Kaohsiung J Med Sci September 2008 • Vol 24 • No 9 453
According to the Annual Data Report of the United States Renal Data System (USRDS) in 2004, Taiwan had the highest incidence of end-stage renal disease (ESRD) and the second highest prevalence globally [1]. This fact ap-pears to underline the marked impact of the ESRD pop-ulation on the health care budget in Taiwan, where less than 0.2% of the total population on dialysis treatment accounted for more than 7% of the total expenditure of
Received: Apr 10, 2008 Accepted: Oct 28, 2008 Address correspondence and reprint requests to: Dr Shang-Jyh Hwang, Division of Nephrology, Department of Internal Medicine, Kaohsiung Medical University Hospital, 100 Tzyou 1st Road, Kaohsiung 807, Taiwan.
E-mail: [email protected]
H
EALTH
-
RELATED
Q
UALITY OF
L
IFE IN
T
AIWANESE
D
IALYSIS
P
ATIENTS
:
E
FFECTS OF
D
IALYSIS
M
ODALITY
Lih-Wen Mau,1Herng-Chia Chiu,2Pi-Yu Chang,3Su-Chen Hwang,4and Shang-Jyh Hwang5,6
1Chronic Disease Research Group, Minneapolis Medical Research Foundation, Minneapolis,
Minnesota, USA, 2Institute of Healthcare Administration, College of Health Science, 3Center of
Administration Management, and 4Department of Nursing, Kaohsiung Medical University Hospital, 5Division of Nephrology, Department of Internal Medicine, and 6School of Renal Care,
College of Medicine, Kaohsiung Medical University, Kaohsiung, Taiwan.
Taiwan has the highest incidence and prevalence of end-stage renal disease worldwide. However, not many studies have focused on the influence of dialysis modality on health-related quality of life (HRQoL) for dialysis patients in Taiwan. This study intended to compare the differences in HRQoL between peritoneal dialysis (PD) and hemodialysis (HD) and to evaluate the effects of dialysis modality on patient HRQoL. A cross-sectional survey using the Taiwan-version 36-item short-form health survey questionnaire (SF-36) was completed by 244 dialysis patients (58 PD and 186 HD patients) at two hospital-based dialysis units in southern Taiwan. Patient characteristics, diagnoses and laboratory data were individually extracted from the annual survey and matched with primary HRQoL data. Multiple linear regression analysis was performed to evaluate the effects of dialysis modality on HRQoL. Compared with HD patients, PD patients had higher scores in six of the eight SF-36 subscales, including physical functioning, role limitations due to physical and emotional problems, bodily pain, vitality, and mental health. However, only role limitations due to emotional problems and bodily pain reached significant difference levels (p< 0.05). After control-ling for patient characteristics, comorbid conditions and laboratory values, the bodily pain score was 7.88 points higher for PD patients compared with HD patients, while the social functioning score was 9.00 points higher for HD patients compared with PD patients (p< 0.05). The present study provides cross-sectional confirmation for equivalent levels of HRQoL between PD and HD patients except for the subscales of bodily pain and social functioning. In addition to dialysis modality, HRQoL for dialysis patients may be more related to personal attributes, interactions with multiple diseases, social support and quality of care received. When informing patients about modality choices for dialysis, trade-offs should be discussed and individual preferences for specific aspects of HRQoL should be considered.
Key Words:health-related quality of life, hemodialysis, peritoneal dialysis, SF-36 (Kaohsiung J Med Sci 2008;24:453–60)
the National Health Insurance (NHI) program in 2002 [2]. Because of the increasing expense and resource utilization for ESRD patients, most discussions have focused on cost containment for dialysis-related ser-vices. Few studies have focused on health-related quality of life (HRQoL) for peritoneal dialysis (PD) and hemodialysis (HD) patients in Taiwan.
HD is considered a high-volume and high-cost treatment compared with PD. Overall, 96% of ESRD patients use HD instead of PD (high-volume) and the annual cost per person per year for HD is more than 30% higher than for PD (US$20,488 vs. US$15,295) in Taiwan [3]. The issue of HRQoL for HD versus PD patients is critical to future care planning and service utilization because Taiwan’s NHI operates with a global budget for dialysis treatments.
