452 Kaohsiung J Med Sci October 2005 • Vol 21 • No 10 Radiation therapy is considered effective in nasopharyngeal
carcinoma (NPC) and other head and neck malignancies. However, it is not without morbidity, and complications can develop as a result of damage to neighboring structures. The irradiation field of head and neck neoplasms may include brain tissue, which may result in brain radiation necrosis. Reported cases of cerebral radionecrosis are still rare in Taiwan. We present seven cases that were clinically diagnosed as cerebral radionecrosis among NPC patients in our institute. We also review cases of extracranial malignancies, diagnostic modalities and treatment from the literature.
C
EREBRAL
R
ADIONECROSIS
IN
P
ATIENTS
WITH
N
ASOPHARYNGEAL
C
ARCINOMA
Ying-Che Hsu, Ling-Feng Wang, Ka-Wo Lee, Kuen-Yao Ho, Chih-Jen Huang,1 and Wen-Rei Kuo Departments of Otolaryngology and 1Radiation Oncology, Kaohsiung Medical University
Chun-Ho Memorial Hospital, Kaohsiung Medical University, Kaohsiung, Taiwan.
This study involved seven patients with cerebral radionecrosis following radiation therapy for nasopharyngeal carcinoma (NPC). Their charts were reviewed and the relationship of extracranial malignancies to cerebral radionecrosis was investigated. The radiation dose ranged from 70 to 135 Gy, and the latency was from 6 to 39 months. Two of seven patients died of NPC-related complications during follow-up. The crude incidence of cerebral radionecrosis in patients with NPC was 0.93% in our series. Improvement of symptoms could be achieved by corticosteroid therapy, with or without surgery. In a review of the literature, there were 306 cases of cerebral radionecrosis in extracranial malignancies. The nasopharynx is the most common primary site in cerebral radionecrosis of extracranial malignancies, followed by the scalp and sinonasal tract. The 3-year overall survival rate in our series was 68.57%, as provided by the Kaplan-Meier product limited method. Cerebral radionecrosis in NPC patients should be differentiated from tumor recurrence, in order to apply the appropriate treatment.
Key Words: radionecrosis, nasopharyngeal carcinoma (Kaohsiung J Med Sci 2005;21:452–9)
Received: April 24, 2005 Accepted: August 11, 2005
Address correspondence and reprint requests to: Dr. Wen-Rei Kuo, Department of Otolaryngology, Kaohsiung Medical University,
100 Tzyou 1st Road, Kaohsiung 807, Taiwan.
E-mail: [email protected]
M
ATERIALSANDM
ETHODSFrom 1991 to 2001, 775 patients with newly diagnosed NPC received complete radiotherapy at Kaohsiung Medical University Hospital. By May 2004, seven patients had a clinical diagnosis of cerebral radionecrosis. Their charts were retrospectively reviewed. There were four male and three female patients. The mean age at diagnosis of cerebral radionecrosis was 52.7 years (range, 34–74 years).
Four of seven patients had received neoadjuvant or adjuvant chemotherapy with a cisplatin-based regimen (cisplatin, 5-fluorouracil, and leucovorin). None had concurrent chemoradiotherapy. One patient had diabetes mellitus. Five patients with documented recurrence had been re-irradiated. All patients were treated with 6 MV photons using the same technique of two lateral-opposed fields, supplemented by an anterior field. The radiation dose per course was 65–70 Gy, delivered in 2-Gy fractions
via the lateral portal once daily for 5 days per week, and 1.5-Gy (6 patients) or 1.8-Gy (1 patient) fractions 10 times via the anterior portal. The total radiation dose ranged from 70 to 135 Gy (mean, 111 Gy), and the mean latent period from the end of the last radiation to the diagnosis of cerebral radionecrosis was 26.3 months (range, 6–39 months).
Computed tomography (CT) or magnetic resonance imaging (MRI) of the brain was performed in all patients. The diagnosis of cerebral radionecrosis was confirmed by surgical intervention in two cases and clinically diagnosed based on CT or MRI in five cases. Five patients had a further MRI perfusion-diffusion weighted scan. One had a Tc99m-hexamethyl-propyleneamine oxime (HMPAO) single photon emission CT (SPECT) scan of the brain.
