Association between traditional systemic anti-psoriatic drugs and tuberculosis risk in patients with psoriasis with or without psoriatic arthritis: Results from a nationwide cohort study
Yi-Ju Chen, MD, PhD, 1,2 Chun-Ying Wu, MD, PhD, 3,4,5, Jui-Lung Shen, MD, PhD,1 Tzu-Ting Chen, MS, 4 Yun-Ting Chang, MD, PhD.1,6
1Department of Dermatology, 3Faculty of Medicine, National Yang-Ming University,
Taipei, Taiwan
2Department of Dermatology and 4Department of Internal Medicine, Taichung
Veterans General Hospital, Taichung, Taiwan
5 Department of Public Health, College of Public Health, China Medical University,
Taichung
6Department of Dermatology, Taipei Veterans General Hospital, Taipei, Taiwan
Requests for reprints should be addressed to Yun-Ting Chang, MD, PhD,
Department of Dermatology, Taipei Veterans General Hospital and National Yang-Ming University, No. 201, Sec. 2, Shi-Pai Rd. Taipei, 112, Taiwan. TEL: +886-2-2875-7340; FAX: +886-2-2875-7666; Email: [email protected]
association
Running title: traditional systemic anti-psoriatic drugs and TB risk in psoriasis
patients
Word Count: 2736 Tables Count: 5 Figures Count: 0 Reference number: 40
Y.J. Chen and C.Y. Wu contributed equally to this manuscript.
Funding: Partly from Taichung Veterans General Hospital research grants
(TCVGH-1006801B, TCVGH-1006802C).
Competing interests: The authors have no conflicts of interest to report.
Capsule summary
1. The association between tuberculosis and traditional systemic anti-psoriatic drugs for psoriasis patients is unknown.
2. This nationwide cohort study demonstrated that severe psoriasis is associated with an elevated TB risk.
3. Traditional systemic anti-psoriatic therapy does not seem to be strongly associated TB development in psoriasis patients.
Abstract
Background: Although the link between tuberculosis (TB) and biologics use is
well-established, the risk of TB among psoriasis patients exposed to traditional systemic therapies remains elusive.
Objectives: The aim is to investigate the association between traditional systemic
therapies and TB among psoriasis patients.
Methods: We conducted a retrospective cohort study on the risk of active TB among
psoriasis and psoriatic arthritis patients, utilizing the National Health Insurance Research Database of Taiwan 1996-2008. Standardized incidence ratios (SIR) of TB were analyzed in comparison with age- and gender-matched general population. Logistic regression was used in a nested case-control analysis to estimate the odds ratios (OR) of TB related to exposure to traditional systemic agents during the year before TB development .
Results: Among the 81,266 patients in the psoriasis cohort, 497 new active TB cases
were identified. The incidence rate of TB was 102 cases per 100,000 person-years among psoriasis patients (SIR of 1.22, 95% confidence interval [CI] 1.18-1.33). The risk of TB was higher in patients with severe disease (SIR 1.52, 95% CI 1.46-1.74). To facilitate comparisons with the 497 active TB cases, a total of 1,988 matched control subjects were selected for a nested case control study. Patients taking systemic corticosteroids and non-steroidal anti-inflammatory drugs (NSAID) were associated
with higher incidence of TB, especially frequent users, after adjustment for multiple TB risk factors, drug exposures, hospital visits and level of urbanization. Stratified analyses of current users and new users of these drugs revealed similar results. Finally, traditional systemic anti-psoriatic treatment is not associated with TB on any of the analyses.
Limitation: NHIRD did not contain information regarding severity of psoriasis,
status of smoking, alcohol use, diet, laboratory parameters, chest radiograph, history of recent contact with an individual with TB. Misclassification of disease cannot be ruled out in a registry-based database. The accessibility of healthcare may be
associated with the level of urbanization, which could confound the effect of drugs in multivariate analyses.
Conclusions: Severe psoriasis may be associated with an elevated TB risk.
Traditional systemic therapies do not seem to be strongly associated with TB occurrence.
Introduction
An increased prevalence of active TB has been reported in patients with systemic lupus erythematosus (SLE)1,2 and rheumatoid arthritis (RA),3 and the risk of active TB increased further in patients taking antitumor necrosis factor (TNF)-α regimens. 4-8 A disturbance of immune function and treatments with immunosuppressive agents are thought to be related to the susceptibility of TB in these patients.1-3 However, the studies investigating the association between psoriasis and TB are limited.
It is now recommended to obtain a thorough exposure history, utilize tuberculin skin test (TST) or Interferon-γ release assays (IGRA) in BCG-vaccinated patients,9 and consider a chest X ray as TB screening method for all patients being treated with any TNF-α inhibitors, and continue TB screening annually thereafter or for 6 months after discontinuation, as proposed by the National Psoriasis Foundation (NPF)10 and British Association of Dermatologists (BAD).11 Currently, either TST or IGRA was recommended before using TNF-α antagonists for patients in Taiwan.12 The
consensus of latent tuberculosis infection (LTBI) screening protocol before starting biologics for psoriasis has yet to be established in Taiwan. Finally, there are no guidelines for TB testing before starting non-biologic systemic therapies.10
Our aims were to investigate the risk of new active TB in psoriasis patients and the association between traditional systemic therapies and TB occurrence, using data
from National Health Insurance (NHI) claims published by the National Health Research Institute (NHRI). The effects of age at diagnosis, gender, coexisting risk factors and treatment modalities on TB development were also evaluated.
