Allergic rhinitis and associated risk of migraine among children: A nationwide population-based cohort study
I-Chung Wang, MD1; Jeng-Dau Tsai, MD2,3; Cheng-Li Lin, MS4,5; Te-Chun Shen, MD6,7; Tsai-Chung Li, PhDd5; Chang-Ching Wei, MD1,7
1Children’s Hospital, China Medical University Hospital, Taichung, Taiwan; 2Department of pediatrics, Chung Shan Medical University Hospital, Taichung, Taiwan;
3Institute of medicine, Chung Shan Medical University, Taichung, Taiwan;
4Management Office for Health Data, China Medical University Hospital, Taichung, Taiwan;
5Institute of Biostatistics, China Medical University, Taichung, Taiwan;
6Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, China Medical University Hospital, Taichung, Taiwan
7College of Medicine, China Medical University, Taichung, Taiwan;
Address correspondence to Chang-Ching Wei
China Medical University Hospital, Taichung, Taiwan;
College of Medicine, China Medical University, Taichung, Taiwan; No2, Yu-Der Road
Taichung 40402, Taiwan
Tel.: +886-4-22052121-4639; Fax: 886-4-2203-2798 E-mail: [email protected]
Running title: migraine in allergic rhinitis Keywords: allergic rhinitis, migraine Table: 6
Figure: 1
Word count: abstract 250, text 2274
Welfare Clinical Trial and Research Center of Excellence (MOHW104-TDU-B-212-113002), China Medical University Hospital, Academia Sinica Taiwan Biobank, Stroke Biosignature Project (BM104010092), NRPB Stroke Clinical Trial Consortium (MOST 103-2325-B-039 -006), Tseng-Lien Lin Foundation, Taichung, Taiwan, Taiwan Brain Disease Foundation, Taipei, Taiwan, and Katsuzo and Kiyo Aoshima Memorial Funds, Japan.
Financial Disclosure: The authors have indicated they have no financial relationships relevant to this article to disclose.
Conflict of Interest: None. Author’s contributions
I-Chung Wang and Jeng-Dau Tsai made equal contribution to this study.
I-Chung Wang, Jeng-Dau Tsai, Chang-Ching Wei, and Te-Chun Shen conceptualized and designed the study, drafted the manuscript, and approved the final manuscript as submitted.
Cheng-Li Lin, Tsai-Chung Li conducted the initial analyses, reviewed and revised the manuscript, and approved the final manuscript as submitted.
Chang-Ching Wei coordinated and supervised the data collection, critically reviewed the manuscript, and approved the final manuscript as submitted.
Abstract
Background: Increased frequency of migraine was reported in adults with allergic rhinitis (AR). Although migraine is less common in children than in adults, it can begin in early childhood and persist into adulthood. We conducted this population-based cohort study to investigate the incidence and subsequent risk of migraine in children with AR.
Methods: From 2000 to 2007, 461850 children with recently diagnosed AR and 460718 non-AR controls were included in the study. By the end of 2008, incidences of migraine in both cohorts, the AR to non-AR cohort hazard ratios (HRs), and confidence intervals (CIs) were measured.
Results: The incidence of migraine during the study period was 3.2-fold higher in the AR cohort (95% CI: 2.97–3.46) than in the non-AR cohort (11.4 vs. 3.49 per 10000 person-years). The risk was greater for boys than for girls, and for children aged <6 years. The HR for migraine in children with AR was 1.44 (95% CI: 1.31–1.58) for those with ≤2 annual AR related medical visits, whereas, 14.8 (95% CI: 13.6–16.2) for those with >4 visits (P < 0.0001, the trend test). The risk of migraine development in the AR cohort was highest within the first year after AR diagnosis (HR: 4.89; 95% CI: 3.98–6.00). Children with AR were more likely to have migraine without aura than migraine with aura.
Conclusions: Children with AR had a higher incidence and subsequent risk of migraine. Physicians should be more aware of migraine in children with AR who complain of headache.