The importance of HRQoL in clinical research has been extensively discussed over recent decades and it is now widely accepted as an important indicator of health care treatment outcomes [4]. Quality of life of ESRD patients is influenced by the disease itself and by the type of alternative therapies a patient receives. Many studies on quality of life have been done on PD and HD patients around the world, with empirical evidence indicating that differences in HRQoL are associated with PD and HD treatments [5–12]. No consistent findings yet exist to show whether PD or HD treatments are associated with better HRQoL. Previous HRQoL studies of assessments of dialysis patients in Taiwan have used self-developed research instruments [13,14], which caused difficulties in mak-ing cross-national comparisons. Recent studies usmak-ing the SF-36 or the QoL questionnaire developed by the World Health Organization (WHOQoL) primarily focused on HD patients [15,16] or PD patients [17].
The present study compared the differences in HRQoL between PD and HD patients using the 36-item short-form health survey questionnaire (SF-36), Taiwan version, and examined the effects of dialysis modality on HRQoL, adjusting for patient character-istics, clinical diagnoses and laboratory variables.
M
ETHODSSample and data sources
The study design consisted of a cross-sectional, face-to-face interview survey using the SF-36, Taiwan version, on two hospital-based dialysis units, one in
a university hospital and one in a municipal teaching hospital, in Kaohsiung City. All registered dialysis patients of the two hospitals were included in the study (n= 244). All were stable dialysis patients who had been on dialysis for more than 3 months during the recruitment period. On average, the PD patients (n= 58) had received dialysis treatment for 39 months and the HD patients (n= 186) for 49 months.
Two sources of data were used for the study. Primary data were collected by the SF-36 survey over 3 months in 2000. For corresponding patient charac-teristics, clinical diagnoses and laboratory information, data from the 2000 annual survey performed by the Taiwan Society of Nephrology were used. Laboratory data were collected within the time frame in which the SF-36 survey took place. Patient characteristics, diag-noses and laboratory data were individually extracted and matched with the HRQoL data.
Measurement and study variables
The research instrument was the Taiwan version of the 36-item short-form health survey questionnaire (SF-36), which originated from the Medical Outcome Study [18]. The SF-36 has been widely used and vali-dated as a quality-of-life assessment instrument for general populations and for patients with kidney dis-eases cross-nationally [19–26].
The SF-36, Taiwan version, was developed by the Laboratory of Health Databank and Center for Popu-lation; the validity and reliability of the SF-36, Taiwan version, has been thoroughly examined in a nation-wide Health Survey Research study; item discrimi-native validity and internal reliability have reached acceptable levels [27]. Like the original SF-36, the Taiwan version comprises eight subscales: physical functioning (PF), role limitations due to physical prob-lems (RP), role limitations due to emotional probprob-lems (RE), social functioning (SF), bodily pain (BP), general health (GH), vitality (VT), and mental health (MH). A total score ranging from 0 to 100 is calculated for each domain, a higher score indicating a better quality-of-life state in that domain. The scores for the eight domains are further summarized into two measures: the Physical Component Scale (PCS) and the Mental Component Scale (MCS). The PCS and MCS scores are also converted into a 0–100-point scale [18].
In addition to HRQoL assessment, three types of study variables were derived from the Taiwan Society of Nephrology data set: patient characteristics, clinical
diagnoses and laboratory variables. Patient character-istics included age, gender, marital status, educational level and working status. Clinical diagnoses focused on the primary cause of ESRD and patients’ chronic conditions. The primary cause of ESRD was classified as diabetes and non-diabetes. Several major chronic diseases in ESRD patients were selected for the meas-urement of comorbid conditions, including cardio-vascular disease, renal osteodystrophy, liver disease, gastrointestinal disease, nervous system disease, pruritus and other systemic diseases. To consider the SF-36 scores in relation to important clinical aspects [28,29], the laboratory variables hematocrit, serum albumin and Kt/Vurea, were included in the analyses.
Erythropoietin treatment and length of time on dialysis were also considered. The laboratory data were col-lected at the time of the SF-36 survey.