Patients and methods Data sources
This retrospective nationwide cohort study was based on data from the National Health Insurance Research Database (NHIRD) released by the NHRI. Taiwan began its NHI program in 1995 to finance health care for all of its residents. There are currently more than 25 million enrollees in the program, representing approximately 99% of Taiwan’s entire population. The NHIRD contains registration files and original claims data for care reimbursements for all enrollees, making it one of the largest and most complete nationwide population-based health care services datasets in the world.13-16 In this database, the diagnostic codes are in the format of the
International Classification of Diseases, Revision 9, Clinical Modification (ICD-9-CM). Patients were diagnosed by board-certified physicians in the corresponding specialties. The accuracy of diagnosis of major diseases in the NHIRD, such as diabetes mellitus, hypertension and stroke, has been validated.17, 18 Personal
information including body weight, height, family history, laboratory examination information, lifestyle and habits such as smoking and alcohol use was not available from the NHIRD.
Psoriasis cohort
We identified a total of 85,356 patients with at least 3 visits within a one-year observation period or who were admitted for psoriasis or psoriatic arthritis (ICD9
696.0, 696.1, 696.8) to a department of Dermatology or Rheumatology. Patients entered the study cohort at the first diagnosis of psoriasis. We excluded patients who received a diagnostic code for TB (ICD9 code 010-018) (n=2,984) or anti-TB
medications (see below) before entry into the study cohort (n=1,586). Since biologics were not approved for use in psoriasis and psoriatic arthritis in Taiwan until late 2009, patients using biologics were not included in this study. A total of 81,266 patients with psoriasis and psoriatic arthritis comprised the psoriasis cohort. All sampled individuals were followed up from the date of diagnosis to the date of censorship, i.e. the date of diagnosis of outcome of interest (i.e. active TB), death, or the end of 2008. Follow-up time was measured in numbers of years.
Those with severe psoriasis were defined as those ever received photothearpies or any of systemic therapies after diagnosis. Those never received phototherapies or systemic therapies were defined as mild psoriasis patients.19,20
This study has been approved by the ethical board review of Taipei Veterans General Hospital, Taiwan.
Case definition
During follow up, TB cases were identified as those with at least 3 diagnoses within a one-year observation period or hospitalization for TB (ICD-9 CM codes 010– 018), as well as prescriptions for at least two classes of first-line anti-TB medications (isoniazid, rifampin, pyrazinamide, or ethambutol), with treatment lasting for at least
6 months, as described before.21, 22 TB cases that occurred before the date of cohort entry were excluded.
We also separated cases of TB into pulmonary TB (PTB) (ICD9 codes 010-012) and extra-pulmonary TB (EPTB) (ICD9 codes 013-018) for relative risk analyses.
Nested case control study
To investigate the association between antipsoriatic drugs and the risk of TB, we used a nested case control analysis within the psoriasis cohort to address the complex patterns of drug exposure over time.22, 23 Compared to a full cohort approach using a survival analysis with time dependent variables, a nested case-control analysis is computationally more efficient, while producing odds ratios that are unbiased estimators of incidence rate ratios with little or no loss in precision.23, 24
Four control subjects were randomly selected from the psoriasis cohort for each case of TB after matching on age, gender, date of diagnosis of psoriasis (i.e. date of cohort entry) and duration of follow up, and ensured that each control subject was alive and at risk on the day when the case occurred. The date of case occurrence was designated as the index date.
Covariate assessment
Risk factors for TB were identified and included diabetes mellitus (ICD9-CM code 250), chronic renal failure CM code 585, V56.0), organ transplant (ICD9-CM code V42.0, V42.1), silicosis (ICD9-(ICD9-CM code 502), HIV (ICD9-(ICD9-CM code 042)
and malignant diseases (ICD9-CM code 140-208), diagnosed at least 3 times before and during follow-up.
Potential confounders included coexisting psoriatic arthritis, treatment modalities, numbers of hospital visits, geographic locations (northern, central, southern, and eastern Taiwan), and levels of urbanization. Traditional systemic antipsoriatic drugs (including methotrexate [MTX], acitretin, cyclosporine, azathioprine and mycophenolate mofetil); common drugs for arthritis (systemic corticosteroids, NSAID, and selective cyclooxygenase-2 [COX-2] inhibitors); and phototherapies (including ultraviolet B (UVB) and psoralen plus ultraviolet A [PUVA]) used to treat extensive skin lesions in psoriasis, were also considered covariate factors. Urbanization of cities/counties was stratified into eight levels (from 1 indicating the most urbanized to 8 indicating the least urbanized), based on the classifications published by the Institute of Occupational Safety and Health (IOSH), Executive Yuan, Taiwan.25 As there were only very small numbers of psoriasis cases in some levels, we combined levels 3 and 4 into one group, denoted level 3, and levels 5 through 8 into another group, denoted level 4.
