行政院國家科學委員會專題研究計畫 成果報告
解構台灣民眾「逛醫院」現象(第 2 年)
研究成果報告(完整版)
計 畫 類 別 : 個別型 計 畫 編 號 : NSC 96-2416-H-004-007-MY2 執 行 期 間 : 97 年 08 月 01 日至 99 年 07 月 31 日 執 行 單 位 : 國立政治大學公共行政及企業管理教育中心 計 畫 主 持 人 : 周麗芳 共 同 主 持 人 : 陳曾基 報 告 附 件 : 出席國際會議研究心得報告及發表論文 處 理 方 式 : 本計畫可公開查詢中 華 民 國 99 年 10 月 31 日
目錄 前言 P. 1 Introduction P. 2 Methods P. 3 Results P. 4 Discussion P. 5 References P. 8 Tables P. 10 計畫成果自評 P. 15
前言
在本多年期研究計畫經費贊助下,於執行研究計畫期間,已有數篇論文產出與 國際會議發表,目前尚有兩篇完稿論文投稿審查中,其中一篇已經初審修正後 再審中,以下謹以該篇論文為主軸作為期末報告。
(Revised manuscript under peer review. Please do not quote.)
Application of Frequent Itemsets Mining to Analyze
Patterns of One-Stop Visits in Taiwan
INTRODUCTION
The people in Taiwan have free choice of healthcare providers and therapies within the universal National Health Insurance (NHI) program starting in 1995. The NHI provides comprehensive benefits in ambulatory care for western and Chinese
medicines, dentistry, medications, laboratory examinations, surgeries, and inpatients services. The NHI and its contracted hospitals don't set a limit of physician visits within a day by a patient [1]. A patient can visit ambulatory clinics of any specialty in hospitals directly without formal referral and is only charged by a differential
copayment [2,3]. The great freedom in Taiwan’s NHI caused not only a high number of annual visits per capita [1], but also a unique “one-stop shopping phenomenon” [4], which refers to visits of several specialties at the same facility in one day by a patient. A previous study estimated 7.6% of people in Taiwan had one-stop visits during a year [4].
Most literatures referring to one-stop shopping of health care focused on improving the service process through integrated settings. For example, the medical mall, developed in the USA in late 1980s, created a one-stop shop for ambulatory primary care, dental services, specialties for referral, pharmacy, physical therapy, government services, diagnostics, and other health care needs [5]. The integrated process for patients could save time intervals between their physician consultation, assessment, investigation and management [6-9]. Hospitals also provided additional services to their patients and visitors, with mall-like retail shops in or around their facilities, letting patients feel as at the mall [10].
The visits to multiple specialties, if not integrated, would increase not only the expense but also the potential risk of polypharmacy [11]. Although the percentage of persons with one-stop visits in Taiwan has been reported in a previous study [4], the patterns of one-stop visits needed to be further clarified. To our knowledge, there was no study on patterns of visits to multiple specialties in one day, especially for a large population.
In the current study, we analyzed a nationally representative claims dataset of 1 million people in Taiwan to calculate the frequency of one-stop visits. Because the one-stop shopping phenomenon is not rare in Taiwan and medical practice includes 24 specialties and 22 subspecialties, the number of combination patterns of specialties visited by patients would be hardly calculable with regular statistics or database programs. We thus adopted one of data mining techniques (the frequent itemsets mining) to compute the combination patterns of specialties in the one-stop visits. The analysis of the special case of one-stop visits in Taiwan will extend the application of data mining techniques to health services research.
METHODS
Data Sources
The single-payer NHI in Taiwan has covered almost all inhabitants (22,314,647 beneficiaries at the end of 2005, equaling 98.0% of all population). The NHI's
electronic claims datasets, merged into a large computerized database as the National Health Insurance Research Database (NHIRD), have been released to the public for research purpose since 1999 [12]. The database contains original claims for
reimbursement plus registration files of beneficiaries and healthcare facilities. The identification numbers of persons and healthcare facilities in the datasets have been encrypted to protect privacy, but the encrypted identification numbers remain unique so that record-linking within datasets is feasible. All researchers who apply for use of the NHIRD are required to sign a written agreement declaring that they could not violate the privacy of patients or healthcare providers and should acknowledge the NHIRD on publication.
One special subset of NHIRD, the Longitudinal Health Insurance Database for 2005 (LHID2005), contains all the registration and original claims data of 1,000,000 persons from 1996 to 2008. These 1,000,000 persons were randomly sampled from the 22,717,053 beneficiaries of the NHI program during the period from 1 January to 31 December 2005. According to NHIRD, there was no significant difference in the age, gender distribution and utilization between the people in the LHID2005 and those in the complete NHIRD datasets. Our analysis was limited to the year 2005.
Study Design
In 2005, the 1-million-person cohort had 15,037,163 ambulatory visit records. Only those with physician consultations of western medicine, dentistry, and traditional Chinese medicine were analyzed. We excluded the visits to emergency departments, prescription refills, home care by nurses, and preventive services without physician consultation.