Statistical techniques
The distributions of patient characteristics, clinical diagnoses and laboratory data were determined and compared by dialysis modality using χ2statistics for
the percentages of categorical variables or t statistics for the means of continuous variables. Unadjusted mean scores on the SF-36 subscales were compared for PD and HD patients by t tests. Multiple linear regression analysis was used to examine the effect of dialysis modality on the mean scores of the eight SF-36 domains and the summary scores of the PCS and MCS, adjusted for statistically significant factors that were found in the descriptive comparison of PD and HD patients, which included patient characteristics (age, employment status, educational level), primary cause of ESRD (diabetic vs. non-diabetic), laboratory data (hematocrit level, albumin level), and erythro-poietin treatment. The Kt/V value was excluded from regression analysis because its estimation was different between PD and HD patients.
R
ESULTSDescriptions of patient characteristics and
chronic conditions
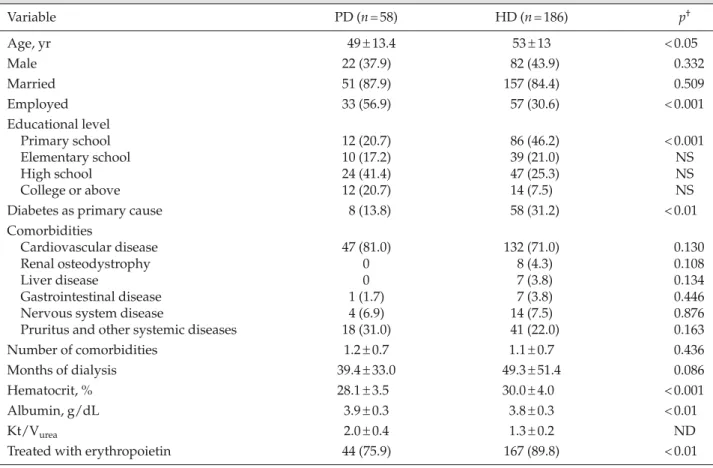
Table 1 shows the distributions of patient charac-teristics, chronic conditions, and laboratory data by dialysis modality. Compared with HD patients, PD patients were significantly younger (p<0.05), and a larger proportion of them were employed (p<0.001).
The distribution of education level was significantly different between PD and HD patients (p<0.001). More than 40% of HD patients only finished primary high school compared with 20.7% of HD patients (p<0.001). Table 1 also shows a significantly higher percent-age of HD patients with diabetes as the primary cause of ESRD (13.8% for PD vs. 31.2% for HD; p< 0.01). There was no significant difference in the prevalence of cardiovascular disease or other comorbidities be-tween PD and HD patients. Mean hematocrit value was higher for HD patients (p< 0.001), while the albu-min serum level was higher in the PD group (p< 0.01). The difference in the proportion of PD and HD patients who received erythropoietin treatment also reached the significant level (p< 0.01). Table 1 shows the values of Kt/V for PD and HD patients; however, no comparison of Kt/V values could be made because of different time frames of data collection. All the sta-tistically significant variables presented in Table 1 are included in the multiple regression models in Table 2.
Comparison of SF-36 scores of PD and
HD patients
Table 3 shows the mean scores (out of a possible 100) for the eight subscales and the two components of the SF-36 by dialysis modality. All scores for the eight SF-36 subscales, except SF and GH, were higher in PD than HD patients. No significant difference in the scores was found between HD and PD patients except on the RE and BP subscales. Compared with PD patients, HD patients reported higher scores for RE and BP (p< 0.05). The PCS and MCS scores were also higher in PD patients compared with HD patients, but differences were not statistically significant.
SF-36 scores of PD and HD patients
compared with the general population
The mean SF-36 subscale scores for the general popu-lation are also provided in Table 3. In general, patients receiving dialysis (PD and HD) reported lower scores reflecting physical function (e.g. PF and RP). The scores reflecting mental function (e.g. VT and MH) tended to be similar to those observed in the general population without kidney failure.