Statistical analysis
The demographic data of the study population were first analyzed. Follow-up for each subject began at the date of diagnosis and ended at the date of censorship, i.e. the
date of diagnosis of outcome of interest, death, or the end of 2008, and was measured in numbers of years. The total person years of observation for the entire cohort were used to estimate TB incidence rates among psoriasis patients. Next, we compared the incidence rate of TB among psoriasis patients with that of the Taiwanese general population by utilizing standardized incidence ratios (SIR). SIR was calculated as follows: the number of TB cases that occurred among patients with psoriasis or psoriatic arthritis, divided by the expected number of TB cases according to national age-specific, gender-specific, and period-specific TB rates. Yearly reports of TB rates were obtained from the TB Registry of the CDC, Taiwan. We pooled the 6-year TB registry reports of Taiwan from 2003 to 2008 as the standard.
We further estimated the relative risks of PTB and EPTB in patients of psoriasis cohort compared with Taiwanese general population,26 with 95% confidence intervals (CI) based on Poisson's distribution.
To assess the associations between drug exposures and TB, odds ratios (OR) and 95% confidence intervals (CI) were estimated from nested case control analysis within the psoriasis cohort. Conditional logistic regression was used to adjust these estimates for the use of each traditional anti-psoriatic drugs, corticosteroids, NSAIDs, and COX-2 inhibitors, as well as for age, gender, presence of psoriatic arthritis, number of hospital visits, geographic location, level of urbanization, and all other
clinical risk factors and covariates mentioned above. To assess the effects of drug exposure, we analyzed the risk among systemic drug users according to the number of non-biologic systemic agents prescriptions obtained within 1 year prior to the index date. We stratified the risk according to the frequency of prescriptions during the observation period. A trend test for these ordered categories was performed based on Cochran-Armitage trend test. We also stratified the risk of TB according to the timing of prescriptions: individuals with any of the above prescriptions within 45 days prior to the index date (current users) and individuals who began these prescriptions within 90 days prior to the index date (new users).
Sensitivity analyses focused on (1) individuals never receiving systemic anti-psoriatic drugs or phototherapies; (2) individuals ever receiving traditional systemic anti-psoriatic drugs or phototherapies; (3) severe psoriasis patients without retinoids; (4) individuals never receiving systemic corticosteroids; (5) individuals without psoriatic arthritis; and (6) individuals without coexistent autoimmune diseases, such as RA or SLE. These sensitivity analyses were conducted to examine whether the main findings were robust to different assumptions.
All analyses were performed using SAS 10.1 software (SAS Institute Inc., Cary, NC, USA).
Results
Characteristics of study subjects in psoriasis cohort
We identified a total of 81,266 patients with psoriasis and psoriatic arthritis but without prior history of TB or anti-TB drug use. The mean age of patients at diagnosis was 44.1 years (median [inter-quartile range, IQR], 43.0 [28.7- 57.8]). There were 31,708 (39.0%) female and 49,558 (61.0%) male patients. The mean follow-up time for psoriasis cohort was 5.98 years (median [IQR], 6.0 [3.6-8.5]).
Incidence rate of TB in psoriasis cohort
During the observation period, which consisted of 486,331 person-years, a total of 497 cases of active TB were identified after diagnosis of disease in the psoriasis cohort. The incidence rate of TB in psoriasis cohort was 102 per 100,000 person years, in comparison with 67.5 TB cases per 100,000 person years in the general population of Taiwan.4 A slightly increased overall TB risk was observed in the psoriasis cohort (SIR 1.22, 95% confidence interval [CI] 1.18-1.33).
