Taiwan J Obstet Gynecol • September 2010 • Vol 49 • No 3 385 ■ RESEARCH LETTER ■
A 34-year-old primigravid woman presented at 29 weeks of gestation for evaluation of fetal ascites and an intra-abdominal echogenic cystic mass (Figure 1) in one twin of a twin pregnancy. The woman had not under-gone any assisted reproductive technology. Aspiration of the ascites and the cystic mass revealed multiple epithelial cells and cytogenetic analysis demonstrated a 46,XX karyotype in the affected co-twin. Ultrasound following aspiration showed a distended vagina con-necting to the uterine cavity and compressing the uri-nary bladder (Figure 2). Ultrafast magnetic resonance imaging (MRI) of the affected co-twin revealed mas-sive ascites, a compressed urinary bladder, a distended vagina, a dilated uterus, and a dilated distal colon, consistent with a diagnosis of persistent cloaca with hydrometrocolpos and ascites (Figure 3). The unaffected co-twin (1,306 g) and affected co-twin (2,108 g) were delivered uneventfully by cesarean section at 31 weeks of gestation. Both twins had a karyotype of 46,XX. A zygosity test determined dizygosity. The affected co-twin had meconium peritonitis, urinary ascites, and a per-sistent cloaca. The urinary, genital, and intestinal tracts converged into a cloacal canal with a single opening at the perineum. The ascites was caused by drainage of the urine into the abdominal cavity via the vagina, the
uterus and the Fallopian tubes, as well as by irritation of the peritoneum by urine and meconium. Hydrometro-colpos was caused by fluid accumulation resulting from distal vaginal obstruction through backward pres-sure from the cloacal canal. The hydrometrocolpos compressed the bladder causing partial bladder outlet obstruction. Dilation of the distal colon was caused by direct compression from the hydrometrocolpos and narrowing of the rectal communication. The affected infant was doing well at 1 year and 6 months of age, after corrective reconstructive surgery.
A persistent cloaca results from failure or maldevel-opment of the urorectal septum that divides the urogen-ital sinus and anorectal canal [1]. Hydrometrocolpos
P
RENATAL
D
IAGNOSIS OF
P
ERSISTENT
C
LOACA
W
ITH
H
YDROMETROCOLPOS AND
A
SCITES BY
M
AGNETIC
R
ESONANCE
I
MAGING IN
O
NE
F
ETUS OF
A
D
IZYGOTIC
T
WIN
P
REGNANCY
Chih-Ping Chen1,2,3,4,5,6*, Yu-Peng Liu7,8, Tung-Yao Chang9, Fuu-Jen Tsai4,10, Chen-Yu Chen1, Pei-Chen Wu1, Teresa Hsiao-Tien Chen11, Wayseen Wang2,12
Departments of1Obstetrics and Gynecology, 2Medical Research and 7Radiology, Mackay Memorial Hospital, 5Institute of Clinical and Community Health Nursing, 6Department of Obstetrics and Gynecology,
National Yang-Ming University, 8Mackay Medicine, Nursing and Management College, 11Taipei American School, 9Taiji Fetal Medicine Center, and 12Department of Bioengineering, Tatung University, Taipei, 3Department of
Biotechnology, Asia University, 4School of Chinese Medicine, College of Chinese Medicine, China Medical University, 10Departments of Medical Genetics and Medical Research, China Medical University Hospital, Taichung, Taiwan.
*Correspondence to: Dr Chih-Ping Chen, Department
of Obstetrics and Gynecology, Mackay Memorial Hospital, 92, Section 2, Chung-Shan North Road, Taipei, Taiwan.