One-stop visits in the current study were operationally defined as more than one visit for different specialties at the same healthcare facility on the same day by a patient. At first, the patients who had one-stop visits were extracted. The numbers and percentage of patients with one-stop visits in each age group and gender were calculated. We also compared them with the 1-million-person cohort.
The NHI in Taiwan divided medical specialties into 24 specialties and 22
subspecialties. The subspecialties, existing mostly at hospitals, were considered as different ones from their main specialties in our study. As to the combination patterns of specialties in one-stop visits, there would be theoretically 1,035 two-specialty combinations, 15,180 three-specialty combinations, 163,185 four-specialty
combinations, and so on. If the number of visits in a day by a patient was not limited, the total kinds of possible specialty combinations would be about 7×1013. The
solution without additional module or scripting. Besides, the statistical software is usually not suitable for processing a large amount of data. To overcome these difficulties, we adopted the frequent itemsets mining to tackle our research problem.
The frequent itemsets mining, a type of association rule mining, was developed in 1990s to analyze which groups of goods or sets of items were frequently purchased together. It has been used extensively in commercial marketing [13-15]. The most important concept of frequent itemsets mining is "minimal support". Among all items bought by a customer in one transaction there can be many subsets of items (itemsets), i.e. many possible combinations of individual items. If an itemset is repeatedly
purchased with the frequency not less than the minimal support, then it is marked as a frequent itemset. The preset minimal support enables efficient computing of large-scale data. We have applied such a data mining technique to analyze the Taiwan’s NHI claims databases in previous researches [16-18].
In the current study, the one-stop visits made by a patient to the same facility in one day correspond to items of one transaction in frequent itemsets mining. We set the minimal support for visit frequency at different levels iteratively, from 1000, 500, 100 and so on, to obtain frequent combinations of specialties (itemsets) in one-stop visits. The frequent combinations of specialties would be stratified by number of specialties (number of items in an itemset) in the final display.
Data Processing
The open-source software Perl (version 5.10.0) [19] was used for computing. The module of Data::Mining::AssociationRules version 0.1 by Dan Frankowski [20] was modified and integrated into the programming script. The regular statistics were displayed. In calculating the percentages of patients, the denominator was 1,000,000 according to the registry for beneficiaries in 2005.
RESULTS
There were 504,183 women and 495,817 men among the 1,000,000-person cohort in 2005. The ambulatory care visits with physician consultation amounted to 13,682,469 visits, and 79,371 (7.9%) persons did not have any visit during the year. The average number of visits per person was 13.7 (SD 14.6) in 2005. Nearly one fourth (n = 3,342,907) of visits were made to outpatient departments of hospitals.
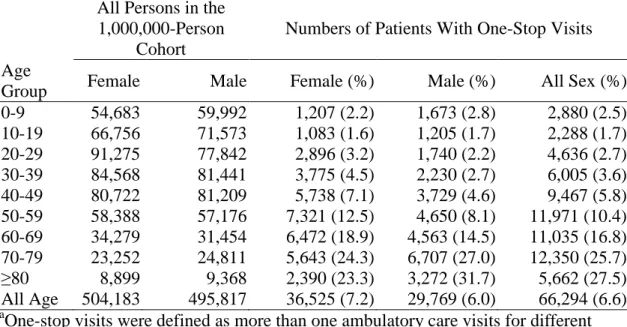
One-stop visits occurred 144,132 times and involved 296,822 visits (2.2% of all visits) by 66,294 (6.6%) persons. The percentage of the persons with one-stop shopping behavior increased with age after age 10 and reached to the highest in the age group ≥80 years as 27.5% (5,662 of 20,579). In general, women were more likely to have this behavior than men (7.2% vs. 6.0%) (Table 1).
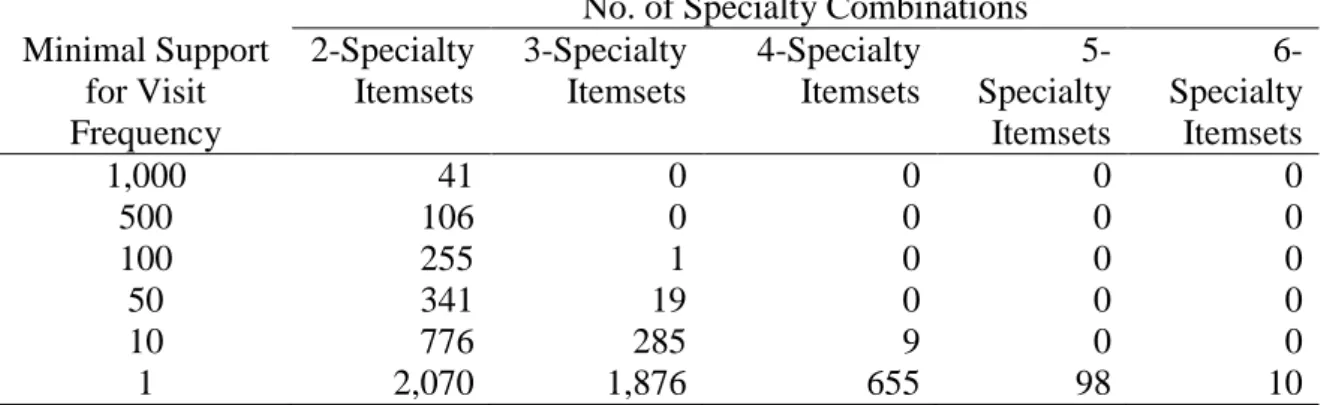
When we set the minimal support for visit frequency at 1000, only 41 two-specialty itemsets were found in all visits. Until the minimal support set at 100, one three-specialty itemset began to appear. When the minimal support set at 10, the four-specialty itemsets could be obtained. The largest number of specialties visited at the same facility in one day by a patient was six. The overall number of different
combinations was 4,709(Table 2).
