medical University Hospital, China Medical University, Taichung, Taiwan
dGraduate Institute of Integrated Medicine, China Medical University, Taichung, Taiwan
eProteomics Core Laboratory, Department of Medical Research, China Medical University Hospital, Taichung, Taiwan
fDepartment of Laboratory Medicine, China Medical University Hospital, Taichung, Taiwan
gDivision of Infectious Diseases, Department of Internal Medicine, China Medical University Hospital, Taichung, Taiwan
hDepartment of Neonatology, Children’s Hospital, China Medical University Hospital, China Medical University, Taichung, Taiwan
iSchool of Chinese Medicine and Department of Pediatrics, Children's Hospital, China Medical University, Taichung, Taiwan
jGraduate Institute of Biostatistics, College of Management, China Medical University, Taichung, Taiwan
kDepartment of Healthcare Administration, College of Health Science, Asia University, Taichung; Taiwan
lDepartment of Medical Research, China Medical University Hospital, Taichung, Taiwan
mDepartment of Laboratory Medicine, Linkou Chang-Gung Memorial Hospital, Taoyuan; Taiwan;
nDepartment of Medical Biotechnology and Laboratory Science, Chang Gung University, Kweu-Shan, Taoyuan; Taiwan.
#Correspondence and reprints: Jang-Jih Lu, MD, PhD
Department of Laboratory Medicine, Linkou Chang-Gung Memorial Hospital, 5 Fu-Hsin Street, Kweishan, Taoyuan 333, Taiwan
E-mail: [email protected]. Tel: 886-3-3281200#2542 Fax: 886-3-3971827
Running title: Clonal Dissemination of GBS in central Taiwan
Word count:
Abstract: 250 words
Main text: 2,308 words
Abstract
Background/Purpose(s): The aim of this study was to investigate clinical
presentation, serotype distribution and genetic correlation of group B streptococcus (GBS) diseases. Since serotype VI prevalence far exceed ed that reported in prior studies, genetic relationship of isolates was further analyzed.
Methods: GBS isolate s obtaining from patients with invasive diseases and pregnant women with colonization between June 2007 and December 20 10 were analyzed. All isolates were test ed for serotypes by multiplex PCR assay and p ulsed-field gel electrophoresis (PFGE) . S erotype VI isolates were further analyzed by m ultilocus sequence typing (MLST).
Results: A total of 134 GBS isolates were recovered from blood of 126 patients with invasive disease ( 94.0 %) and anogenital swabs of 8 pregnant women ( 6.0 %). Most common serotype was Ib (21. 6 %), followed by V (20.1%), VI (1 8.7 %), III (1 5.7 %), II ( 11.9 %), Ia (1 1.2 %), and IX (0. 7 %). Serotype VI was also the leading type in infants with early onset disease (EOD) (37.5%) and colonizing pregnant women (37.5%). PFGE distinguished 33 pulsotypes, reflecting genetic diversity among GBS isolates . Among 25 serotype VI isolates tested, 14 were ST-1, 7 were ST-679, 3 were ST-678, 1 was ST-681 and distributed into 4 PFGE pulsotypes. ST-678, ST-679 andST-681 were novel sequence types; ST-678 and ST-679 were single-locus variants of ST-1 that belongs to clonal complex (CC) 1.
Conclusions: CC1 dissemination of serotype VI GBS thus emerges as an important invasive pathogen in infants and non-pregnant adults in central Taiwan. Serotype prevalence of GBS must be continuously monitored geographically to guide prevention strategy of GBS vaccines.
Keywords: group B Streptococcus, multilocus sequence typing (MLST), pulse-field gel electrophoresis (PFGE), sequence type
Introduction
Group B Streptococcus (GBS), also known as Streptococcus agalactiae, is a major cause of invasive infection in neonates, pregnant women, and non-pregnant adults over age 65 or those immunocompromised by underlying medical conditions. GBS, an encapsulated gram-positive bacterium, colonizes human gastrointestinal and genital tracts. Neonates acquire colonization and infection with GBS vertically, either in utero by the ascending route or at delivery. Since initiation of maternal intrapartum chemoprophylaxis (IAP) in 1996 in the United States, the incidence of early-onset disease (EOD) has declined by 65% compared with the pre-prevention era baseline rate in 1993. Still, maternal IAP does not reduce the incidence of late-onset disease (LOD) . In addition to neonates, growing prevalence of invasive GBS disease in non-pregnant adults has been reported, with common clinical syndromes of bacteremia without focus, skin and/or soft-tissue infection and pneumonia. Most (88.0%) adult GBS cases had underlying conditions, diabetes the most common (41.0-44.4%) . Vaccinating pregnant women with glycoconjugate vaccine could potentially prevent invasive GBS diseases of newborn .