Introduction
Allergic rhinitis (AR) is a common allergic disease among children, affecting 14.3–61.9% of the pediatric population.1-3 AR frequently occurs with other
comorbidities, such as asthma, middle ear effusions, sinusitis, lymphoid hypertrophy with obstructive sleep apnea, and headache.4-6 Children with concurrent symptoms of AR and headache are commonly diagnosed with sinus headaches in clinical settings. 7, 8 However, when the headache occurs recurrently, migraine is the most probable
differential diagnosis.8 Migraine has a great effect on a child’s quality of life,
including increased instances of absence from school , learning disabilities, decreased interactions with family members, and decreased socialization with peers.9, 10 In addition, migraine may persist into adulthood.11 Therefore, identifying the triggering factors and underlying mechanisms of migraine is important to prevent and treat the disease. Migraine is a neurovascular pain syndrome,12, 13 which involves alteration of brain excitability, intracranial arterial dilatation, sensitization of the trigeminovascular system, and neurogenic inflammation in genetically susceptible individuals.12-15 The levels of proinflammatory mediators, such as histamine, prostaglandins F2a, and leukotrienes elevate during episodes of migraine.16-19 Interestingly, these mediators also play a crucial role in AR.20 Moreover, migraine frequently accompanied by sinus-associated symptoms, such as runny nose, congestion, and ocular symptoms.8
Previous studies reported a high prevalence of migraine in patients with AR.
However, these studies, with a limited number of patients, are cross-sectional studies and mainly focus on adults.21-23 The exact incidence and subsequent risk of migraine in children with AR remains unknown. To investigate whether AR is a risk factor for childhood migraine, we conducted a population-based cohort study with the
hypothesis that children with AR have a greater subsequent risk for migraine than those without AR.
Materials and methods
Data Sources
In this population-based cohort study, data were obtained from reimbursement claims of the universal National Health Insurance Research Database (NHIRD). This claims data are available from Taiwan’s National Health Insurance (NHI), which is a
government-run, single-payer, modest cost-sharing program, covering almost all citizens and contracting with all hospitals in Taiwan.24,25 We used a dataset consisting of a randomly selected sample of half of all insured children in Taiwan.25-27 Because of personal electronic data privacy regulations, the insurants’ records are encrypted before being released to researchers; thus, informed consent was not required in this study. Although the identification information was scrambled, this study also received approval from the Institutional Review Board at China Medical University Hospital (CMU-REC-101-012). The International Classification of Disease, Ninth Revision, Clinical Modification (ICD-9-CM) was used to for diagnosis.
Study Design and Subjects
We identified patients aged <18 years with newly diagnosed AR between 2000 and 2007 as the AR cohort. To improve diagnostic reliability and avoid overestimation of incidence, children with AR were defined as at least three records with ICD-9-CM code 477 in any diagnosis field of inpatient claims or ambulatory claims.25,26 Baseline was set as the date of AR diagnosis. In this study, we used the method of “1: 1” matching to screen the control subjects in order to control the potential confounders.
Hence, we randomly selected one non-AR children for every AR child using frequency matching by sex, age (in 1-year intervals), urbanization of residential area and baseline year. Migraine was defined as at least two records with ICD-9-CM code 364 in any diagnosis field of inpatient claims or ambulatory claims. Subjects with a history of migraine before baseline or those lacking information on age, sex, or urbanization of residence area were excluded. The comorbidities of AR and migraine were identified and defined by ICD-9-CM code, including chronic rhinosinusitis (473), obstructive sleep apnea (327.23), anxiety (300), depression (311), obesity (278), hypertension (401-405).28 All subjects were followed up until migraine diagnosis, death, loss to follow-up, withdrawal from the insurance system, or the end of 2008.
Statistical analysis
In this cohort study, we used the person-years to be the denominator for estimating the incidence rate under considering about the individual follow-up duration in the study. The date of diagnosis of AR was defined as the index date used to initiate follow-up person-years measurement. The follow-up person-years were measured for each child from the index date to the date the children had the diagnosis of migraine, or censored because of loss to follow-up, or death, or withdraw from the insurance
system, or the end of 2008. Follow-up person-years were used to estimate the incidence density rates (IR) and hazard ratios (HRs) of migraine for the AR cohort, which were compared with those of the non-AR cohort based on age, sex, and urbanization. HR was determined using the Cox proportional hazard regression model. The Cox model was also used to estimate the HR of migraine associated with the annual mean medical visits for AR. Furthermore, we analyzed if the association varied with the length of the follow-up period after AR diagnosis. A Kaplan–Meier plot showed the probability of migraine-free survival, and the log-rank test was used to test the difference between the AR and non-AR cohorts. We performed all data analyses using the SAS statistical software (version 9.2 for Windows; SAS Institute Inc., Cary, NC). Kaplan–Meier survival curves were plotted using the R software (version 2.14.1; R Development Core Team, Vienna, Austria). A 2-sided p-value <0.05 was considered statistically significant.