Comparison of PD and HD patients
between the US and Taiwan
We compared the present results to the study of Diaz-Buxo et al [11], as shown in the Figure. On the
Table 1.Patient characteristics and chronic conditions of peritoneal dialysis (PD) and hemodialysis (HD) patients* Variable PD (n= 58) HD (n= 186) p† Age, yr 49± 13.4 53± 13 < 0.05 Male 22 (37.9) 82 (43.9) 0.332 Married 51 (87.9) 157 (84.4) 0.509 Employed 33 (56.9) 57 (30.6) < 0.001 Educational level Primary school 12 (20.7) 86 (46.2) < 0.001 Elementary school 10 (17.2) 39 (21.0) NS High school 24 (41.4) 47 (25.3) NS College or above 12 (20.7) 14 (7.5) NS
Diabetes as primary cause 8 (13.8) 58 (31.2) < 0.01
Comorbidities
Cardiovascular disease 47 (81.0) 132 (71.0) 0.130
Renal osteodystrophy 0 8 (4.3) 0.108
Liver disease 0 7 (3.8) 0.134
Gastrointestinal disease 1 (1.7) 7 (3.8) 0.446
Nervous system disease 4 (6.9) 14 (7.5) 0.876
Pruritus and other systemic diseases 18 (31.0) 41 (22.0) 0.163
Number of comorbidities 1.2± 0.7 1.1± 0.7 0.436
Months of dialysis 39.4± 33.0 49.3± 51.4 0.086
Hematocrit, % 28.1± 3.5 30.0± 4.0 < 0.001
Albumin, g/dL 3.9± 0.3 3.8± 0.3 < 0.01
Kt/Vurea 2.0± 0.4 1.3± 0.2 ND
Treated with erythropoietin 44 (75.9) 167 (89.8) < 0.01
*Data presented as mean± standard deviation or n (%); †Student’s t test for continuous variables and χ2test for categorical variables, with p< 0.05 considered statistically significant. NS = no significant difference between the two groups; ND = not determined.
Table 2.Regression analysis of subscales and physical and mental components of the SF-36 (n= 233)*
PF RP BP GH VT SF RE MH PCS MCS
Age −0.630† −0.206 −0.114 −0.295† −0.270† −0.239† −0.308 −0.160 −0.189† −0.065
Working status 6.035 3.594 8.514† 4.635 10.079† 5.196 2.642 4.271 3.907† 2.135
Ref.: unemployed
Education level −2.025 13.993† 4.882 0.673 1.455 −1.273 9.131 0.748 1.402 0.899
Ref.: less than high school
Primary cause of end- −20.814† −21.843† −3.774 −10.547† −7.549† −12.907† −7.427 −7.461† −7.589† −2.264
stage renal disease Ref.: non-diabetic
patients
Hematocrit level −0.565 0.014 0.302 −0.183 −0.061 0.051 0.649 −0.113 −0.118 0.100 Albumin level 17.797† 0.426 7.617 1.045 8.977 13.960† −16.906 5.416 6.006† −0.198
Treated with EPO −2.128 −2.921 9.677 −2.194 −0.982 −0.570 6.290 −2.970 0.200 −0.216 Dialysis modality 4.610 7.785 −7.880† 7.728 6.270 9.004† −13.811 0.981 3.074 −0.244
Ref.: peritoneal dialysis
Adjusted R2(%) 37.1 10.5 12.6 10.0 16.2 17.6 3.7 8.2 28.0 2.1
*Each regression model was adjusted for age, gender, working status, education level, primary cause of diabetes mellitus, number of comorbidities, hematocrit and albumin level; †p< 0.05. PF = physical functioning; RP = role limitations due to physical problems; BP = bodily pain; GH = general health; VT = vitality; SF = social functioning; RE = role limitations due to emotional problems; MH = mental health; PCS = Physical Component Scale; MCS = Mental Component Scale; Ref. = reference group for comparison; EPO = erythropoietin.
physical subscales, the PF scores were similar between PD and HD patients in Taiwanese and US samples. However, PF scores of US PD and HD patients were much lower than in the present study (44.8 vs. 71.37 for PD, 41.4 vs. 65.11 for HD, p< 0.05). The HRQoL score for BP was very similar between US PD and HD patients, but significantly different between Taiwanese PD and HD patients (76.49 vs. 64.92, p< 0.05). On the mental subscales, the SF and MH scores for PD and HD patients in Taiwan were similar to the US scores. The VT score for US PD patients was 42.30 compared with 52.35 for Taiwanese PD patients. The significant difference in role limitations due to mental health prob-lems between Taiwanese PD and HD patients (58.17 vs. 42.67, p< 0.05) was not found in the US samples.