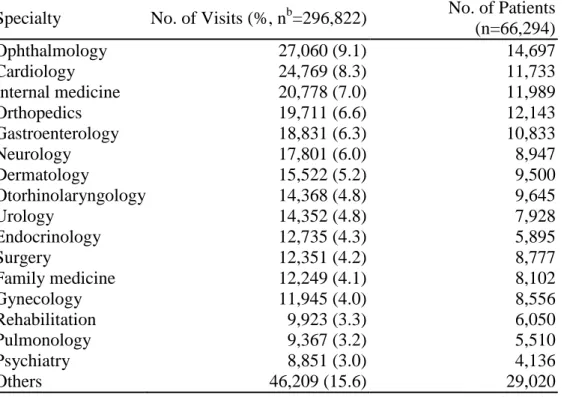
Among one-stop visits, the most frequently visited specialties were ophthalmology, internal medicine, and cardiology. These three specialties had accounted for 72,607 (24.4%) visits in all one-stop visits (Table 3).
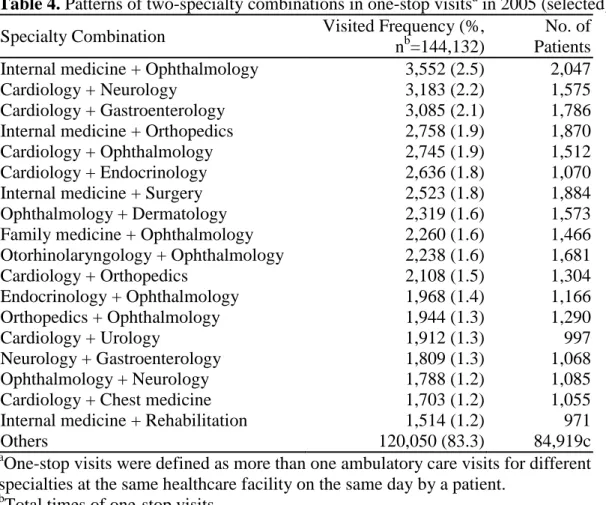
As to the combinations of specialties in one-stop visits, internal medicine plus ophthalmology was the most frequent combination with a visited frequency of 3,552 times (2.5% of 144,132 times of one-stop visits), followed by cardiology plus neurology with a visited frequency of 3,183 times (2.2%). The two-specialty
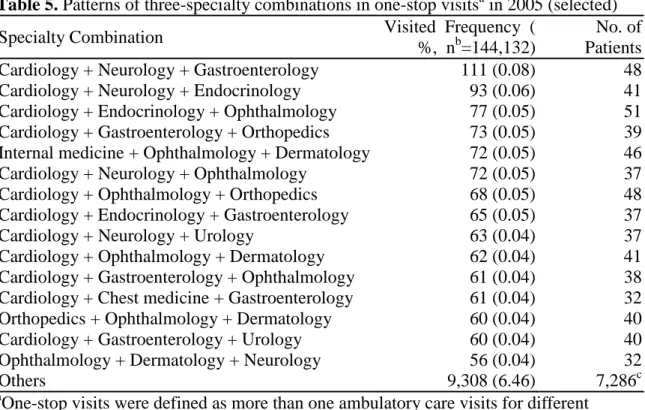
combinations (itemsets) with a visited frequency >=1000 were selectively displayed in Table 4. The most frequent three-specialty combination was cardiology plus neurology and gastroenterology, but only with a visited frequency of 111 times (0.08%) (Table 5).
DISCUSSION
The association rule mining, also known as market basket analysis, has been used to analyze the large database for the commercial marketing for more than one decade [14]. Our research team had successfully applied this data mining technique in medical researches, especially to analyze the co-prescriptions of drugs. We had identified the drugs prescribed in combination with antacids from the Taiwan NHI claims [16]. We had also analyzed the prescription patterns of Chinese herbal
medicine for patients with allergic rhinitis [17], and chronic hepatitis [18] in Taiwan. In the current study, we further extended the frequent itemsets mining, a type of association rule mining, to the study of patient's behavior. Our approach offered another novel application of this data mining technique.
The possible reasons of the one-stop shopping phenomenon in Taiwan would be as follows: First, the NHI and its contracted hospitals don't set a limit of physician visits within a day by a patient. Direct visits to any specialty clinic in hospitals without formal referral are only charged by a differential copayment. Second, the hospitals are very easily accessible in this densely populated island country. They generally
provide varieties of specialties in their outpatient departments and advanced medical equipments in ambulatory cares. It is very convenient for the patients to have different kinds of medical services at one site in a day. Third, the number of people with
multimorbidity might increase in Taiwan’s aging society. The current practice of medicine in Taiwan is fragmented into many subspecialties without integration and the multimorbid patients might not be treated efficiently.