Results
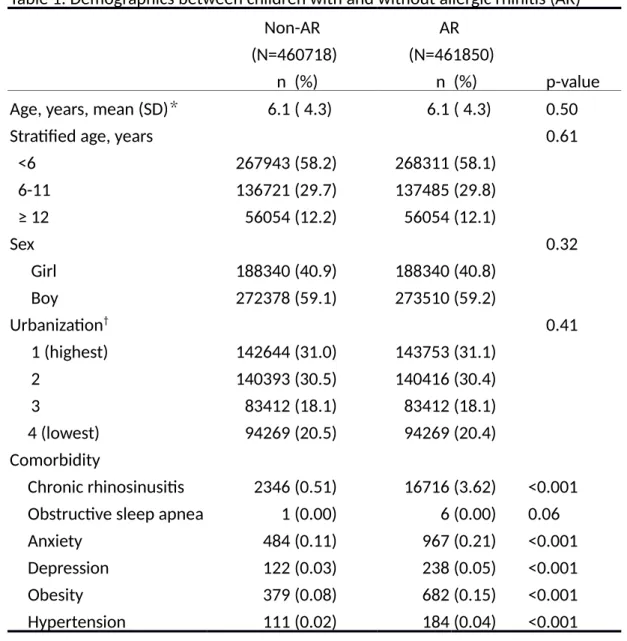
A total of 461850 subjects in the AR cohort and 460718 in the non-AR cohort were enrolled in this study (Table 1). Most (58.1%) of the subjects were aged <5 years. The AR cohort had more boys (59.2%) and residents of highly urbanized areas (61.5 %). Figure 1 illustrates the migraine-free survival rate of the AR cohort compared with that of the non-AR cohort. The migraine-free survival rate was significantly lower in the AR cohort compared to the non-AR cohort (Fig. 1, log-rank test, P < 0.001). The incidence of migraine was 3.2-fold higher in the AR cohort than in the non-AR cohort (11.4 vs. 3.49 per 10000 person-years; Table 2). An age-specific analysis showed that the incidence of migraine was significantly increased with age in both the cohorts. The adjusted Hazard ratio (HR) for migraine decreased from 3.75 (95% CI: 3.24– 4.34) for subjects aged <6 years to 3.17 (95% CI: 2.69–3.74) for those aged ≥12 years in the AR cohort compared to the non-AR cohort. A sex-specific analysis showed that the prevalence of migraine was approximately 1.5-fold higher in girls in both the cohorts. In contrast, the adjusted HR (3.32; 95% CI: 2.97–3.71) for migraine was higher for boys in the AR cohort compared to the non-AR cohort. Urbanization level-specific analyses showed that the incidence rate of migraine was highest for children living in areas of least urbanization. In table 3, an age-specific analysis showed that the incidence rates of migraine in girls were 6.29, 20.9, and 46.9 per 10000 person-years in age groups of <6, 6–11, and ≥12 person-years, respectively and that in boys were 5.73, 13.5, and 21.3 per 10000 person-years in age groups of <6, 6–11, and ≥12 years, respectively. The HR of migraine in girls was 8.22 (95% CI: 7.09–9.52) in age group of ≥12 years compared to age group of <6 years in girls, and 3.92 (95% CI: 3.34– 4.59) in boys. Table 4 shows the association between the frequency of medical visits
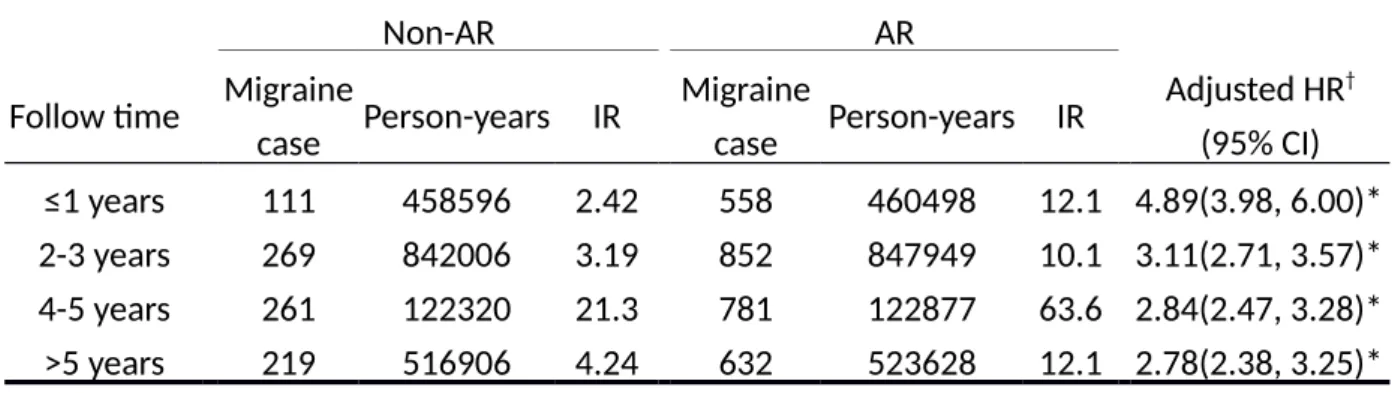
per year for AR and the incidence of migraine. Compared with the non-AR cohort, the risk of migraine in the AR cohort increased from 1.44 (95% CI: 1.31–1.58) for those with ≤2 visits to 14.8 (95% CI: 13.6–16.2) for those with >4 visits (trend test, P < 0.0001). This pattern of increased risks was similar for both genders (Table 4). Table 5 describes the risk of migraine stratified by median follow-up duration. The risk of migraine was highest among the subjects in the AR cohort who were followed up during the first year of migraine diagnosis (HR = 4.89; 95% CI: 3.98–6.00), and the risk of migraine decreased with time. In AR cohort, 281 children (10%) were
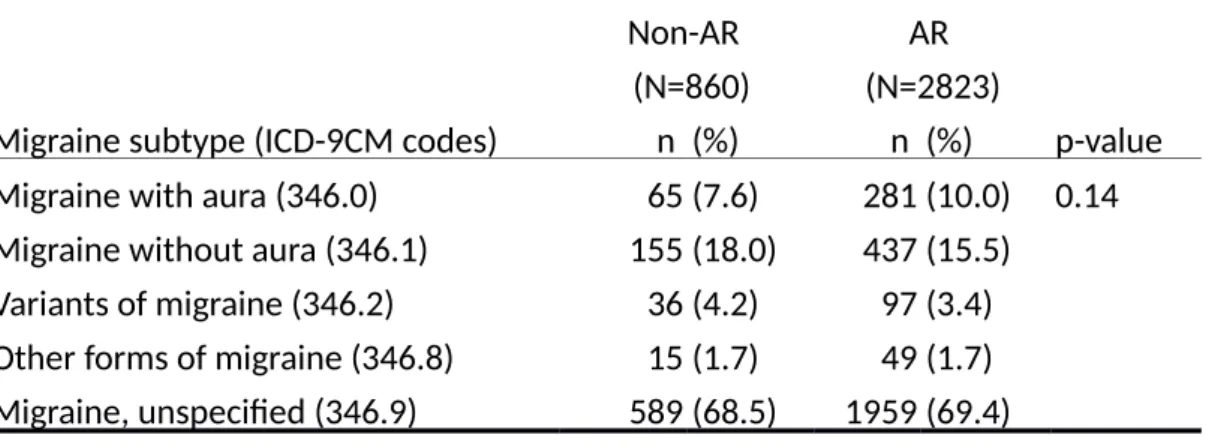