Regression analyses on HRQoL of
dialysis patients
The results of multiple regression analysis for the eight subscales and two components of the SF-36 are presented in Table 2. After controlling for patient
characteristics, chronic conditions and laboratory data, dialysis modality was significantly associated with BP and SF. The score for BP was 7.88 points higher for PD patients compared with HD patients, while the SF score was 9.00 points higher for HD patients compared with PD patients (p< 0.05). Across the regression models for each subscale, age and diabetes were associated with several of the SF-36 scales. The model for PF had the highest volume of variance explained (adjusted R2=
37.1%) and PD patients scored higher for PF. However, we found no significant difference in PCS between PD and HD patients in the adjusted regression models.
D
ISCUSSIONHRQoL is considered to be an important indicator of health care treatment outcomes. However, assessments of HRQoL in ESRD patients are few and have mainly focused on HD patients in Taiwan [14,15]. The present study is one of the few HRQoL studies of dialysis Table 3.Comparison of SF-36 scores between peritoneal dialysis (PD) and hemodialysis (HD) patients*
Subscale General population† PD (n= 51) HD (n= 182) p
Physical functioning (PF) 92.24± 16.16 71.37± 20.95 65.11± 28.84 0.087 Role-physical (RP) 83.65± 33.27 41.67± 39.58 39.84± 42.45 0.783 Bodily pain (BP) 84.84± 19.42 76.49± 22.72 64.92± 23.33 < 0.05 General health (GH) 69.29± 21.27 45.65± 22.79 48.12± 23.10 0.499 Vitality (VT) 68.27± 18.66 52.35± 22.86 51.76± 22.54 0.868 Social functioning (SF) 86.81± 17.05 63.97± 23.54 67.10± 21.84 0.375 Role-emotional (RE) 79.40± 36.07 58.17± 42.08 42.67± 43.95 < 0.05 Mental health (MH) 73.01± 16.55 64.78± 18.05 61.21± 19.34 0.238
Physical Component Scale (PCS) NA 41.75± 11.05 40.39± 12.26 0.476
Mental Component Scale (MCS) NA 43.84± 10.50 42.30± 10.61 0.360
*Data presented as mean±standard deviation; †mean score for each subscale for the general population was derived from Tseng et al [27]. 150 100 Scor e 50 0
Taiwan-PD Taiwan-HD US-PD US-HD
Physical functioning Role-physical Bodily pain General health Vitality Social functioning Role-emotional Mental health Figure.SF-36 physical subscales of peritoneal dialysis (PD) and hemodialysis (HD) patients: a comparison of the present study and US samples from the study of Diaz-Buxo et al [11]. Data are expressed as mean (95% confidence interval).
patients that compares HRQoL between PD and HD patients in Taiwan. According to the present find-ings, PD patients scored higher in six of the eight sub-scales of the SF-36. It seems that the selection of PD may have benefits in terms of HRQoL. However, it should be noted that HRQoL data are descriptive and self-reported. Comparison of the results between PD and HD patients needs to be interpreted cautiously. Because only the differences in the mean scores for RE and BP are significant between the PD and HD patients, it is more reasonable to conclude that PD and HD patients have equivalent levels of HRQoL [10,11]. In general, PD and HD patients in the US had equivalent levels of HRQoL [11]. The crude significant differences in the scores for BP and RE were not found in the US samples. Compared with the US dialysis samples of PD and HD patients, our study patients had better HRQoL in the components of physical health; however, the HRQoL in the components of mental health was relatively lower. Of note, the com-parison of the present study with the US samples is still descriptive and the US HD sample had a higher mean age, and included more males and more diabetic patients [11]. Comparing our data to another HD sam-ple in Taiwan [15], our HD samsam-ple is younger and has better HRQoL in the PCS and MCS. However, our HD sample has lower scores for the subscales of RE, RP and BP. It might be possible that younger HD patients tend to have higher expectation of role playing.
Adjusting for patient characteristics, primary cause of ESRD and laboratory data, SF and BP became the only two subscales that were significantly associated with dialysis modalities. The SF score was 9 points higher for HD compared with PD patients, which might be because PD patients experienced greater distress and isolation owing to a lack of social support from similar patients and medical staff compared with the in-center HD patients [10]. On the other hand, BP score was 7.88 points lower for HD compared with PD patients. As reported by Merkus et al for the NECOSAD Study group [20], PD patients may see themselves as less physically impaired and self-perceive a lower degree of BP.