By structure of surface capsular polysaccharide (CPS), isolates were serotyped as Ia, Ib, II through VIII, and provisional IX . Serotypes Ia, Ib, II, III and V accounted for 96% of neonatal cases and 88-93% of adult cases , targets of protective immunity and candidates of GBS vaccines. In contrast to these, serotype VI has been rarely cited in Europe and America: 1% in infants younger than 90 days and 0.1% in non-pregnant adults , yet predominant in Japan among GBS strains isolated from pregnant women with colonization (5.6-24.7%) and neonates with EOD (8.5%) . In Taiwan, the past 20 years have seen serotype VI reported sporadically: 2.6% in patients with invasive disease during 1994-2004 , 4% between 2001 and 2004 . Still, prevalence rose to
10.5% in non-pregnant patients between 2006 and 2008 and 12% in cases of invasive disease from 1998 to 2009 .
To understand the epidemiology of GBS diseases in central Taiwan, we collected GBS isolates from invasive disease patients and pregnant women with colonization, analyzing serotype distribution and genetic correlation by pulse-field gel electrophoresis (PFGE) . Since serotype VI prevalence far exceed ed that reported in prior studies, genetic relationship of isolates was further analyzed by multilocus sequence typing (MLST).
Material and Methods GBS isolates
From June 2007 to December 2010, GBS isolates obtaining from blood of patients with invasive diseases along with anogenital swabs of colonizing pregnant women at China Medical University Hospital (CMUH) in central Taiwan, were analyzed. One isolate per patient was included, GBS strains grouped by clinical outcome and anatomical isolation sites: invasive strains from blood (n126) and colonizing strains from anogenital specimens (n8). Case details were gleaned from medical records. Primary bacteremia was defined as the presence of viable bacteria in blood without obvious site of active infection. GBS disease in infants was categorized as early onset disease (EOD) (birth-6 days) and late onset disease (LOD) (age 7-89 days) . This project was approved by the Institutional Review Board of our hospital (DMR100-IRB-237-1).
Identification and serotyping
Isolates cultured onto 5% sheep blood plate for 24h at 37C in 5% CO2 atmosphere were identified according to colony morphology, -hemolysis, Gram staining, and Lancefield grouping with type B antisera. Serotyping was performed via multiplex PCR assay previously described by Imperi et al. .
Antimicrobial susceptibility testing
Isolates were rated for susceptibility to penicillin, clindamycin and erythromycin, as per Clinical and Laboratory Standards Institute guidelines by microdilution MIC method . The double-disk diffusion test was applie d to uncover inducible clindamycin resistance .
Pulsed-field gel electrophoresis (PFGE)
endonuclease SmaI (New England BioLabs, Beverly, MA) as previously described , with modification. After digestion, PFGE was performed on the CHEF-DR III System (Bio-Rad Laboratories, Hercules, CA), with these parameters: switch time of 1-5s for 8 hr, 3.5-45s for 12 hr; 6 V/cm; 14°C; 120 angle. PFGE patterns were then examined with Bionumerics software (Applied Maths, Kortrijik, Belgium) and a dendrogram was generated using the unweighted pair group method with arithmetic mean (UPGMA) algorithm. The Dice similarity coefficient was employed, with optimization position tolerance settings of 1.0% and 1.5%, respectively. Isolates with similarities of 80% clustered as highly genetically related and grouped as one pulsotype (PT).
Multilocus sequence typing (MLST)
MLST evaluated twenty-five serotype VI isolates, sequencing seven housekeeping genes, as originally described , sequence type (ST) determined via Streptococcus agalactiae MLST database (http://pubmlst.org/sagalactiae). Sequence types not previously described were submitted and assigned at the S. agalactiae MLST database.
Statistical analysis
Data were analyzed using SAS version 9.3 (SAS Institute, Cary, NC) . Trend over time was analyzed using logistic regression analysis. Chi-square test or Fisher's exact test were used for the comparison of proportions; 2-tailed p < .05 was considered to be statistically significant.