migraine with aura and 437 children (15.5%) were migraine without aura; In non-AR cohort, 65 children (7.6%) were migraine with aura and 155 children (18%) were migraine without aura (P =0.14) (Table 6).
Discussion
This is the first population-based cohort study that provides evidence of the incidence and relative risk of migraine in children with AR. Previous studies have reported high prevalence of migraine in AR patients. Ku et al. reported migraine in 34% of AR patients and in 4% of non-AR controls.21 Similarly, Saberi et al. and Ozturk et al. observed a higher prevalence of migraine in the AR patients than in non-AR controls.22,23 However, these were hospital-based and cross-sectional studies with limited numbers of patients, where no causal relationship was confirmed. In addition, these studies essentially focused on adult patients,21-23 and the exact incidence rate and relative risks of migraine in children with AR is not clear. Our results suggest that children with AR are more likely to develop migraine regardless of sex, age, and urbanization of living area. An earlier onset of AR showed an increased risk of migraine. The risk of migraine was greater within the first year of AR diagnosis. In addition, children with AR who have frequent AR-related medical visits had relatively higher risks of migraine attack. Thus, the physicians need to be aware of migraine symptoms when children are diagnosed with AR.
Although migraine is less common in children than in adults, it can begin in childhood, and increase in prevalence with age from 3% in young children to 15% in adolescents.29-33 Our study showed that the incidence rate of childhood migraine was 3.49 of 10000 person-years in the non-AR cohort and 11.4 of 10000 person-years in
the AR cohort. Further, the results suggest that the incidence of migraine increases with age, peaking in adolescence with a 6-fold increase from that in pre-school children, in both the cohorts. The incidence rate of migraine increased with age in both genders, with equal gender distribution in children aged <12 years, and female preponderance thereafter. Consistent with previous study, the incidence of migraine is higher among girls than boys after the onset of the menarche.34 Puberty is associated with pulsatile release of gonadotropin releasing hormone (GnRH) from the
hypothalamus. It is considered that the resetting of hypothalamic hormones plays an important role in the increased prevalence of migraine at puberty,35 and alters the trigeminovascular system, which is the main neural pathway involved in migraine.12 Our study shows the highest incidence rate of childhood migraine in children living in less urbanized areas. The relation between childhood migraine and population density in different living areas has not been well documented.