E-mail: [email protected] Accepted: October 9, 2009
u
v
Figure 1.Prenatal ultrasound at 29 weeks of gestation show-ing fetal ascites with an intraabdominal echogenic cystic mass. u= uterus; v = vagina.
is caused by accumulated secretions from the repro-ductive glands resulting from obstruction of the vagina by an intact hymen, a midplane transverse vaginal septum or vaginal atresia, and/or from accumulation of urine caused by a stenotic urogenital sinus, associ-ated vesicovaginal fistulas, vesicouterine fistulas and urethrovaginal fistulas, or cloacal anomalies [2]. Hydrometrocolpos may present in association with a variety of malformations and syndromes, such as cloacal dysgenesis sequence, McKusick-Kaufman syndrome, Ellis-van Creveld syndrome, and Bardet-Biedl syndrome [3–5]. Fetal hydrometrocolpos secondary to a cloacal anomaly can be identified by complementary MRI [6–8]. A dizygotic twin pregnancy with a persistent cloaca in one fetus is very rare. Subramanian [9] suggested that the rectal signal caused by retained meconium on fetal MRI is an important imaging marker of cloacal anom-aly in association with hydrometrocolpos, as clearly demonstrated in the current case. The MRI findings in this case were in accordance with previous observa-tions suggesting that MRI provides useful information in patients with a dilated distal colon in addition to hydrometrocolpos and ascites, thus facilitating the prenatal diagnosis of cloacal anomalies.
Acknowledgments
This work was supported by research grants NSC-96-2314-B-195-008-MY3 and NSC-97-2314-B-195-006-MY3 from the National Science Council, and MMH-E-98004 from Mackay Memorial Hospital, Taipei, Taiwan.
References
1. Petrikovsky BM, Walzak MP Jr, D’Addario PF. Fetal cloacal anomalies: prenatal sonographic findings and differential diagnosis. Obstet Gynecol 1988;72:464–9.
2. Chen CP, Liu FF, Jan SW, Chang PY, Lin YN, Lan CC. Ultrasound-guided fluid aspiration and prenatal diagnosis of duplicated hydrometrocolpos with uterus didelphys and septate vagina. Prenat Diagn 1996;16:572–6.
3. Schaap C, de Die-Smulders CE, Kuijten RH, Fryns JP. McKusick-Kaufman syndrome: the diagnostic challenge of abdominal distension in the neonatal period. Eur J Pediatr 1992;151:583–5.
4. Yapar EG, Ekici E, Aydogdu T, Senses E, Gökmen O. Diagnos-tic problems in a case with mucometrocolpos, polydactyly, congenital heart disease, and skeletal dysplasia. Am J Med
Genet 1996;66:343–6.
5. Sahinoglu Z, Mulayim B, Ozden S, et al. The prenatal diag-nosis of cloacal dysgenesis sequence in six cases: can the termination of pregnancy always be the first choice? Prenat
Diagn 2004;24:10–6.
6. Hayashi S, Sago H, Kashima K, et al. Prenatal diagnosis of fetal hydrometrocolpos secondary to a cloacal anomaly by magnetic resonance imaging. Ultrasound Obstet Gynecol 2005; 26:577–9.
7. Hung YH, Tsai CC, Ou CY, Cheng BH, Yu PC, Hsu TY. Late prenatal diagnosis of hydrometrocolpos secondary to a cloacal anomaly by abdominal ultrasonography with com-plementary magnetic resonance imaging. Taiwan J Obstet
Gynecol 2008;47:79–83.
8. Liu YP, Chen CP. Fetal MRI of hydrometrocolpos with sep-tate vagina and uterus didelphys as well as massive urinary ascites due to cloacal malformation. Pediatr Radiol 2009; 39:877.
9. Subramanian S. Importance of rectal signal on fetal mag-netic resonance imaging in patients having hydrometrocol-pos. Taiwan J Obstet Gynecol 2008;47:375.
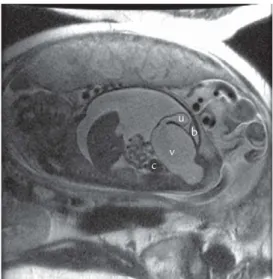
Taiwan J Obstet Gynecol • September 2010 • Vol 49 • No 3 386 C.P. Chen, et al u b v c
Figure 3. Magnetic resonance imaging showing a com-pressed urinary bladder (b), a distended vagina (v), a dilated uterus (u) and a dilated distal colon (c).
u b
v
Figure 2.Ultrasound following aspiration showing a distended vagina (v) connecting to the uterine cavity (u) and compressing the urinary bladder (b).