Results
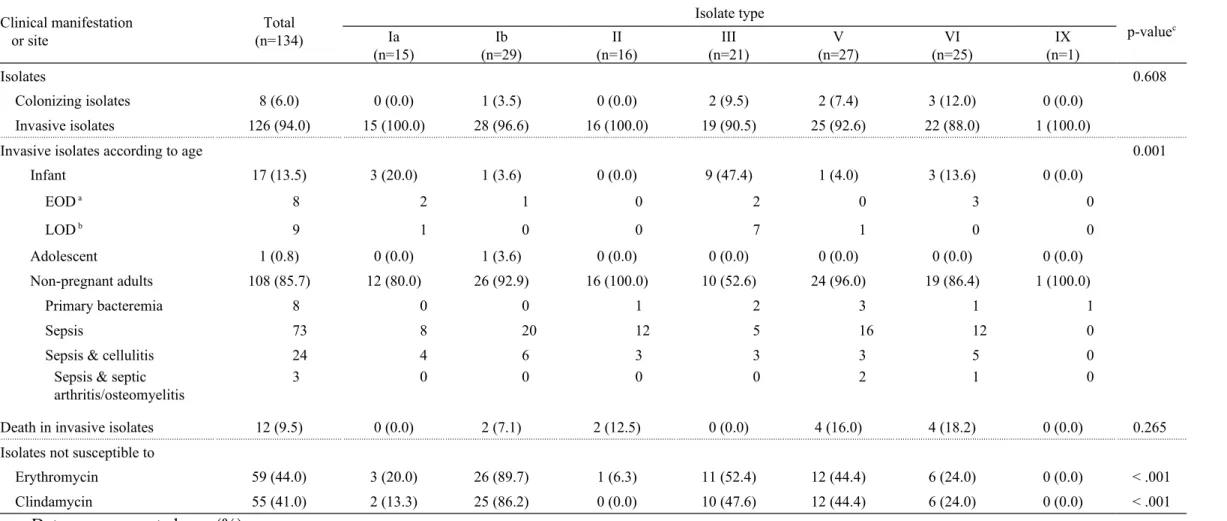
A total of 134 GBS isolates were recovered from blood of 126 (94.0%) patients with invasive disease and anogenital swabs of eight pregnant women (6.0%). (Table 1) Among invasive cases, infants had higher prevalence of serotype III isolate whereas non-pregnant adults had higher prevalence of serotypes Ib, II, V, and VI. Among patients with invasive diseases, the overall mortality was 9. 5 % (1 2 / 126 ) , and mortality did not d iffer with regard to serotypes (p 0.265). Clinical presentations of 17 infants emerged as 8 EOD and 9 LOD . One adolescent with acute lymphocytic leukemia had sepsis. Of 108 non-pregnant adults (57% female), most common manifestation was sepsis (n73, 68%), followed by sepsis with cellulitis (n24, 22%), primary bacteremia (n8, 7%), and sepsis with arthritis/osteomyelitis (n3, 3%). Overall, types Ib (n29, 21.6%) and V (n27, 19.1%) were predominant, followed by VI (n25, 18.7%), III (n21, 15.7%), II (n16, 11.9%), Ia (n15, 11.2%), and IX (n1, 0.7%). Type III was most common in infants, type VI (37.5%) in infants with EOD. Of 108 non-pregnant adults, type Ib (24.1%) was most frequent and type VI (17.5%) was third. Type VI (37.5%) was also most common in colonizing isolates. Every isolate proved susceptible to penicillin; still, 44% (59/134) and 41% (55/134) of strains were resistant to erythromycin and clindamycin, re s pectively . I nducible clindamycin resistanc e was not detected in these strains . Serotype Ib showed highest resistance to erythromycin (86%) (p < .001) and clindamycin (90%) (p < .001). (Table 1)Among 25 serotype VI isolates, resistance rates to erythromycin and clindamycin both tallied 24% (Tables 1-2). The proportion of invasive serotype VI increase d from 12.5% in 2007 to 15.9% (unpublished data, CMUH) in 2012, but the increasing trend was not statistically significant (P for trend 0.9236 ).
1). We defined a major pulsotype as comprising at least five strains: i.e., six major PFGE pulsotypes (3, 4, 18, 25, 26, 27) containing 96 (72%) of 134 isolates (Table 3, Figure 1), pulsotype 27 (25%, 34/134) most common. Serotypes Ib and V were most homogenous; Ia, II, III, and VI heterogenous, each contained two or three pulsotypes (Table 3). Pulsotypes 3, 4 and 25 contained solely isolates of serotypes Ia, III and VI, respectively. Pulsotypes 18, 26 and 27 showed more diversity: each comprised two or three serotypes (Table 3).