PTB cases comprised the most common subtype (90.54%), followed by TB of bone/joint (3.02%), TB of central nervous system/meninges (CNS) (2.21%), TB of skin or subcutaneous tissue (2.21%) and miliary TB (2.01%). The relative incidence rate ratio (IRR) of EPTB in psoriasis was two-fold that of the general population. (Table 1)
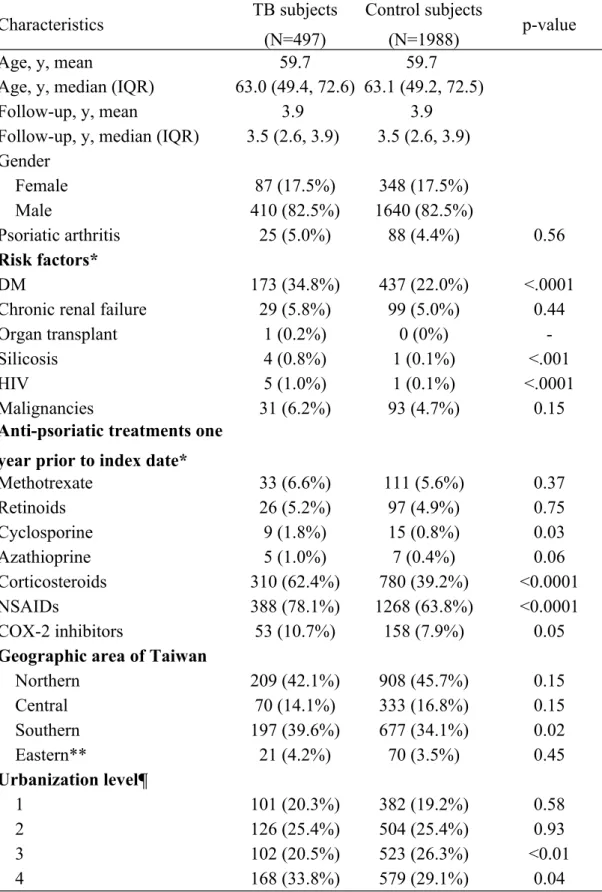
The demographic characteristics of TB cases and controls in the psoriasis cohort are presented in Table 2. Risk factors for TB were most commonly observed in the case group, including diabetes, silicosis and HIV co-infection. No significant
differences were observed between the study groups in the use of traditional systemic anti-psoriatic treatments or presence of psoriatic arthritis. Patients with TB were found to have received more corticosteroids and COX-2 inhibitors. TB cases were most commonly observed in southern Taiwan and less urbanized areas. (Table 2)
Association between drug exposure and TB
There were no significant associations for traditional systemic agents and TB occurrence within 1 year before the index date, after adjusting for age, gender, treatment modalities, level of urbanization, geographic location, hospital visits and presence of arthritis. (Table 3) Frequent traditional anti-psoriatic drug use was not associated with a more chance for TB. However, frequent users of systemic
corticosteroids and NSAIDs had a significantly higher chance of developing TB than non-frequent users. (Table 3) Further stratified analyses of current users and new users revealed similar results. (Table 4)
Sensitivity analysis
Sensitivity analyses suggested that the primary findings are robust. (Table 5) Patient with mild psoriasis has comparable TB risk than general population. However, patients with severe psoriasis appeared to have a higher risk of TB (SIR 1.52, 95% CI
1.46-1.74) than mild psoriasis. In addition, psoriasis patients without psoriatic arthritis or other autoimmune diseases are still associated with TB occurrence.
Discussion
This large cohort study demonstrates a higher relative risk for EPTB in psoriasis cohort (Table 1), as described in other autoimmune diseases.27, 28 TB of bone and joints constitutes the most common form of EPTB in these patients. The insidious onset of TB arthritis may mimic other common joint diseases which might lead to delayed diagnoses.29-31 Cutaneous TB can mimic hypertrophic form of psoriasis. Although the incidence is low, physicians should be aware of the possibility of EPTB in psoriasis patients presenting with arthritis or poorly controlled hypertrophic skin lesions.
Our study implied that the severity of psoriasis is associated with active TB. Bordignon et al.32 identified an unexpected high prevalence of LTBI in patients with psoriasis by analyzing their immune response in vitro to different M. tuberculosis (Mtb) antigens on IGRA. Silva et al.33 further demonstrated the activation of
interferon-γ (IFN-γ), IL-10 and T-cell proliferation in response to Mtb antigens are reduced in TST-negative patients, mostly seen in severe psoriasis.33 These results suggested that aberrant T cell response to Mtb antigen in severe psoriasis may lead to reactivation of latent TB.
Long-term use of systemic immunosuppressive drugs may partly explain the association between TB and psoriasis. TNF-α antagonists are known to be implicated
in an increased rate of TB4-8 and even with disseminated and extrapulmonary TB.6, 34 Increased risk of TB with systemic corticosteroid use has been quantified in several population studies.21,22,31
However, studies investigating the association between MTX and TB occurrence revealed conflicting results in psoriasis 35 and RA patients22,35-38 Although reactivation of LTBI has been reported in transplant recipients using cyclosporine,39 no cases have been reported at a lower dose of cyclosporine used in dermatologic settings.40 Except for corticosteroids, here we found no significant associations between traditional anti-psoriatic drugs and TB occurrence. These results were consistent across different sensitivity analyses for new and current users.
An association between NSAID and TB development was observed in our analyses. A possible interaction between NSAID use and psoriatic arthritis could confound these results. We excluded subjects who received NSAID or COX-2 inhibitors with a diagnosis of arthritis for further analyses. Similar results were observed in any of these analyses. (data not shown here) It implied that the
association between NSAID and TB was because of reasons other than arthritis. We postulated that NSAID may be commonly used for patients presenting with early symptoms of TB. However, further studies are needed to elucidate their relationship.
NHIRD in Taiwan which contains detailed pharmacy claims from each study subject and is widely accepted for epidemiological studies. In addition to common risk factors, we also took geographic location and urbanization level of patients' habitat into consideration, which are well-known confounding factors for TB.26, 27 Finally, to reduce the confounding by indication, we conducted several sensitivity analyses which suggested the results are robust.