A search of the English-language literature was undertaken in PubMed (http://www.ncbi.nlm.nih.gov/).
R
ESULTSThe incidence of cerebral radionecrosis in NPC in this series was 0.93% (7/755). Clinical symptoms and signs included epilepsy, change in consciousness, memory impairment, vertigo/dizziness, and headache (Table 1A and 1B). Epilepsy was the main presenting symptom for Patient 5, while Patient 4 only had vague symptoms and
developed epilepsy 19 months after the diagnosis of cerebral radionecrosis by CT scan. Two patients (2 and 7) had consciousness change as the initial manifestation. Patient 3 had severe vertigo that made her normal daily activity impossible. Patients 1 and 6 complained of headache as their main symptom. Six of the seven patients had an associated optic neuropathy.
Cerebral radionecrosis was mainly in the temporal lobe of the brain. In five patients, diffusion-perfusion weighted MRI of the intracranial lesion showed a high signal in the diffusion-weighted image, and a low signal in the perfusion-weighted image. Patients 1 and 2 had initial surgical treatment with surgicopathologic documentation, while the other patients were treated conservatively. Patient 7 received betamethasone (0.75 mg/day), Patients 1, 3, 5, and 6 were given prednisolone (15 mg/day), and Patient 2 was treated with cortisone (25 mg/day).
Patient 1 formed a brain abscess 20 months after the diagnosis of cerebral radionecrosis and underwent craniotomy. Patient 3 developed intracranial hemorrhage 17 months after diagnosis and presented with epilepsy. The follow-up period lasted for a mean of 21.3 months (range, 4–36 months). Six patients had a favorable response to corticosteroids, with or without surgery, while one (Patient 4) was treated only with an anti-epileptic agent. Two patients eventually died of NPC-related complications during follow-up.
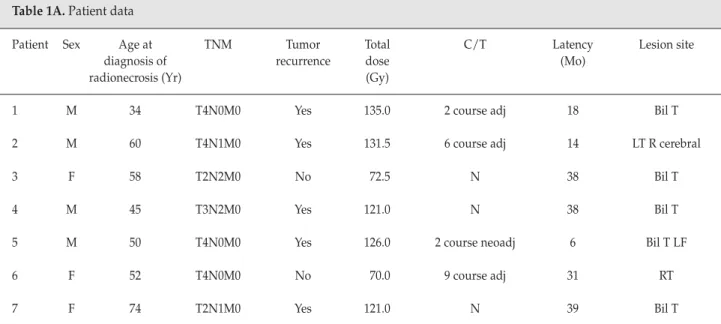
Table 1A. Patient data
Patient Sex Age at TNM Tumor Total C/T Latency Lesion site
diagnosis of recurrence dose (Mo)
radionecrosis (Yr) (Gy)
1 M 34 T4N0M0 Yes 135.0 2 course adj 18 Bil T
2 M 60 T4N1M0 Yes 131.5 6 course adj 14 LT R cerebral
3 F 58 T2N2M0 No 72.5 N 38 Bil T
4 M 45 T3N2M0 Yes 121.0 N 38 Bil T
5 M 50 T4N0M0 Yes 126.0 2 course neoadj 6 Bil T LF
6 F 52 T4N0M0 No 70.0 9 course adj 31 RT
7 F 74 T2N1M0 Yes 121.0 N 39 Bil T
C/T = chemotherapy; adj = adjuvant chemotherapy; Bil T = bilateral temporal; neoadj = neoadjuvant chemotherapy; LF = left frontal; RT = right temporal; TNM = tumor-node-metastasis staging.
T
able 1B.