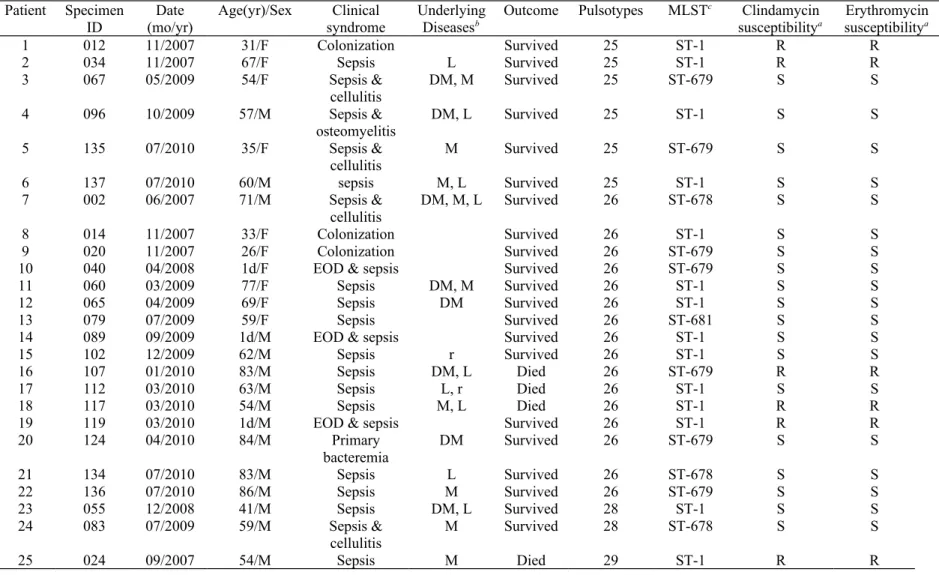
Table 2 depicts clinical data of 25 patients infected or colonized with serotype VI isolates, distributed into four pulsotypes. Pulsotype26 was most common, accounting for 64%(n 16) of 25 isolates; 6(24%) pulsotype 25, 2 (8%) pulsotype 28 and 1 (4%) pulsotype 29. The 25serotype VI isolates studied by MLST contained four sequence types, including ST-1 (n 14), and three novel STs, ST-678 (allelic profile 1,37,2,1,1,2,2) (n 3), ST-679 (allelic profile 1,9,2,1,1,2,2) (n 7), and ST-681 (allelic profile 35,2,2,1,1,2,2) (n 1). ST-678, ST-679 and ST-681 had never been defined before this study. All but one serotype VI isolate (patient 12, ST-681) displayed ST-1 or single-locus variant (SLV) of it (ST-678 and ST-679), belonging to clonal complex (CC) 1.Isolates from three neonates with EOD and three pregnant women with colonization were ST-1 (n 4) or ST-679 (n 2). Four non-pregnant adults with sepsis and underlying conditions died. No correlation surfaced between pulsotypes, STs and isolation dates.
Discussion
In this study, serotype VI was predominant in EOD infants (3/8, 37.5%) and colonized pregnant women (3/8, 37.5%), ranking third (17.5%) among non-pregnant adults with invasive infection. Overall, 25 isolates (18.7%) belonged to serotype VI in 134 GBS isolates; 96% of them ST-1, ST-678 or ST-679 (latter two SLVs of ST-1), based on MLST analysis and belonging to clonal complex (CC) 1, divided into four pulsotypes. Previous studies disclosed 9.4% to 12% prevalence of serotype VI in southern and northern Taiwan. Therefore, prevalence of 18.7% in this study points to cloncal dissemination of serotype VI GBS, CC1as an important pathogen in central Taiwan.
Earlier (1994-2004) study in southern Taiwan identified only 2.6% invasive isolates as serotype VI . A 1998-2009 study in northern Taiwan disclosed its emergence in non-pregnant adults with invasive GBS disease, 12% prevalence . In addition, 10.5% of GBS isolates from non-pregnant patients were serotype VI in southern Taiwan (2006-2008). A recent study in southern Taiwan (2008-2010) unveiled 9.4 % isolates obtaining from hospitalized non-pregnant adults as serotype VI
. Based on upward trends of serotype VI GBS in Taiwan , Japan , Malaysia , Thai-Myanmar border , and our current study (18.7%), it is possible that type VI has emerged as a prominent pathogen in Taiwan since the late 1990s and in Asia since the mid-1980s.