There are several limitations to our present study. First, it was difficult to infer causation between drugs of interest and risk of TB based on an observational study, without a random assignment of treatments. Thus, confounding by indication may exist. We did not have personal information regarding lifestyle, laboratory
parameters, chest radiograph, family history or history of recent contact with an individual with TB, all of which may contribute to TB. Those who received
immunosuppressants could be more likely to be evaluated for TB. Patients from rural areas are more likely to have TB, as shown by a higher proportion in cases, and less likely to have access to healthcare. They may be less likely to receive psoriasis therapy. Therefore, the effect of systemic drugs in developing TB could be partly reduced in multivariate analyses in which the urbanization level could be a
confounding variable. Disease severity was also not recorded in the database. Here, we took the use of traditional systemic anti-psoriatic drugs or phototherapy as a
proxy for more severe disease.19 Coding error of disease is possible in an
administrative database. To minimize this bias, we only enrolled patients receiving at least 3 diagnoses of psoriasis and TB in a one-year observation period. Active TB cases were further identified by additional pharmacological information. Finally, since LTBI screening is not routinely performed in psoriasis patients, we could not estimate the prevalence of LTBI or TB reactivation among our psoriasis cohort.
In conclusion, we found that psoriasis patients may be at risk of TB, and use of traditional systemic anti-psoriatic drugs does not seem to be strongly associated with TB in patients with psoriasis or psoriatic arthritis.
ACKNOWLEDGEMENTS
This study is based in part on data from the National Health Insurance Research Database provided by the Bureau of National Health Insurance, Department of Health and managed by the National Health Research Institute. The interpretations and conclusions contained herein do not represent those of the Bureau of National Health Insurance, Department of Health or the National Health Research Institute.
Reference
1. Tam LS, Li EK, Wong SM, Szeto CC. Risk factors and clinical features for tuberculosis among patients with systemic lupus erythematosus in Hong Kong. Scand J Rheumatol 2002;31:296-300.
2. Mok MY, Lo Y, Chan TM, Wong WS, Lau CS. Tuberculosis in systemic lupus erythematosus in an endemic area and the role of isoniazid prophylaxis during corticosteroid therapy. J Rheumatol 2005;32:609-15.
3. Carmona L, Hernandez-Garcia C, Vadillo C, Pato E, Balsa A, Gonzalez-Alvaro I, et al. Increased risk of tuberculosis in patients with rheumatoid arthritis. J Rheumatol 2003;30:1436-9.
4. Dixon WG, Hyrich KL, Watson KD, Lunt M, Galloway J, Ustianowski A, et al. Drug-specific risk of tuberculosis in patients with rheumatoid arthritis treated with anti-TNF therapy: results from the British Society for Rheumatology Biologics Register (BSRBR). Ann Rheum Dis 2010;69:522-8.
5. Wallis RS, Broder MS, Wong JY, Hanson ME, Beenhouwer DO. Granulomatous infectious diseases associated with tumor necrosis factor antagonists. Clin Infect Dis 2004;38:1261-5.
6. Keane J, Gershon S, Wise RP, Mirabile-Levens E, Kasznica J, Schwieterman WD, et al. Tuberculosis associated with infliximab, a tumor necrosis factor alpha-neutralizing agent. N Engl J Med 2001;345:1098-104.
7. Mohan AK, Cote TR, Block JA, Manadan AM, Siegel JN, Braun MM.
Tuberculosis following the use of etanercept, a tumor necrosis factor inhibitor. Clin Infect Dis 2004;39:295-9.
8. Gomez-Reino JJ, Carmona L, Valverde VR, Mola EM, Montero MD. Treatment of rheumatoid arthritis with tumor necrosis factor inhibitors may predispose to significant increase in tuberculosis risk: a multicenter active-surveillance report. Arthritis Rheum 2003;48:2122-7.
9. Jensen PA, Lambert LA, Iademarco MF, Ridzon R. Guidelines for preventing the transmission of Mycobacterium tuberculosis in health-care settings, 2005. MMWR Recomm Rep 2005;54(RR-17):1-141.
10. Doherty SD, Van Voorhees A, Lebwohl MG, Korman NJ, Young MS, Hsu S, et al. National Psoriasis Foundation consensus statement on screening for latent tuberculosis infection in patients with psoriasis treated with systemic and biologic agents. J Am Acad Dermatol 2008;59:209-17.
11. Smith CH, Anstey AV, Barker JN, Burden AD, Chalmers RJ, Chandler DA, et al. British Association of Dermatologists' guidelines for biologic interventions for psoriasis 2009. Br J Dermatol 2009;161:987-1019.
12. Chen DY, Shen GH, Hsieh TY, Hsieh CW, Lan JL. Effectiveness of the combination of a whole-blood interferon-gamma assay and the tuberculin skin test in detecting latent tuberculosis infection in rheumatoid arthritis patients receiving adalimumab therapy. Arthritis Rheum 2008;59:800-6.
13. Chang YT, Chen TJ, Liu PC, Chen YC, Chen YJ, Huang YL, et al.
Epidemiological study of psoriasis in the national health insurance database in Taiwan. Acta Derm Venereol 2009;89:262-6.