Patient data
Patient
Clinical symptoms and signs of cer
ebral radionecr osis Systemic Tr eatment Duration of Clinical Epilepsy Consciousness Memory V ertigo/ Headache Associated disease Sur gery Corticoster oid follow-up after outcome change impairment dizziness optic neur opathy therapy diagnosis of cer ebral radionecr osis (Mo) 1 – – + + ++* + – Y es Y es 25
Brain abscess formation 20 months later
2 – +* + + – + – Y es Y es 15
Death at 15 months follow–up
3 – – – ++* + + DM No Y es 31
Bilateral intracranial hemorr
hage 17 months later 4 + – – + + + – No No 26
Epilepsy developed 19 months after diagnosis by CT scan
5 +* – + – – + – N o Y es 12 Impr oved 6 – – – + +* + – N o Y es 36 Impr oved 7 – +* + + – – – N o Y es 4
Death at 4 months follow–up
*Initial pr
esenting symptom for diagnosis of cer
ebral radionecrosis; – = none; + = mild to moderate; ++ = sever
e; DM = diabetes mellitus; CT = computed tomography
Chemotherapy r
D
ISCUSSIONThe incidence of NPC is higher in Southeast Asia than in the West. Radiation therapy is the main treatment modality, and the irradiation field inevitably covers the medial and inferior temporal lobes of the brain, owing to the close proximity to the skull base. In addition, the radiation dose is usually 65–70 Gy, which exceeds the tolerance of brain tissue.
Radionecrosis is a late complication of radiotherapy. The first case of extracranial neoplasm with cerebral radionecrosis was described by Fischer and Holfelder in 1930 [1]. In 1984, Glass et al reported nine cases of cerebral radionecrosis and reviewed another 65 cases in the literature [2]. Since then, another 232 patients have been reported, including our series (Table 2) [2–31], giving a total of 306 cases of cerebral radionecrosis in extracranial malignancy. The most common primary site of malignancy is the nasopharynx (mainly NPC), followed by the scalp and the sinonasal tract.
In our institute, cerebral radionecrosis was detected in seven cases, giving a crude incidence of 0.93%. The reported incidence of radionecrosis in NPC patients ranges from 0.40% to 18.60% with different radiation regimens [3,32,33]. Lee et al reported that 64 Gy at the conventional fraction of 2 Gy daily would lead to a 5% necrotic rate in 10 years [32]. Hence, the incidence of radionecrosis in NPC in our patients is thought to be underestimated. This may be because the fractional dose via the anterior portal was low (1.5 or 1.8 Gy) compared to the normal fractional dose (1.8–2.0 Gy). Other anatomic sites reported in the literature are summarized in Table 2.
The period between the last irradiation and the diagnosis of cerebral radionecrosis in our series ranged from 6 to 39 months (mean, 26.3 months). Latency has been reported at 1 month to 16 years after the end of irradiation [34], with approximately 80% occurring within 3 years after the last dose of radiotherapy [2]. The mechanism is thought to be endothelial cell damage, resulting in brain tissue ischemia in long-term follow-up [35,36].
The radiation dose in our series ranged from 70 to 135 Gy (mean, 111 Gy). The average dose was higher in our series because five of our seven cases had documented recurrent disease. A dose of 60 Gy delivered in 1.8–2-Gy fractions represents the upper limit of the “safe dose” to brain tissue [37]. To treat NPC, the radiation dose inevitably exceeds this limit. The irradiation field used to treat NPC and other malignancies of the sinonasal tract and scalp may include a part of the brain tissue. The ratio of brain tissue irradiated may be higher for scalp tumors than those in the nasopharynx, which makes the scalp the second most frequent tumor site associated with cerebral radionecrosis. The threshold for injury may be lowered by hypertension [38] or concomitant chemotherapy [39,40], although the effect of induction or adjuvant chemotherapy has not been reported. Old age or systemic illness may play a role in developing radionecrosis. Lee et al analyzed their irradiation regimen and concluded that the most significant factor was the fractional dose [32]. Prolonging the treatment time offered little protective effect [32], and yet, the overall treatment time had a significant impact [41]. The age at the time of radiotherapy also appeared to affect the volume of radionecrosis [42].