In considering the BP subscale it is interesting to note that working status is significantly associated with the HRQoL score for BP, in addition to dialysis modal-ity. Similar to the study by Blake et al in Ireland [21], unemployed ESRD patients scored significantly lower than employed patients for BP and VT in our study
sample. It is possible that maintaining working status is one concern for ESRD patients in selecting a dialysis modality. However, the design of our cross-sectional study could not compare the direct and indirect effects between dialysis modality and working status and their effects on HRQoL in ESRD patients.
Independent of dialysis modality, physical, psy-chologic and social functioning are highly interrelated [5]. Most dialysis patients were selected for PD or HD by their physicians based on diagnosis or comorbidity. Consistent with previous studies, the present findings indicate that dialysis patients with diabetes as the primary cause of ESRD had significantly lower scores on six subscales of the SF-36 [12]. Management and care of dialysis patients with diabetes may be more important than dialysis modality to improve the HRQoL of such patients. Indeed, there is an interaction effect of dialysis modality and diabetes on the HRQoL of SF and BP (data not shown).
The present study is limited to a cross-sectional study with a relatively small sample size. The results on the effects of dialysis modality may not be fully generalized to all dialysis patients in Taiwan. For future research, a longitudinal study with a larger sample size is suggested to extend the implications of the findings and to examine the interrelationships between dialysis modality and physical and psycho-social functioning of chronic dialysis patients [29]. Aside from these findings, there are many other fac-tors associated with HRQoL that we did not include in our analyses, such as family support, health behav-iors and socioeconomic status, which make cross-national or cross-study comparisons difficult.
In conclusion, the present study provides cross-national confirmation of equivalent levels of HRQoL between PD and HD patients, except for the BP and SF subscales. In addition to dialysis modality, HRQoL for dialysis patients may be more related to personal attributes, interactions of multiple diseases, social support and quality of care received. When informing patients about modality choices, trade-offs should be discussed and individual preferences for specific aspects of HRQoL should be considered.
A
CKNOWLEDGMENTSThe authors wish to thank the members of the Chronic Disease Research Group’s publication group
for editorial assistance and advice, and for assistance with manuscript preparation. We also appreciate the help provided by the nurses of the dialysis units of the study hospitals for primary data collection.
R
EFERENCES1. US Renal Data System. USRDS Annual Data Report, 2004. The National Institutes of Health, National Institute of Diabetes, Digestive and Kidney Diseases, Bethesda, MD, USA.
2. Bureau of National Health Insurance, Department of Health, Executive Yuan, Taiwan, R.O.C. National Health
Insurance Annual Statistical Report for 2002. Taipei:
Department of Health, Executive Yuan, Taiwan, R.O.C., 2003.
3. Mau LW, Hwang SJ, Lin JY, et al. Establishment of
Risk-adjusted Model for End-stage Renal Disease Patients. Based on Kao-Ping Areas. Taipei: Department of Health,
Executive Yuan, Taiwan, R.O.C., 2003.
4. Patrick DL, Deyo RA. Generic and disease-specific measures in assessing health status and quality of life.
Med Care 1992;27(Suppl 3):S217–32.
5. Valderabano F, Jofre R, Lopez-Gomez JM. Quality of life in end-stage renal disease patients. Am J Kidney Dis 2001;38:443–64.
6. Manns B, Johnson JA, Taub K, et al. Quality of life in patients treated with hemodialysis or peritoneal dialy-sis: what are the important determinants? Clin Nephrol 2003;60:341–51.
7. Wasserfallen JB, Halabi G, Saudan P, et al. Quality of life on chronic dialysis: comparison between haemodialysis and peritoneal dialysis. Nephrol Dial Transplant 2004;19: 1594–9.
8. Gokal R, Figueras M, Olle A, et al. Outcomes in peri-toneal dialysis and hemodialysis: a comparative assess-ment of survival and quality of life. Nephrol Dial
Transplant 1999;14(Suppl 6):24–30.
9. Harris SA, Lamping DL, Brown EA, et al. Clinical out-comes and quality of life in elderly patients on peri-toneal dialysis versus hemodialysis. Perit Dial Int 2002; 22:463–70.