Our study revealed that the elderly were more likely to have one-stop shopping behavior and the percentage was above 25% in those aged 70 and over.
Multimorbidity in the elderly might be the major reason. Before age 70, the percentage of one-stop shopping among men was lower than that among women. Perhaps men tended to delay health help-seeking [21]. After age 70, the gender disparity reversed. Because of shorter life expectancy, men might have poorer health at the late stage of life.
facility in a day, there would be theoretically a hundred trillion of combination patterns. In reality, the time constraint prevents a patient from visiting too many specialties in one day. In the current study, the greatest number of visited specialties in a one-stop shopping was only six, far fewer than the number of items held in a shopping basket of a supermarket. The number of combination patterns in our study was correspondingly fewer than that in commercial market basket analyses.
In the current study, ophthalmology was the most frequently visited specialty in one-stop visits, although it was only at the 7th place among all ambulatory visits in Taiwan [4]. A study of multimorbidity in Sweden also found that comorbidity occurred beyond chance and the most frequent pattern of co-existing diseases was visual impairment with heart disease [22]. The comorbidity of the visual problem with other diseases reflected the prevalence of diseases among specific patient groups at the demand side in Taiwan. On the other hand, the underlying reason might be at the supply side in that the ophthalmologist’s techniques could not be easily substituted by other specialists and the hospitals offered more advanced equipments than practicing ophthalmologists.
As comorbidity usually increased with age and in patients with chronic conditions, the other top frequently visited specialties in one-stop visits for cardiology, internal medicine, orthopedics, gastroenterology, and neurology were compatible with the chronic conditions usually seen in the elderly [23,24]. The otorhinolaryngology in the 7th place might just reflect the high service volume of this specialty in Taiwan’s ambulatory care for diseases of the respiratory system [4].
As for the combination patterns, the top ones with minimal support of 1000 might reflect the frequent comorbid conditions in patients with one-stop visits. Many combinations, such as those between cardiology, neurology, gastroenterology and endocrinology, could be substituted by family medicine or internal medicine to decrease the fragmentation of care. On the other hand, some combinations might reflect the necessity of different specialties’ management, such as internal medicine, cardiology, endocrinology, neurology, otorhinolaryngology or family medicine plus ophthalmology, orthopedics, surgery, urology or rehabilitation. These combinations could be considered into integrated care clinics if the healthcare facilities intend to improve the service process and patient satisfaction.
In the current study, the patterns of specialty combinations in one-stop visits were extremely diverse and the number of visits in each combination, even the most
frequent one, was relatively low. The practical meaning is that it would be difficult for hospitals to offer customized, integrated, and efficient services under circumstances of low economies of scale. The one-stop visits are indeed convenient to patients who need various specialties to treat their problems. But the risk of induced demand and polypharmacy deserves further attention. The NHI in Taiwan has to establish a more regulated referral system with family physicians as health gatekeepers, especially for those with multiple chronic diseases.
Limitations
Our study has some limitations. First, the income and residence of beneficiaries were not available in the NHIRD for privacy protection. The influence of socioeconomic
factors on one-stop visits couldn’t be explored. Second, the claims didn't contain data about the referral. We couldn't differentiate whether the one-stop visits were initiated by physicians’ referral in the same healthcare facility or out of patients’ free choice. Third, our study design might overlook the influence of disease types. In the NHI, only three diagnoses could be coded in one ambulatory visit. The coding was
undertaken by physicians for administrative purpose and seldom verified. Fourth, our study was limited to specialties visited in one day. If a patient visited several
specialties of the same healthcare facility in a short period of days, it might otherwise imply the inefficiency of managerial operation. Finally, because the phenomenon of one-stop visits is a special, if not unique, case of health care in one specific country (Taiwan), our data-mining approach can be applied to other countries only when a similar environment without strict regulation on patient access to health care exists and extensive datasets are openly available to analysis.
Conclusions
With the data mining technique, we had successfully analyzed the diverse patterns of specialty combinations in one-stop visits from large-scale datasets, what was hardly feasible with an ordinary statistical method. Our approach demonstrated another novel application of frequent itemsets mining to the research of patients’ behaviors. The results could provide useful information either for the hospital manager to set up integrated care of health service and for the policymaker to rebuild the health care system.
Acknowledgments
This study is based in part on data from the National Health Insurance Research Database provided by the Bureau of National Health Insurance, Department of Health and managed by National Health Research Institutes. The interpretation and
conclusions contained herein do not represent those of Bureau of National Health Insurance, Department of Health or National Health Research Institutes. This study was supported by grants from and the National Science Council (NSC 96-2416-H-004-007-MY2) and the Taipei Veterans General Hospital (V98S2-006).
REFERENCES
1. Cheng TM (2003) Taiwan's new national health insurance program: genesis and experience so far. Health Aff (Millwood) 22: 61-76.