The clinical symptoms of cerebral radionecrosis are variable. It may manifest major symptoms, such as changes in consciousness and seizures, or minor complaints, such as dizziness, vertigo or memory impairment. In our series, consciousness change was detected in two cases, headache in two, epilepsy in one and vertigo in one. One patient had vague symptoms. If a patient has neurologic or psychiatric symptoms, an encephalopathy must be ruled out [4]. Patients with temporal lobe radionecrosis have significant impairments in memory, language, motor ability, and executive function, compared with those without radionecrosis [5]. Asymptomatic patients are sometimes found by follow-up imaging studies.
Distinguishing radionecrosis from tumor is a challenge in traditional imaging studies. The general characteristics of cerebral radionecrosis and tumors are summarized in Table 3. Differentiating radionecrosis from recurrent tumor is difficult with CT or MRI findings alone because of similar
Table 2. Primary malignancy site of cerebral radionecrosis in extracranial malignancy Location n Nasopharynx In the literature [2–17] 220 This series 7 Total 227 Scalp [2,18–22] 32 Sinonasal tract [2,17,23–28] 23 Ear [2,17] 9 Oropharynx [2] 2 Lacrimal gland [2] 4 Submandibular gland [2] 1 Parotid gland [2,29,30] 5
Glomus jugulare tumor [2] 1
Orbit [2,31] 2
imaging characteristics. Scintigraphic studies, such as
18
F-fluorodeoxyglucose positron emission tomography or
201
Tl chloride SPECT, have been reported to sensitively distinguish recurrent tumor from radionecrosis [43]. Recent MRI techniques, such as perfusion- and diffusion-weighted scans or MR spectroscopy to detect the brain N-acetylaspartate/choline ratio, may also help distinguish the lesion [7,8,44]. However, pitfalls in scintigraphic imaging have also been reported [18,23,24].
The standard diagnosis of radiation necrosis is histologic verification, and two of our seven patients had initial surgical treatment. The pathologic features of radionecrosis were fibrinoid and coagulation necrosis of the brain tissue. Even though surgery is an invasive procedure, it should be undertaken if the diagnosis is unclear. The surgical exploration rate may be reduced and the diagnostic rate may be increased by combining imaging studies and clinical characteristics. The clinical diagnosis of cerebral radionecrosis without pathologic proof in NPC patients has been discussed [6], and one study reported direct biopsy
under local anesthesia via a left temporal craniotomy by the neurosurgeon [30].
Treatment includes conservative management with corticosteroid or invasive procedures, such as craniotomy to clean necrotic tissue or brain lobectomy [9]. Six of our seven cases showed clinical improvement after corticosteroid therapy, with or without surgical treatment. The reported regimen is dexamethasone 4–16 mg/day for 4–6 weeks, which is gradually tapered off [3,10]. Tsui et al point out that a perfusion and diffusion mismatch might imply injured tissue, such as edema and potentially salvageable brain tissue, and this may be used to predict response to treatment [8]. Lee et al reported a mortality rate of 8% due to uncontrolled sepsis, with a 44% associated side-effect rate in corticosteroid treatment [3]. Hyperbaric oxygen therapy has also been reported [45].
Patient 3 developed a brain abscess 17 months after the diagnosis of cerebral radionecrosis. She underwent craniotomy and her symptoms improved, which stabilized her condition for the following 5 months of follow-up.
Table 3. Diagnostic tools and general characteristics of recurrent nasopharyngeal carcinoma and cerebral radionecrosis
Diagnostic tool Recurrent nasopharyngeal Cerebral radionecrosis Note
carcinoma
Angiography Avascular space-occupying lesion
CT [4] Low-density, Digitiform or round hypodense lesion Reported detection rate: 50%
post-contrast enhancement Post-contrast enhancement Detection rate < MRI
PET-18 FDG B uptake ? uptake Expensive and limited availability
SPECT B uptake ? uptake No significant differences in
sensitivity or specificity for
FDG-PET and 201Tl SPECT
MRI [6] Low signal in T1W, Low signal in T1W, Poorly differentiated from
high signal in T2W High signal in T2W tumor with only T1W, T2W
Heterogeneous contrast Heterogeneous contrast Superior sensitivity to
enhancement enhancement CT scan
Irregular or cystic shape Lesions best shown on T2W
MRI perfusion-weighted High signal Low signal
scan (rrCBV map)
MRI diffusion-weighted Low signal High signal
scan (ADC map) [7]
MR spectroscopy [44] B NAA/Cr ratio B Choline peak and ? NAA/Cr ratio
CT = computed tomography; MRI = magnetic resonance imaging; PET-18 FDG = 18
F-fluorodeoxyglucose positron emission tomography; SPECT = single photon emission computed tomography; T1W = T1 weighted; T2W = T2 weighted; rrCBV = relative regional blood volume; ADC = apparent diffusion coefficient; NAA/Cr = N-acetylaspartate/choline ratio.