Invasive GBS serotypes vary among geographic regions and age groups . Globally, in infants aged younger than 90 days, main serotypes were III (49%) and Ia (23%). This study showed similar results, but type Ib (21.6%) most common in non-pregnant adults, sharply differing from Skoff et al.: serotypes V (29.2%), Ia (24.3%), II (13.5%) and III (11.4%) predominant. In our study, 17.5% of invasive and 37.5% of
colonizing strains were serotype VI, far higher than previous studies:1% in infants less than 90 days old and 0.1% in non-pregnant adults . In addition, our study showed that serotype VI strains obtained from term infants with EOD and colonized pregnant women tallied 37.5%. Further evidence arose from our 201 1 -2012 surveillance: 14% (19/136) invasive and 13.6% (9/66) colonizing isolates from pregnant women were serotype VI (unpublished CMUH data). Serotype VI was first detected in 1977 at the Centers for Disease Control, Atlanta . A majority of serotype VI distributed in Japan since the mid-1980s accounted for 5.6-26.6% in pregnant women with colonization and EOD (8.5%). Pregnant women colonized with it were also common in Malaysia (17%) , Thai-Myanmar border(16.7%) , and Iran (12.5%) . Nonetheless, serotype VI has been reported sporadically in America , Korea, Greek , the Netherlands , Kuwait, and Australia .
Besides ST1, novel sequence types 678 and 679, SLV of ST1 never reported, belonging CC1, were exhibited by serotype VI in this study. In addition, earlier study (2001-2004) revealed two strains of serotype VI GBS with CC1 (ST1). Non-invasive serotype VI GBS strains with reduced penicillin susceptibility belonging to ST1 and ST-458 (a SLV of ST-1) were reported in Japan . Wong et al. noted emergence of serotype VI GBS as an invasive pathogen since 2006 in northern Taiwan , later in southern Taiwan by Wang et al. after 2008 . Specific clone CC1 serotype VI might play a role in vertical transmission in cases with EOD from colonized pregnant women and invasive disease in immunocompromised non-pregnant adults in central
three serotypes (Table 3, Figure 1). Serotypes Ib and V were most homogenous, with unique pulsotypes; Ia, II, III and VI heterogenous, including two or three pulsotypes and indicating greater genetic diversity. Similar heterogeneity between serotypes and PFGE pulsotypes has been reported in southern Brazil , Italy and America . Cieslewicz et al. viewed GBS capsular polysaccharide structural diversity as driven by horizontal gene transfer, through introduction of novel DNA sequence and genetic recombination.Martins et al. later unearthed clear evidence for in vivo capsular switching in Streptococcus agalactiae . Classical and convenient typing by bacteria capsular polysaccharide composition fails to mirror genetic diversity of species .
Main limitation of this study is small sample size, especially in infants and colonized pregnant women. Still, to our knowledge, this is the largest case series of invasive serotype VI GBS infection by strains belonging to genetic lineage CC1, regarding detail clinical manifestations, PFGE and MLST studies, particularly in infants, pregnant women and non-pregnant adults. Immunizing pregnant women with capsular (CPS)-based conjugate vaccines (Ia, Ib, II, III, V), prevalent serotypes found in North America and Europe, could potentially prevent invasive GBS disease of newborns .These provide no essential protection for individuals in areas where predominant capsular types like serotype VI have arisen. It is also alarming that resistance to clinidamycin and erythromycin in serotype VI GBS isolates from pregnant cases with colonization and newborn with EOD. Neonatal GBS infection was still a common threat in Taiwan, with incidence of 1 per 1000 live births of infants during 2001-2005 . Considering geographical location, the emergence of type VI, CC1 GBS strains in central Taiwan mandates inclusion in GBS vaccine in Asia for pregnant women. GBS serotype distribution should be continuously monitored to guide prevention strategy, such as effective vaccines.
Acknowledgments
The study was partly funded by grants from China Medical University Hospital (DMR-100-049) at Taichung, Chang Gung Memorial Hospital (CMRPG3B0642) at Taoyuan, and the National Science Council (NSC-101-2320-B-182A-002-MY3). We thank Hui-Chen Chen for performing PFGE, and Prof. Philippe Glaser (Institut Pasteur, Paris, France) for reading critically the manuscript.
Conflict of Interest
States, 1999-2005. JAMA 2008;299:2056-65.
2. Skoff TH, Farley MM, Petit S, Craig AS, Schaffner W, Gershman K, et al. Increasing burden of invasive group B streptococcal disease in nonpregnant adults, 1990-2007. Clin Infect Dis 2009;49:85-92.
3. Lamagni TL, Keshishian C, Efstratiou A, Guy R, Henderson KL, Broughton K, et al. Emerging Trends in the Epidemiology of Invasive Group B
Streptococcal Disease in England and Wales, 1991-2010. Clin Infect Dis 2013;57:682-8.