14. Chen YJ, Chang YT, Shen JL, Chen TT, Wang CB, Chen CM, et al. Association between systemic antipsoriatic drugs and cardiovascular risk in patients with psoriasis with or without psoriatic arthritis: A nationwide cohort study. Arthritis Rheum 2012;64:1879-87.
15. Wu CY, Wu MS, Kuo KN, Wang CB, Chen YJ, Lin JT. Effective reduction of gastric cancer risk with regular use of nonsteroidal anti-inflammatory drugs in Helicobacter pylori-infected patients. J Clin Oncol. 2010;28:2952-7.
16. Wu CY, Kuo KN, Wu MS, Chen YJ, Wang CB, Lin JT. Early Helicobacter pylori eradication decreases risk of gastric cancer in patients with peptic ulcer disease. Gastroenterology. 2009;137:1641-8 e1-2.
17. Cheng CL, Kao YH, Lin SJ, Lee CH, Lai ML. Validation of the National Health Insurance Research Database with ischemic stroke cases in Taiwan.
Pharmacoepidemiol Drug Saf 2011;20:236-42.
18. Lin CC, Lai MS, Syu CY, Chang SC, Tseng FY. Accuracy of diabetes diagnosis in health insurance claims data in Taiwan. J Formos Med Assoc 2005;104:157-63.
19. Gelfand JM, Neimann AL, Shin DB, Wang X, Margolis DJ, Troxel AB. Risk of myocardial infarction in patients with psoriasis. JAMA 2006;296:1735-41. 20. Mehta NN, Azfar RS, Shin DB, Neimann AL, Troxel AB, Gelfand JM. Patients
with severe psoriasis are at increased risk of cardiovascular mortality: cohort study using the General Practice Research Database. Eur Heart J 2010;31:1000-6.
21. Brassard P, Kezouh A, Suissa S. Antirheumatic drugs and the risk of tuberculosis. Clin Infect Dis 2006;43:717-22.
22. Brassard P, Lowe AM, Bernatsky S, Kezouh A, Suissa S. Rheumatoid arthritis, its treatments, and the risk of tuberculosis in Quebec, Canada. Arthritis Rheum 2009;61:300-4.
23. Essebag V, Platt RW, Abrahamowicz M, Pilote L. Comparison of nested case-control and survival analysis methodologies for analysis of time-dependent exposure. BMC Med Res Methodol 2005;5:5.
cardiology. Am Heart J 2003;146:581-90.
25. Lin HC, Lin YJ, Liu TC, Chen CS, Chiu WT. Urbanization and stroke prevalence in Taiwan: analysis of a nationwide survey. J Urban Health 2007;84:604-14.
26. Lo HY, Chou P, Yang SL, Lee CY, Kuo HS. Trends in tuberculosis in Taiwan, 2002-2008. J Formos Med Assoc 2011;110:501-10.
27. Hou CL, Tsai YC, Chen LC, Huang JL. Tuberculosis infection in patients with systemic lupus erythematosus: pulmonary and extra-pulmonary infection compared. Clin Rheumatol 2008;27:557-63.
28. Gonzalez Leon R, Garrido Rasco R, Chinchilla Palomares E, Garcia Hernandez FJ, Castillo Palma MJ, Sanchez Roman J. Tuberculosis in a cohort of patients with systemic lupus erythematosus. Reumatol Clin 2010;6:256-61.
29. Hunfeld KP, Rittmeister M, Wichelhaus TA, Brade V, Enzensberger R. Two cases of chronic arthritis of the forearm due to Mycobacterium tuberculosis. Eur J Clin Microbiol Infect Dis 1998;17:344-8.
30. Al-Sayyad MJ, Abumunaser LA. Tuberculous arthritis revisited as a forgotten cause of monoarticular arthritis. Ann Saudi Med 2011;31:398-401.
31. Ocguder A, Tosun O, Akkurt O, Oguz T, Colakoglu T. Tuberculosis of the foot: a rare involvement in osteoarticular tuberculosis. J Clin Rheumatol 2006;12:304-5.
32. Bordignon V, Bultrini S, Prignano G, Sperduti I, Piperno G, Bonifati C, et al. High prevalence of latent tuberculosis infection in autoimmune disorders such as psoriasis and in chronic respiratory diseases, including lung cancer. J Biol Regul Homeost Agents 2011;25:213-20.
33. Silva LC, Silveira GG, Arnone M, Romiti R, Geluk A, Franken KC, et al. Decrease in Mycobacterium tuberculosis specific immune responses in patients with untreated psoriasis living in a tuberculosis endemic area. Arch Dermatol Res 2010;302:255-62.
34. Smith JD, Knox JM. Psoriasis, methotrexate and tuberculosis. Br J Dermatol 1971;84:590-3.
35. Binymin K, Cooper RG. Late reactivation of spinal tuberculosis by low-dose methotrexate therapy in a patient with rheumatoid arthritis. Rheumatology (Oxford) 2001;40:341-2.