Cheng et al reported six cases complicated by brain abscess formation in 28 patients with temporal lobe radionecrosis following radiotherapy for NPC [46]. Cerebral radiation necrosis is a predisposing cause of brain abscess formation, as is the use of corticosteroids. Surgical excision is the recommended treatment.
Six of our patients had optic neuropathy, possibly because of the higher radiation dose due to tumor recurrence. One patient with a lower irradiation dose had diabetes mellitus (Patient 3), which may exacerbate the impairment of microcirculation caused by radiotherapy. The patient developed intracranial hemorrhage 17 months after the diagnosis of cerebral radionecrosis (55 months after the end of radiotherapy). Cheng et al reported five cases of acute hemorrhage in late radiation necrosis of the temporal lobe [47]. The interval between the onset of hemorrhage and cranial irradiation was long (mean, 7.8 years), and rupture of the thin-walled new blood vessel is the hypothesized hemorrhage mechanism.
Clinical improvement has been reported in the treatment of cerebral radionecrosis using anti-coagulation therapy with heparin and warfarin [48]. Anti-platelet treatment with pentoxyfyllin, aspirin, and ticlopidine has also been used, but the potential risk of bleeding from these agents must be considered [49].
The follow-up time after diagnosis of cerebral radionecrosis ranged from 4 to 36 months (mean, 21.3 months). Two of our seven patients died. The 3-year overall survival rate in our series was 68.57%, as provided by the Kaplan-Meier product limited method. Lee et al found a 5-year survival rate for cerebral radionecrosis in NPC of 59%, with or without treatment [33]. The weak points of our sampling were the relatively short follow-up time and the limited numbers of cases.
C
ONCLUSIONSPatients with NPC comprise the majority of those with cerebral radionecrosis following treatment for extracranial malignancies. Differential diagnosis with tumor recurrence is needed. Since advances in the treatment of NPC have resulted in an accumulation of long-term survivors, cerebral radionecrosis may become a major clinical concern. Several studies have shown that a promising first-line treatment is with corticosteroids [3,4, 10,11]. The consequences of cerebral radionecrosis, which include brain abscess and acute hemorrhage, are also of chief concern.
R
EFERENCES1. Fischer AW, Holfelder H. Lokales Amyloid in Gehirn. Eine spatfolge von rontgenbestrahlungen. Dtsch Z Chir 1930;227: 475–83.
2. Glass JP, Hwang TL, Leavens ME, et al. Cerebral radiation necrosis following treatment of extracranial malignancies. Cancer 1984;54:1966–72.
3. Lee AW, Ng SH, Ho JH, et al. Clinical diagnosis of late temporal lobe necrosis following radiation therapy for nasopharyngeal carcinoma. Cancer 1988;61:1535–42. 4. Hu JQ, Guan YH, Zhao LZ, et al. Delayed radiation
encephalopathy after radiotherapy for nasopharyngeal cancer: a CT study of 45 cases. J Comput Assist Tomogr 1991;15:181–7. 5. Cheung M, Chan AS, Law SC, et al. Cognitive function of patients with nasopharyngeal carcinoma with and without temporal lobe radionecrosis. Arch Neurol 2000;57:1347–52. 6. Lee AW, Cheng LO, Ng SH, et al. Magnetic resonance imaging
in the clinical diagnosis of late temporal lobe necrosis following radiotherapy for nasopharyngeal carcinoma. Clin Radiol 1990; 42:24–31.
7. Tsui EY, Chan JH, Leung TW, et al. Radionecrosis of the temporal lobe: dynamic susceptibility contrast MRI. Neuroradiology 2000;42:149–52.