4. Schrag SJ, Zywicki S, Farley MM, Reingold AL, Harrison LH, Lefkowitz LB, et al. Group B streptococcal disease in the era of intrapartum antibiotic prophylaxis. N Engl J Med 2000;342:15-20.
5. Heath PT. An update on vaccination against group B streptococcus. Expert review of vaccines 2011;10:685-94.
6. Edwards MS, Lane HJ, Hillier SL, Rench MA, Baker CJ. Persistence of functional antibodies to group B streptococcal capsular polysaccharides following immunization with glycoconjugate vaccines. Vaccine 2012. 7. Slotved H-C, Kong F, Lambertsen L, Sauer S, Gilbert GL. Serotype IX, a
proposed new Streptococcus agalactiae serotype. J Clin Microbiol 2007;45:2929-36.
8. Edmond KM, Kortsalioudaki C, Scott S, Schrag SJ, Zaidi AK, Cousens S, et al. Group B streptococcal disease in infants aged younger than 3 months: systematic review and meta-analysis. Lancet 2012;379:547-56.
9. Lachenauer CS, Kasper DL, Shimada J, Ichiman Y, Ohtsuka H, Kaku M, et al. Serotypes VI and VIII predominate among group B streptococci isolated from pregnant Japanese women. J Infect Dis 1999;179:1030-3.
10. Ueno H, Yamamoto Y, Yamamichi A, Kikuchi K, Kobori S, Miyazaki M. Characterization of Group B Streptococcus Isolated from Women in Saitama City, Japan. Jpn J Infect Dis 2012;65:516-21.
11. Kimura K, Matsubara K, Yamamoto G, Shibayama K, Arakawa Y. Active screening of group B streptococci with reduced penicillin susceptibility and altered serotype distribution isolated from pregnant women in kobe, Japan. Jpn J Infect Dis 2013;66:158-60.
12. Hoshina K, Suzuki Y, Nishida H, Kaneko K, Matsuda S, Kobayashi M, et al. Trend of neonatal group B streptococcal infection during the last 15 years. Pediatr Int 2002;44:641-6.
13. Ho YR, Li CM, Su HP, Wu JH, Tseng YC, Lin YJ, et al. Variation in the number of tandem repeats and profile of surface protein genes among invasive group B Streptococci correlates with patient age. J Clin Microbiol
2007;45:1634-6.
14. Tien N, Ho CM, Lin HJ, Shih MC, Ho MW, Lin HC, et al. Multilocus
sequence typing of invasive group B Streptococcus in central area of Taiwan. J Microbiol Immunol Infect 2011;44:430-4.
15. Wang YH, Su LH, Hou JN, Yang TH, Lin TY, Chu C, et al. Group B streptococcal disease in nonpregnant patients: emergence of highly resistant strains of serotype Ib in Taiwan in 2006 to 2008. J Clin Microbiol
2010;48:2571-4.
16. Wong SS, Tsui K, Liu Q-D, Lin L-C, Tsai CR, Chen L-C, et al. Serotypes, surface proteins, and clinical syndromes of invasive Group B streptococcal infections in northern Taiwan, 1998–2009. Journal of Microbiology, Immunology and Infection 2011;44:8-14.
17. Imperi M, Pataracchia M, Alfarone G, Baldassarri L, Orefici G, Creti R. A multiplex PCR assay for the direct identification of the capsular type (Ia to IX) of Streptococcus agalactiae. J Microbiol Methods 2010;80:212-4.
18. Clinical and Laboratory Standards Institute. Performance standards for antimicrobial susceptibility testing, 19th informational supplement. M100-S19. Wayne, PA: CLSI; 2009.
19. Oliveira IC, De Mattos MC, Areal MF, Ferreira-Carvalho BT, Figuiredo AM, Benchetrit LC. Pulsed-field gel electrophoresis of human group B streptococci isolated in Brazil. J Chemother 2005;17:258-63.
20. Jones N, Bohnsack JF, Takahashi S, Oliver KA, Chan M-S, Kunst F, et al. Multilocus sequence typing system for group B streptococcus. J Clin Microbiol 2003;41:2530-6.
21. Wang YH, Chen HM, Yang YH, Yang TH, Teng CH, Chen CL, et al. Clinical and microbiological characteristics of recurrent group B streptococcal
infection among non-pregnant adults. Int J Infect Dis 2014;26:140-5. 22. Matsubara K, Katayama K, Baba K, Nigami H, Harigaya H, Sugiyama M.