Our study indicates that children with an early onset of AR are at higher risk to develop migraine in their later life, suggesting that the physicians need to pay more attention when these children complain of headache. During brain maturation, the developmental change in the neural network of the brain are important as the nervous system may respond differently to external stimuli and/or disease (e.g., migraine).35 Early onset of AR may affect the neural network functioning and stability during
brain maturation that is important in the pathophysiology of migraine in young children.35
Although the pathophysiology of migraine remains unclear, alteration of brain excitability, intracranial arterial dilatation, sensitization of the trigeminovascular system, 36, 37 and neurogenic inflammation are considered to play a crucial role in the pathogenesis of migraine.12-15 The levels of several inflammatory mediators, including leukotriene, prostaglandins, calcitonin gene-related peptide (CGRP), histamine, and nitric oxide (NO), were observed to elevate during episodes of migraine headache16-19 and these mediators also play a crucial role in allergic diseases.20 AR is an
immunoglobulin E (IgE)-mediated phenomenon involving activation and
degranulation of above inflammatory mediators by mast cells and basophils in the nasal mucosa close to the central nervous system (CNS) vasculature.20 These mediators play a critical role in neurogenic switching, a mechanism for shifting the site of inflammation in allergy and chemical sensitivity in the nervous system.38, 39 Leukotrienes are proinflammatory lipid mediators, which induced vasoconstriction, increased vascular permeability and edema by directly affecting vascular structure.40 Prostaglandins are arachidonic acid metabolites synthesized by stimulated mast cells via the cyclooxygenase pathway, and are important mediators of pain and
peptide, present in nonmyelinated fibers of the trigeminal ganglion.42 Histamine is released by the mast cells and has several effects, such as causing pain,increasing NO release, causing vasodilation and increasing vascular permeability, leading to local neurogenic inflammation.43, 44 Endothelium-dependent vasodilation and
neurotransmission of nociceptive information in the CNS are considered to be crucial in the development of migraine headaches.21 All these inflammatory mediators also play roles in the pathogenesis of AR and support the possible relationship between AR and migraine.
This study had certain limitations. Detailed clinical information and lab data associated with allergic diseases and migraine, including serum IgE levels, eosinophil levels, skin prick test, and family history of allergic diseases and migraine, were not included in the database. The incidence rate may be underestimated in current study, because less severe or less frequent migraine in children may not be recognized by caregivers or may be given over-the-counter medications to treat their headaches. Lastly, the ethnic population in this study was Chinese, thus, the results may not be applicable to other populations.
In conclusion, this population-based retrospective cohort study reveals a significantly increased incidence of migraine in children with AR regardless of age and sex. Children with AR should be closely observed for comorbid symptoms of
headache specifically within the first year after AR is diagnosed. Future investigations of environmental and genetic factors related to AR and subsequent risk prediction of migraine are recommended.
Acknowledgements
The study was supported in part by Taiwan Ministry of Health and Welfare Clinical Trial and Research Center of Excellence (MOHW104-TDU-B-212-113002), China Medical University Hospital, Academia Sinica Taiwan Biobank, Stroke Biosignature Project (BM104010092), NRPB Stroke Clinical Trial Consortium (MOST 103-2325-B-039 -006), Tseng-Lien Lin Foundation, Taichung, Taiwan, Taiwan Brain Disease Foundation, Taipei, Taiwan, and Katsuzo and Kiyo Aoshima Memorial Funds, Japan.
Figure Legends
Figure 1. The Kaplan-Meier analysis of cumulative incdience of migraine for allergic rhinitis (AR) cohort compared to non-AR cohort.
Reference
1. Ait-Khaled N, Pearce N, Anderson HR, et al. Global map of the prevalence of symptoms of rhinoconjunctivitis in children: The International Study of Asthma and Allergies in Childhood (ISAAC) Phase Three. Allergy. 2009;64:123-148.
2. Nathan RA, Meltzer EO, Selner JC,et al. Prevalence of allergic rhinitis in the United States. J Allergy Clin Immun. 1997;99:S808-S814.
3. Brozek JL, Bousquet J, Baena-Cagnani CE, et al. Allergic Rhinitis and its Impact on Asthma (ARIA) guidelines: 2010 revision. J Allergy Clin Immunol. 2010;126:466-476.