8. Tsui EY, Chan JH, Ramsey RG, et al. Late temporal lobe necrosis in patients with nasopharyngeal carcinoma: evaluation with combined multi-section diffusion weighted and perfusion weighted MR imaging. Eur J Radiol 2001;39: 133–8.
9. Lee AW, Ng SH, Tse VK, et al. Bilateral temporal lobectomy for necrosis induced by radiotherapy for nasopharyngeal carcinoma. Acta Oncol 1993;32:343–4.
10. Shaw PJ, Bates D. Conservative treatment of delayed cerebral radiation necrosis. J Neurol Neurosurg Psychiatry 1984;47: 1338–41.
11. Woo E, Lam K, Yu YL, et al. Cerebral radionecrosis: is surgery necessary? J Neurol Neurosurg Psychiatry 1987;50:1407–14. 12. Jen YM, Hsu WL, Chen CY, et al. Different risks of symptomatic
brain necrosis in NPC patients treated with different altered fractionated radiotherapy techniques. Int J Radiat Oncol Biol Phys 2001;51:344–8.
13. Wong ET. Recurrent cystic radiation necrosis of the brain. Oncol Rep 1998;5:685–7.
14. Chong VE, Fan YF. Radiation-induced temporal lobe necrosis. AJNR Am J Neuroradiol 1997;18:784–5.
15. Julow J, Slowik F, Kelemen J, et al. Late post-irradiation necrosis of the brain. Acta Neurochir (Wien) 1979;46:135–50. 16. Bederson JB, Harsh GRt, Walker JA, et al. Radiation-induced
bilateral cystic temporal lobe necrosis: reversal of memory deficit after fenestration and internal shunting: Case report. J Neurosurg 1990;72:503–5.
17. Dwyer J, Gilbert JJ, Heeneman H. Lethal delayed radiation necrosis of the brain as a complication of radiotherapy for cancer in the head and neck. J Otolaryngol 1985;14:301–4. 18. Matheja P, Rickert C, Weckesser M, et al. Scintigraphic pitfall:
delayed radionecrosis. Case illustration. J Neurosurg 2000; 92:732.
19. Vallee B, Malhaire JP, Person H, et al. Delayed cerebral pseudo-tumoral radionecrosis following scalp-tumor irradiation. Case report and review of literature. J Neurol 1984;231:135–40. 20. Kerob D, Kolb F, Margulis A, et al. Delayed cerebral
radionecrosis following radiation therapy of cutaneous squamous cell carcinomas of the head. Ann Dermatol Venereol 2002;129:41–5.
21. Hugon J, Vallat JM, Dumas M, et al. Cerebral radionecrosis after radiotherapy for frontal cutaneous epithelioma. Nouv Presse Med 1981;10:1072.
22. Ciaudo-Lacroix C, Lapresle J. Pseudo-tumoral form of delayed radionecrosis of the brain. Ann Med Interne (Paris) 1985;136: 137–41.
23. de Vries B, Taphoorn MJ, van Isselt JW, et al. Bilateral temporal lobe necrosis after radiotherapy: confounding SPECT results. Neurology 1998;51:1183–4.
24. Hsu YC, Ho KY, Kuo WR, et al. Cerebral radionecrosis with cystic degeneration following radiotherapy for nasal cavity squamous cell carcinoma: a case report. Kaohsiung J Med Sci 2004;20:308–12.
25. Baron SH. Brain radiation necrosis following treatment of an esthesioneuroblastoma (olfactory neurocytoma). Laryngoscope 1979;89:214–23.
26. Miyagami M, Maejima S, Satoh K, et al. Delayed radiation necrosis of the temporal lobe following radiation therapy of maxillary carcinoma. No To Shinkei 1989;41:623–30.
27. Jiang GL, Morrison WH, Garden AS, et al. Ethmoid sinus carcinomas: natural history and treatment results. Radiother Oncol 1998;49:21–7.
28. Tran TA, Fuller GN, Whitman GJ, et al. Radiologic-pathologic conferences of the University of Texas M.D. Anderson Cancer Center. Delayed cerebral radiation necrosis. AJR Am J Roentgenol 2003;180:70.