Seroepidemiologic studies of serotype VIII group B Streptococcus in Japan. J Infect Dis 2002;186:855-8.
23. Dhanoa A, Karunakaran R, Puthucheary SD. Serotype distribution and antibiotic susceptibility of group B streptococci in pregnant women. Epidemiol Infect 2010;138:979-81.
24. Turner C, Turner P, Po L, Maner N, De Zoysa A, Afshar B, et al. Group B streptococcal carriage, serotype distribution and antibiotic susceptibilities in pregnant women at the time of delivery in a refugee population on the Thai-Myanmar border. BMC Infect Dis 2012;12:34.
25. Wilkinson HW. Nontypable group B streptococci isolated from human sources. J Clin Microbiol 1977;6:183-4.
26. Jannati E, Roshani M, Arzanlou M, Habibzadeh S, Rahimi G, Shapuri R. Capsular serotype and antibiotic resistance of group B streptococci isolated from pregnant women in Ardabil, Iran. Iran J Microbiol 2012;4:130-5. 27. Manning SD, Foxman B, Pierson CL, Tallman P, Baker CJ, Pearlman MD.
Correlates of antibiotic-resistant group B streptococcus isolated from pregnant women. Obstet Gynecol 2003;101:74-9.
28. Uh Y, Kim HY, Jang IH, Hwang GY, Yoon KJ. Correlation of serotypes and genotypes of macrolide-resistant Streptococcus agalactiae. Yonsei Med J 2005;46:480-3.
29. Tsolia M, Psoma M, Gavrili S, Petrochilou V, Michalas S, Legakis N, et al. Group B streptococcus colonization of Greek pregnant women and neonates: prevalence, risk factors and serotypes. Clin Microbiol Infect 2003;9:832-8. 30. van Elzakker E, Yahiaoui R, Visser C, Oostvogel P, Muller A, Ho YR, et al.
Epidemiology of and prenatal molecular distinction between invasive and colonizing group B streptococci in The Netherlands and Taiwan. Eur J Clin
belonging to different age groups. Clin Microbiol Infect 2008;14:260-7. 33. Kimura K, Nagano N, Nagano Y, Wachino J, Suzuki S, Shibayama K, et al.
Predominance of sequence type 1 group with serotype VI among group B streptococci with reduced penicillin susceptibility identified in Japan. J Antimicrob Chemother 2011;66:2460-4.
34. Nagano N, Nagano Y, Toyama M, Kimura K, Tamura T, Shibayama K, et al. Nosocomial spread of multidrug-resistant group B streptococci with reduced penicillin susceptibility belonging to clonal complex 1. J Antimicrob
Chemother 2012;67:849-56.
35. Palmeiro JK, Dalla-Costa LM, Fracalanzza SE, Botelho AC, da Silva
Nogueira K, Scheffer MC, et al. Phenotypic and genotypic characterization of group B streptococcal isolates in southern Brazil. J Clin Microbiol
2010;48:4397-403.
36. Gherardi G, Imperi M, Baldassarri L, Pataracchia M, Alfarone G, Recchia S, et al. Molecular epidemiology and distribution of serotypes, surface proteins, and antibiotic resistance among group B streptococci in Italy. J Clin Microbiol 2007;45:2909-16.
37. Martins ER, Melo-Cristino J, Ramirez M. Evidence for rare capsular switching in Streptococcus agalactiae. J Bacteriol 2010;192:1361-9.
38. Cieslewicz MJ, Chaffin D, Glusman G, Kasper D, Madan A, Rodrigues S, et al. Structural and genetic diversity of group B streptococcus capsular
polysaccharides. Infect Immun 2005;73:3096-103.
39. Tettelin H, Masignani V, Cieslewicz MJ, Donati C, Medini D, Ward NL, et al. Genome analysis of multiple pathogenic isolates of Streptococcus agalactiae: implications for the microbial "pan-genome". Proc Natl Acad Sci U S A 2005;102:13950-5.
40. Yu HW, Lin HC, Yang PH, Hsu CH, Hsieh WS, Tsao LY, et al. Group B streptococcal infection in Taiwan: maternal colonization and neonatal infection. Pediatr Neonatol 2011;52:190-5.