36. di Girolamo C, Pappone N, Melillo E, Rengo C, Giuliano F, Melillo G. Cavitary lung tuberculosis in a rheumatoid arthritis patient treated with low-dose
methotrexate and steroid pulse therapy. Br J Rheumatol 1998;37:1136-7. 37. Solomon DH. The comparative safety and effectiveness of TNF-alpha
38. Vadillo Font C, Hernandez-Garcia C, Pato E, Morado IC, Salido M, Judez E, et al. Incidence and characteristics of tuberculosis in patients with autoimmune rheumatic diseases. Rev Clin Esp 2003;203:178-82.
39. Vachharajani TJ, Oza UG, Phadke AG, Kirpalani AL. Tuberculosis in renal transplant recipients: rifampicin sparing treatment protocol. Int Urol Nephrol 2002;34:551-3.
40. Behnam SM, Behnam SE, Koo JY. Review of cyclosporine immunosuppressive safety data in dermatology patients after two decades of use. J Drugs Dermatol 2005;4:189-94.
Table 1. Crude incidence rate ratios of PTB and EPTB among psoriasis patients, in comparison with the general population
TB types N
Psoriasis (cases/100,000)
General population (cases per 100,000)
Incidence rate ratio* 95% CI
PTB 450 92.5 63.5 1.46 1.36-1.79
EPTB 47 9.7 4.0 2.45 1.91-4.55
Abbreviation: CI, confidence interval; EPTB, extra-pulmonary tuberculosis; N, number; PTB, pulmonary tuberculosis; TB, tuberculosis.
Table 2. Characteristics of TB and control subjects
Abbreviations: COX-2 inhibitors, cyclo-oxygenase 2 inhibitors; DM, diabetes mellitus; HIV, human immunodeficiency virus infection; IQR, inter-quartile range;
Characteristics TB subjects
(N=497)
Control subjects
(N=1988) p-value
Age, y, mean 59.7 59.7
Age, y, median (IQR) 63.0 (49.4, 72.6) 63.1 (49.2, 72.5)
Follow-up, y, mean 3.9 3.9
Follow-up, y, median (IQR) 3.5 (2.6, 3.9) 3.5 (2.6, 3.9) Gender Female 87 (17.5%) 348 (17.5%) Male 410 (82.5%) 1640 (82.5%) Psoriatic arthritis 25 (5.0%) 88 (4.4%) 0.56 Risk factors* DM 173 (34.8%) 437 (22.0%) <.0001
Chronic renal failure 29 (5.8%) 99 (5.0%) 0.44
Organ transplant 1 (0.2%) 0 (0%)
-Silicosis 4 (0.8%) 1 (0.1%) <.001
HIV 5 (1.0%) 1 (0.1%) <.0001
Malignancies 31 (6.2%) 93 (4.7%) 0.15
Anti-psoriatic treatments one year prior to index date*
Methotrexate 33 (6.6%) 111 (5.6%) 0.37 Retinoids 26 (5.2%) 97 (4.9%) 0.75 Cyclosporine 9 (1.8%) 15 (0.8%) 0.03 Azathioprine 5 (1.0%) 7 (0.4%) 0.06 Corticosteroids 310 (62.4%) 780 (39.2%) <0.0001 NSAIDs 388 (78.1%) 1268 (63.8%) <0.0001 COX-2 inhibitors 53 (10.7%) 158 (7.9%) 0.05
Geographic area of Taiwan
Northern 209 (42.1%) 908 (45.7%) 0.15 Central 70 (14.1%) 333 (16.8%) 0.15 Southern 197 (39.6%) 677 (34.1%) 0.02 Eastern** 21 (4.2%) 70 (3.5%) 0.45 Urbanization level¶ 1 101 (20.3%) 382 (19.2%) 0.58 2 126 (25.4%) 504 (25.4%) 0.93 3 102 (20.5%) 523 (26.3%) <0.01 4 168 (33.8%) 579 (29.1%) 0.04
NSAIDs, non-steroidal anti-inflammatory drugs.
*Corticosteroids, indicating oral and injection systemic corticosteroids but not topical use; chronic renal failure, including hemodialysis; malignancy, including all cancers; phototherapy including UVB and PUVA therapy.
**Including eastern Taiwan and offshore islands
¶Urbanization levels, a total of 8 levels published by the Institute of Occupational Safety and Health, Taiwan, 2009. Level 1 denotes the most urbanized area, and level 8 denotes the least urbanized area. As there were only very small numbers of psoriasis cases in some levels, we combined levels 3 and 4 into one group, denoted level 3, and levels 5 through 8 into another group, denoted level 4.