4. Thompson AK, Juniper E, Meltzer EO. Quality of life in patients with allergic rhinitis. Ann Allergy Asthma Immunol. 2000;85:338-347.
5. Spector SL. Overview of comorbid associations of allergic rhinitis. J Allergy Clin Immunol. 1997;99:S773-780.
6. Lack G. Pediatric allergic rhinitis and comorbid disorders. J Allergy Clin Immunol. 2001;108:S9-15.
7. Cady RK, Schreiber CP. Sinus headache or migraine? Considerations in making a differential diagnosis. Neurology. 2002;58:S10-S4.
8. Cady RK, Dodick DW, Levine HL, et al. Sinus headache: a neurology, otolaryngology, allergy, and primary care consensus on diagnosis and treatment. Mayo Clin Proc. 2005;80:908-916.
9. Powers SW, Patton SR, Hommel KA, et al. Quality of life in childhood migraines: Clinical impact and comparison to other chronic illnesses. Pediatrics. 2003;112:E1-E5.
10. Arruda MA, Bigal ME. Migraine and migraine subtypes in preadolescent children Association with school performance. Neurology. 2012;79:1881-1888.
11. Bille B. A 40-year follow-up of school children with migraine. Cephalalgia. 1997;17:488-491.
12. Pietrobon D, Moskowitz MA. Pathophysiology of Migraine. Annu Rev Physiol. 2013;75:365-391.
13. Capuano A, De Corato A, Lisi L,et al. Proinflammatory-activated trigeminal satellite cells promote neuronal sensitization: relevance for migraine
pathology. Mol Pain. 2009;5.
14. Longoni M, Ferrarese C. Inflammation and excitotoxicity: role in migraine pathogenesis. Neurol Sci. 2006;27 Suppl 2:S107-S110.
genetics and functional neuroimaging. Headache. 2013;53:401-12. 16. Bockowski L, Sobaniec W, Zelazowska-Rutkowska B. Proinflammatory
plasma cytokines in children with migraine. Pediatr Neurol. 2009;41:17-21. 17. Gazerani P, Pourpak Z, Ahmadiani A, et al. A correlation between migraine,
histamine and immunoglobulin E. Scand J Immunol. 2003;57:286-290. 18. LaMancusa R, Pulcinelli FM, Ferroni P, et al. Blood leukotrienes in headache:
correlation with platelet activity. Headache. 1991;31:409-414.
19. Ince H, Aydin OF, Alacam H, et al. Urinary leukotriene E4 and prostaglandin F2a concentrations in children with migraine: a randomized study. Acta Neurol Scand. 2014;130:188-192.
20. Wilson AM, Orr LC, Sims EJ, et al. Effects of monotherapy with intra-nasal corticosteroid or combined oral histamine and leukotriene receptor antagonists in seasonal allergic rhinitis. Clin Exp Allergy. 2001;31:61-68.
21. Ku M, Silverman B, Prifti N, et al. Prevalence of migraine headaches in patients with allergic rhinitis. Ann Allergy Asthma Immunol. 2006;97:226-230. 22. Ozturk A, Degirmenci Y, Tokmak B, et al. Frequency of migraine in patients
with allergic rhinitis. Pak J Med Sci. 2013;29:528-531.
23. Saberi A, Nemati S, Shakib RJ, et al. Association between allergic rhinitis and migraine. J Res Med Sci. 2012;17:508-512.
24. Davis K, Huang AT. Learning from Taiwan: experience with universal health insurance. Ann Intern Med . 2008;148:313-314.
25. Wei CC, Tsai JD, Lin CL, et al. Increased risk of idiopathic nephrotic syndrome in children with atopic dermatitis. Pediatr Nephrol. 2014;29:2157-2163. 26. Wei CC, Chang CH, Lin CL, et al. Neonatal jaundice and increased risk of
attention‐deficit hyperactivity disorder: a population‐based cohort study. J Child Psychol Psychiatry. 2015;56: 460-467.
27. Wei CC, Lin CL, Shen TC, et al. Increased incidence of juvenile-onset systemic lupus erythematosus among children with asthma. Pediatr Allergy Immunol. 2014;25:374-379.
28. Giannini G, Cevoli S, Sambati L, et al. Migraine: risk factor and comorbidity. Neurol Sci, 2012; 33: 37-41.
29. Bille BS. Migraine in school children. A study of the incidence and short-term prognosis, and a clinical, psychological and electroencephalographic
comparison between children with migraine and matched controls. Acta Paediatr Suppl.1962;136:1-151.