Table 1. Serotype distribution of group B streptococcus disease in children, pregnant women and non-pregnant adults, by age, clinical manifestations, and resistance of erythromycin and clindamycin, 2007-2010
Clinical manifestation or site Total (n=134) Isolate type p-valuec Ia (n=15) Ib (n=29) II (n=16) III (n=21) V (n=27) VI (n=25) IX (n=1) Isolates 0.608 Colonizing isolates 8 (6.0) 0 (0.0) 1 (3.5) 0 (0.0) 2 (9.5) 2 (7.4) 3 (12.0) 0 (0.0) Invasive isolates 126 (94.0) 15 (100.0) 28 (96.6) 16 (100.0) 19 (90.5) 25 (92.6) 22 (88.0) 1 (100.0)
Invasive isolates according to age 0.001
Infant 17 (13.5) 3 (20.0) 1 (3.6) 0 (0.0) 9 (47.4) 1 (4.0) 3 (13.6) 0 (0.0) EOD a 8 2 1 0 2 0 3 0 LOD b 9 1 0 0 7 1 0 0 Adolescent 1 (0.8) 0 (0.0) 1 (3.6) 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) Non-pregnant adults 108 (85.7) 12 (80.0) 26 (92.9) 16 (100.0) 10 (52.6) 24 (96.0) 19 (86.4) 1 (100.0) Primary bacteremia 8 0 0 1 2 3 1 1 Sepsis 73 8 20 12 5 16 12 0
Sepsis & cellulitis 24 4 6 3 3 3 5 0
Sepsis & septic arthritis/osteomyelitis
b LOD, late-onset disease.
Table 2. Clinical data and general characteristics of 25 serotype VI GBS isolates from patients with invasive GBS disease or colonization during 2007-2010
Patient Specimen
ID (mo/yr)Date Age(yr)/Sex syndromeClinical UnderlyingDiseasesb Outcome Pulsotypes MLST
c Clindamycin
susceptibilitya susceptibilityErythromycina
1 012 11/2007 31/F Colonization Survived 25 ST-1 R R 2 034 11/2007 67/F Sepsis L Survived 25 ST-1 R R 3 067 05/2009 54/F Sepsis & cellulitis DM, M Survived 25 ST-679 S S 4 096 10/2009 57/M Sepsis & osteomyelitis DM, L Survived 25 ST-1 S S 5 135 07/2010 35/F Sepsis & cellulitis M Survived 25 ST-679 S S 6 137 07/2010 60/M sepsis M, L Survived 25 ST-1 S S 7 002 06/2007 71/M Sepsis & cellulitis DM, M, L Survived 26 ST-678 S S 8 014 11/2007 33/F Colonization Survived 26 ST-1 S S 9 020 11/2007 26/F Colonization Survived 26 ST-679 S S
10 040 04/2008 1d/F EOD & sepsis Survived 26 ST-679 S S
11 060 03/2009 77/F Sepsis DM, M Survived 26 ST-1 S S
12 065 04/2009 69/F Sepsis DM Survived 26 ST-1 S S
13 079 07/2009 59/F Sepsis Survived 26 ST-681 S S
14 089 09/2009 1d/M EOD & sepsis Survived 26 ST-1 S S
15 102 12/2009 62/M Sepsis r Survived 26 ST-1 S S
16 107 01/2010 83/M Sepsis DM, L Died 26 ST-679 R R
17 112 03/2010 63/M Sepsis L, r Died 26 ST-1 S S
aS, susceptible, MIC 0.25 g/mL; R, resistant, MIC 1g/mL
bDM, diabetes mellitus; L, liver diseases; M, malignancy; r: renal diseases
cMultilocus sequence type of 7 housekeeping genes (adhP, pheS, atr, glnA, sdhA, glcK, tkt). Allelic profiles of ST-1 (1, 1, 2, 1, 1, 2, 2); ST-678 ( 1, 37, 2, 1, 1, 2, 2); ST-679 (1, 9, 2, 1, 1, 2, 2); ST-681 (35, 2, 2, 1, 1, 2, 2)
Table 3.Major pulsotypescorrelating with serotype among 96 of 134 GBS isolates
during 2007-2010
PFGE Pulsotypes
No. of isolates in each serotype Tota l Ia Ib II III V VI 3 5 5 4 7 7 18 25 24 1 25 6 6 26 19 2 1 16 27 34 1 12 21 Total 96 8 24 13 8 21 22
Fig. 1. Phylogenitic analysis of the pulsed field gel electrophoresis (PFGE) profiles of 134 GBS strains obtained during 2007-2010. The dendrogram was concocted by the unweighted pair group method with arithmetic mean (UPGMA) algorithm.
Pulsotypes, shown to the right of the dendrogram with PFGE-80, were termed as strains clustering on the dentrogram at a 80% similarity cutoff point. Additionally denoted are isolates designation and serotype by multiplex-PCR identified in each isolate.