2. Bureau of National Health Inssurance: Referral Services in National Health Insurance, Taiwan. Available:
http://www.nhi.gov.tw/english/webdata.asp?menu=11&menu_id=592&webdat a_id=3165. Accessed 2010 March 3.
3. Bureau of National Health Inssurance: Copayments in National Health Insurance, Taiwan. Available:
http://www.nhi.gov.tw/english/webdata.asp?menu=11&menu_id=592&webdat a_id=3161. Accessed 2010 March 3.
4. Chen TJ, Chou LF, Hwang SJ (2006) Patterns of ambulatory care utilization in Taiwan. BMC Health Serv Res 6: 54.
5. Anonymous (1996) Medical mall: one-stop shopping for outpatients. ED Manag 8: 40-44.
6. Nguyen T (2005) One stop shopping: providing today’s competitive cardiovascular service. J Interv Cardiol 18: 107-110.
7. Birns J, Vilasuso M, Cohen DL (2006) One-stop clinics are more effective than neurology clinics for TIA. Age Ageing 35: 306-308.
8. Jackson J (2009) One-stop outpatient and pre-operative assessment. Nurs Manag (Harrow) 15: 24-28.
9. Reid MJ, David LA, Nicholl JE (2009) A one-stop carpal tunnel clinic. Ann R Coll Surg Engl 91: 301-304.
10. Romano M (2002) One-stop shopping. Forget the typical gift shop. As retail options soar, patients might think they’re at the mall, not the community hospital. Mod Healthc 32(10): 32-35.
11. Tamblyn RM, McLeod PJ, Abrahamowicz M, Laprise R (1996) Do too many cooks spoil the broth? Multiple physician involvement in medical management of elderly patients and potentially inappropriate drug combinations. CMAJ 154: 1177-1184.
12. National Health Research Institutes: National Health Insurance Research
Database. Available: http://w3.nhri.org.tw/nhird//en/index.htm. Accessed 2010 Feb 06.
13. Agrawal R, Imielinski T, Swami A. Mining association rules between sets of items in large databases. Proceedings of the 1993 ACM SIGMOD International Conference on Management of Data, 207-216.
Customer Support. New York: John Wiley & Sons.
15. Han J, Kamber M (2006) Data Mining: Concepts and Techniques. San Francisco: Morgan Kaufmann.
16. Chen TJ, Chou LF, Hwang SJ (2003) Application of a data-mining technique to analyze coprescription patterns for antacids in Taiwan. Clin Ther 25: 2453-2463.
17. Kung YY, Chen YC, Hwang SJ, Chen TJ, Chen FP (2006) The prescriptions frequencies and patterns of Chinese herbal medicine for allergic rhinitis in Taiwan. Allergy 61: 1316-1318.
18. Chen FP, Kung YY, Chen YC, Jong MS, Chen TJ, et al. (2008) Frequency and pattern of Chinese herbal medicine prescriptions for chronic hepatitis in Taiwan. J Ethnopharmacol 117: 84-91.
19. ActiveState ActivePerl. Available: http://www.activestate.com/activeperl/. Accessed 2010 March 3.
20. Frankowski D (2004) Data-Mining-AssociationRules-0.10. Available: http://search.cpan.org/~dfrankow/Data-Mining-AssociationRules-0.10/. Accessed 2010 March 3.
21. Galdas PM, Cheater F, Marshall P (2005) Men and health help-seeking behaviour: literature review. J Adv Nurs 49: 616-623.
22. Marengoni A, Rizzuto D, Wang HX, Winblad B, Fratiglioni L (2009) Patterns of chronic multimorbidity in the elderly population. J Am Geriatr Soc 57: 225-230.
23. Liu Z, Albanese E, Li S, Huang Y, Ferri CP, et al. (2009) Chronic disease prevalence and care among the elderly in urban and rural Beijing, China - a 10/66 Dementia Research Group cross-sectional survey. BMC Public Health 9: 394.
24. Naughton C, Bennett K, Feely J (2006) Prevalence of chronic disease in the elderly based on a national pharmacy claims database. Age Ageing 35: 633-636.
Table 1. Distribution of patients with one-stop visitsa in 2005, stratified by age and sex
All Persons in the 1,000,000-Person
Cohort
Numbers of Patients With One-Stop Visits
Age
Group Female Male Female (%) Male (%) All Sex (%) 0-9 54,683 59,992 1,207 (2.2) 1,673 (2.8) 2,880 (2.5) 10-19 66,756 71,573 1,083 (1.6) 1,205 (1.7) 2,288 (1.7) 20-29 91,275 77,842 2,896 (3.2) 1,740 (2.2) 4,636 (2.7) 30-39 84,568 81,441 3,775 (4.5) 2,230 (2.7) 6,005 (3.6) 40-49 80,722 81,209 5,738 (7.1) 3,729 (4.6) 9,467 (5.8) 50-59 58,388 57,176 7,321 (12.5) 4,650 (8.1) 11,971 (10.4) 60-69 34,279 31,454 6,472 (18.9) 4,563 (14.5) 11,035 (16.8) 70-79 23,252 24,811 5,643 (24.3) 6,707 (27.0) 12,350 (25.7) ≥80 8,899 9,368 2,390 (23.3) 3,272 (31.7) 5,662 (27.5) All Age 504,183 495,817 36,525 (7.2) 29,769 (6.0) 66,294 (6.6) a
One-stop visits were defined as more than one ambulatory care visits for different specialties at the same healthcare facility on the same day by a patient.