30. Deubner DC. An epidemiologic study of migraine and headache in 10-20 year olds. Headache. 1977;17:173-180.
Officers of Schools Association. Practitioner. 1978;221:407-411.
32. Sillanpaa M. Changes in the prevalence of migraine and other headaches during the first seven school years. Headache. 1983;23:15-19.
33. Lipton RB, Stewart WF, Celentano DD, Reed ML. Undiagnosed migraine headaches. A comparison of symptom-based and reported physician diagnosis. Arch Intern Med. 1992;152:1273-1278.
34. Akyol A, Kiylioglu N, Aydin I, et al. Epidemiology and clinical characteristics of migraine among school children in the Menderes region. Cephalalgia. 2007;27:781-7.
35. Borsook D, Erpelding N, Lebel A, et al. Sex and the migraine brain. Neurobiol Dis. 2014;68:200-214.
36. Vapaatalo H. Tolfenamic Acid and Migraine - Aspects on Prostaglandins and Leukotrienes. Pharmacol Toxicol. 1994;75:76-80.
37. May A, Goadsby PJ. The trigeminovascular system in humans:
Pathophysiologic implications for primary headache syndromes of the neural influences on the cerebral circulation. J Cerebr Blood F Met. 1999;19:115-127.
38. Meggs WJ. Neurogenic switching: a hypothesis for a mechanism for shifting the site of inflammation in allergy and chemical sensitivity. Environ Health Perspect. 1995;103:54-56.
39. Barnes NC, Piper PJ, Costello JF. Comparative effects of inhaled leukotriene C4, leukotriene D4, and histamine in normal human subjects. Thorax.
1984;39:500-504.
40. Lamancusa R, Pulcinelli FM, Ferroni P, et al. Blood Leukotrienes in Headache - Correlation with Platelet Activity. Headache. 1991;31:409-414.
41. Nicol GD, Klingberg DK, Vasko MR. Prostaglandin E2 increases calcium conductance and stimulates release of substance P in avian sensory neurons. J Neurosci. 1992;12:1917-1927.
42. Fox FE, Kubin M, Cassin M, et al. Calcitonin gene-related peptide inhibits proliferation and antigen presentation by human peripheral blood mononuclear cells: Effects on B7, interleukin 10, and interleukin 12. J Invest Dermatol. 1997;108:43-48.
43. Anselmi B, Tarquini R, Panconesi A, et al. Serum beta-endorphin increase after intravenous histamine treatment of chronic daily headache. Recenti Prog Med. 1997;88:321-324.
44. Krabbe AA, Olesen J. Headache provocation by continuous intravenous infusion of histamine. Clinical results and receptor mechanisms. Pain. 1980;8:253-259.
Table 1. Demographics between children with and without allergic rhinitis (AR) Non-AR (N=460718) AR (N=461850) n (%) n (%) p-value
Age, years, mean (SD)* 6.1 ( 4.3) 6.1 ( 4.3) 0.50
Stratified age, years 0.61
<6 267943 (58.2) 268311 (58.1) 6-11 136721 (29.7) 137485 (29.8) ≥ 12 56054 (12.2) 56054 (12.1) Sex 0.32 Girl 188340 (40.9) 188340 (40.8) Boy 272378 (59.1) 273510 (59.2) Urbanization† 0.41 1 (highest) 142644 (31.0) 143753 (31.1) 2 140393 (30.5) 140416 (30.4) 3 83412 (18.1) 83412 (18.1) 4 (lowest) 94269 (20.5) 94269 (20.4) Comorbidity Chronic rhinosinusitis 2346 (0.51) 16716 (3.62) <0.001 Obstructive sleep apnea 1 (0.00) 6 (0.00) 0.06
Anxiety 484 (0.11) 967 (0.21) <0.001
Depression 122 (0.03) 238 (0.05) <0.001
Obesity 379 (0.08) 682 (0.15) <0.001
Hypertension 111 (0.02) 184 (0.04) <0.001
Chi-square test, and *t-test comparing subjects with and without allergic rhinitis †The urbanization level was categorized by the population density of the residential area into 4 levels, with level 1 as the most urbanized and level 4 as the least
Table 2. The incidence rate and relative risk of migraine in children with allergic rhinitis (AR) compared to children without AR stratified by demographics in Cox proportional hazard regression