29. Iwai Y, Yamanaka K, Oda J, et al. Tracer accumulation in radiation necrosis of the brain after thallium-201 SPECT and [11C]methionine PET—case report. Neurol Med Chir (Tokyo) 2001;41:415–8.
30. Coghlan KM, Magennis P. Cerebral radionecrosis following the treatment of parotid tumors: a case report and review of the literature. Int J Oral Maxillofac Surg 1999;28:50–2. 31. Barcikowska M, Chodakowska M, Klimowicz I, et al. A case of
radionecrosis mimicking metastatic tumor of the cerebral hemisphere. Folia Neuropathol 1995;33:55–7.
32. Lee AW, Foo W, Chappell R, et al. Effect of time, dose, and fractionation on temporal lobe necrosis following radiotherapy for nasopharyngeal carcinoma. Int J Radiat Oncol Biol Phys 1998;40:35–42.
33. Lee AW, Law SC, Ng SH, et al. Retrospective analysis of nasopharyngeal carcinoma treated during 1976–1985: late
complications following megavoltage irradiation. Br J Radiol 1992;65:918–28.
34. Chandler A, Tucker FC, Herzberger EE. Late radiation necrosis of the brain. Wis Med J 1964;63:297–300.
35. Hopewell JW. The late vascular effects of radiation. Br J Radiol 1974;47:157–8.
36. Conomy JP, Kellermeyer RW. Delayed cerebrovascular consequences of therapeutic radiation. A clinicopathologic study of a stroke associated with radiation-related carotid arteriopathy. Cancer 1975;36:1702–8.
37. Keime-Guibert F, Napolitano M, Delattre JY. Neurological complications of radiotherapy and chemotherapy. J Neurol 1998;245:695–708.
38. Hopewell JW, Wright EA. The nature of latent cerebral irradiation damage and its modification by hypertension. Br J Radiol 1970;43:161–7.
39. Price RA, Jamieson PA. The central nervous system in childhood leukemia. II. Subacute leukoencephalopathy. Cancer 1975;35:306–18.
40. Byfield JE. Ionizing radiation and vincristine: possible neurotoxic synergism. Radiol Clin Biol 1972;41:129–38. 41. Lee AW, Kwong DL, Leung SF, et al. Factors affecting risk of
symptomatic temporal lobe necrosis: significance of fractional dose and treatment time. Int J Radiat Oncol Biol Phys 2002;53: 75–85.
42. Cheung MC, Chan AS, Law SC, et al. Impact of radionecrosis on cognitive dysfunction in patients after radiotherapy for nasopharyngeal carcinoma. Cancer 2003;97:2019–26. 43. Kahn D, Follett KA, Bushnell DL, et al. Diagnosis of recurrent
brain tumor: value of 201Tl SPECT vs 18F-fluorodeoxyglucose
PET. AJR Am J Roentgenol 1994;163:1459–65.
44. Chong VF, Rumpel H, Fan YF, et al. Temporal lobe changes following radiation therapy: imaging and proton MR spectroscopic findings. Eur Radiol 2001;11:317–24.
45. Leber KA, Eder HG, Kovac H, et al. Treatment of cerebral radionecrosis by hyperbaric oxygen therapy. Stereotact Funct Neurosurg 1998;70:229–36.
46. Cheng KM, Chan CM, Fu YT, et al. Brain abscess formation in radiation necrosis of the temporal lobe following radiation therapy for nasopharyngeal carcinoma. Acta Neurochir (Wien) 2000;142:435–40.
47. Cheng KM, Chan CM, Fu YT, et al. Acute hemorrhage in late radiation necrosis of the temporal lobe: report of five cases and review of the literature. J Neurooncol 2001;51:143–50. 48. Glantz MJ, Burger PC, Friedman AH, et al. Treatment of
radiation-induced nervous system injury with heparin and warfarin. Neurology 1994;44:2020–7.
49. Giglio P, Gilbert MR. Cerebral radiation necrosis. Neurologist 2003;9:180–8.