Table 2. Numbers of specialtycombinations (itemsets)a for one-stop visitsb at different minimal supports for visit frequency of an itemset, stratified by number of specialties in an itemset
No. of Specialty Combinations Minimal Support for Visit Frequency 2-Specialty Itemsets 3-Specialty Itemsets 4-Specialty Itemsets 5-Specialty Itemsets 6-Specialty Itemsets 1,000 41 0 0 0 0 500 106 0 0 0 0 100 255 1 0 0 0 50 341 19 0 0 0 10 776 285 9 0 0 1 2,070 1,876 655 98 10 a
Subsets of specialties visited by a patient at the same health care facility on the same day.
b
One-stop visits were defined as more than one ambulatory care visits for different specialties at the same healthcare facility on the same day by a patient.
Table 3. Numbers of visits and patients in all one-stop visitsa in 2005, stratified by consulted specialty (selected)
Specialty No. of Visits (%, nb=296,822) No. of Patients (n=66,294) Ophthalmology 27,060 (9.1) 14,697 Cardiology 24,769 (8.3) 11,733 Internal medicine 20,778 (7.0) 11,989 Orthopedics 19,711 (6.6) 12,143 Gastroenterology 18,831 (6.3) 10,833 Neurology 17,801 (6.0) 8,947 Dermatology 15,522 (5.2) 9,500 Otorhinolaryngology 14,368 (4.8) 9,645 Urology 14,352 (4.8) 7,928 Endocrinology 12,735 (4.3) 5,895 Surgery 12,351 (4.2) 8,777 Family medicine 12,249 (4.1) 8,102 Gynecology 11,945 (4.0) 8,556 Rehabilitation 9,923 (3.3) 6,050 Pulmonology 9,367 (3.2) 5,510 Psychiatry 8,851 (3.0) 4,136 Others 46,209 (15.6) 29,020 a
One-stop visits were defined as more than one ambulatory care visits for different specialties at the same healthcare facility on the same day by a patient.
b
Table 4. Patterns of two-specialty combinations in one-stop visitsa in 2005 (selected) Specialty Combination Visited Frequency (%,
nb=144,132)
No. of Patients Internal medicine + Ophthalmology 3,552 (2.5) 2,047 Cardiology + Neurology 3,183 (2.2) 1,575 Cardiology + Gastroenterology 3,085 (2.1) 1,786 Internal medicine + Orthopedics 2,758 (1.9) 1,870 Cardiology + Ophthalmology 2,745 (1.9) 1,512 Cardiology + Endocrinology 2,636 (1.8) 1,070 Internal medicine + Surgery 2,523 (1.8) 1,884 Ophthalmology + Dermatology 2,319 (1.6) 1,573 Family medicine + Ophthalmology 2,260 (1.6) 1,466 Otorhinolaryngology + Ophthalmology 2,238 (1.6) 1,681 Cardiology + Orthopedics 2,108 (1.5) 1,304 Endocrinology + Ophthalmology 1,968 (1.4) 1,166 Orthopedics + Ophthalmology 1,944 (1.3) 1,290 Cardiology + Urology 1,912 (1.3) 997 Neurology + Gastroenterology 1,809 (1.3) 1,068 Ophthalmology + Neurology 1,788 (1.2) 1,085 Cardiology + Chest medicine 1,703 (1.2) 1,055 Internal medicine + Rehabilitation 1,514 (1.2) 971 Others 120,050 (83.3) 84,919c a
One-stop visits were defined as more than one ambulatory care visits for different specialties at the same healthcare facility on the same day by a patient.
b
Total times of one-stop visits. c
Table 5. Patterns of three-specialty combinations in one-stop visitsa in 2005 (selected) Specialty Combination Visited Frequency (
%, nb=144,132)
No. of Patients Cardiology + Neurology + Gastroenterology 111 (0.08) 48 Cardiology + Neurology + Endocrinology 93 (0.06) 41 Cardiology + Endocrinology + Ophthalmology 77 (0.05) 51 Cardiology + Gastroenterology + Orthopedics 73 (0.05) 39 Internal medicine + Ophthalmology + Dermatology 72 (0.05) 46 Cardiology + Neurology + Ophthalmology 72 (0.05) 37 Cardiology + Ophthalmology + Orthopedics 68 (0.05) 48 Cardiology + Endocrinology + Gastroenterology 65 (0.05) 37 Cardiology + Neurology + Urology 63 (0.04) 37 Cardiology + Ophthalmology + Dermatology 62 (0.04) 41 Cardiology + Gastroenterology + Ophthalmology 61 (0.04) 38 Cardiology + Chest medicine + Gastroenterology 61 (0.04) 32 Orthopedics + Ophthalmology + Dermatology 60 (0.04) 40 Cardiology + Gastroenterology + Urology 60 (0.04) 40 Ophthalmology + Dermatology + Neurology 56 (0.04) 32 Others 9,308 (6.46) 7,286c a
One-stop visits were defined as more than one ambulatory care visits for different specialties at the same healthcare facility on the same day by a patient.