Non- AR AR Migraine case Person-years IR Migraine case Person-years IR Adjusted HR† (95% CI) All 860 2467121 3.49 2823 2487530 11.4 3.20(2.97, 3.46)* Stratified age <6 228 1478222 1.54 888 1491356 5.95 3.75(3.24, 4.34)* 6-11 443 799155 5.54 1318 804980 16.4 2.92(2.62, 3.25)* ≥ 12 189 189744 9.96 617 191195 32.3 3.17(2.69, 3.74)* Sex Girl 449 993799 4.52 1416 999369 14.2 3.09(2.78, 3.44)* Boy 411 1473323 2.79 1407 1488162 9.45 3.32(2.97, 3.71)* Urbanization 1 (highest) 262 766914 3.42 834 777089 10.7 3.10(2.69, 3.56)* 2 258 753815 3.42 862 759355 11.4 3.27(2.85, 3.77)* 3 145 447876 3.24 508 450378 11.3 3.44(2.86, 4.14)* 4 (lowest) 195 498516 3.91 619 500709 12.4 3.07(2.61, 3.61)*
IR, incidence rate, per 10,000 person-years
Adjusted HR ( hazard ratio)†, adjusted for age, sex and comorbidity of chronic rhinosinusitis, anxiety, depression, obesity, and hypertension
Table 3 The incidence rate and relative risk of migraine in children with allergic rhinitis (AR) stratified by age in both genders in Cox proportional hazard regression
Migraine case Person-years IR Adjusted HR† (95% CI) Girl <6 381 605914 6.29 1.00(Reference) 6-11 650 311334 20.9 3.29(2.90, 3.74)* ≥ 12 385 82120 46.9 8.22(7.09, 9.52)* p for trend <0.001 Boy <6 507 885441 5.73 1.00(Reference) 6-11 668 493645 13.5 2.34(2.09, 2.63)* ≥ 12 232 109075 21.3 3.92(3.34, 4.59)* p for trend <0.001
IR, incidence rate, per 10,000 person-years
Adjusted HR (hazard ratio)†, adjusted for comorbidity of chronic rhinosinusitis, anxiety, depression, obesity, and hypertension
Table 4. The risk of migraine by allergic rhinitis related medical visits per year in Cox proportional hazard regression
Average frequency for medical visits, per year
Migraine case Person-years IR Adjusted HR† (95% CI) All None 860 2467121 3.49 1.00(Reference) ≤2 937 1780526 5.26 1.44(1.31, 1.58)* 3-4 505 398001 12.7 3.83(3.43, 4.27)* > 4 1381 309003 44.7 14.8(13.6, 16.2)* p for trend <0.0001 Girl None 449 993799 4.52 1.00(Reference) ≤2 508 732581 6.93 1.47(1.30, 1.68)* 3-4 251 153583 16.3 3.77(3.23, 4.41)* > 4 657 113205 58.0 14.7(13.0, 16.6)* p for trend <0.0001 Boy None 411 1473323 2.79 1.00(Reference) ≤2 429 1047945 4.09 1.39(1.22, 1.60)* 3-4 254 244419 10.4 3.92(3.34, 4.58)* > 4 724 195798 37.0 15.3(13.5, 17.3)* p for trend <0.0001
IR, incidence rate, per 10,000 person-years
Adjusted HR ( hazard ratio)†, adjusted for age, sex and comorbidity of chronic rhinosinusitis, anxiety, depression, obesity, and hypertension
27
Table 5 The incidence rate and relative risk of migraine in children with allergic rhinitis (AR) compared to children without AR stratified by follow-up years in Cox proportional hazard regression
Non-AR AR
Adjusted HR† (95% CI) Follow time Migraine
case Person-years IR Migraine case Person-years IR ≤1 years 111 458596 2.42 558 460498 12.1 4.89(3.98, 6.00)* 2-3 years 269 842006 3.19 852 847949 10.1 3.11(2.71, 3.57)* 4-5 years 261 122320 21.3 781 122877 63.6 2.84(2.47, 3.28)* >5 years 219 516906 4.24 632 523628 12.1 2.78(2.38, 3.25)* IR, incidence rate, per 10,000 person-years
Adjusted HR ( hazard ratio)†, adjusted for age, sex and comorbidity of chronic rhinosinusitis, anxiety, depression, obesity, and hypertension
28
Table 6. The frequency of childhood migraine subtype in allergic rhinitis (AR) cohort and non-AR cohort
Non-AR (N=860)
AR (N=2823)
Migraine subtype (ICD-9CM codes) n (%) n (%) p-value Migraine with aura (346.0) 65 (7.6) 281 (10.0) 0.14 Migraine without aura (346.1) 155 (18.0) 437 (15.5)
Variants of migraine (346.2) 36 (4.2) 97 (3.4) Other forms of migraine (346.8) 15 (1.7) 49 (1.7) Migraine, unspecified (346.9) 589 (68.5) 1959 (69.4) Chi-square test