10. Griffin KW, Wadhwa NK, Friend R, et al. Comparison of quality of life in hemodialysis and peritoneal dialysis patients. Adv Perit Dial 1994;10:104–8.
11. Diaz-Buxo JA, Lowie EG, Lew NL, et al. Quality of life evaluation using short form 36: comparison in hemo-dialysis and peritoneal hemo-dialysis patients. Am J Kidney Dis 2000;35:293–300.
12. Lee HB, Song KI, Kim JH, et al. Dialysis in patients with diabetic nephropathy: CAPD versus hemodialysis.
Perit Dial Int 1996;16(Suppl 1):S269–74.
13. Chen ML, Ku NP. Health-related quality of life for dial-ysis patients and its associated factors. Taiwan Nursing
Research 1996;6:393–404.
14. Hong CJ. A comparison of quality of life between peri-toneal and hemodialysis patients. Acta Nephrologica,
Taiwan Society of Nephrology 1992;12:83–7.
15. Chiang CK, Peng YS, Chiang SS, et al. Health-related quality of life of hemodialysis patients in Taiwan: a mul-ticenter study. Blood Purif 2004;22:490–8.
16. Yang SC, Kuo PW, Wang JD, et al. Quality of life and its determinants of hemodialysis patients in Taiwan mea-sured with WHOQOL-BREF (TW). Am J Kidney Dis 2005;46:635–41.
17. Chen YC, Hung KY, Kao TW, et al. Relationship between dialysis adequacy and quality of life in long-term peritoneal dialysis patients. Perit Dial Int 2000;20: 534–40.
18. Ware JE, Sherbourne CD. The MOS 36-item short-form health survey (SF-36): conceptual framework and item selection. Med Care 1992;30:473–83.
19. Mingardi G, Cornalba L, Cortinovis E, et al. Health-related quality of life in dialysis patients: a report from an Italian study using the SF-36 Health Survey. Nephrol
Dial Transpl 1999;14:1503–10.
20. Merkus MP, Jager KJ, Dekker FW, et al. Quality of life in patients on chronic dialysis: self-assessment 3 months after the start of treatment. The NECOSAD Study Group. Am J Kidney Dis 1997;29:584–92.
21. Blake C, Codd MB, Cassidy A, et al. Physical function, employment and quality of life in end-stage renal dis-ease. J Nephrol 2000;13:142–9.
22. Loos C, Briancon S, Frimat L, et al. Effects of end-stage renal disease on the quality of life older patients. J Am
Geriatr Soc 2003;51:229–33.
23. Franke GH, Reimer J, Philipp T, et al. Aspects of qual-ity of life through end-stage renal disease. Qual Life Res 2003;12:103–15.
24. Maor Y, King M, Olmer L, et al. A comparison of three measures: the time trade-off technique, global health-related quality of life and the SF-36 in dialysis patients.
Clin Epidemio 2001;54:565–70.
25. Sesso R, Rodrigues-Neto JF, Ferraz MB. Impact of socioeconomic status on the quality of life of ESRD patients. Am J Kidney Dis 2003;4:186–95.
26. Isotani S, Fujisawa M, Ichikawa Y, et al. Quality of life of living kidney donors: the short-form 36-item health questionnaire survey. Urology 2002;60:588–92.
27. Tseng HM, Lu JFR, Tsai YJ. Assessment of health-related quality of life in Taiwan (I): norming and vali-dation of SF-36 Taiwan version. Taiwan J Public Health 2003;22:512–8.
28. Merkus MP, Jager KJ, Dekker FW, et al. Predictors of poor outcome in chronic dialysis patients: the Netherlands Cooperative Study on the adequacy of dialysis (The NECOSAD Study Group). Am J Kidney Dis 2002;35: 69–79.
29. Allen KL, Miskulin D, Yan G, et al. Association of nutritional markers with physical and mental health status in prevent hemodialysis patients from the HEMO Group. J Ren Nutr 2002;12:160–9.
收文日期:97 年 4 月 10 日 接受刊載:97 年 10 月 28 日 通訊作者:黃尚志醫師 高雄醫學大學附設醫院腎臟內科 高雄市 807 三民區自由一路 100 號