b
Total times of one-stop visits. c
計畫成果自評
本研究計畫成果內容係依照原申請計畫逐步執行,與原計畫相符,亦達成預期 目標。本研究團隊於研究計畫執行期間的成果可分為四個面向:(一)利用全民 健康保險研究資料庫的歸人抽樣檔,瞭解特殊病患的 pathway and access to medical care,首篇論文已發表(Pattern and consequences of first visits to
obstetricians/gynecologists by adolescents: a nationwide study in Taiwan. J Chin Med Assoc 2010;73(3):144-149.),另有一篇論文則係探討精神科就診情形,已完成初 稿。(二)藉助研究經費特別訂購全民健康保險研究資料庫資料,特別是持有重 大傷病卡的病患 cohort data,建立架構以提供實證資料給各種研究構想,首篇 論文已發表(The effect of weather on peritoneal dialysis prescription - seasonal variation in PD dialysate utilization. Perit Dial Int 2010;30:320-328.),預期未來陸 續會有其他成果發表。(三)探討 doctor-shopping 與 polypharmacy 的關係,意 即欲瞭解是 seeking help 或 seeking drugs,初步成果兩篇已於國際會議發表( Relationship of doctor shopping and polypharmacy: a nationwide study in Taiwa. Value Health 2008;11:A39.)、(Benzodiazepine use among frequent attenders to emergency departments: a nationwide study in Taiwan. Value Health 2009;12:A364.) 。(四)利用資料探勘的技術(特別是 association rule mining)分析 doctor-shopping 行為,已完成兩篇論文投稿審查中,其中一篇已經初審修正後再審中 。
出席國際學術會議心得報告
計畫編號 NSC 96-2416-H-004-007-MY2 計畫名稱 解構台灣民眾「逛醫院」現象 出國人員姓名 服務機關及職稱 周麗芳 國立政治大學 財政學系 教授 會議時間地點 2010 年 5 月 15 至 19 日 美國喬治亞州亞特蘭大市 Hilton Atlanta會議名稱 ISPOR (International Society for Pharmacoeconomics and Outcomes Research) 15th International Annual Meeting
發表論文題目 Drugs cheaper than threepenny: the market of extremely low-priced drugs within the National Health Insurance in Taiwan
一、參加會議經過
國際藥品經濟與效果研究學會 (International Society for Pharmacoeconomics and Outcomes Research, ISPOR) 係相當活躍的國際學術組織,本會加上全球各地分會,擁有 超過 8000 名會員。ISPOR 在台灣亦有分會(Taiwan Chapter)。ISPOR 每年舉行三大會議, 北美與歐洲各一,另一則在其他地區舉行(2010 年 9 月在泰國普吉市)。ISPOR 出版有 「Value in Health」月刊,為 SCI 期刊資料庫收錄,2009 年的 Impact Factor 為 3.032,在 Health Care Sciences & Services 類別 69 種期刊中排名第 7。
今(2010)年 ISPOR 在美國喬治亞州亞特蘭大市舉行的第十五屆國際會議,為期五 天,依往例會議前兩天(5 月 15 日至 16 日)係在週末,舉辦短期教育課程(short course program, educational symposium),後三天(5 月 17 日至 19 日)為科學研究性質活動。ISPOR 年度國際會議,參與者一年比一年增加,今年有 1,024 件 poster presentations、60 場 research podiums、38 場 workshops、12 場 issue panels。台灣學界向來參與 ISPOR 盛會相當踴躍, 今年有國立陽明大學醫學院衛生福利研究所黃文鴻教授(曾任衛生署藥政處長,也是筆 者二十多年前就讀碩士班時的老師)率領研究團隊參加。
此次會議 poster presentations 主要分成幾大部分:(第一天)Methods & Concepts、 Cancer、Diabetes/Endocrine Disorders、GI Disorders、Urinary/Kidney Disorders、(第二天) Health Care Decision Maker’s Case Studies、Health Policy、Mental Health、Muscular-Skeletal Disorders、Neurological Disorders、Sensory Systems Disorders、(第 三天)Cardiovascular Disorders、Individual’s Health、Infections、Respiratory-Related Disorders、Systemic Disorders/Conditions。所有論文摘要皆收錄於「Value in Health」期刊 2010 年第 13 卷第 3 期。本人此次與會發表論文被歸類在 Health Policy 類下 Health Care Costs & Management 主題(PHP50)(Value in Health 2010;13(3):A90.)。
本人發表論文題目為:「Drugs cheaper than threepenny: the market of extremely
品市場的現況規模,特別以藥品單價為一元作為劃分點,研究資料來自國家衛生研究院 全民健康保險研究資料庫 2007 年門診系統抽樣檔與特約藥局完整申報檔,研究結果顯 示:健保給付的口服藥品品項中,三分之一的品項單價小於等於一元;在所有開立的口 服藥品處方中,低價藥品佔了開立品項總數的將近一半,然而總金額卻只佔 4.1%,還不 及銷售第一名的單一品項的總金額。低價藥品是台灣醫療體系相當獨特的現象,值得進 一步深入研究。 此次會議不僅舉辦了眾多各類活動,也提供寬敞空間供各國學者自由討論意見交 流,是相當成功的國際會議。本人係近年內第四次參加 ISPOR 會議,欣見 ISPOR 與藥 品經濟逐年蓬勃發展。 二、與會心得 藥品在醫療扮演重要的角色,製藥亦是生技產業的主軸,藥品經濟則能協助相關議 題的規劃評估。與世界先進大國相較,台灣藥品市場規模並不大,不過,台灣有全民健 保,又有量大價廉的全民健康保險資料庫可供學術研究使用,是台灣學界得天獨厚之處。 台灣目前已有不少學者利用健康保險資料庫發表藥品流行病學、藥品利用、藥品經濟的 研究,成果豐碩,國際能見度應更高於以往。
1