Table 3. Frequent users vs. infrequent users of prescriptions and the risk of TB among case and control subjects, in one year before the index date
1 Y Cases Controls OR (95% CI)
Adjusted OR* (95% CI) p-value ** Anti-psoriatic drugs¶ Non-user 433 1784 1 1 0.094 Infrequent user 36 104 1.43 (0.96-2.11) 1.12 (0.73-1.70) Frequent user 28 100 1.15 (0.75-1.78) 0.98 (0.62-1.55) Corticosteroids§ Non-user 187 1208 1 1 <0.0001 Infrequent user 179 498 2.32 (1.84-2.92) 2.08 (1.62-2.66) Frequent user 131 282 3.00 (2.32-3.88) 3.04 (2.24-4.14) NSAIDs§ Non-user 109 720 1 1 <0.0001 Infrequent user 201 707 1.88 (1.46-2.42) 1.63 (1.24-2.13) Frequent user 187 561 2.20 (1.70-2.86) 1.85 (1.36-2.52) COX-2 inhibitors§ Non-user 444 1830 1 1 0.048 Infrequent user 20 52 1.59 (0.94-2.68) 1.15 (0.66-2.01) Frequent user 33 106 1.28 (0.86-1.92) 0.97 (0.63-1.51) Abbreviations: CI, confidence interval; COX-2 inhibitors, cyclo-oxygenease 2 inhibitors; M, months; NSAID, non-steroidal anti-inflammatory drugs; TB, tuberculosis; Y, years.
¶Infrequent users, less than 90 days prescriptions per year; frequent users, 90 days or more prescriptions per year.
§Infrequent users, less than 2 prescriptions per month; frequent users, 2 and more prescriptions per month.
*Adjusted for age, gender, risk factors of TB (diabetes mellitus, chronic renal failure, silicosis, HIV infection, malignancy), use of anti-psoriatic drugs within one year prior to the index date, NSAID, COX-2 inhibitors, and geographic regions of Taiwan, urbanization level, hospital visits and psoriatic arthritis.
Table 4. The adjusted odd ratios of TB in different exposures of non-biologic systemic drugs in psoriasis
Psoriasis with TB
Psoriasis without TB
Crude OR Adjusted OR¶
(95% CI) (95% CI)
Current users*
Anti-psoriatic drugs§ 34 101 1.37 (0.92-2.05) 0.83 (0.52-1.31) Methotrexate and others§ 26 64 1.66 (1.04-2.65) 1.00 (0.59-1.70) Oral retinoids 10 37 1.08 (0.53-2.19) 0.72 (0.33-1.59) Corticosteroids 197 251 4.54 (3.64-5.68) 3.98 (3.12-5.06) NSAIDs 236 488 2.78 (2.27-3.41) 2.20 (1.76-2.76) COX-2 inhibitors 27 63 1.76 (1.11-2.79) 1.20 (0.71-2.01) New users** Anti-psoriatic drugs§ 10 21 1.92 (0.90-4.11) 1.51 (0.67-3.41) Methotrexate and others§ 7 17 1.88 (0.76-4.63) 1.57 (0.61-4.09) Oral retinoids 4 10 1.60 (0.50-5.14) 1.30 (0.36-4.68) Corticosteroids 86 118 3.32 (2.46-4.47) 2.92 (2.14-4.00)
NSAIDs 70 121 2.53 (1.85-3.46) 2.31 (1.66-3.22)
COX-2 inhibitors 15 28 2.18 (1.15-4.11) 1.97 (1.01-3.84) Abbreviations: CI, confidence interval; COX-2 inhibitors, cyclo-oxygenease 2
inhibitors; M, months; NSAID, non-steroidal anti-inflammatory drugs; TB, tuberculosis.
*Current user, individuals receiving drugs of interest within 45 days prior to index date.
**New user, individuals starting drugs of interest within 90 days prior to index date, without any of above prescriptions between 91-365 days prior to index date.
¶ Adjusted for age, gender, diabetes, chronic renal failure or hemodialysis, organ transplant, silicosis, HIV, prior malignancies, phototherapy, hospital visits, current use or new use of drugs of interest, geographic locations, level of urbanization, and hospital visits.
§ We divided systemic anti-psoriatic drugs into: methotrexate and others (including azathioprine and cyclosporine); and oral retinoids. Since some may use more than one drug, the total number of drug users may not equal to the sum of number in each drug categories.
Table 5. Sensitivity analyses for TB risk among psoriasis cohort, based on different assumptions.
Study cohorts Overall, N Observed, N Expected, N SIR 95% CI
Psoriasis cohort 81,266 497 407 1.22 1.18-1.33
Mild psoriasis* 50,729 283 266 1.06 1.02-1.19
Severe psoriasis§ 30,537 214 140 1.52 1.46-1.74
Severe psoriasis cohort excluding those receiving retinoids
20,941 147 98 1.49 1.39-1.76
Psoriasis cohort excluding those ever receiving systemic corticosteroids
8,179 44 29 1.52 1.37-2.04
Psoriasis cohort excluding psoriatic arthritis
77,795 472 390 1.21 1.17-1.32
Psoriasis cohort excluding
coexistent RA, SLE 80,828 492 404 1.22 1.18-1.33
Abbreviations: CI, confidence interval; N, number; RA, rheumatoid arthritis; SIR, standardized incidence rate; SLE, systemic lupus erythematosus.
*Mild psoriasis indicates original psoriasis cohort patients who did not receive any of systemic anti-psoriatic drugs or phototherapies
§Severe psoriasis indicates original psoriasis cohort patients ever received phototherapies or systemic anti-psoriatic drugs.