DRUGS CHEAPER THAN THREEPENNY: THE MARKET OF
EXTREMELY LOW-PRICED DRUGS WITHIN THE NATIONAL
HEALTH INSURANCE IN TAIWAN
Chou LF1, Chen TJ2,3, Chou YC4,5 1
Department of Public Finance, National Chengchi University, Taipei,
Taiwan, 2Institute of Hospital and Health Care Administration, School of Medicine, National Yang-Ming University, Taipei, Taiwan,
3
Department of Family Medicine, Taipei Veterans General Hospital, Taipei, Taiwan, 4
Pharmacy Department, Taipei Veterans General Hospital, Taipei, Taiwan, 5
Institute of Pharmacology, School of Medicine, National Yang-Ming University, Taipei, Taiwan
OBJECTIVES: The National Health Insurance in Taiwan always faces the problem
of soaring drug expenditure. However, among the drug benefit scheme there is a great discrepancy in drug unit prices, with a lot of extremely low-priced drugs. The purpose of the study was to analyze the market situation of these cheap drugs. METHODS: The analysis was limited to the ambulatory setting. The data sources came from the claims datasets of prescriptions dispensed at contracted pharmacies (GO, complete) and at hospitals and clinics (OO, 1/500 sampling) in 2007, offered by the National Health Insurance Research Database in Taiwan. For favorable comparisons, the focus was on oral drugs with solid forms, e.g. tablets and capsules. The operational
definition of a cheap drug was set to the unit price not greater than 1 New Taiwan dollar (NTD). One NTD was equal to 0.03 US dollar in 2010. RESULTS: During the year, 13,594 distinct drug items had been prescribed 803,961,618 times with total expenditure of 87,794,653,006 NTD. Among them, 8,795 oral drug items accounted for 687,629,169 prescribed items (85.5% of total prescribed items) and
63,177,684,194 NTD (72.0% of total drug expenditure). According to the last price of each oral drug item at the end of 1997, the average unit price was 10.3 +/- 92.4 NTD, with minimum 0.06, maximum 4,111, median 1.5, 25 percentile 0.8 and 75 percentile 4.3, and 2,873 items (32.7% of oral drug items) had a unit price <= 1 NTD. While the top one item among all oral drugs had already a market share of 5.2%, 19 items 25% and 99 items 50%, the cheap drugs with aggregate frequency of 323,571,583
prescribed items (47.1% of all prescribed oral drug items) only accounted for 2,583,591,026 NTD (4.1% of expenditure for oral drugs and 2.9% of total drug expenditure). CONCLUSIONS: The drug market of the National Health Insurance in Taiwan was abundant in cheap drugs. The unreasonably low prices of drugs might not guarantee the quality of pharmaceutical care and the sustainability of a healthy
96 年度專題研究計畫研究成果彙整表
計畫主持人:周麗芳 計畫編號:96-2416-H-004-007-MY2 計畫名稱:解構台灣民眾「逛醫院」現象 量化 成果項目 實際已達成 數(被接受 或已發表) 預期總達成 數(含實際已 達成數) 本計畫實 際貢獻百 分比 單位 備 註 ( 質 化 說 明:如 數 個 計 畫 共 同 成 果、成 果 列 為 該 期 刊 之 封 面 故 事 ... 等) 期刊論文 1 2 100% 研究報告/技術報告 0 0 100% 研討會論文 0 0 100% 篇 論文著作 專書 0 0 100% 申請中件數 0 0 100% 專利 已獲得件數 0 0 100% 件 件數 0 0 100% 件 技術移轉 權利金 0 0 100% 千元 碩士生 0 0 100% 博士生 0 0 100% 博士後研究員 0 0 100% 國內 參與計畫人力 (本國籍) 專任助理 0 0 100% 人次 期刊論文 1 2 100% 研究報告/技術報告 0 0 100% 研討會論文 2 0 100% 篇 論文著作 專書 0 0 100% 章/本 申請中件數 0 0 100% 專利 已獲得件數 0 0 100% 件 件數 0 0 100% 件 技術移轉 權利金 0 0 100% 千元 碩士生 0 0 100% 博士生 0 0 100% 博士後研究員 0 0 100% 國外 參與計畫人力 (外國籍) 專任助理 0 0 100% 人次其他成果